Introduction
Partial nephrectomy (PN) is emerging as a
nephron-sparing surgery (NSS) in the management of select renal
tumours, including benign renal tumours, renal tumours in an
anatomically or functionally solitary kidney, renal tumours with
potential renal function of the opposite kidney and small renal
tumours (T1a and T1b) when the contralateral kidney is normal
(1). PN is a technically more
complex surgery than radical nephrectomy (RN) and has been shown to
be associated with a slightly higher rate of complications
(2–4). Ureteral obstruction as a result of
surgery is rare and most cases are transient.
The study was approved by the ethics committee of
the First Affiliated Hospital, School of Medicine, Zhejiang
University, Zhejiang, China. Informed consent was obtained from the
patient.
Case report
A 64-year-old female who had undergone PN in 2011 in
The First Affiliated Hospital, Zhejiang University, Zhejiang, China
for treatment of a tumour in the left kidney was admitted in
February 2011 after 20 days of moderate left lower back pain.
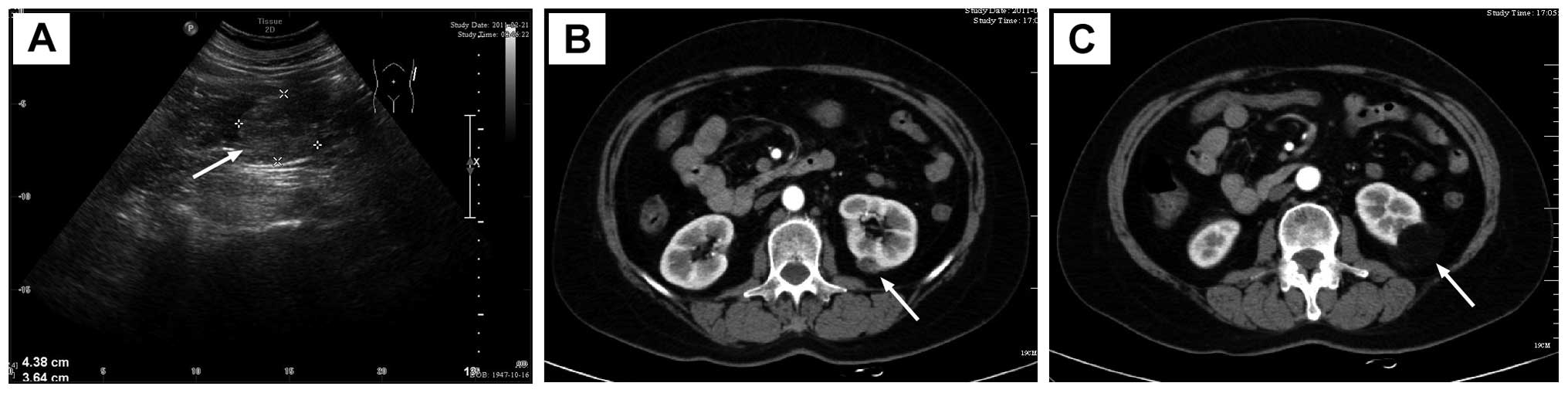
Imaging revealed two renal masses in the lower pole of the left
kidney (Fig. 1). Following
appropriate preoperative preparation, open PN was performed and the
two masses were resected. The collection system was not opened
during the surgery and the wounds were carefully closed with
absorbable sutures. The wounds of the kidney were covered with
perirenal fat and fibrin glue was used to adhere the fat to the
kidney. The wounds were carefully sutured and a temporary drainage
tube was placed near the left kidney. Pathological examination of
surgical specimens revealed renal angiomyolipoma. The drainage tube
was removed on the 5th postoperative day. The patient recovered
completely and was discharged on the 7th postoperative day.
