Introduction
An increase has been noted in the rate of detection
of small early lung cancers with recent improvements in imaging
technology such as computed tomography (CT). In particular, since
high-resolution computed tomography (HRCT) scans with low radiation
dose were first applied for lung cancer screening during the late
1990s to 2000s (1–3), there has been a marked increase in the
detection of ground-glass opacity (GGO) in peripheral lung lesions.
GGO is a non-specific finding that may be caused by various
diseases, including inflammation, fibrosis and cancer, while other
studies have reported that GGO is related to bronchioalveolar
carcinoma (BAC) (4).
Positron emission tomography (PET) with F-18
2′-deoxy-2fluoro-D-glucose (FDG) has been used to differentiate
malignant from benign lesions due to the higher metabolic activity
of malignant lesions indicated by high secondary isotope uptake.
Numerous reports are available regarding the usefulness of FDG-PET
in differentiating malignant pulmonary nodules from benign ones
(5,6). In Japan, cancer screening with whole
FDG-PET has been available for asymptomatic individuals, albeit
with a high procedure fee. Moreover, it has been reported that a
wide variety of cancer types are detectable by FDG-PET at
potentially curable stages (7–9). New
modalities such as FDG-PET combined with computed tomography
(FDG-PET/CT) are now well-established for the evaluation of various
cancer types (10–13). Clinically, PET/CT has contributed to
the evaluation of lung cancer staging, while the usefulness of
FDG-PET/CT for the differential diagnosis in small nodules showing
GGO remains controversial (14–17).
We report a noteworthy case of early lung cancer
with GGO lesions, which revealed definite intense FDG uptake during
repeated health screening with a PET/CT scan.
Patient and methods
This study was performed with the patient’s informed
consent and with approval for the study from the ethics committee
of Tokorozawa PET Diagnostic Imaging Clinic, Japan.
A 62-year-old man received health screening,
