Several mutations in genes encoding chromatin
remodeling complexes have been found in recent years using
comprehensive genome-wide analyses with next-generation sequencers.
Chromatin remodeling is a molecular mechanism of regulation of gene
expression levels based on changes to chromatin structure; that is,
regulation of the interaction of proteins with double-stranded DNA
by changing the nucleosome structure in an ATP-dependent manner.
This mechanism has impacts on transcription, replication, repair,
methylation, and recombination of DNA (1). Dysfunction in the mechanism is likely
to contribute to carcinogenesis, and aberrations in chromatin
remodeling have been found in approximately 10% of all human
cancers (2). Chromatin remodeling
complexes alter the structure of nucleosomes by local ATP-dependent
sliding of nucleosomes or by modification of histones (3,4). In
sliding, the loosened chromatin structures appear to facilitate
binding of proteins to double-stranded DNA, while the mechanism of
histone modification is unclear (3). Chromatin remodeling complexes are also
predicted to be involved in regulation of higher-order chromatin
structures.
There are several types of chromatin remodeling
complexes, including the SWItch/sucrose non-fermentable (SWI/SNF)
complex, imitation SWI (ISWI) complex, INO80 complex and
chromodomain helicase DNA-binding protein (CHD) complex. The
SWI/SNF complex is involved in activation or inhibition of
transcription, and plays a crucial role in carcinogenesis. Isakoff
et al showed that inactivation of SNF5p (SNF5)
in murine fibroblasts leads to both increased and decreased
expression of genes (5).
SNF5 encodes SNF5, a core member of the SWI/SNF complex, and
these results suggest that the SWI/SNF complex is involved in
activation and inhibition of transcription. Medina et al
found that ectopic expression of SWI/SNF related, matrix
associated, actin dependent regulator of chromatin subfamily a,
member 4 (SMARCA4) in SMARCA4-deficient cells
altered expression of ~1% of all genes (6). SMARCA4 encodes BRG1, which is
also a core member of the SWI/SNF complex, and these findings
suggest that the SWI/SNF complex induces changes in gene expression
and may play a crucial role in carcinogenesis.
The SWI/SNF complex is composed of many subunits,
including an ATP-dependent catalytic subunit and a core subunit
that is involved in construction of the complex and contains ARID1A
(7–11). In this review, we focus on the
relationships of ARID1A mutations with ovarian and
endometrial cancers, and we discuss the possible use of ARID1A as a
molecular target in diagnosis and treatment.
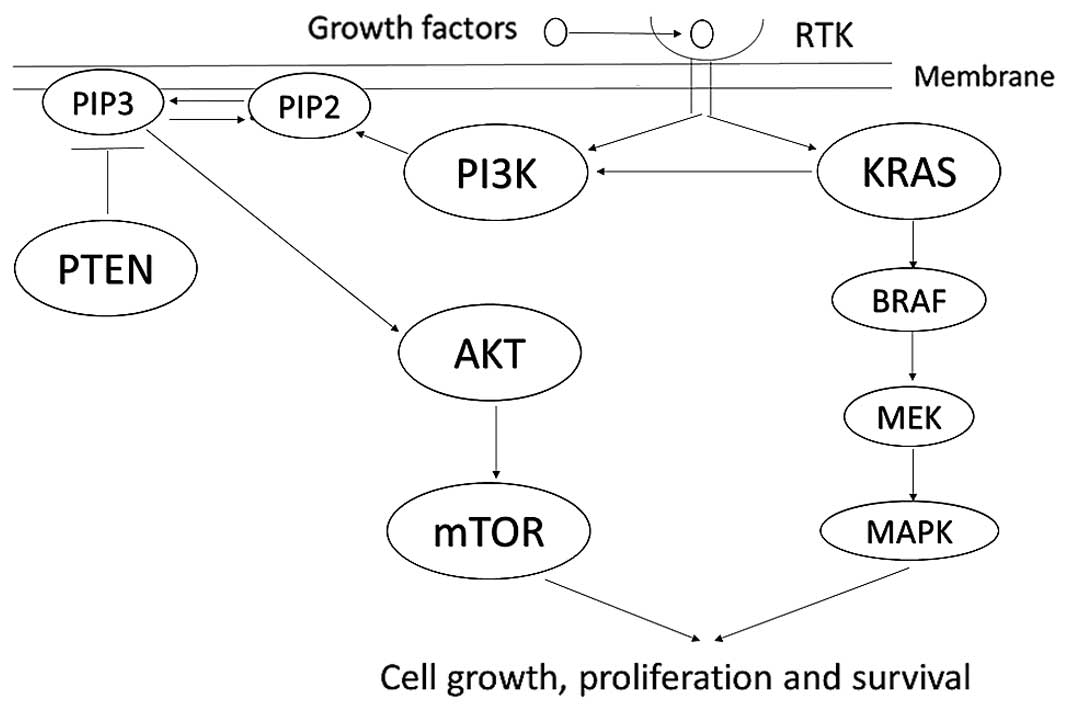
An association between loss of ARID1A protein
expression and activation of the PI3K/AKT pathway has also been
found in type I endometrial carcinomas. ARID1A mutations are
present in 40% of low-grade endometrioid adenocarcinomas, and loss
of ARID1A expression occurs in 26–29% of low-grade and 39% of
high-grade endometrioid adenocarcinomas (32,49).