However, the patient was re-admitted on the 14th
postoperative day due to the discharge of increasingly milky, thin,
odourless fluid every day from the unclosed external orifice of the
drainage tube. The amount of fluid reached 800 ml on the second day
after re-admission. The creatinine concentrations of the fluid and
urine were 1847 and 4640 μmol/l, respectively. The result of
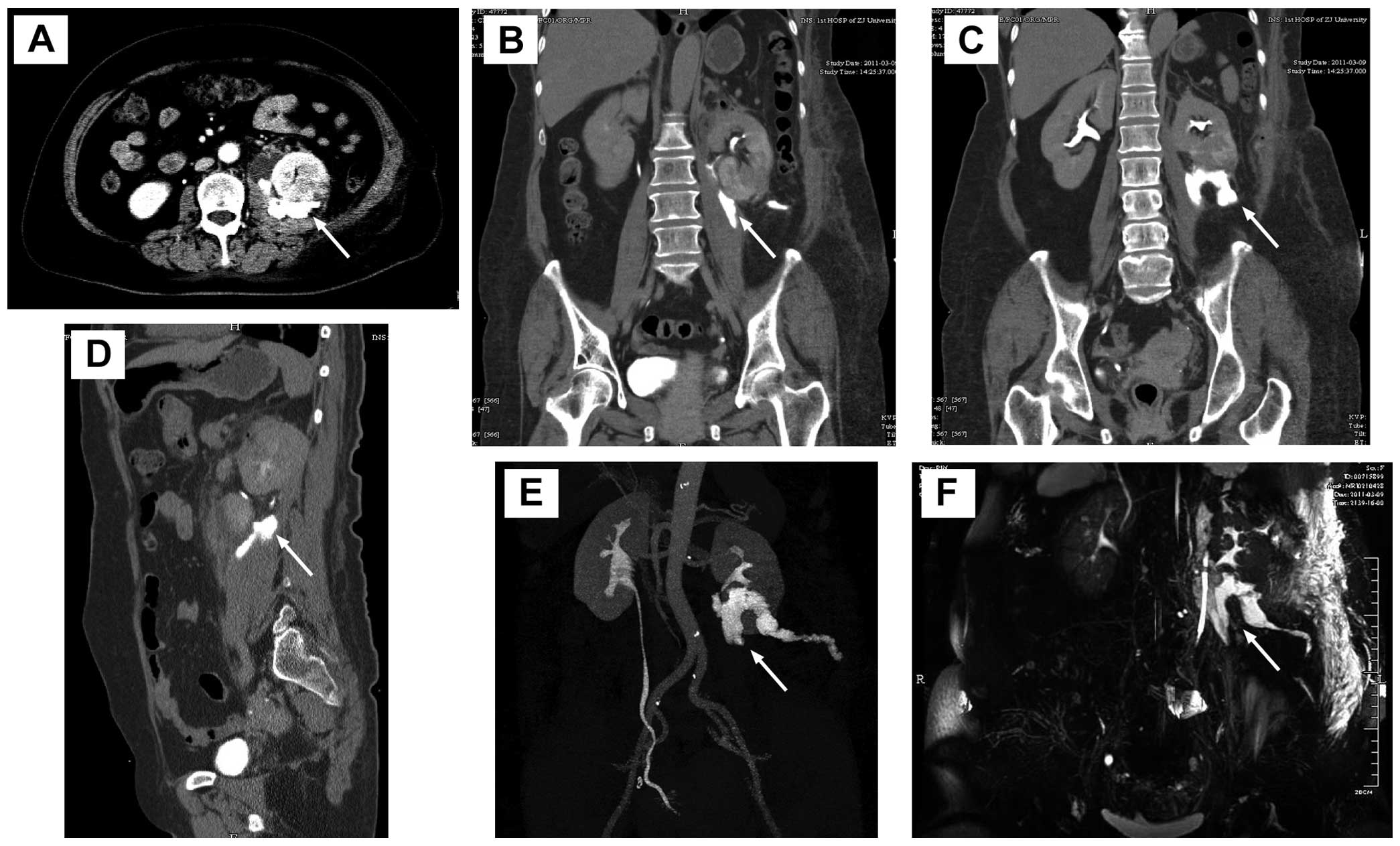
qualitative analysis of chyle was negative. CT urography (Fig. 2A–E) revealed a clear renal
collecting system and no significant hydronephrosis. However,
contrast remained in the left kidney and upper ureter and leakage
in the perirenal space and along the psoas muscle, and was drained