including a PET/CT scan, in September 2005 at Tokorozawa PET
Diagnostic Imaging Clinic. 18F-FDG PET/CT scans were
obtained with a Biograph Duo (Siemens CTI) as described in our
previous study (11,18). To determine semi-quantitative FDG
uptake, regions of interest (ROIs) were placed over the lesion,
including the highest uptake area (circular ROI, 1 cm in diameter),
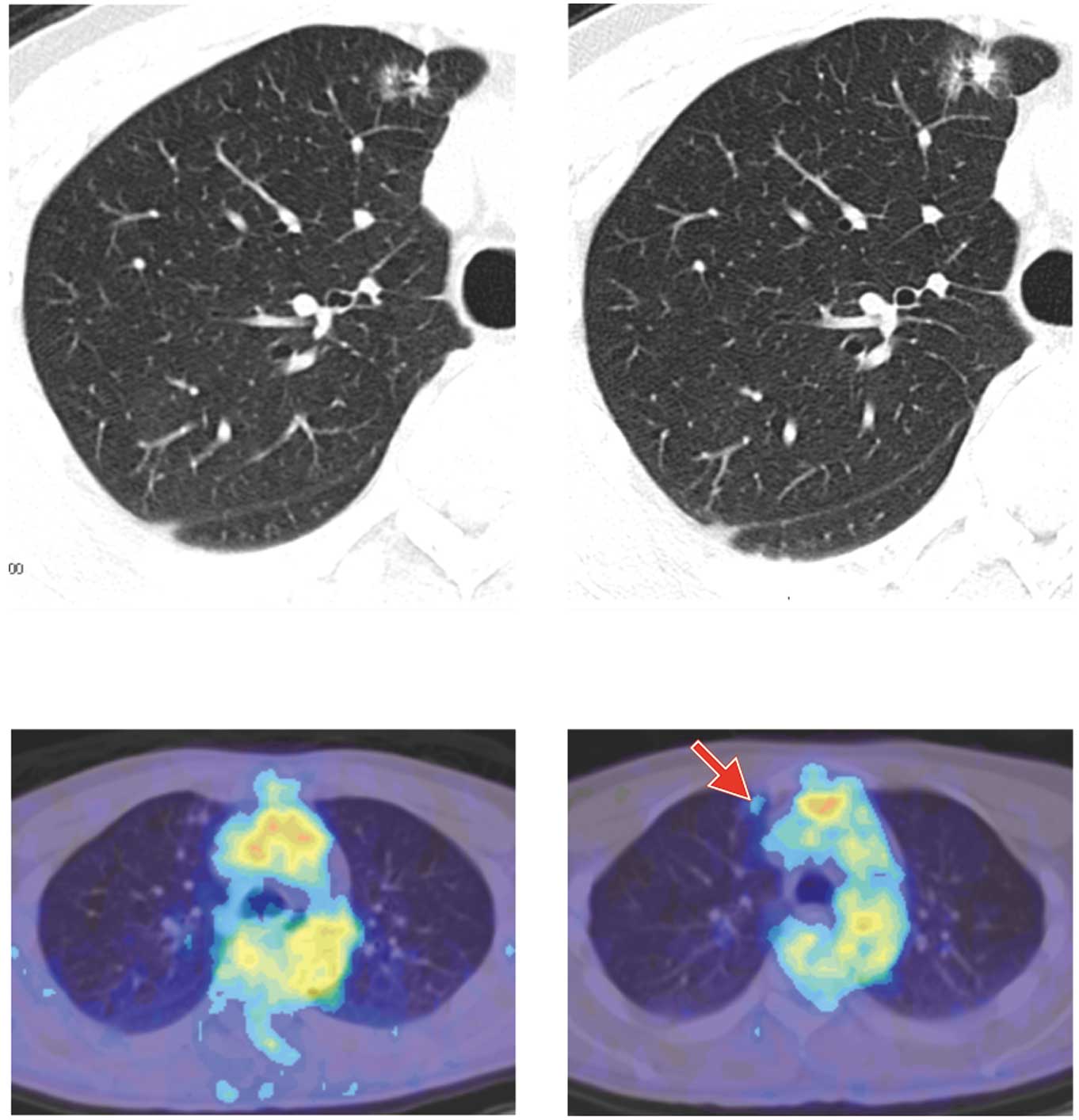
and the standardized uptake value (SUV) was calculated. The CT scan
revealed a GGO lesion (10 mm) in the upper lobe of the right lung
(Fig. 1A). PET/CT revealed no
abnormal FDG uptake in this GGO lesion (Fig. 1C), and also suggested no apparent
malignant findings in the whole body. Physical examination revealed
no apparent abnormal findings, and no abnormalities were revealed
in the blood analysis, including tumor markers such as
carcinoembryonic antigen (CEA) and CA19–9. The patient consulted a
chest surgeon but no explanatory thoracotomy was performed at the
patient’s request. Three months later, the patient received another
CT scan but no change was noted in the abnormal shadow of the right
upper lobe. A year later, he again underwent health screening with
a PET/CT scan. The CT scan revealed a larger size (15 mm) abnormal
shadow in the upper lobe of the right lung, and a small solid area
with pleural indentation was noted in the GGO lesion (Fig. 1B). PET/CT revealed abnormal FDG
uptake in this GGO lesion with SUVmax 1.2 (Fig. 1D).
Results
Explanatory thoracotomy was performed and biopsy
specimens were obtained at the National Defense Medical College
Hospital, Japan. Frozen sections of the tumor revealed a growth of
cancer cells. The patient underwent right upper lobectomy plus
dissection of the hilar and mediastinal lymph nodes.
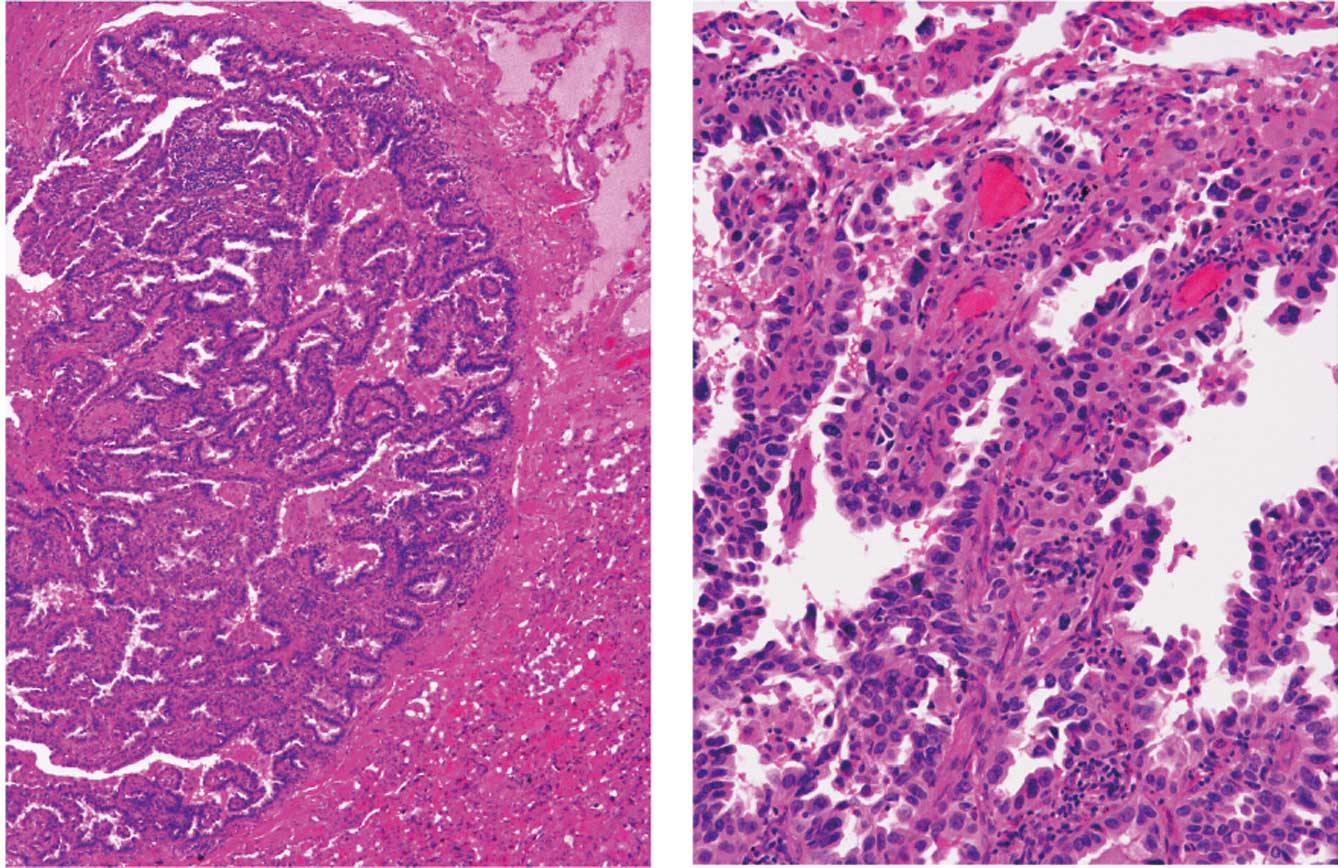
Macroscopically, the tumor in the right upper lobe measured
13×13×10 mm in diameter, and the cut surface of the tumor was solid
with a blue-white color. The microscopic findings revealed growth
of atypical cells with a glandular and papillary pattern with
