Introduction
Radical resection of colorectal cancer is a
highly-traumatic abdominal surgery, which often directly leads to
excessive intestinal stress response (1), intestinal mucosal barrier dysfunction,
increase in permeability and translocation of pathogenic bacteria
and endotoxin, eventually resulting in expanded infection
threatening life. As one of the adjuvant treatment means of rapid
rehabilitation, the preoperative supplement of carbohydrate can
alleviate the surgery-induced stress response to a certain extent
(2), the clinical effect, however,
is not significant. Some studies have demonstrated that probiotics
are able to protect the intestinal mucosal barrier and improve the
imbalance of intestinal flora, and its role in the postoperative
rehabilitation therapy has attracted increasing attention (3). In this study, the effects of
preoperative oral administration of glucose solution combined with
postoperative probiotics on early inflammatory response, intestinal
barrier function and postoperative infective complications in
patients after colorectal cancer surgery were observed.
Patients and methods
General data
A total of 60 patients treated and scheduled to
undergo radical resection of colorectal cancer in The Second
Affiliated Hospital of Kunming Medical University (Kunming, China)
from March 2017 to December 2017 were selected and randomly divided
into the glucose solution group (n=30) and the combined probiotics
group (n=30). In the glucose solution group, 18 cases were male and
12 cases were female, aged 62.35 ±13.71 years. In the combined
probiotics group, there were 20 males and 10 females aged
61.03±15.28 years. Patients underwent various preoperative
examinations and were definitely diagnosed via pathological
examination. Exclusion criteria were: patients with severe organ
dysfunction, diabetes mellitus, delayed gastric emptying or other
surgical contraindications. General data, such as sex and age, were
comparable between the two groups. Before this study, all patients
or guardians signed the informed consent.
The study was approved by the Ethics Committee of
The Second Affiliated Hospital of Kunming Medical University.
Methods
Patients in both groups orally took 12.5% glucose
solution before surgery, and those in the combined probiotics group
received bifidus-triple viable preparation (Inner Mongolia Shuangqi
Pharmaceutical Co., Ltd., Inner Mongolia, China) every day for 7
consecutive days. After surgery, patients were treated with
nutritional support, anti-infection and prevention of stress
ulcer.
Detection indexes
The following indexes were detected at 1 day before
surgery and at 1, 3 and 7 days after surgery. The serum endotoxin
and insulin-like growth factor-I (IGF-I) were detected using the
Multiskan FC full-automatic microplate reader (Molecular Devices,
LLC, Sunnyvale, CA, USA). The serum D-lactic acid was detected
using the ultraviolet-visible spectrophotometer (Thermo Fisher
Scientific, Inc., Waltham, MA, USA). The midstream urinary
lactulose/mannitol (L/M) concentration in the morning was measured
using the LC2000 high-performance liquid chromatograph (Hitachi,
Tokyo, Japan). White blood cell count (WBC) and C-reactive protein
(CRP) were detected using the Labospect003 full-automatic
biochemical analyzer (Hitachi). A totla of 200 mg fresh feces
samples in two groups were kept in aseptic bag and stored in
refrigerator at −80°C. Total DNA in fecal samples was extracted by
QIAamp DNAStool MiniKit extraction kit (Qiagen, Dusseldorf,
Germany) according to its specifications. The copy number of
intestinal flora in faeces before surgery and at 7 days after
surgery was detected using the Thermal Cyclers quantitative
SYBR-Green PCR instrument (Thermo Fisher Scientific, Inc.). The
specific gene 16SrRNA of bacterial species was selected as the
amplification region. The specific reaction procedure was as
follows: pre-denaturation at 95°C for 5 min, denaturation at 95°C
for 30 sec, annealing for 40 sec, extension at 60°C for 30 sec, 40
cycles in total. Then the extension at 72°C for 5 min. Intestinal
bacterial primer sequences and annealing temperatures were as
follows: Bacillus bifidus: forward,
5′-GGGTGGTAATGCCCGGATG-3′ and reverse, 5′-TAAGCCATGGACTTTCACACC-3′;
59°C; Escherichia coli: forward,
5′-CATTGACGTTACCCGCAGAAGAAGC-3′ and reverse,
5′-CTCTACGAGACTCAAGCTTGC-3′; 64°C; Lactic acid bacteria:
forward, 5′-AGCAGTAGGGAATCTTCCA-3′ and reverse,
5′-ATTYCACCGCTACACATG-3′; 58°C; Enterococcus: forward,
5′-AACCTACCCATCAGAGGG-3′ and reverse, 5′-GACGTTCAGTTACTAACG-3′;
57°C. The experimental results were analyzed using the
2−ΔΔCq method (4).