Moreover, in a classification of endometrial carcinomas based on
mutations in 9 genes, including ARID1A, PTEN,
PIK3CA, KRAS, P53 and BRAF,
ARID1A mutation was detected in 47% of low-grade
endometrioid adenocarcinomas, 60% of high-grade endometrioid
adenocarcinomas, 11% of serous adenocarcinomas, and 24% of
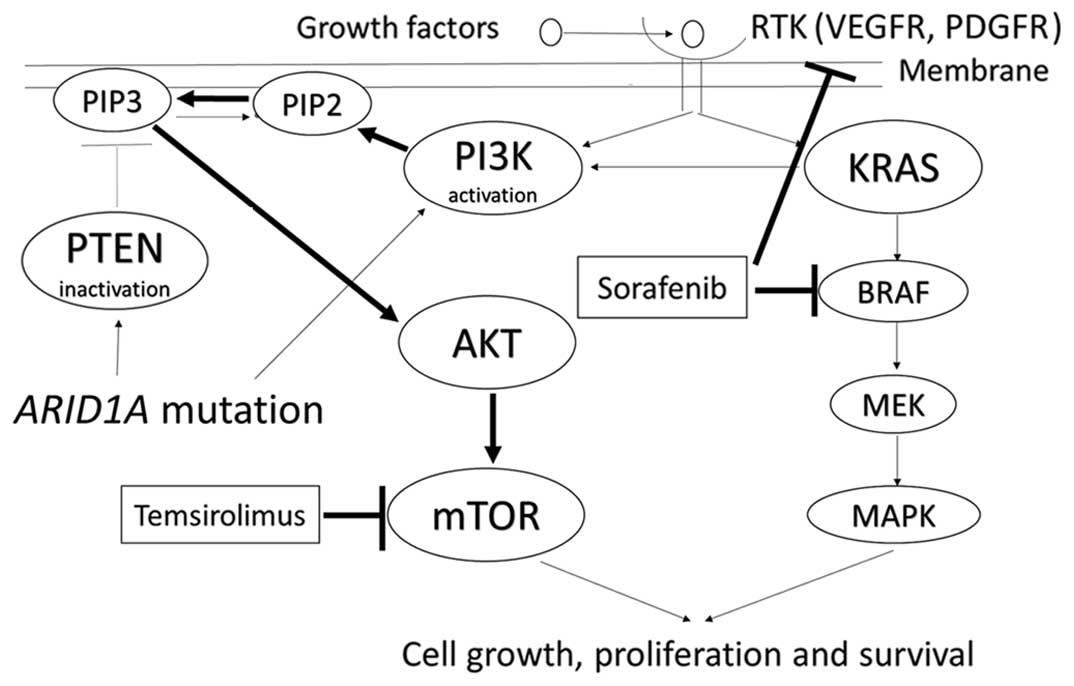
carcinosarcomas (50). Mutations of
PTEN and PIK3CA also frequently occur in uterine
endometrial carcinomas with ARID1A mutation, and these
mutations induce aberrant activation of PI3K, phosphorylation of
AKT, and inhibition of cell survival and apoptosis (51).
Another characteristic of type I endometrial
carcinomas is induction of microsatellite instability (MSI). The
cause of MSI may be a defect in DNA mismatch repair function, and
loss of ARID1A expression may be associated with MSI in uterine
endometrioid adenocarcinomas. Bosse et al found a strong
association between ARID1A loss and sporadic MSI, and concluded
that ARID1A may be a causative gene for MSI through a role in
epigenetic silencing of the mutL homolog 1 (MLH1)
gene in endometrial cancer (52).