fibroblastic formation, a feature of well-differentiated
adenocarcinoma (Noguchi classification type C; pT1N0MO; Fig. 2). No metastatic lesions were
observed in the dissected lymph nodes and the patient received no
chemotherapy following the surgery. Five years after thoracotomy,
PET/CT revealed no abnormalities and there were no signs of either
recurrence or systemic metastasis in any other examinations.
Discussion
Low-dose HRCT scans were first applied for lung
cancer screening between the late 1990s and early 2000s (1–3). In
their study, Henschke et al reported that CT screening
significantly reduced lung cancer mortality in a cohort of
approximately 8,000 smokers (19).
The development of FDG-PET/CT has contributed to the evaluation of
human cancer staging, and the usefulness of PET/CT is well
established for cancer staging. This imaging modality increases the
otolaryngologist’s and radiation oncologist’s confidence when
treating head and neck cancer patients, leading to appropriate
management changes (20). We have
reported that this modality was clinically useful for evaluating
human cancers, including rare carcinoma cases (18,21–23).
In the present study, we reported a lung cancer case with GGO,
which revealed an increased intense FDG uptake by FDG-PET/CT during
annual cancer screening, and the repeated FDG-PET/CT examinations
were used to evaluate the pulmonary nodules with GGO.
In lung cancer screening with low-dose HRCT, there
has been a marked increase in the detection of GGO in peripheral
lung lesions. Computer-aided diagnosis (CAD) systems provide a
useful second opinion in detecting pulmonary nodules when
physicians carry out lung cancer screening with low-dose HRCT
(24). Certain reports indicate
that CT findings on GGO with a solid area are useful in
differentiating between benign and malignant lesions (25). In our case, the CT scan revealed
that the pulmonary lesion with GGO had a slightly increased size
with a solid area after a one year interval between screenings.
