Introduction
Gastric cancer is the fifth most common cancer and
the third leading cause of cancer mortality worldwide (1). Surgery alone is no longer acceptable
as a standard treatment for resectable gastric cancer (2). Optimal locoregional treatment for
gastric cancer can be achieved by a combination of radical surgery
with individualized neoadjuvant or adjuvant treatment, with modern
3D radiotherapy and optimum target therapy (3). Many clinical trials showed that
although chemotherapy and target therapy are effective in
short-term treatment for advanced gastric cancer (4–6), these
treatments do not improve overall survival (OS) rate (<1 year).
Thus, sensitive validated biomarkers for early detection of the
tumor and a more accurate prediction of disease outcome as well as
patient response to treatments can significantly improve efficacy
of the treatments and greatly decrease the mortality of gastric
cancer.
Sphingosine-1-phosphate (S1P) has been
identified to play an important regulatory role in proliferation,
inflammation, vasculogenesis and anti-apoptosis (7). Sphingosine-1-phosphate phosphatase 1
(SGPP1), which is intracellularly localized on endoplasmic
reticulum (ER), is responsible for converting S1P to
sphingosine (8). SGPP1 is
located in the region 14q23.2 of the chromosome (9). Furthermore, overexpression of SGPP1
may elevate ceramide levels and induce apoptosis, whereas knockdown
of SGPP1 enhanced resistance to TNF-α, the chemotherapeutic
agent daunorubicin (8) and
radiotherapy (10).
In the present study, we aimed to examine the
possible role of SGPP1 in the progression of gastric cancer and
determine whether SGPP1 may serve as a prognostic biomarker.
Materials and methods
Materials
Human gastric cancer cell lines, AGS and HGC27 were
obtained from the European Collection of Cell Cultures, (ECACC;
Salisbury, UK). Reagents and kits were obtained from Promega
Corporation (Madison, WI, USA) and Gibco Invitrogen Corporation
(Paisley, Scotland, UK). Anti-SGPP1 antibody (Santa Cruz
Biotechnology, Inc., Santa Cruz, CA, USA), TRI reagent
(Sigma-Aldrich, Poole, UK), Universal Z Probe (TCS Biologicals
Ltd., Oxford, UK), and the DC Protein Assay kit (Bio-Rad, Hemel
Hempstead, UK) were also used in the present study.
Gastric tissues
Gastric adenocarcinoma or Siewert type III
gastroesophageal junction (GEJ) adenocarcinoma tissues (282 of
paraffin-embedded tissues and 218 of fresh-frozen tissues), along
with matched normal tissue from the same patients, were collected
immediately after surgical resection at the Beijing Cancer Hospital
and were stored in the Tissue Bank of Peking University Oncology
School. Clinicopathological factors, including age, gender,
histological type, Lauren type, tumor location, vascular invasion,
TNM stage and lymph node metastasis, were recorded and stored in
the patients' database. All protocols were reviewed and approved by
the Local Ethics Committee. Informed consent was obtained from the
patients before therapy.
The gastric tissues used in the present study were
obtained from gastric cancer patients with cT2-4N0M0 or cT1-4N1-3M0
treated between January, 2003 and December, 2011. Gastrectomy with
D2 lymphadenectomy was performed and no treatment was conducted
before the surgery. Primary tumor site, grade, depth of tumor
invasion, status of lymph node metastasis, distant metastasis and
TNM stage were recorded in histopathology reports. Pathological
stage was determined according to the seventh edition of the TNM
staging system recommended by the International Union against
Cancer.
Immunohistochemistry (IHC)
Sections (4 mm) obtained from formalin-fixed,
paraffin-embedded tissues were mounted on poly-L-lysine-coated
slides and then deparaffinised in xylene and rehydrated through
alcohol to distilled water. Endogenous peroxidase activity was
blocked with 3% hydrogen peroxide for 15 min at room temperature.
After pressure cooking the slides in 10 mmol/l EDTA (pH 8.0) for 3
min, the sections were incubated with 5% goat serum, then incubated
overnight at 4°C with SGPP1 antibody (1:200; Santa Cruz
Biotechnology, Inc.) and without the primary antibody as a negative
control. Primary antibodies were detected using a two-step EnVision
system (Dako, Glostrup, Denmark). Horseradish peroxidase and
diaminobenzedene hydrochloride were the enzyme and chromogen used,
respectively. Staining score was independently assessed by two
pathologists. The percentage of positive cells and the intensity of
cytoplasmic staining were analyzed. Thus all final scoring
estimations were stratified as follows: −, 0% of stained cells; +,
<20% weakly to moderately stained cells; ++, 10–20% intensively
stained cells and 20–50% weakly stained cells; and +++, 20–50%
positive cells with moderate-to-marked staining or >50% positive
cells. There was a low level of discrepancy (<5% cases) among
the pathologists in terms of scoring, but a consensus was reached
after joint review.
RNA isolation and RT-PCR
Total RNA was isolated from the homogenized gastric
tissues and cell lines using the Total RNA Isolation reagent (TRI
reagent; Sigma-Aldrich). Synthesis of cDNA and subsequent PCR were
performed as previously described (11). SGPP1 primers used were:
sense, 5′-GGGCAACGAACTCTTCTAC-3′ and antisense, 5′-TCC
AGGTGTCAAGAGTGAA-3′.
Quantitative RT-PCR
The level of SGPP1 transcripts was
quantitatively analyzed with the iCycler iQ5 system with qPCR
Master Mix (both from Bio-Rad) as previously described (12). SGPP1 primers designed using
the Beacon Design software (Premier Biosoft, Palo Alto, CA, USA)
were as follows: sense, 5′-ATGGACAAGCATCCCTTCC-3′ and antisense,
5′- ACTGAACCTGACCGTACA
CTCTGTCAGGGAAATACCAA3-3′. The underlined sequence in the reverse
primers was the additional Z sequence, which is complementary to
the Universal Z Probe (TCS Biologicals Ltd., Oxford, UK). Internal
standard GAPDH primer sequences used were: sense,
5′-CTGAGTACGTCGTGGAGTCC-3′ and antisense, 5′- ACTGAACCTGACCGTACA
GAGATGATGACCCTTTTG-3′. To exclude the effect of tissue
heterogeneity, the SGPP1 quantification was normalized
against the corresponding CK19 (an epithelial marker) of each
individual sample. The primers used for CK19 were: sense, 5′-CAGGTC
CGAGGTTACTGAC-3′ and antisense, 5′- ACTGAACCTGACCGTACA
CCGTTTCTGCCAGTGTGTCTTC-3′.
Construction of SGPP1 ribozyme transgenes
and transfection
Anti-SGPP1 ribozyme transgenes were used to
knock down the expression of SGPP1 in the AGS and HGC27
gastric cancer cells and were generated using the methods
previously described (13).
Briefly, an anti-SGPP1 hammerhead ribozyme was designed
based on the secondary structure of SGPP1 mRNA and generated
using the Zuker's RNA mFold program. The ribozymes that
specifically target DAP3 were generated using the touchdown PCR
with the appropriate primers (sense,
5′-CTGCAGTTCAACCACTTCTCCCAGAGCTGATGAGTCCGTGAGGA-3′ and antisense,
5′-ACTAGTAGAGAAAGCACTGAGAAAGGGAGTTTCGTCCTCACGGACT-3′). The
amplified ribozymes were cloned into the pEF6/V5-His TOPO TA
plasmid vector (Invitrogen, Paisley, UK) in accordance with the
protocol provided. Ribozyme transgenes and control plasmids were
transfected into HGC27 and AGS cells individually using an Easyjet
Plus electroporator (EquiBio, Kent, UK). After up to 5 days of
selection with blasticidin, the transfectants were verified for
knockdown of SGPP1.