The body temperature was measured every 4 h with an
electronic thermometer, and the duration of fever was recorded
(from the first day after operation to the time with normal body
temperature after operation, axillary temperature <37.4°C), and
the average heart rate was recorded by the ECG monitor. In
addition, the time of the first anal exsufflation (the time from
the beginning of the operation to the first anal exsufflation) was
recorded.
Statistical analysis
Statistical Product and Service Solutions 20.0
software (SPSS, Inc., Chicago, IL, USA) was used for statistical
analysis. Measurement data were presented as mean ± standard
deviation (mean ± SD). ANOVA and Dunnett's post hoc test was used
for multiple comparisons. P<0.05 was considered to indicate a
statistically significant difference.
Results
Comparison of endotoxin and IGF-I
levels before and after surgery between the two groups
The endotoxin level was increased compared with that
before surgery in both groups and was increased more significantly
in the glucose solution group than that in the combined probiotics
group. Τhere were statistically significant differences at 1 and 3
days after surgery between the two groups (P<0.05). The IGF-I
level was decreased in both groups and declined more significantly
in the combined probiotics group than that in the glucose solution
group. Τhere were statistically significant differences at 1, 3 and
7 days after surgery between the two groups. The above results
indicate that the preoperative application of glucose combined with
postoperative supplement of probiotics can inhibit the decline in
IGF-I, accelerate the removal of endotoxin and protect the