In Japan, cancer screening with whole FDG-PET has
been available for use in asymptomatic individuals, albeit with
high procedure fees, and it has been reported that a wide variety
of cancer types are detectable by FDG-PET at potentially curable
stages (7–9). Murano et al reported that
FDG-PET cancer screening was beneficial to patients above the
break-even age despite the exposure to radiation (26). In our PET center, we performed
cancer screening by PET/CT with informed consent including that for
radiation exposure, and 140 cases of cancer were detected by PET/CT
and other modalities among 7,236 examinations in a period of
approximately 5 years and 7 months between August 2005 and March
2011. A total of 140 cancer patients were pathologically diagnosed
as having various cancers: 33 lung, 17 thyroid, 17 breast, 11 colon
and 62 other cancer types, whereas PET/CT revealed no significant
FDG uptake in 22 of the 140 patients. The total detection rate was
1.93%, and the detection rate with PET/CT was 1.55%.
In this study, we have reported a rare case of early
lung cancer with GGO lesions. The patient underwent thoracotomy and
at present is without recurrence. Thus, intense FDG uptake during
an annual follow-up repeated health screening with FDG-PET/CT may
prove useful in detecting such cancer types.
Acknowledgements
The authors are grateful to Mr. Kenji Kawai for his
technical assistance.
References
|
1
|
Kaneko M, Eguchi K, Ohmatsu H, Kakinuma R,
Naruke T, Suemasu K and Moriyama N: Peripheral lung cancer:
screening and detection with low-dose spiral CT versus radiography.
Radiology. 201:798–802. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Abe Y, Hanai K, Nakano M, Ohkubo Y,
Hashizume T, Kakizaki T, Nakamura M, Niki N, Egichi K, Fujino T and
Moriyama N: A computer-aided diagnosis (CAD) system in lung cancer
screening with computed tomography. Anticancer Res. 25:483–488.
2005.PubMed/NCBI
|
|
3
|
Abe Y, Nakamura M, Ozeki Y, Machida K and
Ogata T: Lung cancer: Low-dose helical computed tomography. Cancer
Imaging: Lung and Breast Carcinoma. 1. Hayat MA: Elsevier; Academic
Press; pp. 203–207. 2007
|
|
4
|
Nakata M, Saeki H, Takata I, Segawa Y,
Mogami H, Mandai K and Eguchi K: Focal ground-glass opacity
detected by low-dose helical CT. Chest. 121:1464–1467. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gould MK, Maclean CC, Kuschner WG, Rydzak
CE and Owens DK: Accuracy of positron emission tomography for
diagnosis of pulmonary nodules and mass lesions: a meta-analysis.
JAMA. 285:914–924. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kim SK, Allen-Auerbach M, Goldin J, Fueger
BJ, Dahlbom M, Brown M, Czernin J and Schiepers C: Accuracy of
PET/CT in characterization of solitary pulmonary lesions. J Nucl
Med. 48:214–220. 2007.PubMed/NCBI
|
|
7
|
Yasuda S and Shohtsu A: Cancer screening
with whole-body 18F-fluorodeoxyglucose positron-emission
tomography. Lancet. 350:18191997. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yasuda S, Ide M, Fujii H, Nakahara T,
Mochizuki Y, Takahashi W and Shohtsu A: Application of positron
emission tomography imaging to cancer screening. Br J Cancer.
83:1607–1611. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ide M: Cancer screening with FDG-PET. Q J
Nucl Med Mol Imaging. 50:23–27. 2006.PubMed/NCBI
|
|
10
|
Cronin CG, Swords R, Truong MT,
Viswanathan C, Rohren E, Giles FJ, O’Dwyer M and Bruzzi JF:
Clinical utility of PET/CT in lymphoma. AJR Am J Roentgenol.
194:W91–W103. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ueda S, Saeki T, Tsuda H, Shigekawa T,
Omata J, Moriya T, Yamamoto J, Osaki A, Fujiuchi N, Misumi M, et
al: 18F-fluorodeoxyglucose positron emission tomography optimizes
neoadjuvant chemotherapy for primary breast cancer to achieve
pathological complete response. Int J Clin Oncol. 2011.(E-pub ahead
of print).
|
|
12
|
Xie L, Saynak M, Veeramachaneni NK, Fried
DV, Jagtap MR, Chiu WK, Higginson DS, Lawrence MV, Khandani AH,
Qaqish BF, Chen RC and Marks LB: Non-small cell lung cancer:
Prognostic importance of positive FDG PET findings in the
mediastinum for patients with N0-1 disease at pathologic analysis.