Western blotting
HGC27 and AGS cells were plated into small flasks at
a density of 25×105 cells/well. Proteins were isolated
from cells by lysis buffer. Protein concentrations were determined
using the DC Protein Assay kit (Bio-Rad) and an ELx800
spectrophotometer (Bio-Tek, Bedfordshire, UK). Western blot
analysis was performed after SDS-PAGE and transferred onto
membranes. The proteins were probed with the
anti-SGPP1-antibody (1:500) and anti-GAPDH-antibody
(1:1,000) (Santa-Cruz Biotechnology, Inc.) as an internal control,
followed by a peroxidase-conjugated secondary antibody (1:1,000).
Protein bands were visualized and photographed using a UVITech
imager (UVITech, Inc., Cambridge, UK).
Cell growth assay
Crystal violet assay was conducted as previously
described (11). Cells were added
into 96-well plates at 2×103 cells/well. The cells were
fixed in 4% paraformaldehyde at room temperature for 10 min after
1, 3 and 5 days. After being washed, the plates were stained with
0.5% crystal violet solution. The plates were washed with tap water
and air-dried. Acetic acid (10%) was added to each well for
extraction of dye. Growth rates under normal conditions and under
treatment were assessed. Absorbance of the staining was determined
by a spectrophotometer at 540 nm (EL×800; Bio-Tek).
Cell matrix adhesion assay
The cell matrix adhesion assay was performed as
previously described (14). Cells
were added to a 96-well plate precoated with Matrigel (5 mg/well)
(2×104 cells/well). After 40 min of incubation,
non-adherent cells were washed off using BSS buffer. The remaining
cells were fixed with 4% paraformaldehyde, stained with 0.5%
crystal violet solution and counted.
Wound-healing assay
The motility of gastric cancer cells was analyzed
using a wound-healing assay as previously described (15). The cells were grown until they
reached confluence. A scrape in the cell monolayer was made in one
direction with a fine gauge needle. The wounded cell monolayers
were washed with PBS to remove cell debris. The migration of the
invading cell front was recorded on a time lapse video recorder and
analyzed using Optimas 6.0 motion analysis (Meyer Instruments,
Houston, TX, USA).
Invasion assay
The in vitro Matrigel invasion assay was
performed as previously described (15). Transwell inserts with 8-mm pore size
were coated with 50 µg of Matrigel (Collaborative Research
Products, Bedford, MA, USA) and air-dried. Following rehydration,
4×104 cells were added to each well. After 3 days of
incubation, the cells that had migrated through the matrix to the
other side of the insert were fixed, stained and counted.
Statistical analysis
Statistical analysis was performed using the SPSS
software (SPSS standard version 13.0; SPSS Inc.). The relationship
between SGPP1 expression and tumor grade, TNM staging and
nodal status was assessed using the Mann-Whitney U test and
Kruskal-Wallis test. Survival was analyzed using the Kaplan-Meier
survival analysis. Results are presented as mean ± SEM. P<0.05
was considered statistically significant.
Results
Immunohistochemical staining of SGPP1 in
human gastric specimens
In total, 282 paraffin-embedded specimens of gastric
cancer patients from Beijing Cancer Hospital were included in the
IHC study. This cohort comprised 196 males (69.5%) and 86 females
(31.5%), with a median age of 69 (22–87) years. The patients
underwent surgery without any prio treatment. The median follow-up
time was 41.13 (1.00–137.17) months. The result was that, 36
patients had recurrence, 130 patients succumbed to gastric cancer,
15 patients succumbed to other causes (heart attack and cerebral
haemorrhage), 11 were lost in follow-up and 107 remained alive and
progression-free.
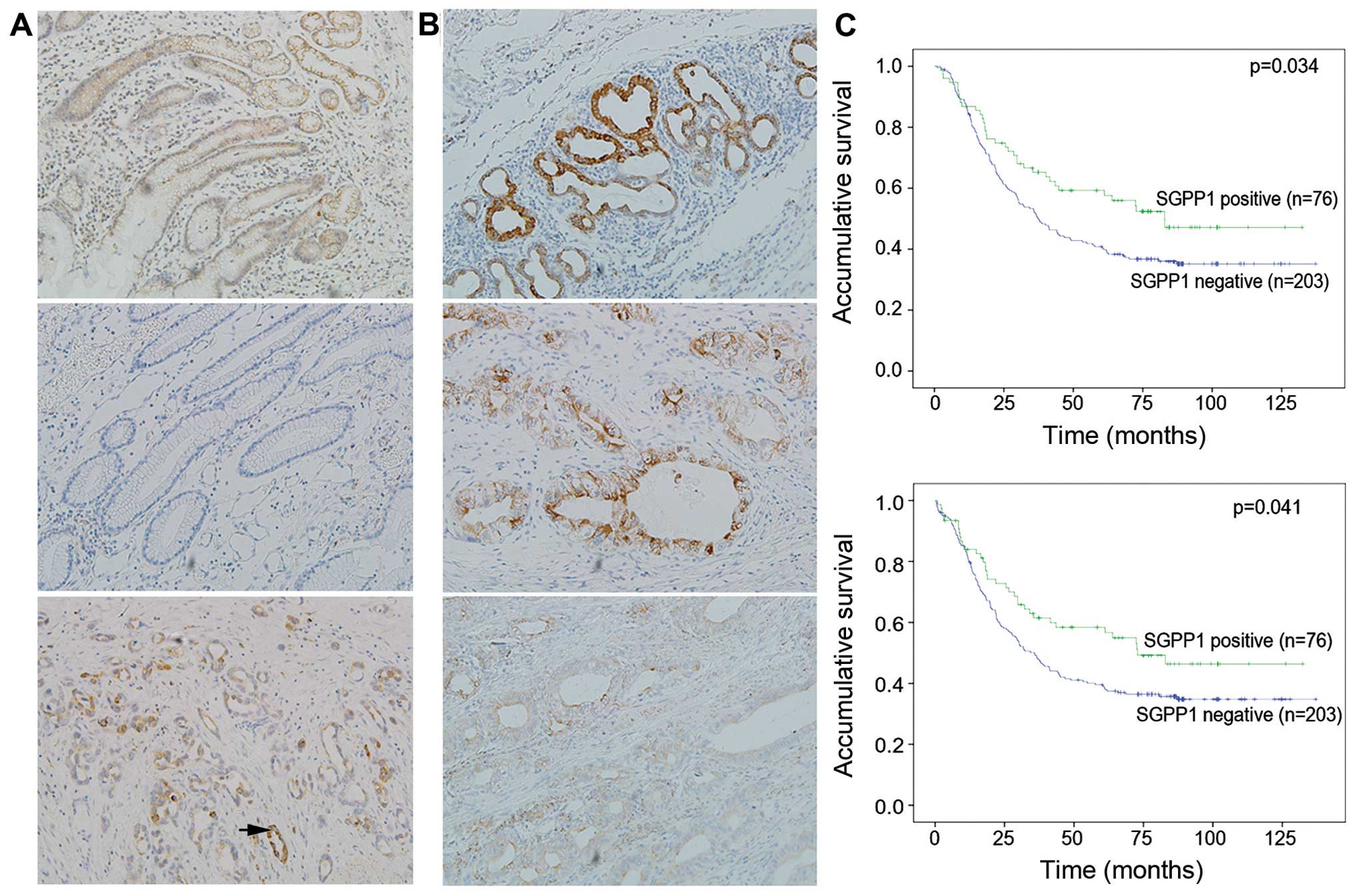
Negative staining results were considered as low
expression and '+', '++', '+++' as high expression. SGPP1
was mainly detected in cytoplasm and the staining was obviously
stronger in normal tissue compared with tumor tissues (p<0.001).