In addition to its role in cancer development,
ARID1A may also have a crucial role in progression of cancer. In
immunohistochemical staining of atypical endometrial hyperplasia
and uterine endometrioid carcinomas with an anti-ARID1A antibody,
Mao et al defined the lack of staining in focal tumor areas
as 'clonal loss', whereas the absence of ARID1A immunoreactivity in
almost all tumor cells was defined as 'complete loss'. Clonal loss
occurred at rates of 16% in atypical endometrial hyperplasia, 24%
in uterine low-grade endometrioid carcinomas and 9% in uterine
high-grade endometrioid carcinomas, whereas the respective rates of
complete loss were 0, 25 and 44% in these diseases (53). This suggests that loss of ARID1A
expression plays important roles in the early phase of tumor
development and progression.
Uterine endometrial clear cell carcinoma (UCCC) is a
rare disease that accounts for <5% of all endometrial
carcinomas. The genetic basis of UCCC is mostly unknown, but
downregulation of ARID1A has been found in 14–22% of UCCC cases,
with these rates being lower than those in ovarian clear cell
carcinoma (54–57).
A novel treatment strategy directly targeting
enhancer of zeste homolog 2 (EZH2) has recently been reported. EZH2
is often overexpressed in ovarian clear cell adenocarcinomas and
generates the lysine 27 trimethylation on histone H3. GSK126, a
small molecule and highly selective inhibitor of EZH2
methyltransferase, dose-dependently decreases the level of H3K27Me3
in ovarian clear cell adenocarcinoma cells with loss of
ARID1A expression and inhibits their growth (63). The effect of GSK126 is reduced when
expression of ARID1A is restored in these cells. An
association with PI3K-interacting protein 1 gene (PIK3IP1),
a direct target of ARID1A and EZH2 that is also often
mutated in ovarian clear cell adenocarcinoma with ARID1A
mutations. Mutation of ARID1A is related to reduced
expression of PIK3IP1, and administration of GSK126 or restoration
of ARID1A expression led to increased expression of PIK3IP1.
GSK126 suppresses EZH2, and thus has the opposite effect of
ARID1A or EZH2. Both ARID1A and EZH2 act on PIK3IP1,
but ARID1A is more dominant than EZH2. With PIK3IP1
overexpression, PIK3IP1 inhibits cell proliferation and induces
apoptosis in ovarian clear cell adenocarcinomas. Thus,
ARID1A or EZH2 regulate expression of PIK3IP1
and a high rate of mutation of these genes in ovarian clear cell
adenocarcinoma enhances cell proliferation and anti-apoptotic
effects. GSK126 is a molecular-targeted drug that should inhibit
proliferation of ARID1A-mutated ovarian clear cell
adenocarcinoma cells by targeting and inhibiting EZH2. In mice,
GSK126 also affects peritoneal dissemination (63). In the present study, the number of
tumors after treatment with GSK126 was significantly lower than
that in untreated mice after ARID1A-mutated ovarian clear
cell adenocarcinoma cells were injected into the abdominal cavity
(63). Based on all of these
findings, GSK126 is likely to be among the most efficient
molecular-targeted drugs against ovarian clear cell adenocarcinoma
with ARID1A mutations.
Associations between ARID1A expression and prognosis
have recently been reported in stomach cancer, bladder cancer,
bowel cancer, and renal cell cancer, which suggests that
ARID1A expression may serve as a prognostic marker (65–68).
Meta-analysis also confirmed loss of ARID1A is associated
with cancer-specific mortality and cancer recurrence (34). However, this association has only
rarely been reported in gynecologic cancers, including in a
clinically advanced stage and with tumor progression in uterus
endometrioid adenocarcinomas (53).
Thus, the association of ARID1A and prognosis in UCCC
remains uncertain (55–57).
On the contrary, in a study conducted between 2006
and 2011 in 46 patients with International Federation of Gynecology
and Obstetrics (FIGO) stage (1988) III and IV epithelial ovarian
cancers, Yokoyama et al found that the expression level of
ARID1A was correlated with prognosis after chemotherapy.
Twelve patients with a significantly lower level of ARID1A
expression did not achieve complete response (CR). Of 34 patients
who achieved CR, 21 patients who subsequently relapsed had
relatively low levels of ARID1A (69). In addition, shorter progression-free
survival after chemotherapy was found in the 11 patients with
complete loss of ARID1A expression compared to 35 patients with
ARID1A expression (69). In 112
patients with ovarian clear cell adenocarcinoma, Itamochi et
al found an association between ARID1A expression and
prognosis, and a relationship between ARID1A expression and each
FIGO (1988) stage (70). Thus, the
5-year survival rate for FIGO stage I or II patients with positive
tumor expression of ARID1A was 91%, while that for patients with
negative tumor expression of ARID1A was 74%. However, this
difference was not observed in FIGO stages III or IV. Based on
these findings, ARID1A may be a biomarker that is predictive of
prognosis of patients with FIGO stage I and II ovarian clear cell
adenocarcinoma (70).