Radiology. 2011.(E-pub ahead of print).
|
|
13
|
Abe Y, Tamura K, Sakata I, Ishida J, Ozeki
Y, Tamura A, Uematsu K, Sakai H, Goya T, Kanazawa M and Machida K:
Clinical implications of 18F-fluorodeoxyglucose positron
emission tomography/computed tomography (18F-FDG PET/CT)
at delayed phase for diagnosis and prognosis of malignant pleural
mesothelioma. Oncol Rep. 2011 Oct 24; View Article : Google Scholar : (Epub ahead of
print).
|
|
14
|
Chun EJ, Lee HJ, Kang WJ, Kim KG, Goo JM,
Park CM and Lee CH: Differentiation between malignancy and
inflammation in pulmonary ground-glass nodules: the feasibility of
integrated (18)F-FDG PET/CT. Lung Cancer. 65:180–186. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fischer B, Lassen U, Mortensen J, Larsen
S, Loft A, Bertelsen A, Ravn J, Clementsen P, Høgholm A, Larsen K,
et al: Preoperative staging of lung cancer with combined PET-CT. N
Engl J Med. 361:32–39. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cloran FJ, Banks KP, Song WS, Kim and
Bradley YC: Limitations of dual time point PET in the assessment of
lung nodules with low FDG avidity. Lung Cancer. 68:66–71. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fischer BM, Lassen U and Højgaard L:
PET-CT in preoperative staging of lung cancer. N Engl J Med.
364:980–981. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Abe Y, Tamura K, Sakata I, Ishida J,
Fukuba I, Matsuoka R, Shimizu S, Murakami H and Machida K:
Usefulness of 18F-FDG positron emission
tomography/computed tomography for the diagnosis of
pyothorax-associated lymphoma: A report of three cases. Oncol Lett.
1:833–836. 2010.
|
|
19
|
Henschke CI, Boffetta P, Gorlova O, Yip R,
Delancey JO and Foy M: Assessment of lung-cancer mortality
reduction from CT screening. Lung Cancer. 71:328–332. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Fleming AJ Jr and Johansen ME: The
clinician’s expectations from the use of positron emission
tomography/computed tomography scanning in untreated and treated
head and neck cancer patients. Curr Opin Otolaryngol Head Neck
Surg. 16:127–134. 2008.
|
|
21
|
Ueda S, Tsuda H, Asakawa H, Shigekawa T,
Fukatsu K, Kondo N, Yamamoto M, Hama Y, Tamura K, Ishida J, Abe Y
and Mochizuki H: Clinicopathological and prognostic relevance of
uptake level using 18F-fluorodeoxyglucose positron emission
tomography computed tomography fusion imaging (18F-FDG PET/CT) in
primary breast cancer. Jpn J Clin Oncol. 38:250–258. 2008.
View Article : Google Scholar
|
|
22
|
Abe Y, Tamura K, Sakata I, Ishida J, Mukai
M, Ohtaki M, Nakamura M and Machida K: Unique intense uptake
demonstrated by 18F-FDG positron emission
tomography/computed tomography (PET/CT) in primary pancreatic
lymphoma: A case report. Oncol Lett. 1:605–607. 2010.PubMed/NCBI
|
|
23
|
Ozeki Y, Abe Y, Kita H, Tamura K, Sakata
I, Ishida J and Machida K: A case of primary lung cancer lesion
demonstrated by F-18 FDG positron emission tomography/computed
tomography (PET/CT) one year after the detection of metastatic
brain tumor. Oncol Lett. 2:621–623. 2011.PubMed/NCBI
|
|
24
|
Abe Y, Tamura T, Sakata I, Ishida J,
Nagata M, Machida K and Ogata T: Lung cancer: Computer-aided
diagnosis with computed tomography. Cancer Imaging: Lung and Breast
Carcinoma. 1. Hayat MA: Elsevier; Academic Press; pp. 209–214.
2007
|
|
25
|
Suzuki K, Kusumoto M, Watanabe S, Tsuchiya
R and Asamura H: Radiologic classification of small adenocarcinoma
of the lung: radiologic-pathologic correlation and its prognostic
impact. Ann Thorac Surg. 81:413–419. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Murano T, Minamimoto R, Senda M, Uno K,
Jinnouchi S, Fukuda H, Iinuma T, Tsukamoto E, Terauchi T, Yoshida
T, et al: Radiation exposure and risk-benefit analysis in cancer
screening using FDG-PET: results of a Japanese nationwide survey.
Ann Nucl Med. 2011.(E-pub ahead of print).
|