out of the body through the drainage tube. Moreover, no contrast
agent was observed in the middle and lower ureter. In MR urography
images (Fig. 2F), there was fluid
signal in the perirenal space, particularly inside and below the
left kidney. The results of CT and MR urography revealed left
urinary fistula. A 5-F ureteral catheter was inserted into the left
ureter for retrograde pyelography and elevated ∼20 cm but did not
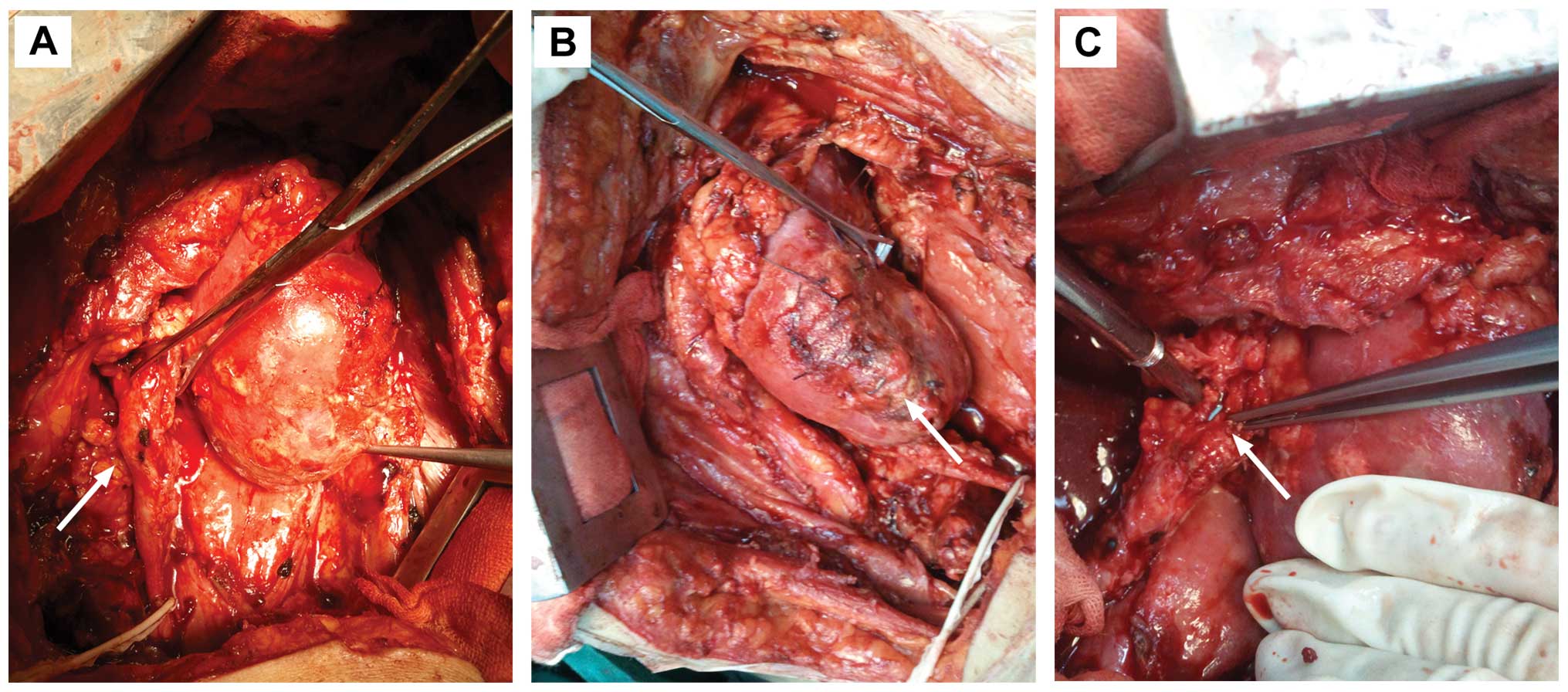
pass to the left renal pelvis. Then reoperation was performed on
the 16th postoperative day to explore the left kidney and ureter in
order to relieve the obstruction, allow unobstructed drainage and
save renal function (Fig. 3).