Advances in comprehensive genome analysis have
permitted identification of mutations in multiple genes encoding
chromatin remodeling factors in human cancers. Genes encoding
proteins making up the SWI/SNF chromatin remodeling complex have
been found to have particularly inactivating mutations at high
frequency, and this complex has been suggested to inhibit malignant
transformation. One such gene is ARID1A, and ARID1A
mutations that eliminate expression of ARID1A protein produce
abnormalities in chromatin remodeling and contribute to canceration
from endometriosis to endometriosis-associated ovarian cancers.
Since chromatin remodeling is involved in regulation of expression
of multiple genes and in genome instability, its dysregulation is
likely to have multiphase and significant impacts on development,
survival, and progression of endometriosis, but the detailed
mechanisms remain unclear. Further studies are needed to determine
the mechanism of chromatin remodeling dysregulation initiated by
ARID1A mutation, to develop methods for early diagnosis via
detection of ARID1A, to investigate new cancer therapy
targeting ARID1A, and to examine the involvement of
ARID1A mutations in development, survival and progression of
cancer cells.
We thank Dr K. Kitagawa, Dr Y. Ohfuji and Dr M.
Hayakawa for helpful assistance. The authors gratefully acknowledge
grant support from the Medical Research Encouragement Prize of The
Japan Medical Association and from the Keio Gijyuku Academic
Development Fund. The funders had no role in data collection and
analysis, decision to publish, or preparation of the
manuscript.
|
1
|
Clapier CR and Cairns BR: The biology of
chromatin remodeling complexes. Annu Rev Biochem. 78:273–304. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vogelstein B, Papadopoulos N, Velculescu
VE, Zhou S, Diaz LA Jr and Kinzler KW: Cancer genome landscapes.
Science. 339:1546–1558. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Saha A, Wittmeyer J and Cairns BR:
Chromatin remodelling: The industrial revolution of DNA around
histones. Nat Rev Mol Cell Biol. 7:437–447. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lorch Y, Maier-Davis B and Kornberg RD:
Mechanism of chromatin remodeling. Proc Natl Acad Sci USA.
107:3458–3462. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Isakoff MS, Sansam CG, Tamayo P,
Subramanian A, Evans JA, Fillmore CM, Wang X, Biegel JA, Pomeroy
SL, Mesirov JP, et al: Inactivation of the Snf5 tumor suppressor
stimulates cell cycle progression and cooperates with p53 loss in
oncogenic transformation. Proc Natl Acad Sci USA. 102:17745–17750.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Medina PP, Carretero J, Ballestar E,
Angulo B, Lopez-Rios F, Esteller M and Sanchez-Cespedes M:
Transcriptional targets of the chromatin-remodelling factor
SMARCA4/BRG1 in lung cancer cells. Hum Mol Genet. 14:973–982. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mohrmann L and Verrijzer CP: Composition
and functional specificity of SWI2/SNF2 class chromatin remodeling
complexes. Biochim Biophys Acta. 1681:59–73. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wang W, Côté J, Xue Y, Zhou S, Khavari PA,
Biggar SR, Muchardt C, Kalpana GV, Goff SP, Yaniv M, et al:
Purification and biochemical heterogeneity of the mammalian SWI-SNF
complex. EMBO J. 15:5370–5382. 1996.PubMed/NCBI
|
|
9
|
Phelan ML, Sif S, Narlikar GJ and Kingston
RE: Reconstitution of a core chromatin remodeling complex from
SWI/SNF subunits. Mol Cell. 3:247–253. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kaeser MD, Aslanian A, Dong MQ, Yates JR
III and Emerson BM: BRD7, a novel PBAF-specific SWI/SNF subunit, is
required for target gene activation and repression in embryonic
stem cells. J Biol Chem. 283:32254–32263. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wang X, Nagl NG Jr, Wilsker D, Van Scoy M,
Pacchione S, Yaciuk P, Dallas PB and Moran E: Two related ARID
family proteins are alternative subunits of human SWI/SNF
complexes. Biochem J. 383:319–325. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chunder N, Mandal S, Basu D, Roy A,
Roychoudhury S and Panda CK: Deletion mapping of chromosome 1 in
early onset and late onset breast tumors - a comparative study in
eastern India. Pathol Res Pract. 199:313–321. 2003. View Article : Google Scholar
|
|
13
|
Varela I, Tarpey P, Raine K, Huang D, Ong
CK, Stephens P, Davies H, Jones D, Lin ML, Teague J, et al: Exome
sequencing identifies frequent mutation of the SWI/SNF complex gene
PBRM1 in renal carcinoma. Nature. 469:539–542. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jones S, Li M, Parsons DW, Zhang X,
Wesseling J, Kristel P, Schmidt MK, Markowitz S, Yan H, Bigner D,
et al: Somatic mutations in the chromatin remodeling gene ARID1A
occur in several tumor types. Hum Mutat. 33:100–103. 2012.