A low expression of SGPP1 was positively associated with
lymph node metastasis (p=0.005) and distant metastasis (p=0.031)
(Table I). Kaplan-Meier survival
curves revealed that patients with a high SGPP1 expression
had a significant increase in OS and progression-free survival
(PFS) in gastric cancer patients (p=0.034, 0.041; Fig. 1). Multivariate analysis indicated
the expression of SGPP1 was an independent prognostic factor
in gastric cancer patients (p=0.041; Table II).
 | Table IAssociation of SGPP1 expression with
clinicopathological characteristics in gastric cancer patients. |
Table I
Association of SGPP1 expression with
clinicopathological characteristics in gastric cancer patients.
| Clinicopathological
characteristics | SGPP1 expression
| P-value |
|---|
| Negative (%) | Positive (%) |
|---|
| Gender | | | 0.357 |
| Male | 138 (71.1) | 56 (28.9) | |
| Female | 65 (76.5) | 20 (23.5) | |
| Age (years) | | | 0.616 |
| ≤60 | 100 (71.4) | 40 (28.6) | |
| >60 | 103 (74.1) | 36(25.9) | |
| Tumor location | | | 0.016 |
| Upper 1/3 | 37 (61.7) | 23 (38.3) | |
| Middle 1/3 | 45 (67.2) | 22 (32.8) | |
| Low 1/3 | 112 (78.3) | 31 (21.7) | |
| Total | 9 (100.0) | 0 (0.0) | |
| Cardia and
non-cardia | | | 0.007 |
| Non-cardiac
cancer | 175 (76.1) | 55 (23.9) | |
| Cardiac
cancer | 28 (57.1) | 21 (42.9) | |
| Tumor size
(cm) | | | 0.855 |
| ≤4.0 | 112 (73.2) | 41 (26.8) | |
| >4.0 | 91 (72.2) | 35 (27.8) | |
| Lauren type | | | 0.560 |
| Intestinal
type | 40 (70.2) | 17 (29.8) | |
| Diffuse | 116 (75.3) | 38 (24.7) | |
| Mixed type | 47 (69.1) | 21 (30.9) | |
|
Differentiation | | | 0.216 |
| Well-moderate | 90 (69.2) | 40 (30.8) | |
| Poor | 113 (75.8) | 36 (24.2) | |
| Well | 7 (58.3) | 5 (41.7) | 0.474 |
| Moderate | 83 (70.3) | 35 (29.7) | |
| Poor | 101 (76.5) | 31 (23.5) | |
| Signet | 12 (70.6) | 5 (29.4) | |
| Histology | | | 0.464 |
|
Adenocarcinoma | 169 (71.9) | 66 (28.1) | |
| Other
typesa | 34 (77.3) | 10 (22.7) | |
| Lymphovascular
invasion | | | 0.486 |
| Absent | 100 (70.9) | 41 (29.1) | |
| Present | 103 (74.6) | 35 (25.4) | |
| Depth of
invasion |
| T1 | 14 (77.8) | 4 (22.2) | 0.385 |
| T2 | 25 (67.6) | 12 (32.4) | |
| T3 | 7 (100.0) | 0 (0.0) | |
| T4 | 157 (72.4) | 60 (27.6) | |
|
T1+T2 | 39 (42.5) | 16 (57.5) | 0.731 |
|
T3+T4 | 164 (26.0) | 60 (74.0) | |
| T1 | 14 (77.8) | 4 (22.2) | 0.787 |
|
T2+T3+T4 | 189 (72.4) | 72 (27.6) | |
| Lymph node
metastasis |
| N0 | 46 (71.9) | 18 (28.1) | 0.005 |
| N1 | 28 (53.8) | 24 (46.2) | |
| N2 | 35 (76.1) | 11 (23.9) | |
| N3 | 94 (80.3) | 23 (19.7) | |
| No | 46 (71.9) | 18 (28.1) | 0.856 |
| Yes | 157 (73.0) | 58 (27.0) | |
| Distant
metastasis | | | 0.031 |
| No | 177 (70.8) | 73 (29.2) | |
| Yes | 26 (89.7) | 3 (10.3) | |
| TNM stage | | | 0.171 |
| I | 26 (74.3) | 9 (25.7) | |
| II | 28 (68.3) | 13 (31.7) | |
| III | 123 (70.7) | 51 (29.3) | |
| IV | 26 (89.7) | 3 (10.3) | |
| I | 26 (74.3) | 9 (25.7) | 0.828 |
| II–IV | 177 (72.5) | 67 (27.5) | |
| I+II | 54 (71.1) | 22 (28.9) | 0.695 |
| III+IV | 149 (73.4) | 54 (26.6) | |
| Table IIPatient survival associated with
clinicopathological characteristics in gastric cancer. |
Table II
Patient survival associated with
clinicopathological characteristics in gastric cancer.
| Clinicopathological
characteristics | Univariate analysis
| Multivariate
analysis
|
|---|
| RR | 95% CI | P-value | RR | 95% CI | P-value |
|---|
| Gender |
| Male vs.
female | 1.211 | 0.858–1.710 | 0.276 | | | |
| Age (years) |
| ≤60 vs.
>60 | 0.787 | 0.579–1.068 | 0.125 | | | |
| Tumor location |
| Upper 1/3 | 0.380 | 0.184–0.784 | 0.009 | | | |
| Middle 1/3 | 0.212 | 0.101–0.446 | 0.230 | | | |
| Low 1/3 | 0.257 | 0.128–0.514 | 0.118 | | | |
| Multiple site | 0.000 | | | | | |
| Tumor size
(cm) |
| >4.0 vs.
≤4.0 | 0.661 | 0.487–0.897 | 0.008 | | | |
| Lauren type |
| Intestinal vs.
diffuse/mixed | 1.042 | 0.718–1.514 | 0.828 | | | |
|
Differentiation |
| Well-moderate vs.
poor | 1.270 | 0.935–1.726 | 0.126 | 1.411 | 1.017–1.957 | 0.039 |
| Histology |
| Adenocarcinoma vs.
other typesa | 1.264 | 0.851–1.877 | 0.246 | | | |
| Lymphovascular
invasion |
| Absent vs.
present | 2.072 | 1.519–2.825 | <0.001 | 1.449 | 1.046–2.007 | 0.026 |
| Depth of
invasion |
| T1 | 0.000 | | 0.938 | | | |
| T2 | 0.160 | 0.160–0.544 | 0.000 | | | |
| T3 | 0.153 | 0.153–2.499 | 0.500 | | | |
| T4 | 1 | | 0.001 | | | |
|
T1+T2 vs.