intestinal mucosal barrier function (Table I).
 | Table I.Changes in endotoxin and IGF-I levels
in both groups. |
Table I.
Changes in endotoxin and IGF-I levels
in both groups.
| Items | Groups | Before surgery | 1 day after
surgery | 3 days after
surgery | 7 days after
surgery |
|---|
| Endotoxin
(pg·ml−1) | Combined
probiotics | 2.25±0.05 | 2.33±0.09 | 2.62±0.40 | 2.40±0.16 |
|
| Glucose solution | 2.40±0.25 |
2.83±0.55a |
2.98±0.54a | 2.58±0.19 |
| IGF-I
(µg·l−1) | Glucose solution | 99.17±62.16 | 89.65±35.06 | 122.33±54.78 | 113.95±63.12 |
|
| Combined
probiotics | 94.15±56.61 |
54.62±25.39a |
91.15±39.92a |
82.04±40.69a |
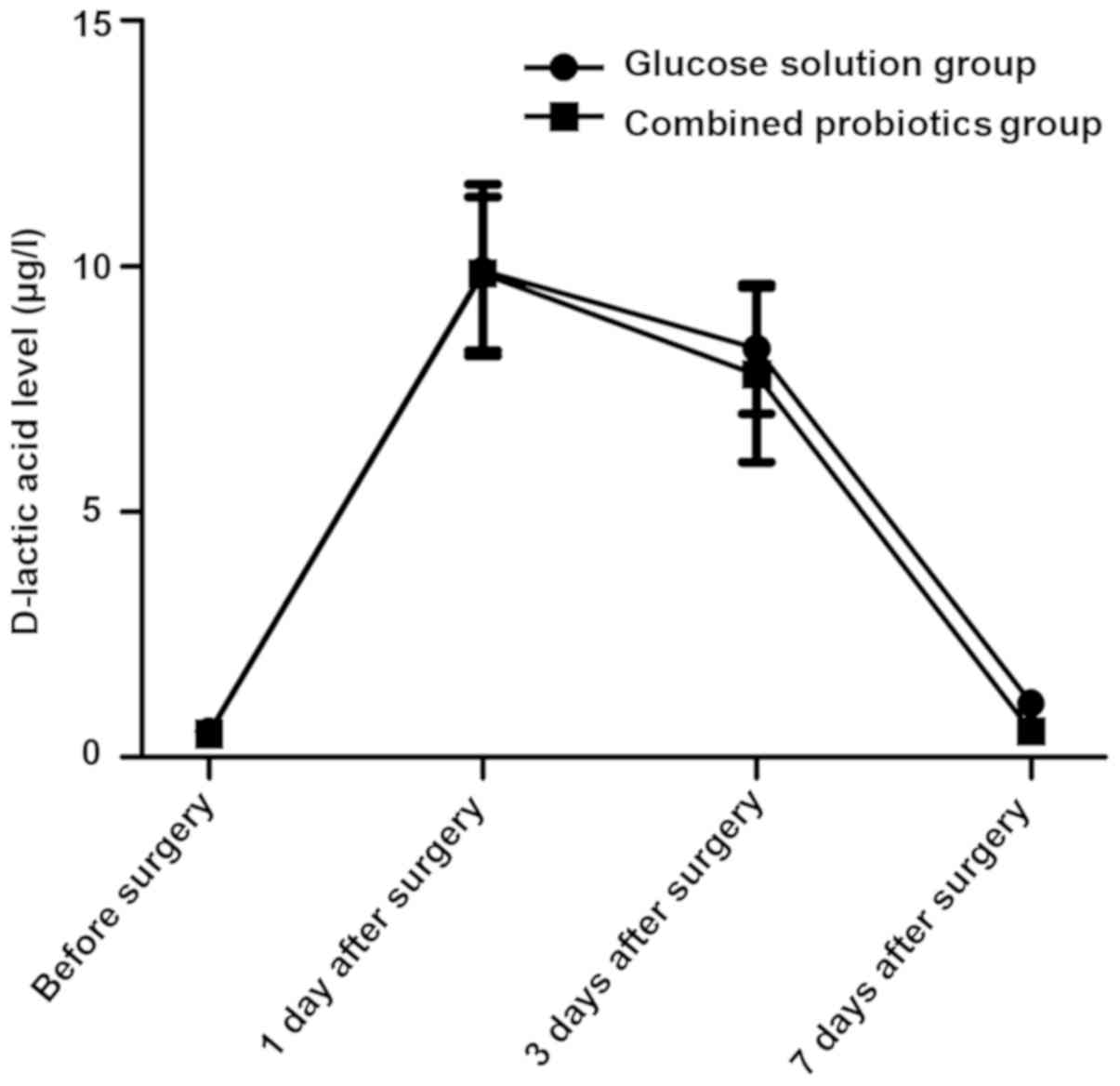
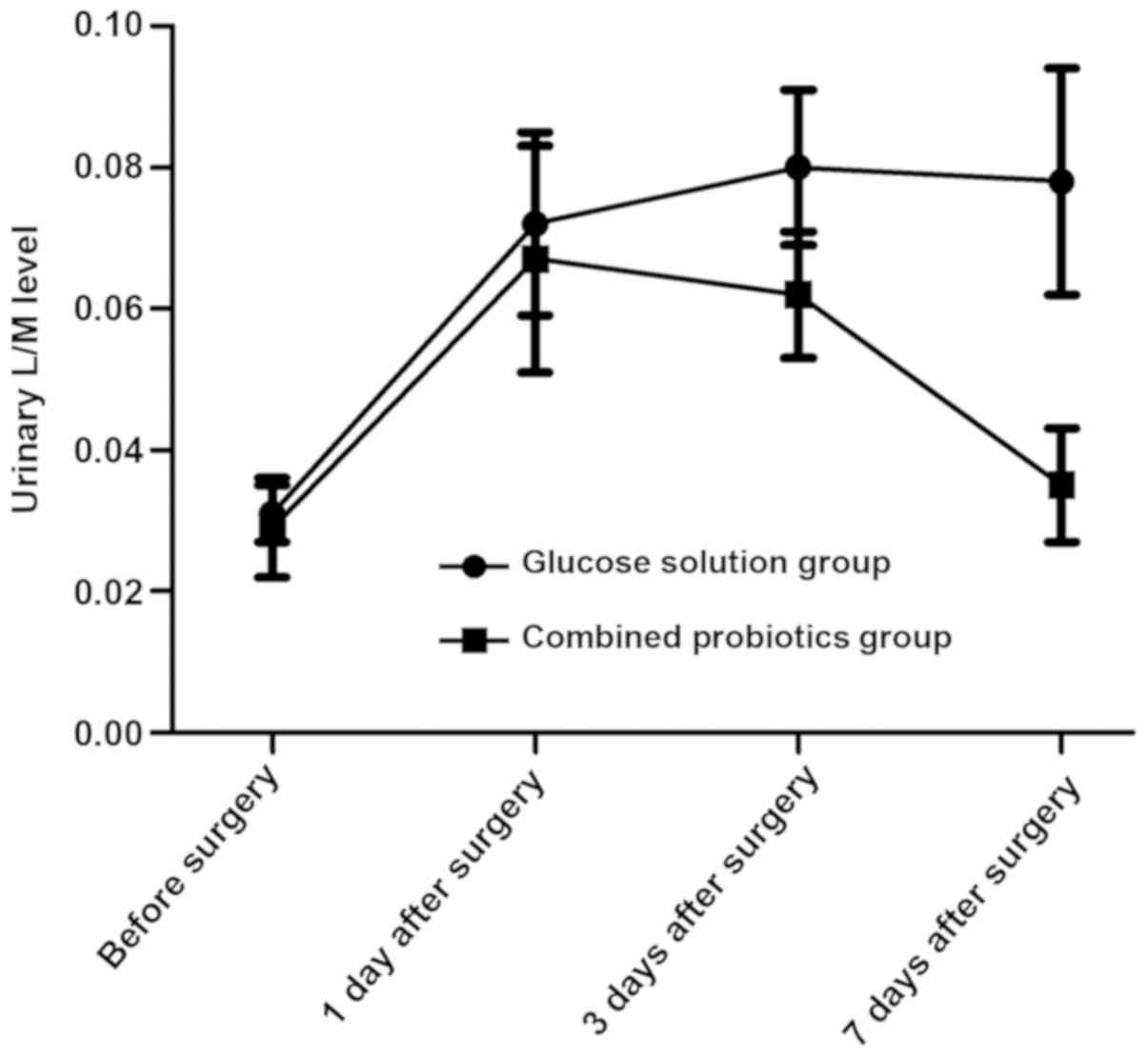
Comparison of D-lactic acid and
urinary L/M levels before and after surgery between the two
groups
The serum D-lactic acid and urinary L/M levels were
increased first and then decreased after surgery in both groups,
and they declined more obviously in the combined probiotics group
than those in the glucose solution group. Differences were
statistically significant at 7 days after surgery between the two
groups (P<0.05). The above results suggest that probiotics are
beneficial in reducing intestinal mucosal damage and permeability
(Figs. 1 and 2).
Comparison of CRP and WBC before and
after surgery between the two groups
The CRP level and WBC were increased first and then
gradually decreased to the normal range after surgery in both
groups, and they declined more obviously in the combined probiotics
group than those in the glucose solution group. Differences were