View Article : Google Scholar
|
|
15
|
Zang ZJ, Cutcutache I, Poon SL, Zhang SL,
McPherson JR, Tao J, Rajasegaran V, Heng HL, Deng N, Gan A, et al:
Exome sequencing of gastric adenocarcinoma identifies recurrent
somatic mutations in cell adhesion and chromatin remodeling genes.
Nat Genet. 44:570–574. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gui Y, Guo G, Huang Y, Hu X, Tang A, Gao
S, Wu R, Chen C, Li X, Zhou L, et al: Frequent mutations of
chromatin remodeling genes in transitional cell carcinoma of the
bladder. Nat Genet. 43:875–878. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Agrawal N, Jiao Y, Bettegowda C, Hutfless
SM, Wang Y, David S, Cheng Y, Twaddell WS, Latt NL, Shin EJ, et al:
Comparative genomic analysis of esophageal adenocarcinoma and
squamous cell carcinoma. Cancer Discov. 2:899–905. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Streppel MM, Lata S, DelaBastide M,
Montgomery EA, Wang JS, Canto MI, Macgregor-Das AM, Pai S, Morsink
FH, Offerhaus GJ, et al: Next-generation sequencing of endoscopic
biopsies identifies ARID1A as a tumor-suppressor gene in Barrett's
esophagus. Oncogene. 33:347–357. 2014. View Article : Google Scholar
|
|
19
|
Huang J, Deng Q, Wang Q, Li KY, Dai JH, Li
N, Zhu ZD, Zhou B, Liu XY, Liu RF, et al: Exome sequencing of
hepatitis B virus-associated hepatocellular carcinoma. Nat Genet.
44:1117–1121. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Fujimoto A, Totoki Y, Abe T, Boroevich KA,
Hosoda F, Nguyen HH, Aoki M, Hosono N, Kubo M, Miya F, et al:
Whole-genome sequencing of liver cancers identifies etiological
influences on mutation patterns and recurrent mutations in
chromatin regulators. Nat Genet. 44:760–764. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dulak AM, Stojanov P, Peng S, Lawrence MS,
Fox C, Stewart C, Bandla S, Imamura Y, Schumacher SE, Shefler E, et
al: Exome and whole-genome sequencing of esophageal adenocarcinoma
identifies recurrent driver events and mutational complexity. Nat
Genet. 45:478–486. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Imielinski M, Berger AH, Hammerman PS,
Hernandez B, Pugh TJ, Hodis E, Cho J, Suh J, Capelletti M,
Sivachenko A, et al: Mapping the hallmarks of lung adenocarcinoma
with massively parallel sequencing. Cell. 150:1107–1120. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shain AH, Giacomini CP, Matsukuma K,
Karikari CA, Bashyam MD, Hidalgo M, Maitra A and Pollack JR:
Convergent structural alterations define SWItch/Sucrose
NonFermentable (SWI/SNF) chromatin remodeler as a central tumor
suppressive complex in pancreatic cancer. Proc Natl Acad Sci USA.
109:E252–E259. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Biankin AV, Waddell N, Kassahn KS, Gingras
MC, Muthuswamy LB, Johns AL, Miller DK, Wilson PJ, Patch AM, Wu J,
et al: Australian Pancreatic Cancer Genome Initiative: Pancreatic
cancer genomes reveal aberrations in axon guidance pathway genes.
Nature. 491:399–405. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cornen S, Adelaide J, Bertucci F, Finetti
P, Guille A, Birnbaum DJ, Birnbaum D and Chaffanet M: Mutations and
deletions of ARID1A in breast tumors. Oncogene. 31:4255–4256. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Stephens PJ, Tarpey PS, Davies H, Van Loo
P, Greenman C, Wedge DC, Nik-Zainal S, Martin S, Varela I, Bignell
GR, et al: Oslo Breast Cancer Consortium (OSBREAC): The landscape
of cancer genes and mutational processes in breast cancer. Nature.