T3+T4 | 5.375 | 2.911–9.924 | <0.001 | 2.627 | 1.372–5.033 | 0.004 |
| Lymph node
metastasis |
| N0 | 0.118 | 0.066–0.211 | <0.001 | | | |
| N1 | 0.241 | 0.148–0.391 | <0.001 | | | |
| N2 | 0.673 | 0.431–0.942 | 0.024 | | | |
| N3 | 1.000 | | <0.001 | | | |
| No vs. yes | 5.391 | 3.055–9.513 | <0.001 | 3.628 | 1.990–6.614 | <0.001 |
| Distant
metastasis |
| No vs. yes | 0.168 | 0.110–0.256 | <0.001 | 0.277 | 0.179–0.428 | <0.001 |
| SGPP1 |
| Negative vs.
positive | 0.673 | 0.465–0.973 | 0.036 | 0.671 | 0.458–0.985 | 0.041 |
Quantification of SGPP1 mRNA expression
in human gastric cancer
mRNA derived from the 219 gastric cancer patient
tissues from the Beijing Cancer Hospital were subjected to a
SGPP1 gene-specific qPCR study. This cohort comprised 144
males (65.8%) and 75 females (34.2%). The patients underwent the
surgery without any prior treatment. The result was that, 86
patients were alive, 130 patients succumbed to gastric cancer, 9
patients had metastasis and 117 remained disease-free.
We compared the transcript levels of SGPP1 in
gastric cancer tissues with adjacent normal tissues of patients.
The transcript level of SGPP1 was significantly different in
the T stage (p=0.009) and TNM stage (p=0.0255). Statistical
analysis revealed significant links between the different clinical
outcomes (p=0.0379) and different transcript levels. A markedly
decreased transcript of SGPP1 was observed in tumor tissues
compared with the normal background tissues (p<0.0001; Table III).
| Table IIICorrelation of the mRNA expression of
SGPP1 and clinical parameters. |
Table III
Correlation of the mRNA expression of
SGPP1 and clinical parameters.
| Category | No. | Median | Q1 | Q3 | P-value |
|---|
| T/Nb | | | | | <0.001 |
| Normal | 183 | 2.50 | 0 | 56 | |
| Tumor | 322 | 0.10 | 0 | 21 | |
| Gender | | | | | 0.7876 |
| Male | 229 | 0.10 | 0 | 16 | |
| Female | 93 | 0.10 | 0 | 29 | |
| Location |
| Cardia | 66 | 0.30 | 0 | 53 | |
| Fundus | 21 | 2.90 | 0 | 52 | 0.3310 |
| Corpus | 61 | 0.10 | 0 | 27 | 0.4796 |
| Pylorus | 130 | 0.00 | 0 | 16 | 0.1696 |
|
Differentiation |
| Diff-H | 1 | 0.00 | N/A | N/A | |
| Diff-HM | 6 | 0.03 | 0 | 1.69 | |
| Diff-M | 62 | 0.03 | 0 | 6 | 0.3812 |
| Diff-ML | 81 | 0.08 | 0 | 28 | 0.2121 |
| Diff-L | 137 | 0.10 | 0 | 29 | 0.2510 |
| T stage |
| T1 | 16 | 0.01 | 0 | 0.64 | |
| T2 | 25 | 0.00 | 0 | 0 | 0.3706 |
| T3 | 31 | 6.20 | 0 | 83 | 0.0586 |
| T4 | 232 | 0.08 | 0 | 26 | 0.2526 |
| | | | | 0.009 |
| T1+T2 | 41 | 0.00 | 0 | 0 | |
| T3+T4 | 273 | 0.10 | 0 | 28 | |
| N stage |
| N0 | 71 | 0.00 | 0 | 5 | |
| N1 | 48 | 0.00 | 0 | 8 | 0.8221 |
| N2 | 64 | 0.00 | 0 | 24 | 0.1375 |
| N3 | 133 | 0.00 | 0 | 45 | 0.0244 |
| | | 0.00 | | 0.0519 |
| N0 | 133 | 0.00 | 0 | 45 | |
| N1+N2+N3 | 245 | 0.00 | 0 | 29 | |
| M stage | | | 0 | | 0.7139 |
| M0 | 280 | 0.10 | 0 | 13 | |
| M1 | 41 | 0.00 | 0 | 93 | |
| TNM stage | | | 0 | | |
| I | 25 | 0.00 | 0 | 0.60 | |
| II | 59 | 0.02 | 0 | 10 | 0.5474 |
| III | 220 | 0.20 | | 30 | 0.0516 |
| IV | 9 | 1.00 | 0 | 258 | 0.0334 |
| | | | | 0.0255 |
| I+II | 84 | 0.00 | 0 | 4 | |
| III+IV | 229 | 0.00 | 0 | 32 | |
| Vascular
invasion | | | | | 0.6462 |
| No invasion | 152 | 0.00 | 0 | 23 | |
| Invasion | 155 | 0.10 | 0 | 19 | |
| Clinical
outcome | | | 0 | | 0.0379 |
| Alive | 134 | 0.00 | 0 | 4 | |
| Dead | 185 | 0.40 | 0 | 45 | |
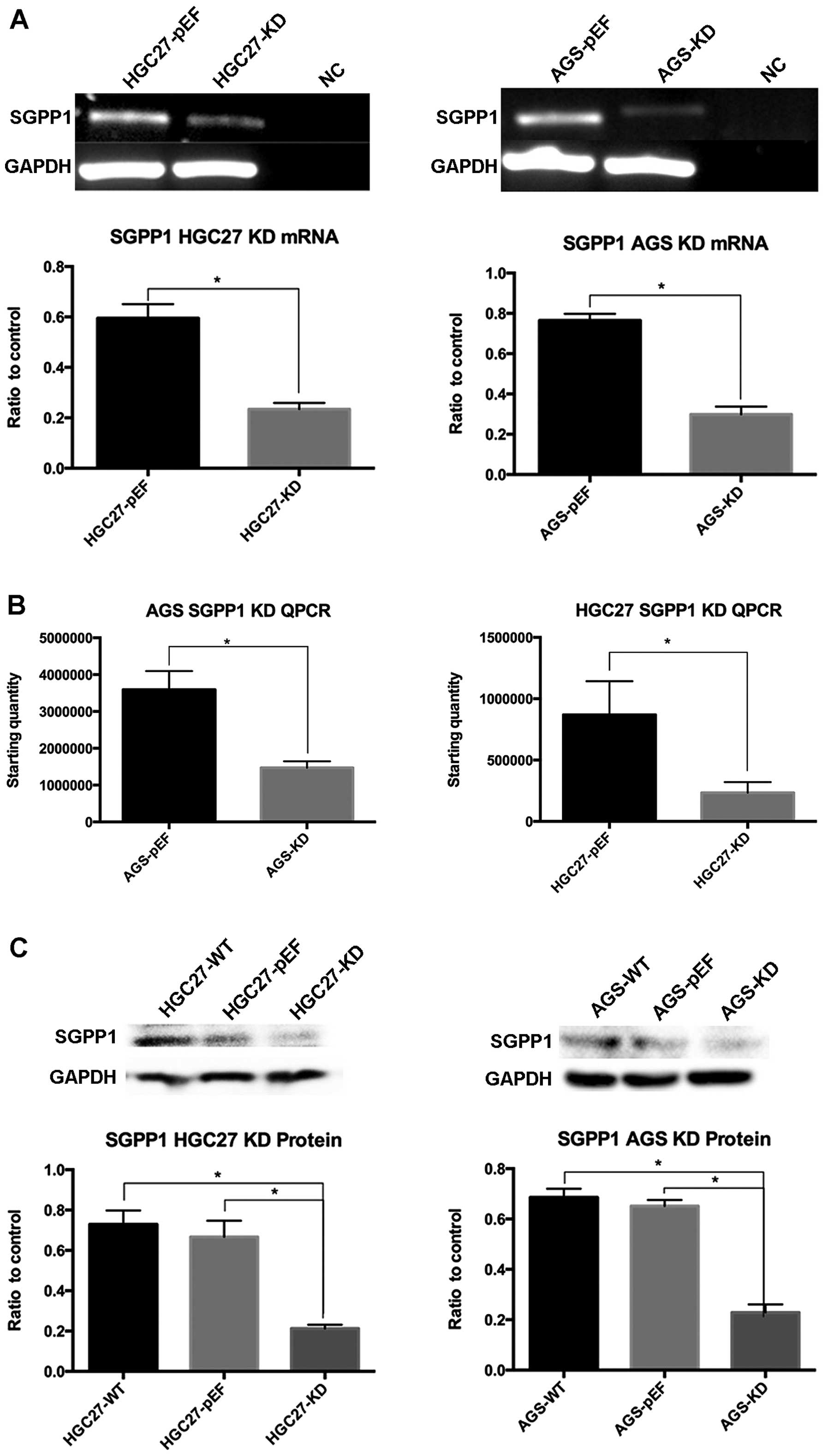
Knockdown effect of SGPP1 on the
functions of gastric cancer cells
The expression of SGPP1 in HGC27 and AGS
cells transfected with corresponding anti-SGPP1 ribozyme transgenes
was examined using conventional PCR. The results showed a
significantly lower expression level of SGPP1 compared with
the control group (2- to 3-fold) (Fig.