During the reoperation, almost complete occlusion of ureteral
stricture was found in the upper ureter 5 cm from the left
ureteropelvic junction. The ureter near the stricture was enfolded
by fibrin glue and exhibited marked stiffness and adhesion. The
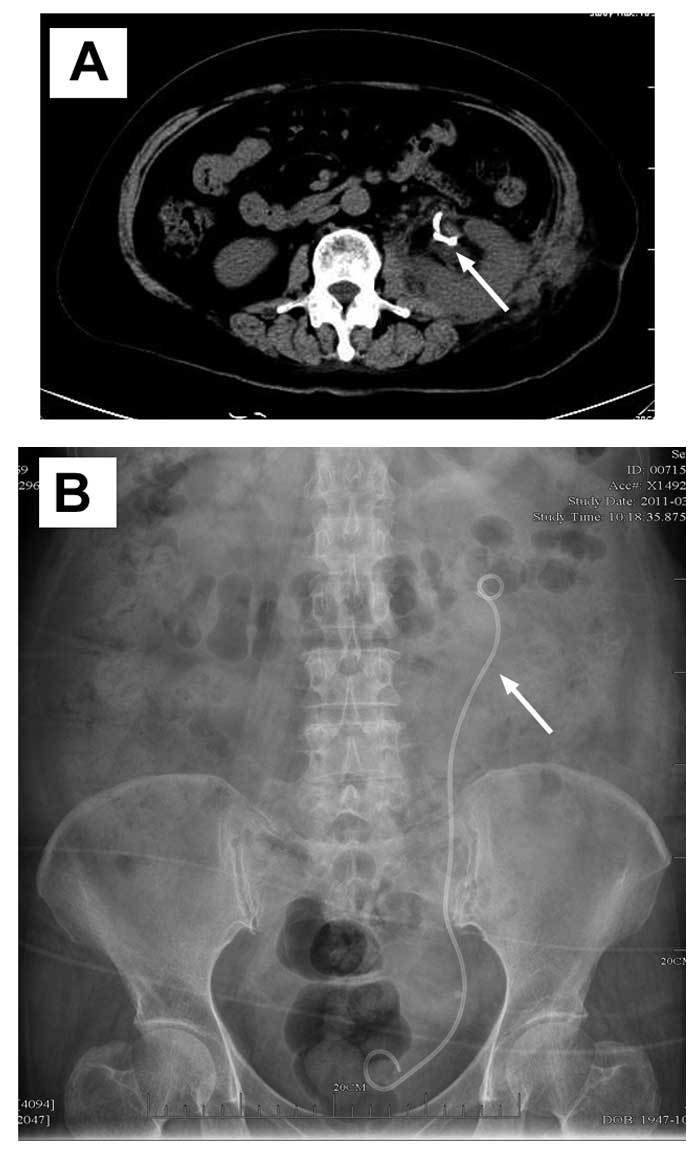
lesion of the ureter was resected and the ureter was anastomosed
end to end with the routine double-J stent (Fig. 4). Pathological examination of
surgical specimens revealed fat fibrous scar tissue hyperplasia
with inflammatory cell infiltration. The double-J tube was removed
by cystoscopy two months after the second surgery. The patient
recovered completely without exudate.
Discussion
PN was first reported in 1884 by Wells for removing
two solid circum renal tumours (5).
In 1887, Czerny (6) employed the
first PN for renal cell cancer (RCC) in a patient with a solitary
kidney. Since then, PN has been performed to manage numerous
urological diseases, including kidney injuries, renal tumours,
renal tuberculosis and partial hydronephrosis. However, its
application was limited for postoperative complications until
Vermooten (7) demonstrated that PN
was oncologically safe for early tumours confined to the kidney and
suggested that it should also be used in patients with a healthy
contralateral kidney in 1950. Since the early 1990s, PN has been
performed mainly as an alternative to RN for small renal tumours
(8–11). With the improvement of laparoscopic
techniques, laparoscopic RN was gradually established and has
become an alternative to open surgery over the last 10 years
(12–14). At present, PN is becoming a standard
therapy for renal tumours <4 cm in size in a number of centres
and is an important therapy for larger T1 tumours (15).