486:400–404. 2012.PubMed/NCBI
|
|
27
|
Giulino-Roth L, Wang K, MacDonald TY,
Mathew S, Tam Y, Cronin MT, Palmer G, Lucena-Silva N, Pedrosa F,
Pedrosa M, et al: Targeted genomic sequencing of pediatric Burkitt
lymphoma identifies recurrent alterations in antiapoptotic and
chromatin-remodeling genes. Blood. 120:5181–5184. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Love C, Sun Z, Jima D, Li G, Zhang J,
Miles R, Richards KL, Dunphy CH, Choi WW, Srivastava G, et al: The
genetic landscape of mutations in Burkitt lymphoma. Nat Genet.
44:1321–1325. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sausen M, Leary RJ, Jones S, Wu J,
Reynolds CP, Liu X, Blackford A, Parmigiani G, Diaz LA Jr,
Papadopoulos N, et al: Integrated genomic analyses identify ARID1A
and ARID1B alterations in the childhood cancer neuroblastoma. Nat
Genet. 45:12–17. 2013. View Article : Google Scholar :
|
|
30
|
Jones S, Wang TL, Shih IeM, Mao TL,
Nakayama K, Roden R, Glas R, Slamon D, Diaz LA Jr, Vogelstein B, et
al: Frequent mutations of chromatin remodeling gene ARID1A in
ovarian clear cell carcinoma. Science. 330:228–231. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wiegand KC, Shah SP, Al-Agha OM, Zhao Y,
Tse K, Zeng T, Senz J, McConechy MK, Anglesio MS, Kalloger SE, et
al: ARID1A mutations in endometriosis-associated ovarian
carcinomas. N Engl J Med. 363:1532–1543. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Guan B, Mao TL, Panuganti PK, Kuhn E,
Kurman RJ, Maeda D, Chen E, Jeng YM, Wang TL and Shih IeM: Mutation
and loss of expression of ARID1A in uterine low-grade endometrioid
carcinoma. Am J Surg Pathol. 35:625–632. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Guan B, Gao M, Wu C-H, Wang T-L and Shih
IeM: Functional analysis of in-frame indel ARID1A mutations reveals
new regulatory mechanisms of its tumor suppressor functions.
Neoplasia. 14:986–993. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Luchini C, Veronese N, Solmi M, Cho H, Kim
J-H, Chou A, Gill AJ, Faraj SF, Chaux A, Netto GJ, et al:
Prognostic role and implications of mutation status of tumor
suppressor gene ARID1A in cancer: A systematic review and
meta-analysis. Oncotarget. Sept 8–2015.Epub ahead of print.
PubMed/NCBI
|
|
35
|
Guan B, Wang TL and Shih IeM: ARID1A, a
factor that promotes formation of SWI/SNF-mediated chromatin
remodeling, is a tumor suppressor in gynecologic cancers. Cancer
Res. 71:6718–6727. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yamamoto S, Tsuda H, Takano M, Tamai S and
Matsubara O: Loss of ARID1A protein expression occurs as an early
event in ovarian clear-cell carcinoma development and frequently
coexists with PIK3CA mutations. Mod Pathol. 25:615–624. 2012.
View Article : Google Scholar
|
|
37
|
Veras E, Mao TL, Ayhan A, Ueda S, Lai H,
Hayran M, Shih IeM and Kurman RJ: Cystic and adenofibromatous clear
cell carcinomas of the ovary: distinctive tumors that differ in
their pathogenesis and behavior: a clinicopathologic analysis of
122 cases. Am J Surg Pathol. 33:844–853. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Wu CH, Mao TL, Vang R, Ayhan A, Wang TL,
Kurman RJ and Shih IeM: Endocervical-type mucinous borderline
tumors are related to endometrioid tumors based on mutation and
loss of expression of ARID1A. Int J Gynecol Pathol. 31:297–303.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ayhan A, Mao TL, Seckin T, Wu CH, Guan B,
Ogawa H, Futagami M, Mizukami H, Yokoyama Y, Kurman RJ, et al: Loss
of ARID1A expression is an early molecular event in tumor
progression from ovarian endometriotic cyst to clear cell and
endometrioid carcinoma. Int J Gynecol Cancer. 22:1310–1315. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Vercellini P, Crosignani P, Somigliana E,
Viganò P, Buggio L, Bolis G and Fedele L: The 'incessant
menstruation' hypothesis: A mechanistic ovarian cancer model with
implications for prevention. Hum Reprod. 26:2262–2273. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yamaguchi K, Mandai M, Toyokuni S,
Hamanishi J, Higuchi T, Takakura K and Fujii S: Contents of
endometriotic cysts, especially the high concentration of free
iron, are a possible cause of carcinogenesis in the cysts through
the iron-induced persistent oxidative stress. Clin Cancer Res.