2A), and the same knockdown effect was observed in qPCR and
western blot analysis (2- to 3-fold) (Fig. 2B and C).
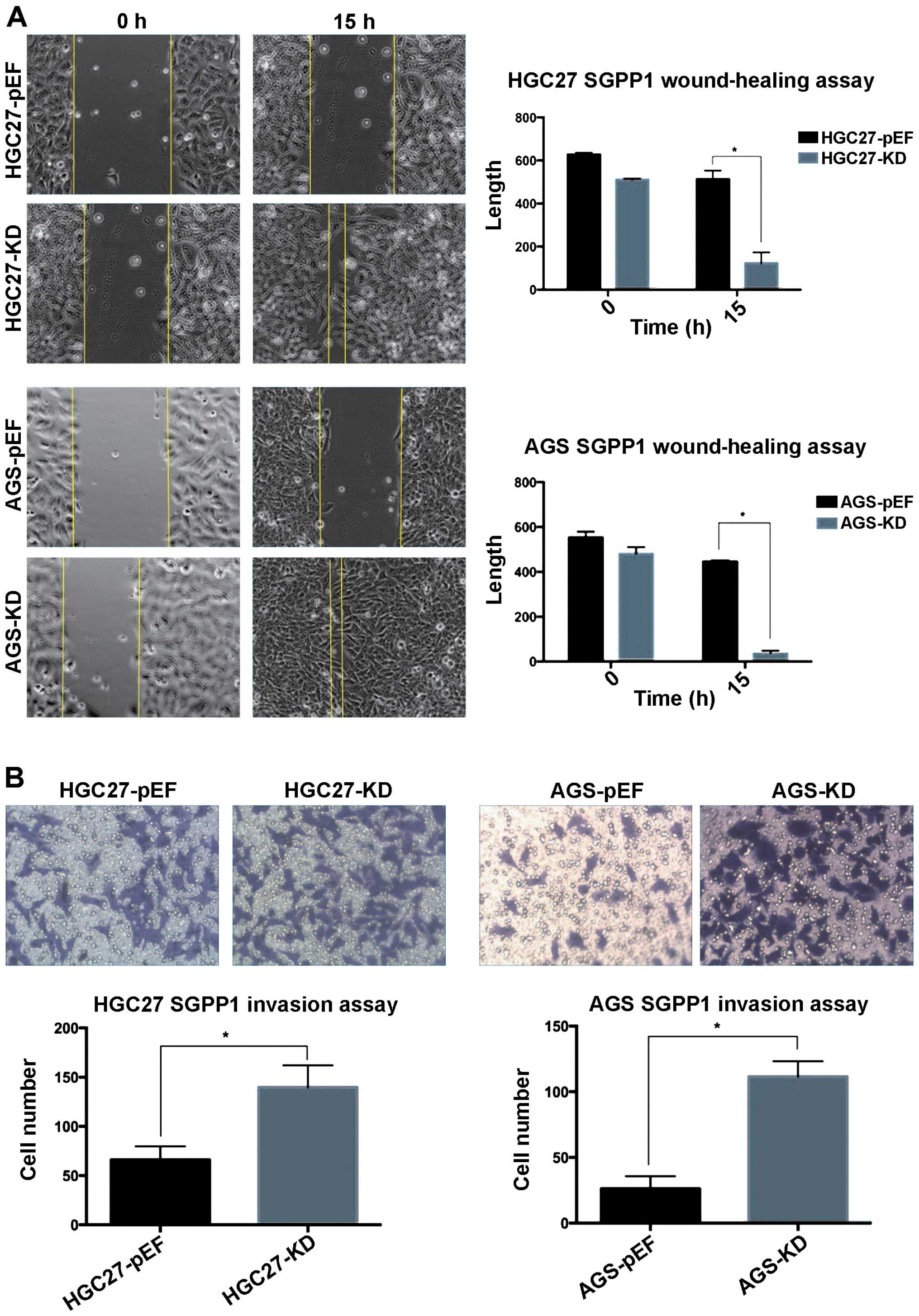
Migration and invasion assay
To determine whether downregulating the expression
of SGPP1 affected the biological behavior of gastric cancer
cell lines, we performed a wound-healing assay of the cells. The
AGS and HGC27 cells transfected with anti-SGPP1 ribozyme
exhibited a significant increase in the ability of migration of
tumor cells compared with the control cells. A significant
difference was identified for the two cells (p<0.05, 2- to
5-fold; Fig. 3A).
The effect of SGPP1 knockdown on cell lines
on migration was investigated using an in vitro invasion
assay. The decrease in the expression of SGPP1 was
significantly correlated with an increase in cell invasion in AGS
and HGC27 cell lines (p<0.05, 3-fold; Fig. 3B).
