Introduction
Hepatitis B virus (HBV) infection is the most common
chronic viral infection worldwide, infecting ~2 billion
individuals, of which >350 million are chronic HBV carriers
(1). The development of
nucleos(t)ide analogs (NAs) has revolutionized the management of
chronic hepatitis B (CHB) in the last two decades (2). At present, five NAs have been approved
as antiviral therapies for CHB in Japan. These agents are
classified according to their chemical structures: Two nucleoside
analogs that include lamivudine (LAM) and entecavir (ETV), two
nucleotide analogs that include adefovir dipivoxil (ADV) and
tenofovir disoproxil fumarate (TDF) (3), and the newly approved tenofovir
alafenamide (TAF) (4-6).
NAs are known to effectively suppress HBV replication and reduce
the risk of disease progression and hepatic events (7). Long-term NA treatment has demonstrated
effectiveness in improving histological findings and reducing the
incidence of hepatocellular carcinoma (HCC) (8,9).
Although NAs are generally safe and comparatively free of major
side effects (10), renal and bone
toxicity may occur in a small yet significant proportion of
patients receiving older generation NAs, for example, ADV and TDF
(11). Given the high number of
patients receiving NAs worldwide, even a small risk of any of these
toxicities can be translated into a major medical issue. TAF was
approved in Japan for HBV treatment in 2017(12). Both TAF and TDF are phosphonamidite
prodrugs of tenofovir (TFV) that share the same intracellular
active metabolite, TFV diphosphate, which is effective against both
HBV and human immunodeficiency virus (HIV)-1 infection (13,14). TAF
has greater plasma stability, which allows for more efficient
uptake by hepatocytes at lower plasma concentrations than TDF;
thus, the circulating concentration of TFV is 90% lower after
administration of a 25 mg dose of TAF than after a 300 mg dose of
TDF (15). This difference likely
contributes to the relatively better safety profile of TAF compared
with TDF, particularly for renal and bone dysfunction. TAF was
shown to have less influence on the glomerular filtration rate
(GFR) and renal tubule function than TDF in international phase III
trials (4-6).
Long-term use of ADV and TDF has been reported, and there are
several cases where renal and tubular dysfunction and bone
metabolism abnormalities occurred (16-19).
At present, few studies have reported the effect of switching to
TAF after long-term use of other NAs (particularly the nucleotide
group). Thus, the present study aimed to evaluate the effect of TAF
(particularly on renal and tubular function) in patients with CHB
who had received NA treatment.
Materials and methods
Patients
The present retrospective, single-center study
included patients with chronic HBV infection. A total of 33
consecutive adult Japanese patients (mean age 61.5±8.7 years; 23
males and 10 females) who received TAF-based monotherapy (Vemlidy;
Gilead Sciences KK) or a combination rescue therapy (including LAM
and ETV combined) after using ADV and/or TDF between May 2017 and
March 2019 at Kurume University Hospital were recruited. The
exclusion criteria were as follows: i) Co-infection with HIV-1 or
hepatitis C virus; ii) other liver diseases such as autoimmune
hepatitis, alcoholic liver disease or metabolic liver disease; iii)
decompensated cirrhosis; and iv) terminal illness.
This study was performed in accordance with the
ethical principles described in the Declaration of Helsinki
(20) and was approved by the
Clinical Research Ethics Committee of Kurume University Hospital
(approval no. 17209). Written informed consent was obtained from
all patients.
Standard doses of LAM (100 mg/day), ADV (10 mg/day),
ETV (0.5 mg/day), TDF (300 mg/day) and TAF (25 mg/day) were
administered. The dosing interval of ADV and TDF was modified by
the attending physician (once every 2 days) when the estimated GFR
(eGFR) decreased to 50 ml/min/1.73 m2 or lower.
Study design
Biochemical (particularly renal tubular function and
phosphorus metabolism) and virological markers were assessed at the
start of TAF administration and 3 and 6 months after switching in
all 33 cases. The patients were divided into two groups: Long-term
NA administration (n=19) and short-term NA administration
(n=14).
In Japan, NA compounds received insurance approvals
at different times: LAM in 2000, ADV in 2004, ETV in 2006(21), TDF in 2014, and TAF in 2017.