Standard indications for PN are divided into the
following categories: absolute, relative and elective indications.
PN is absolutely indicated for patients with an anatomically or
functionally solitary kidney due to unilateral renal agenesis,
previous contralateral nephrectomy or irreversible impairment of
contralateral renal function for a benign disorder (16). Relative indications for PN include
medical conditions that may impair renal function in the future,
such as renal calculus disease, chronic and recurrent
pyelonephritis, vesicoureteral reflux disease, renal artery
stenosis, hypertension and diabetes mellitus. PN is electively
indicated for patients with localised unilateral renal tumours and
a healthy contralateral kidney.
It is generally acknowledged that PN has a higher
overall complication rate than RN (17). The complications of PN are
classified as intraoperative or postoperative. According to
previously established criteria (18), intraoperative complications include
massive haemorrhage, significant injury to an adjacent organ such
as a major vessel, the liver, ureter or pleura, conversion to RN
and renal loss. Postoperative complications of PN are classified as
urological (such as haemorrhage, urinary leakage/fistula,
infection, renal dysfunction, vascular fistula or malformation,
positive margin, local recurrence, renal infarct and renal loss)
and nonurological (such as cardiac, gastrointestinal, pulmonary,
thromboembolic, incisional or other). Postoperative urinary leakage
is defined as drainage of >50 ml daily for more than 1 week with
fluid biochemistry compatible with urine (19). Urinary leakage persisting for more
than 4 weeks after the surgical procedure is generally defined as
urinary fistula following PN. Urinary leakage was one of the most
common complications of PN. The frequency of urinary leakage
occurrence varies between 0.7 and 17.4% in PN (20). Polascik et al found that
urinary leakage occurred in 21.4% (6 of 28) cases of PN in their
earlier surgery, but 0% (0 of 39) cases in their later surgery
after the employment of routine injection of the collecting system
with dilute methylene blue to identify small defects in the
anastomosis (11). Lowrance et
al considered that urinary leakage was the most notable
difference between the PN and RN complications (17). Stephenson et al
comprehensively reviewed complications of PN and RN in a cohort of
1,049 patients treated at a single centre between 1995 and 2002
(3). In total, 66% of patients in
the cohort underwent RN and the remaining 34% underwent PN. The
complication rates of urinary fistula were 5.5% for PN and 60.6%
(20/33) for all complications associated with PN.
Postoperative urinary leakage occurs due to untight
closure of the renal collecting system, ureteral injury or
obstruction. Regardless of the cause, any duration of postoperative
urinary leakage must be appropriately managed as early as possible.
Nonoperative treatment of effective drainage, prevention of
infection and avoidance of ureteral obstruction generally resolve
the urinary leakage. However, a precondition of nonoperative
treatment is no ureteral obstruction. If ureteral obstruction
already exists, double-J stenting is required to reasonably save
ipsilateral renal function. In the present case, there was
discharge of 800 ml of milky, thin, odourless fluid every day from
the unclosed external orifice of a drainage tube at 2 weeks after
the first surgery. The creatinine concentration of the fluid was
almost half of that of urine, but significantly higher than that of
serum. The fluid was milky and negative for qualitative analysis of
chyle. The results of imaging such as CT and MR urography revealed
left urinary fistula. The results of retrograde pyelography made
clear that there was proximal ureteral obstruction. Under the
circumstances, we considered there was ureteral obstruction and
urinary fistula in the left proximal ureter.