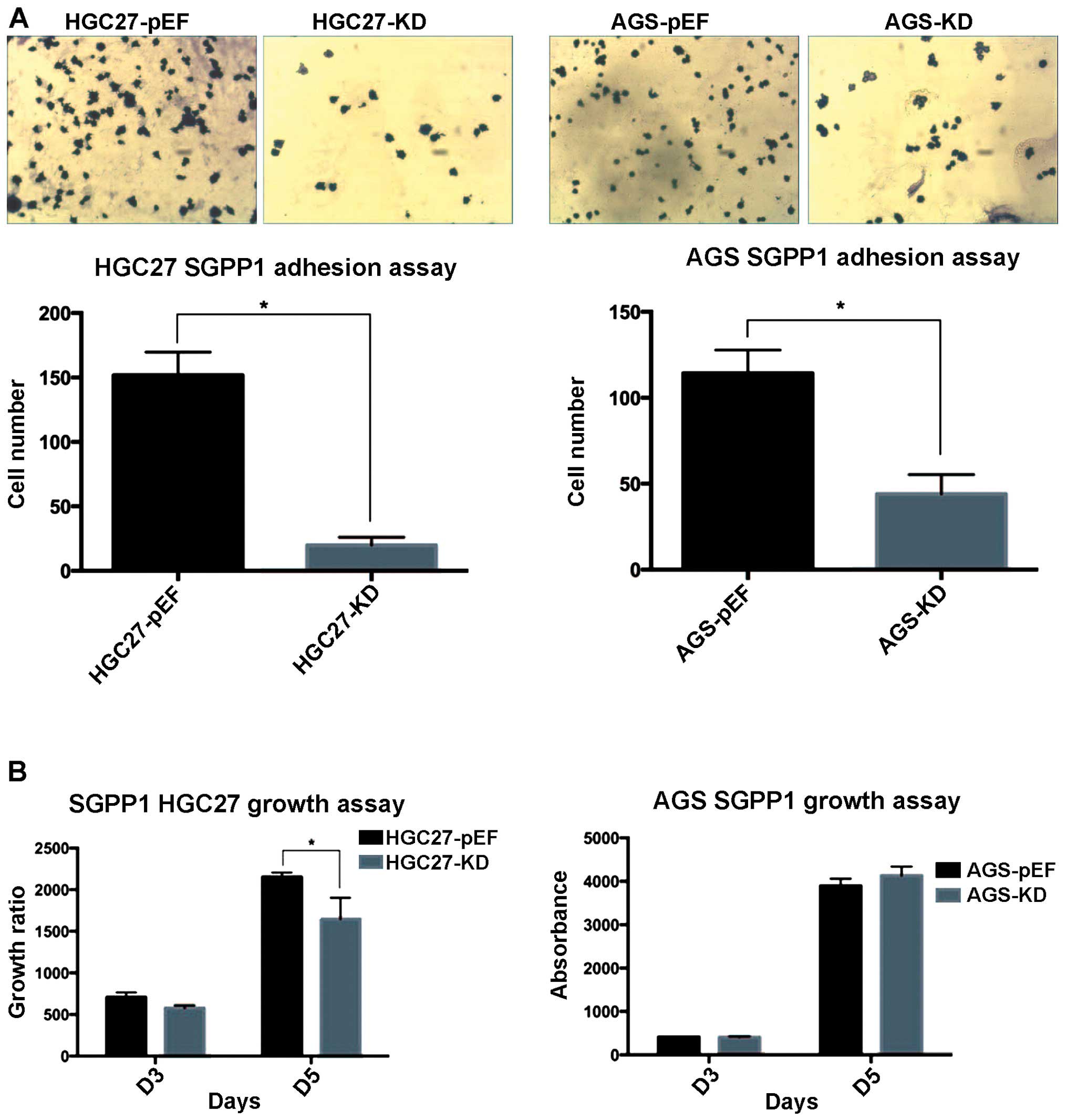
Adhesion and growth assay
An in vitro matrix adhesion assay was used to
investigate the effect of SGPP1 knockdown on cell lines on
the adhesion ability of gastric cancer cell lines. The HGC27 and
AGS cell lines transfected with SGPP1 ribozyme significantly
inhibited matrix adhesion ability compared with the control cell
line (p<0.05, 2- to 5-fold; Fig.
4A).
Furthermore, to determine whether the expression of
SGPP1 affected the growth of gastric cancer cells, we
carried out a growth assay. The results showed that the HGC27 cell
line transfected with SGPP1 ribozyme markedly inhibited
growth on day 5 (p<0.05) and there was no significant difference
on day 3, whereas this effect was not observed in the AGS cell line
transfected with SGPP1 ribosome (Fig. 4B).
Discussion
Gastric cancer has become the fifth most common
cancer worldwide over the past decades. There are ~480,000 new
patients developing this cancer in China each year (1). At the same time, gastric cancer, whose
estimated mortality rates ranks the highest in China, has also
become the third leading cause of cancer mortality worldwide.
Although the incidence rates of gastric cancer have gradually
decreased (16), ~80% of patients
with gastric cancer in China are at an advanced stage (17).
Despite new developments in the treatment for
advanced gastric cancer patients, such as adjuvant chemotherapy
(18), new adjuvant chemotherapy
and concurrent chemoradiotherapy (19) plus surgery or surgery, the 5-year
survival rate of patients has only been marginally improved
(20). The main reason for this
lack of significant improvement is mostly due to the fact that
diagnosis is frequently made after progression to later stages, at
which point current therapeutic strategies exert limited
effectiveness. Furthermore, the major challenge to cancer treatment
is the recurrence of diseases due to therapeutic resistance. In
many patients, microscopic or macroscopic metastases have already
occurred by the time the in situ lesion is detected.
Therefore, early detection and more accurate methods in predicting
disease outcomes, may enable physicians to make informed decisions
regarding the potential necessity of early intervention.
Consequently, early intervention would significantly decrease the
mortality of gastric cancer and greatly improve the 5-year survival
rate.
S1P is a bioactive sphingolipid that is important in
regulating diverse biological processes (21). S1P is a component of cell membranes
with high amphotericity, which enables S1P to possess sufficient
aqueous solubility to move between membranes (22–24) as
a bioactive signalling molecule. S1P is known to be involved in the
regulation of diverse biological behavior. Particularly, S1P has
emerged as an important signalling mediator participating in the
regulation of various cell processes and diseases, including
cancer, wound healing, atherosclerosis and immunity. S1P functions
through either a family of five G protein-coupled membrane
receptors known as S1PR1-5 (25,26) or
intracellular targets, such as, prohibitin 2 (27), TNF receptor-associated factor 2
(TRAF2) (28), and histone
deacetylase (HDAC) (29). Through
interaction of these intracellular targets, S1P regulates a wide
variety of biological effects (30), such as cell movement,
differentiation, survival, inflammation, immunity, calcium
homeostasis, and angiogenesis.
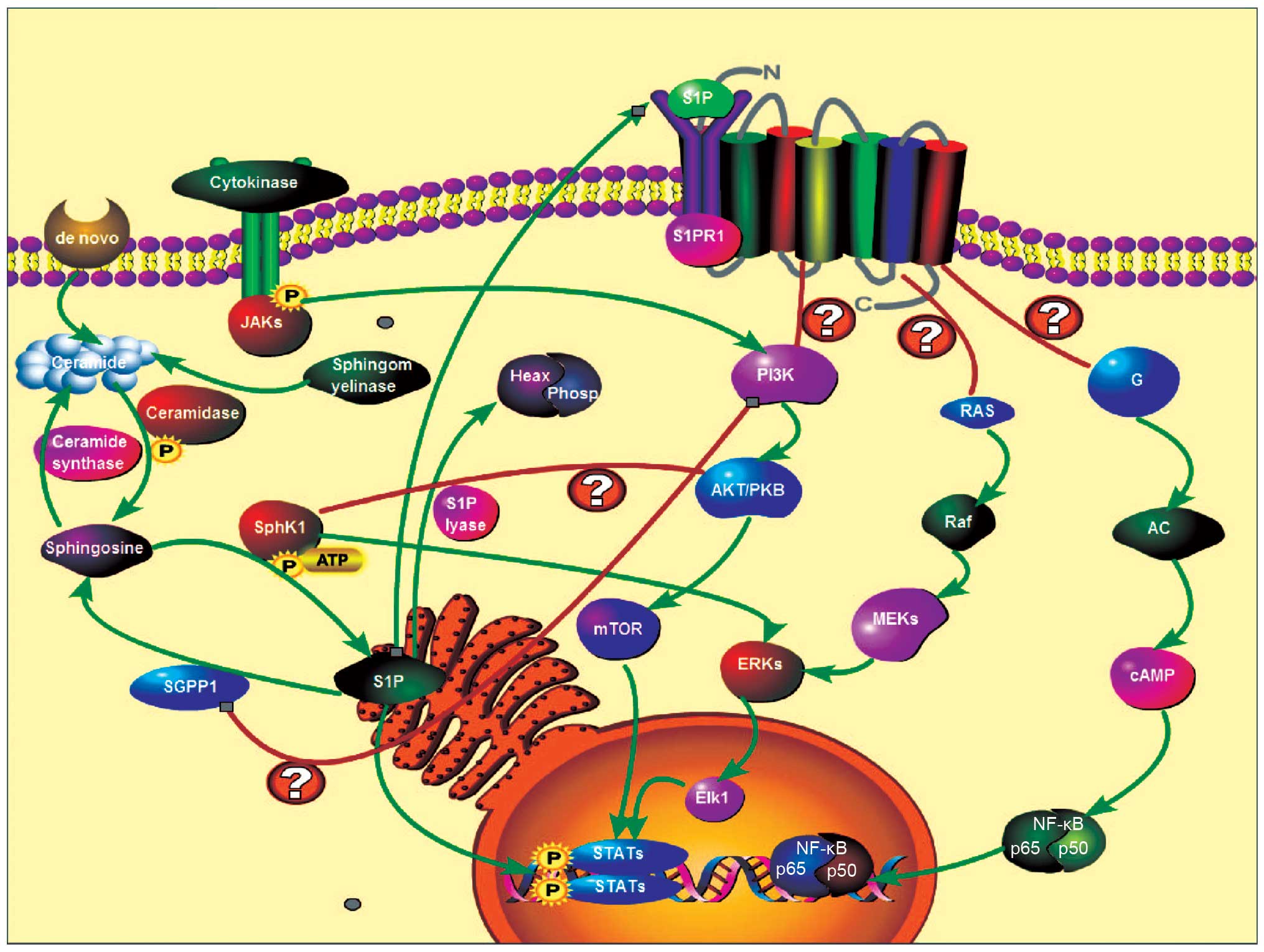
S1P may be dephosphorylated by SGPPs which
convert S1P to sphingosine. Previous studies have shown that
S1P level has a 2-fold increase in the SGPPs knockdown cell
lines (8). There are two isoforms
of SGPPs, SGPP1 (31)
and SGPP2 (32).