14:32–40. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Guan B, Rahmanto YS, Wu R-C, Wang Y, Wang
Z, Wang T-L and Shih IeM: Roles of deletion of Arid1a, a tumor
suppressor, in mouse ovarian tumorigenesis. J Natl Cancer Inst.
106:dju1462014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Tanwar PS, Kaneko-Tarui T, Lee HJ, Zhang L
and Teixeira JM: PTEN loss and HOXA10 expression are associated
with ovarian endometrioid adenocarcinoma differentiation and
progression. Carcinogenesis. 34:893–901. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kuo KT, Mao TL, Jones S, Veras E, Ayhan A,
Wang TL, Glas R, Slamon D, Velculescu VE, Kuman RJ, et al: Frequent
activating mutations of PIK3CA in ovarian clear cell carcinoma. Am
J Pathol. 174:1597–1601. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Yamamoto S, Tsuda H, Takano M, Iwaya K,
Tamai S and Matsubara O: PIK3CA mutation is an early event in the
development of endometriosis-associated ovarian clear cell
adenocarcinoma. J Pathol. 225:189–194. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yamamoto S, Tsuda H, Takano M, Tamai S and
Matsubara O: PIK3CA mutations and loss of ARID1A protein expression
are early events in the development of cystic ovarian clear cell
adenocarcinoma. Virchows Arch. 460:77–87. 2012. View Article : Google Scholar
|
|
47
|
Cheung LW, Hennessy BT, Li J, Yu S, Myers
AP, Djordjevic B, Lu Y, Stemke-Hale K, Dyer MD, Zhang F, et al:
High frequency of PIK3R1 and PIK3R2 mutations in endometrial cancer
elucidates a novel mechanism for regulation of PTEN protein
stability. Cancer Discov. 1:170–185. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Llobet D, Pallares J, Yeramian A,
Santacana M, Eritja N, Velasco A, Dolcet X and Matias-Guiu X:
Molecular pathology of endometrial carcinoma: Practical aspects
from the diagnostic and therapeutic viewpoints. J Clin Pathol.
62:777–785. 2009. View Article : Google Scholar
|
|
49
|
Wiegand KC, Lee AF, Al-Agha OM, Chow C,
Kalloger SE, Scott DW, Steidl C, Wiseman SM, Gascoyne RD, Gilks B,
et al: Loss of BAF250a (ARID1A) is frequent in high-grade
endometrial carcinomas. J Pathol. 224:328–333. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
McConechy MK, Ding J, Cheang MC, Wiegand
KC, Senz J, Tone AA, Yang W, Prentice LM, Tse K, Zeng T, et al: Use
of mutation profiles to refine the classification of endometrial
carcinomas. J Pathol. 228:20–30. 2012.PubMed/NCBI
|
|
51
|
Liang H, Cheung LW, Li J, Ju Z, Yu S,
Stemke-Hale K, Dogruluk T, Lu Y, Liu X, Gu C, et al: Whole-exome
sequencing combined with functional genomics reveals novel
candidate driver cancer genes in endometrial cancer. Genome Res.
22:2120–2129. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Bosse T, ter Haar NT, Seeber LM, v Diest
PJ, Hes FJ, Vasen HF, Nout RA, Creutzberg CL, Morreau H and Smit
VT: Loss of ARID1A expression and its relationship with PI3K-Akt
pathway alterations, TP53 and microsatellite instability in
endometrial cancer. Mod Pathol. 26:1525–1535. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Mao TL, Ardighieri L, Ayhan A, Kuo KT, Wu
CH, Wang TL and Shih IeM: Loss of ARID1A expression correlates with
stages of tumor progression in uterine endometrioid carcinoma. Am J
Surg Pathol. 37:1342–1348. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Hoang LN, McConechy MK, Meng B, McIntyre
JB, Ewanowich C, Gilks CB, Huntsman DG, Köbel M and Lee CH:
Targeted mutation analysis of endometrial clear cell carcinoma.