Van Poppel et al compared the complications
of PN and RN and found that reoperations for complications were
necessary in 4.4% of the PN group (4). It is generally believed that urinary
leakage rarely requires repeat surgery, but in cases of persistent
ureteral obstruction and failed ureteral catheterisation, a
reoperation may be necessary to relieve obstruction. In most cases,
reoperation for urinary leakage results in renal loss. Ramani et
al(21) performed 200
laparoscopic PNs and only 9 (4.5%) patients had urinary leakage,
none of whom required reoperation. Six (3%) required double-J
stenting and 2 (1%) required double-J stenting with CT-guided
drainage. Meeks et al(22)
retrospectively reviewed 127 consecutive patients who underwent PN
and found that 21 patients (16.5%) experienced a urinary leakage
following PN. Most urinary leakages were resolved with prolonged
drainage and no surgical reexplorations were required, but 8
patients required a ureteric stent and 2 patients needed
percutaneous nephrostomy. In the present case, urinary leakage
lasted 2 weeks. Based on imaging findings we considered there was
ureteral obstruction and urinary fistula in the left proximal
ureter. We performed the reoperation on the 16th postoperative day
to explore the left kidney and ureter. The left proximal ureter was
found to be enfolded by fibrin glue which was used to adhere the
fat and kidney wound in the first surgery. Following surgical
reconstruction, the patient recovered completely.
Fibrin glue is a mixture of concentrated autologous
fibrinogen and bovine-derived thrombin, which is used to achieve
haemostasis during PN (23). Fibrin
glue is known for its ability to stop venous oozing from the cut
surface of renal parenchymal tissue. It also facilitates
haemostatic control as it reproduces the final steps of the
coagulation cascade (24). Since
haemorrhage is one of the most common complications of PN, fibrin
glue is commonly used in open (25,26)
and laparoscopic PN (27–29) and fibrin glue-associated
complications have not been reported. However, we report unexpected
ureteral obstruction and urinary fistula due to fibrin glue.
Therefore, we suggest that care must be taken to ensure that the
ureter is not in contact with the fibrin glue during PN
surgery.
In conclusion, we report fibrin glue-associated
ureteral obstruction and urinary fistula following PN. Fibrin glue
is commonly used in PN and fibrin glue-associated complication is
rare. Therefore, we suggest that the surgeon should take
precautions to avoid contact between the ureter with fibrin glue
during surgery.
Abbreviations:
|
PN
|
partial nephrectomy;
|
|
NSS
|
nephron-sparing surgery;
|
|
RN
|
radical nephrectomy
|
Acknowledgements
The present study was supported by the
National Natural Science Foundation of China (No. 30901499) and the
Zhejiang Provincial Natural Science Foundation of China (No.
Y12H160085).
References
|
1
|
Ljungberg B, Cowan NC, Hanbury DC, et al
European Association of Urology Guideline Group: EAU guidelines on
renal cell carcinoma: the 2010 update. Eur Urol. 58:398–406. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lesage K, Joniau S, Fransis K and Van
Poppel H: Comparison between open partial and radical nephrectomy
for renal tumours: perioperative outcome and health-related quality
of life. Eur Urol. 51:614–620. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Stephenson AJ, Hakimi AA, Snyder ME and
Russo P: Complications of radical and partial nephrectomy in a
large contemporary cohort. J Urol. 171:130–134. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Van Poppel H, Da Pozzo L, Albrecht W, et
al European Organization for Research and Treatment of Cancer
(EORTC); National Cancer Institute of Canada Clinical Trials Group
(NCIC CTG); Southwest Oncology Group (SWOG); Eastern Cooperative
Oncology Group (ECOG): A prospective randomized EORTC intergroup
phase 3 study comparing the complications of elective
nephron-sparing surgery and radical nephrectomy for low-stage renal
cell carcinoma. Eur Urol. 51:1606–1615. 2007.
|
|
5
|
Wells S: Successful Removal of Two Solid
Circum Renal Tumours. Br Med J. 1:7581884. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Czerny H: About Nephrectomy. Beitr 2 Klin
Chir. 6:4851890.(In German).
|
|
7
|
Vermooten V: Indications for conservative
surgery in certain renal tumors: a study based on the growth
pattern of the cell carcinoma. J Urol. 64:200–208. 1950.PubMed/NCBI
|
|
8
|
Herr HW: Partial nephrectomy for
unilateral renal carcinoma and a normal contralateral kidney:
10-year followup. J Urol. 161:33–34; discussion 34–35, 1999.
|
|
9
|
Provet J, Tessler A, Brown J, Golimbu M,
Bosniak M and Morales P: Partial nephrectomy for renal cell
carcinoma: indications, results and implications. J Urol.