SGPPs can dephosphorylate S1P to regenerate
sphingosine, leading to S1P inactivation. This, in turn,
would lead cells to apoptosis as well as degeneration (9). SGPPs were highly selective for
sphingolipid substrates (33).
SGPPs have also been reported to be regulated by other
factors. For example, laminar shear stress also downregulates the
expression of SGPP1 while concomitantly stimulating
S1P released from endothelial cells in vitro
(34). SGPP1 may also
control the unfolded protein response and ER stress-induced
autophagy (35), as well as
vascular tone (36). Overexpression
of SGPPs may elevate ceramide levels and provoke apoptosis,
whereas knockdown of SGPP1 enhanced resistance to TNF-α and
the chemotherapeutic agent daunorubicin (8) and radiotherapy (10) (Fig.
5).
In this study, we examined the function of
SGPP1 on gastric cancer cell lines as well as its clinical
significance in gastric cancer progression. SGPP1 is a
potential biomarker candidate for early diagnosis and/or prognosis
for patients with advanced gastric cancer. By accessing a relative
large cohort of gastric cancer, we retrospectively evaluated the
relationship between the level of SGPP1 expression and
clinical characteristics. Our results showed that the patients who
had a higher level of SGPP1 expression had a longer OS and
PFS compared with a lower level of SGPP1 expression. Our
study has demonstrated that a positive expression of SGPP1
was an early diagnosis of improved clinical outcome in gastric
cancer patients. In addition, the study showed that SGPP1
expression was statistically associated with the location of tumor
and lymph node metastasis in gastric cancer patients. Moreover,
multivariate survival analysis showed that SGPP1 was an
independent prognostic factor. Based on these results, we suggest
that SGPP1 was a novel molecular prognosticator in the
evaluation of gastric cancer patient survival.
Invasion and metastasis are major obstacles in the
effort to improve survival of gastric cancer patients (37). Our in vitro study showed that
the cell ability of invasion and migration was markedly increased
in the gastric cell lines which the expression of SGPP1 is
downregulated compared with the negative control. This phenomenon
is similar to the observation in the data, showing a significant
association with lymph node metastasis. Collectively, we suggest
that SGPP1 serves as a novel prognostic marker of cancer
cell invasion and metastasis. In addition, we found that
downregulating the expression of SGPP1 affected the adhesion
and growth ability in HGC27 cells but no significant change
occurred in AGS cells. The reason for this phenomenon may be that
the cancer cell decreases the ability of adhesion from the primary
location and at the same time increases the ability of invasion and
metastasis and epithelial-mesenchymal transition
In conclusion, the result show that SGPP1
expression is significantly lower in tumor tissue than that in the
normal paired tissue, while downregulation of SGPP1 leads to
an increase in cell migration and invasion in gastric cancer. A
lower SGPP1 expression is correlated with lymph node
metastasis and SGPP1 expression knockdown may lead to a more
aggressive invasion and migration ability. Therefore, there is a
significant correlation between SGPP1 expression and OS, PFS
in the gastric cancer cohort. Taken together, the results indicate
SGPP1 is a potential molecular marker that may be used to
predict the effectiveness of prognosis in gastric cancer
patients.
Acknowledgments
The authors wish to thank Cancer Research Wales, the
Albert Hung Foundation, the Yiling Foundation, the Ser Cymru Welsh
Life Science Network, Beijing Municipal Science & Technology
Commission (D141100000414002) and the Natural Science Foundation of
China (81374016) for supporting their work. Dr Xiang Y. Gao is a
recipient of Cardiff University China Medical Scholarship.
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cunningham D and Chua YJ: East meets west
in the treatment of gastric cancer. N Engl J Med. 357:1863–1865.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Petrelli NJ: The debate is over; it's time
to move on. J Clin Oncol. 22:2041–2042. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cunningham D, Allum WH, Stenning SP,
Thompson JN, Van de Velde CJ, Nicolson M, Scarffe JH, Lofts FJ,
Falk SJ, Iveson TJ, et al MAGIC Trial Participants: Perioperative
chemotherapy versus surgery alone for resectable gastroesophageal
cancer. N Engl J Med. 355:11–20. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bang YJ, Van Cutsem E, Feyereislova A,
Chung HC, Shen L, Sawaki A, Lordick F, Ohtsu A, Omuro Y, Satoh T,
et al ToGA Trial Investigators: Trastuzumab in combination with
chemotherapy versus chemotherapy alone for treatment of
HER2-positive advanced gastric or gastro-oesophageal junction
cancer (ToGA): A phase 3, open-label, randomised controlled trial.
Lancet. 376:687–697. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Van Cutsem E, de Haas S, Kang YK, Ohtsu A,
Tebbutt NC, Ming Xu J, Peng Yong W, Langer B, Delmar P, Scherer SJ,
et al: Bevacizumab in combination with chemotherapy as first-line
therapy in advanced gastric cancer: A biomarker evaluation from the
AVAGAST randomized phase III trial. J Clin Oncol. 30:2119–2127.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Payne SG, Milstien S and Spiegel S:
Sphingosine-1-phosphate: Dual messenger functions. FEBS Lett.