Histopathology. 66:664–674. 2015. View Article : Google Scholar
|
|
55
|
Fadare O, Renshaw IL and Liang SX: Does
the loss of ARID1A (BAF-250a) expression in endometrial clear cell
carcinomas have any clinicopathologic significance? A pilot
assessment. J Cancer. 3:129–136. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Zhang ZM, Xiao S, Sun GY, Liu YP, Zhang
FH, Yang HF, Li J, Qiu HB, Liu Y, Zhang C, et al: The
clinicopathologic significance of the loss of BAF250a (ARID1A)
expression in endometrial carcinoma. Int J Gynecol Cancer.
24:534–540. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Fadare O, Gwin K, Desouki MM, Crispens MA,
Jones HW III, Khabele D, Liang SX, Zheng W, Mohammed K, Hecht JL,
et al: The clinicopathologic significance of p53 and BAF-250a
(ARID1A) expression in clear cell carcinoma of the endometrium. Mod
Pathol. 26:1101–1110. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
van Nagell JR Jr and Hoff JT: Transvaginal
ultrasonography in ovarian cancer screening: Current perspectives.
Int J Womens Health. 6:25–33. 2013. View Article : Google Scholar :
|
|
59
|
Takano M, Kikuchi Y, Kudoh K, Goto T,
Furuya K, Kikuchi R, Kita T, Fujiwara K, Shiozawa T and Aoki D:
Weekly administration of temsirolimus for heavily pretreated
patients with clear cell carcinoma of the ovary: A report of six
cases. Int J Clin Oncol. 16:605–609. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Scott JD and Williams RM: Chemistry and
biology of the tetrahydroisoquinoline antitumor antibiotics. Chem
Rev. 102:1669–1730. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Kwan JC and Luesch H: Weapons in disguise
- activating mechanisms and protecting group chemistry in nature.
Chemistry. 16:13020–13029. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Rahman M, Nakayama K, Ishibashi T,
Ishikawa M, Rahman MT, Katagiri H, Katagiri A, Iida K, Kikuchi Y
and Miyazaki K: A case of stage III c ovarian clear cell carcinoma:
The role for predictive biomarkers and targeted therapies. Int J
Mol Sci. 14:6067–6073. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Bitler BG, Aird KM, Garipov A, Li H,
Amatangelo M, Kossenkov AV, Schultz DC, Liu Q, Shih IeM,
Conejo-Garcia JR, et al: Synthetic lethality by targeting EZH2
methyltransferase activity in ARID1A-mutated cancers. Nat Med.
1:231–238. 2015.
|
|
64
|
Helming KC, Wang X, Wilson BG, Vazquez F,
Haswell JR, Manchester HE, Kim Y, Kryukov GV, Ghandi M, Aguirre AJ,
et al: ARID1B is a specific vulnerability in ARID1A-mutant cancers.
Nat Med. 20:251–254. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Park JH, Lee C, Suh JH, Chae JY, Kim HW
and Moon KC: Decreased ARID1A expression correlates with poor
prognosis of clear cell renal cell carcinoma. Hum Pathol.
46:454–460. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Wei XL, Wang DS, Xi SY, Wu WJ, Chen DL,
Zeng ZL, Wang RY, Huang YX, Jin Y, Wang F, et al: Clinicopathologic
and prognostic relevance of ARID1A protein loss in colorectal
cancer. World J Gastroenterol. 20:18404–18412. 2014. View Article : Google Scholar
|
|
67
|
Faraj SF, Chaux A, Gonzalez-Roibon N,
Munari E, Ellis C, Driscoll T, Schoenberg MP, Bivalacqua TJ, Shih
IeM and Netto GJ: ARID1A immunohistochemistry improves outcome
prediction in invasive urothelial carcinoma of urinary bladder. Hum
Pathol. 45:2233–2239. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Wiegand KC, Sy K, Kalloger SE, Li-Chang H,
Woods R, Kumar A, Streutker CJ, Hafezi-Bakhtiari S, Zhou C, Lim HJ,
et al: ARID1A/BAF250a as a prognostic marker for gastric carcinoma:
A study of 2 cohorts. Hum Pathol. 45:1258–1268. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Yokoyama Y, Matsushita Y, Shigeto T,
Futagami M and Mizunuma H: Decreased ARID1A expression is
correlated with chemoresistance in epithelial ovarian cancer. J
Gynecol Oncol. 25:58–63. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Itamochi H, Oumi N, Oishi T, Shoji T,
Fujiwara H, Sugiyama T, Suzuki M, Kigawa J and Harada T: Loss of
ARID1A expression is associated with poor prognosis in patients
with stage I/II clear cell carcinoma of the ovary. Int J Clin
Oncol. 20:967–973. 2015. View Article : Google Scholar : PubMed/NCBI
|