statistically significant at 3 and 7 days after surgery between the
two groups (P<0.05). The above results indicate that probiotics
can improve the systemic inflammatory response (Table II).
| Table II.CRP and WBC before and after surgery
in both groups. |
Table II.
CRP and WBC before and after surgery
in both groups.
| Items | Groups | Before surgery | 1 day after
surgery | 3 days after
surgery | 7 days after
surgery |
|---|
| WBC
(×109·l−1) | Glucose solution | 4.2±0.5 | 15.4±2.3 | 12.8±1.5 | 7.1±1.3 |
|
| Combined
probiotics | 4.3±0.5 | 15.0±2.1 | 8.5±1.1a | 5.6±0.9a |
| CRP
(mg·l−1) | Glucose solution | 6.3±0.4 | 90.1±10.5 | 69.8±9.2 | 46.7±5.3 |
|
| Combined
probiotics | 6.5±0.6 | 86.2±11.4 | 53.0±7.7a | 20.2±4.4a |
Changes in intestinal florae before
and after surgery in both groups
Results of quantitative PCR revealed that the copy
numbers of Bifidobacteria and Lactobacillus were
decreased after surgery in both groups compared with those before
surgery, and they declined more remarkably in the glucose solution
group than those in the combined probiotics group. Besides, the
copy numbers of Escherichia coli and Enterococcus
faecalis were increased, and they were increased more
remarkably in the glucose solution group than those in the combined
probiotic group. There were statistically significant differences
between the two groups (P<0.05). The above results indicate that
the postoperative supplement of probiotics can significantly
improve the intestinal micro-ecological environment and strengthen
the intestinal mucosal barrier function (Table III).
| Table III.Comparison of intestinal florae before
and after surgery in both groups. |
Table III.