531:54–57. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Johnson KR, Johnson KY, Becker KP,
Bielawski J, Mao C and Obeid LM: Role of human
sphingosine-1-phosphate phosphatase 1 in the regulation of intra-
and extracellular sphin-gosine-1-phosphate levels and cell
viability. J Biol Chem. 278:34541–34547. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Le Stunff H, Galve-Roperh I, Peterson C,
Milstien S and Spiegel S: Sphingosine-1-phosphate phosphohydrolase
in regulation of sphingolipid metabolism and apoptosis. J Cell
Biol. 158:1039–1049. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Huang X, Taeb S, Jahangiri S, Emmenegger
U, Tran E, Bruce J, Mesci A, Korpela E, Vesprini D, Wong CS, et al:
miRNA-95 mediates radioresistance in tumors by targeting the
sphingolipid phosphatase SGPP1. Cancer Res. 73:6972–6986. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ji K, Ye L, Toms AM, Hargest R, Martin TA,
Ruge F, Ji J and Jiang WG: Expression of signal-induced
proliferation-associated gene 1 (SIPA1), a RapGTPase-activating
protein, is increased in colorectal cancer and has diverse effects
on functions of colorectal cancer cells. Cancer Genomics
Proteomics. 9:321–327. 2012.PubMed/NCBI
|
|
12
|
Jiang WG, Grimshaw D, Lane J, Martin TA,
Abounader R, Laterra J and Mansel RE: A hammerhead ribozyme
suppresses expression of hepatocyte growth factor/scatter factor
receptor c-MET and reduces migration and invasiveness of breast
cancer cells. Clin Cancer Res. 7:2555–2562. 2001.PubMed/NCBI
|
|
13
|
Parr C and Jiang WG: Metastasis suppressor
1 (MTSS1) demonstrates prognostic value and anti-metastatic
properties in breast cancer. Eur J Cancer. 45:1673–1683. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jiang WG, Hiscox S, Hallett MB, Scott C,
Horrobin DF and Puntis MC: Inhibition of hepatocyte growth
factor-induced motility and in vitro invasion of human colon cancer
cells by gamma-linolenic acid. Br J Cancer. 71:744–752. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Jiang WG, Hiscox SE, Parr C, Martin TA,
Matsumoto K, Nakamura T and Mansel RE: Antagonistic effect of NK4,
a novel hepatocyte growth factor variant, on in vitro angiogenesis
of human vascular endothelial cells. Clin Cancer Res. 5:3695–3703.
1999.PubMed/NCBI
|
|
16
|
Bertuccio P, Chatenoud L, Levi F, Praud D,
Ferlay J, Negri E, Malvezzi M and La Vecchia C: Recent patterns in
gastric cancer: A global overview. Int J Cancer. 125:666–673. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rivera F, Vega-Villegas ME and López-Brea
MF: Chemotherapy of advanced gastric cancer. Cancer Treat Rev.
33:315–324. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sasako M, Sakuramoto S, Katai H, Kinoshita
T, Furukawa H, Yamaguchi T, Nashimoto A, Fujii M, Nakajima T and
Ohashi Y: Five-year outcomes of a randomized phase III trial
comparing adjuvant chemotherapy with S-1 versus surgery alone in
stage II or III gastric cancer. J Clin Oncol. 29:4387–4393. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lee J, Lim H, Kim S, Park SH, Park JO,
Park YS, Lim HY, Choi MG, Sohn TS, Noh JH, et al: Phase III trial
comparing capecitabine plus cisplatin versus capecitabine plus
cisplatin with concurrent capecitabine radiotherapy in completely
resected gastric cancer with D2 lymph node dissection: The ARTIST
trial. J Clin Oncol. 30:268–273. 2012. View Article : Google Scholar
|
|
20
|
Falcone A: Future strategies and adjuvant
treatment of gastric cancer. Ann Oncol. 14(Suppl 2): ii45–47. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hannun YA: Functions of ceramide in
coordinating cellular responses to stress. Science. 274:1855–1859.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Boujaoude LC, Bradshaw-Wilder C, Mao C,
Cohn J, Ogretmen B, Hannun YA and Obeid LM: Cystic fibrosis
transmembrane regulator regulates uptake of sphingoid base
phosphates and lysophosphatidic acid: Modulation of cellular
activity of sphingosine 1-phosphate. J Biol Chem. 276:35258–35264.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hannun YA and Obeid LM: Principles of
bioactive lipid signalling: Lessons from sphingolipids. Nat Rev Mol
Cell Biol. 9:139–150. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wojciak JM, Zhu N, Schuerenberg KT, Moreno
K, Shestowsky WS, Hiraiwa M, Sabbadini R and Huxford T: The crystal
structure of sphingosine-1-phosphate in complex with a Fab fragment
reveals metal bridging of an antibody and its antigen. Proc Natl
Acad Sci USA. 106:17717–17722. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hla T, Lee MJ, Ancellin N, Paik JH and
Kluk MJ: Lysophospholipids - receptor revelations. Science.
294:1875–1878. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Anliker B and Chun J: Lysophospholipid G
protein-coupled receptors. J Biol Chem. 279:20555–20558. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Strub GM, Paillard M, Liang J, Gomez L,
Allegood JC, Hait NC, Maceyka M, Price MM, Chen Q, Simpson DC, et
al: Sphingosine-1-phosphate produced by sphingosine kinase 2 in
mitochondria interacts with prohibitin 2 to regulate complex IV
assembly and respiration. FASEB J. 25:600–612. 2011. View Article : Google Scholar :
|
|
28
|
Alvarez SE, Harikumar KB, Hait NC,
Allegood J, Strub GM, Kim EY, Maceyka M, Jiang H, Luo C, Kordula T,
et al: Sphingosine-1-phosphate is a missing cofactor for the E3
ubiquitin ligase TRAF2. Nature. 465:1084–1088. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hait NC, Allegood J, Maceyka M, Strub GM,
Harikumar KB, Singh SK, Luo C, Marmorstein R, Kordula T, Milstien
S, et al: Regulation of histone acetylation in the nucleus by
sphingosine-1-phosphate. Science. 325:1254–1257. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Xia P and Wadham C: Sphingosine
1-phosphate, a key mediator of the cytokine network: Juxtacrine
signaling. Cytokine Growth Factor Rev. 22:45–53. 2011. View Article : Google Scholar
|
|
31
|
Mandala SM, Thornton R, Galve-Roperh I,
Poulton S, Peterson C, Olivera A, Bergstrom J, Kurtz MB and Spiegel
S: Molecular cloning and characterization of a lipid
phosphohydrolase that degrades sphingosine-1- phosphate and induces
cell death. Proc Natl Acad Sci USA. 97:7859–7864. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ogawa C, Kihara A, Gokoh M and Igarashi Y:
Identification and characterization of a novel human
sphingosine-1-phosphate phosphohydrolase, hSPP2. J Biol Chem.
278:1268–1272. 2003. View Article : Google Scholar
|
|
33
|
Mandala SM: Sphingosine-1-phosphate
phosphatases. Prostaglandins. 64:143–156. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Venkataraman K, Lee YM, Michaud J,
Thangada S, Ai Y, Bonkovsky HL, Parikh NS, Habrukowich C and Hla T:
Vascular endothelium as a contributor of plasma sphingosine
1-phosphate. Circ Res. 102:669–676. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lépine S, Allegood JC, Park M, Dent P,
Milstien S and Spiegel S: Sphingosine-1-phosphate
phosphohydrolase-1 regulates ER stress-induced autophagy. Cell
Death Differ. 18:350–361. 2011. View Article : Google Scholar :
|
|
36
|
Peter BF, Lidington D, Harada A, Bolz HJ,
Vogel L, Heximer S, Spiegel S, Pohl U and Bolz SS: Role of
sphingosine-1-phosphate phosphohydrolase 1 in the regulation of
resistance artery tone. Circ Res. 103:315–324. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Cervantes A, Roselló S, Roda D and
Rodríguez-Braun E: The treatment of advanced gastric cancer:
Current strategies and future perspectives. Ann Oncol. 19(Suppl 5):
v103–v107. 2008. View Article : Google Scholar : PubMed/NCBI
|