145:472–476. 1991.PubMed/NCBI
|
|
10
|
Van Poppel H, Bamelis B, Oyen R and Baert
L: Partial nephrectomy for renal cell carcinoma can achieve
long-term tumor control. J Urol. 160:674–678. 1998.PubMed/NCBI
|
|
11
|
Polascik TJ, Pound CR, Meng MV, Partin AW
and Marshall FF: Partial nephrectomy: technique, complications and
pathological findings. J Urol. 154:1312–1318. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gill IS, Schweizer D, Hobart MG, Sung GT,
Klein EA and Novick AC: Retroperitoneal laparoscopic radical
nephrectomy: the Cleveland clinic experience. J Urol.
163:1665–1670. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Allan JD, Tolley DA, Kaouk JH, Novick AC
and Gill IS: Laparoscopic radical nephrectomy. Eur Urol. 40:17–23.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Berger A, Brandina R, Atalla MA, et al:
Laparoscopic radical nephrectomy for renal cell carcinoma:
oncological outcomes at 10 years or more. J Urol. 182:2172–2176.
2009.PubMed/NCBI
|
|
15
|
Patard JJ, Shvarts O, Lam JS, et al:
Safety and efficacy of partial nephrectomy for all T1 tumors based
on an international multi-center experience. J Urol. 171:2181–2185;
quiz 2435, 2004.
|
|
16
|
Uzzo RG and Novick AC: Nephron sparing
surgery for renal tumors: indications, techniques and outcomes. J
Urol. 166:6–18. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lowrance WT, Yee DS, Savage C, et al:
Complications after radical and partial nephrectomy as a function
of age. J Urol. 183:1725–1730. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Campbell SC, Novick AC, Streem SB, Klein E
and Licht M: Complications of nephron sparing surgery for renal
tumors. J Urol. 151:1177–1180. 1994.PubMed/NCBI
|
|
19
|
Gill IS, Kavoussi LR, Lane BR, et al:
Comparison of 1,800 laparoscopic and open partial nephrectomies for
single renal tumors. J Urol. 178:41–46. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Porpiglia F, Volpe A, Billia M and Scarpa
RM: Laparoscopic versus open partial nephrectomy: analysis of the
current literature. Eur Urol. 53:732–742; discussion 742–743,
2008.
|
|
21
|
Ramani AP, Desai MM, Steinberg AP, et al:
Complications of laparoscopic partial nephrectomy in 200 cases. J
Urol. 173:42–47. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Meeks JJ, Zhao LC, Navai N, Perry KT Jr,
Nadler RB and Smith ND: Risk factors and management of urine leaks
after partial nephrectomy. J Urol. 180:2375–2378. 2008. View Article : Google Scholar
|
|
23
|
Levinson AK, Swanson DA, Johnson DE,
Greskovich FJ III, Stephenson RA and Lichtiger B: Fibrin glue for
partial nephrectomy. Urology. 38:314–316. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hoznek A, Salomon L, Antiphon P, et al:
Partial nephrectomy with retroperitoneal laparoscopy. J Urol.
162:1922–1926. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Scott R, Meddings RN and Buckley JF: Use
of fibrin glue for partial nephrectomy. Urology. 39:5891992.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Dalpiaz O, Neururer R, Bartsch G and
Peschel R: Haemostatic sealants in nephron-sparing surgery: what
surgeons need to know. BJU Int. 102:1502–1508. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Schips L, Dalpiaz O, Cestari A, et al:
Autologous fibrin glue using the Vivostat system for hemostasis in
laparoscopic partial nephrectomy. Eur Urol. 50:801–805. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Msezane LP, Katz MH, Gofrit ON, Shalhav AL
and Zorn KC: Hemostatic agents and instruments in laparoscopic
renal surgery. J Endourol. 22:403–408. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Galanakis I, Vasdev N and Soomro N: A
review of current hemostatic agents and tissue sealants used in
laparoscopic partial nephrectomy. Rev Urol. 13:131–138.
2011.PubMed/NCBI
|