Comparison of intestinal florae before
and after surgery in both groups.
| Groups | Time | Bifidobacteria
(copies/g) | Lactobacillus
(copies/g) | Escherichia coli
(copies/g) | Enterococcus
faecalis (copies/g) |
|---|
| Glucose solution | Before surgery | 9.5±0.5 | 9.2±0.8 | 8.1±0.6 | 8.1±0.7 |
|
| 7 days after
surgery | 8.1±0.6 | 5.6±0.6 | 9.8±0.8 | 9.6±0.8 |
| Combined
probiotics | Before surgery | 9.4±0.6 | 9.1±0.9 | 8.2±0.4 | 8.1±0.6 |
|
| 7 days after
surgery | 8.5±0.5a | 7.9±0.6a |
9.3±0.7a | 9.0±0.9a |
Comparison of the postoperative
general condition between the two groups
It was found after observation for 1 week that the
incidence rates of incision infection and hypoproteinemia were
similar in both groups (P>0.05). The duration of postoperative
fever, average heart rate at 7 days after surgery and first exhaust
time were shorter and lower in the combined probiotics group than
those in the glucose solution group (P<0.05) (Table IV).
| Table IV.Comparison of the postoperative
general condition between the two groups at 7 days after
surgery. |
Table IV.
Comparison of the postoperative
general condition between the two groups at 7 days after
surgery.
| Groups | Average heart
rate | Incision infection
(%) | Hypoproteinemia
(%) | Duration of
postoperative fever (days) | First exhaust time
(days) |
|---|
| Glucose solution | 102.83±8.36 | 10.8 | 7.6 | 6.07±1.11 | 4.3±1.5 |
| Combined
probiotics |
87.46±7.01a |
8.1 | 5.5 |
4.08±0.60a |
3.0±1.3a |
Discussion
According to a number of studies, it has been
confirmed that the surgical trauma-induced stress response directly
causes damage to the intestinal mucosal barrier, and thus, the
intestinal microflora and endotoxin entering the extraintestinal
tissues and organs under the increased permeability of intestinal
mucosa, are likely to lead to uncontrolled systemic inflammatory
response and multiple organ failure (5–8). The
intestinal flora, including anaerobe and probiotics, is an
important component of the intestinal mucosal barrier, among which
probiotics, dominated by Bifidobacteria and
Lactobacillus, can effectively resist the growth of harmful
bacteria through the biological effect (9). Fundamental research has manifested that
probiotics are able to promote the intestinal epithelial growth,
increase the mucus secretion, inhibit the intestinal epithelial
apoptosis and antioxidant function, and regulate the intestinal
immune function (10–12).
Endotoxin is the lipopolysaccharide in the cell wall
of G-bacillus, and bacterial as well as endotoxin translocation
occur when the intestinal mucosal barrier is damaged by a variety
of stimuli, so detecting the endotoxin level in the blood
circulation can evaluate the damage to the intestinal mucosal
barrier (13). IGF-I can promote the
proliferation of intestinal epithelial cells and alleviate
endotoxemia after binding to the corresponding receptors in the
small intestinal crypt epithelial cells (14–16).
Studies have confirmed that the IGF-I level declines under stress
states such as surgical trauma (17,18). The
endotoxin level was increased compared with that before surgery in
both groups, and was increased more significantly in the glucose
solution group than that in the combined probiotics group, and
there were statistically significant differences at 1 and 3 days
after surgery between the two groups (P<0.05). The IGF-I level
was decreased in both groups and declined more significantly in the
combined probiotics group than that in the glucose solution group.
There were statistically significant differences at 1, 3 and 7 days
after surgery between the two groups. The above results indicate
that the preoperative supplement of glucose combined with
postoperative supplement of probiotics can inhibit the decline in
IGF-I, accelerate the removal of endotoxin and protect the
intestinal mucosal barrier function.
D-lactic acid is the metabolite of the innate flora
in the digestive tract, and it can be detected in the blood in case
of the increased permeability of intestinal mucosa, which may serve
as an early index reflecting the intestinal mucosal damage
(19,20). Studies on the rat model of acute
intestinal ischemia have demonstrated that the longer the duration
of ischemia is and the more serious the damage to the intestinal
mucosal barrier is, the higher the D-lactic acid level will be
(19). Besides, urinary L/M is also
a commonly-used index for clinical monitoring of intestinal mucosal
permeability (21). In this study,
the serum D-lactic acid and urinary L/M levels were increased first
and then decreased after surgery in both groups, and they declined
more obviously in the combined probiotics group than those in the
glucose solution group. Differences were statistically significant
at 7 days after surgery between the two groups (P<0.05). The
above results suggest that probiotics are beneficial in reducing
intestinal mucosal damage and permeability. Furthermore, the
intestinal flora indexes were detected. Results of quantitative PCR
revealed that the copy numbers of Bifidobacteria and
Lactobacillus were decreased after surgery in both groups
compared with those before surgery, and they declined more
remarkably in the glucose solution group than those in the combined
probiotics group. Besides, the copy numbers of Escherichia
coli and Enterococcus faecalis were increased, and they
were increased more remarkably in the glucose solution group than
those in combined probiotics group. There were statistically
significant differences between the two groups (P<0.05). The
above results indicate that the postoperative supplement of
probiotics can significantly improve the intestinal
micro-ecological environment and strengthen the intestinal mucosal
barrier function.
Previous studies have revealed that the treatment
combined with probiotics after liver transplantation and other
abdominal operations shortens the application time of antibiotics
and significantly reduces the incidence rate of infection (22). In this study, the incidence rates of
incision infection and hypoproteinemia were similar in both groups
(P>0.05). In the combined probiotics group, however, the
duration of postoperative fever and first exhaust time were
shorter, the average heart rate at 7 days after surgery was lower,
and WBC and CRP clinical indexes reflecting the systemic
inflammatory response, were improved more obviously at 7 days after
surgery, further proving that probiotics can improve the systemic
inflammatory response.
In conclusion, preoperative oral administration of
glucose solution combined with postoperative probiotics can improve
the intestinal barrier function after colorectal cancer surgery,
and benefit the recovery of early inflammatory response after
surgery.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
QX wrote the manuscript. QX and PX recorded the
general data of patients. QX, PX and YC were responsible for the
patient treatment. WL detected and analyzed the indexes. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
The Second Affiliated Hospital of Kunming Medical University
(Kunming, China) and informed consents were signed by the patients
or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bjarnason I, MacPherson A and Hollander D:
Intestinal permeability: An overview. Gastroenterology.
108:1566–1581. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yagci G, Can MF, Ozturk E, Dag B, Ozgurtas
T, Cosar A and Tufan T: Effects of preoperative carbohydrate
loading on glucose metabolism and gastric contents in patients
undergoing moderate surgery: A randomized, controlled trial.
Nutrition. 24:212–216. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Klarin B, Johansson ML, Molin G, Larsson A
and Jeppsson B: Adhesion of the probiotic bacterium
Lactobacillus plantarum 299v onto the gut mucosa in
critically ill patients: A randomised open trial. Crit Care.
9:R285–R293. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Madara JL: Maintenance of the
macromolecular barrier at cell extrusion sites in intestinal
epithelium: Physiological rearrangement of tight junctions. J Membr
Biol. 116:177–184. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Meddings JB and Swain MG: Environmental
stress-induced gastrointestinal permeability is mediated by
endogenous glucocorticoids in the rat. Gastroenterology.
119:1019–1028. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Deitch EA: The role of intestinal barrier
failure and bacterial translocation in the development of systemic
infection and multiple organ failure. Arch Surg. 125:403–404. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Söderholm JD and Perdue MH: Stress and
gastrointestinal tract. II. Stress and intestinal barrier function.
Am J Physiol Gastrointest Liver Physiol. 280:G7–G13. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Schrezenmeir J and de Vrese M: Probiotics,
prebiotics, and synbiotics - approaching a definition. Am J Clin
Nutr 73 (2 Suppl). 361S–364S. 2001. View Article : Google Scholar
|
|
10
|
Ménard S, Laharie D, Asensio C,
Vidal-Martinez T, Candalh C, Rullier A, Zerbib F, Mégraud F,
Matysiak-Budnik T and Heyman M: Bifidobacterium breve and
Streptococcus thermophilus secretion products enhance T
helper 1 immune response and intestinal barrier in mice. Exp Biol
Med (Maywood). 230:749–756. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Peña JA, Rogers AB, Ge Z, Ng V, Li SY, Fox
JG and Versalovic J: Probiotic Lactobacillus spp. diminish
Helicobacter hepaticus-induced inflammatory bowel disease in
interleukin-10-deficient mice. Infect lmmun. 73:912–920. 2005.
View Article : Google Scholar
|
|
12
|
Gaudier E, Michel C, Segain JP, Cherbut C
and Hoebler C: The VSL# 3 probiotic mixture modifies microflora but
does not heal chronic dextran-sodium sulfate-induced colitis or
reinforce the mucus barrier in mice. J Nutr. 135:2753–2761. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Buttenschoen K, Berger D, Hiki N, Strecker
W, Seidelmann M and Beger HG: Plasma concentrations of endotoxin
and antiendotoxin antibodies in patients with multiple injuries: A
prospective clinical study. Eur J Surg. 162:853–860.
1996.PubMed/NCBI
|
|
14
|
van Goudoever JB, Corpeleijn W, Riedijk M,
Schaart M, Renes I and van der Schoor S: The impact of enteral
insulin-like growth factor 1 and nutrition on gut permeability and
amino acid utilization. J Nutr. 138:1829S–1833S. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ozen S, Akisu M, Baka M, Yalaz M, Sozmen
EY, Berdeli A and Kultursay N: Insulin-like growth factor
attenuates apoptosis and mucosal damage in
hypoxia/reoxygenation-induced intestinal injury. Biol Neonate.
87:91–96. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hunninghake GW, Doerschug KC, Nymon AB,
Schmidt GA, Meyerholz DK and Ashare A: Insulin-like growth factor-1
levels contribute to the development of bacterial translocation in
sepsis. Am J Respir Crit Care Med. 182:517–525. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nygren J, Soop M, Thorell A, Efendic S,
Nair KS and Ljungqvist O: Preoperative oral carbohydrate
administration reduces postoperative insulin resistance. Clin Nutr.
17:65–71. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sukhanov S, Higashi Y, Shai SY, Vaughn C,
Mohler J, Li Y, Song YH, Titterington J and Delafontaine P: IGF-1
reduces inflammatory responses, suppresses oxidative stress, and
decreases atherosclerosis progression in ApoE-deficient mice.
Arterioscler Thromb Vasc Biol. 27:2684–2690. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sun XQ, Fu XB, Zhang R, Lu Y, Deng Q,
Jiang XG and Sheng ZY: Relationship between plasma D(−)-lactate and
intestinal damage after severe injuries in rats. World J
Gastroenterol. 7:555–558. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sheedy JR, Wettenhall RE, Scanlon D,
Gooley PR, Lewis DP, McGregor N, Stapleton DI, Butt HL and De
Meirleir KL: Increased d-lactic acid intestinal bacteria in
patients with chronic fatigue syndrome. In Vivo. 23:621–628.
2009.PubMed/NCBI
|
|
21
|
Haas V, Büning C, Buhner S, von Heymann C,
Valentini L and Lochs H: Clinical relevance of measuring colonic
permeability. Eur J Clin Invest. 39:139–144. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Akscyn RM, Franklin JL, Gavrikova TA and
Messina JL: Polytrauma-induced hepatic stress response and the
development of liver insulin resistance. Biochim Biophys Acta Mol
Basis Dis. 1863:2672–2679. 2017. View Article : Google Scholar : PubMed/NCBI
|