Reflecting on the above grouping, all patients who received NA
treatment for ≥10 years were introduced with LAM and were included
in the long-term group. Conversely, all patients who received NA
therapy for <10 years were treated with an NA other than LAM and
were included in the short-term group. Changes in biological and
virological markers were compared between the two groups.
Data collection
All available medical records were evaluated
thoroughly. Body mass index was calculated as weight (kg) divided
by the square of height (m). Hypertension was defined as a clinical
systolic blood pressure ≥140 mmHg and/or clinical diastolic blood
pressure ≥90 mmHg, or the use of antihypertensive agents. Diabetes
mellitus was diagnosed if the fasting blood glucose levels were
>126 mg/dl or the HbA1c levels were >6.9%, according to the
Diagnostic Criteria for Diabetes Mellitus (22) or by the documented use of
antidiabetic agents or insulin. Blood and urine samples were
collected in the morning after an overnight fast. The renal
function was assessed by calculating the eGFR using the chronic
kidney disease (CKD) epidemiology collaboration formula (23). The renal tubular function was
assessed using a urine N-acetyl-β-D-glucosaminidase-creatinine
ratio and urine β2-microglobulin-creatinine (U-BMG/Cr) ratio. The
tubular metabolism of phosphates was assessed using a tubular
maximum for phosphate corrected for the GFR (TmP/GFR) and tubular
reabsorption of phosphate (TRP). TRP was calculated using the
following formula: TRP=(1-urine phosphate/urine creatinine)x(serum
creatinine/serum phosphate). The formula used to calculate TmP/GFR
is dependent on the value of TRP and can be calculated using the
following formulas: If TRP is ≤0.86, then TmP/GFR=TRP x serum
phosphate; if TRP is >0.86, then TmP/GFR=0.3x TRP/(1-0.8x TRP)x
serum phosphate (24).
Serum viral markers
The serum hepatitis B surface antigen (HBsAg) levels
were determined using a chemiluminescence immunoassay (LUMIPULSE
G1200 HBsAg-HQ assay kit; Fujirebio Inc.); the lower limit of
detection was 0.005 IU/ml. The serum HBV DNA levels were determined
using real-time TaqMan PCR assay (Cobas Taqman HBV test, Auto v2.0
kit, Roche Diagnostics, K.K); the lower limit of detection was 2.1
logcopies/ml. The serum hepatitis
B e antigen (HBeAg) and hepatitis B e antibody (HBeAb) levels were
determined using a chemiluminescence enzyme immunoassay (Architect
HBeAg; HBeAb assay kit; Abbott Laboratory; cat. no. 6C32).
Statistical analysis
All data are presented as the mean ± standard
deviation or as percentages. Differences between groups were
compared using a χ2 test or a Mann-Whitney U test, where
appropriate. All statistical analyses were performed using JMP Pro
version 13 (SAS Institute). P<0.05 was considered to indicate a
statistically significant difference.
Results
Baseline characteristics
Table I lists the
baseline clinical and laboratory characteristics at the start of
TAF therapy. In addition, Table SI
lists the treatment history with NAs in all cases. The mean age of
all patients was 61.5±8.7 years, and the majority of patients were
male (70%). Moreover, 9 (27%) patients had arterial hypertension
and 5 (15%) had diabetes mellitus. The mean duration of NA
treatment was 11.2±6.3 years. A total of 21 patients (64%) had a
history of ADV and 24 (73%) had a history of TDF treatment. The
mean total duration of ADV treatment was 9.8±3.0 years, and the
mean total duration of TDF treatment was 2.0±0.8 years. A total of
32 (97%) patients had chronic hepatitis and ADV had been
administered for ~10 years. In addition, the backgrounds of the
long-term and short-term administration groups were compared. A
significant difference was observed between the administration
periods of total NA (16.1±2.4 vs. 4.6±2.7 years; P<0.001) and
ADV (10.5±2.1 vs. 3.3±0.4; P=0.027). Similarly, the rates of NA
treatment history were different. Most patients with a history of
LAM and ADV treatment were included in the long-term group. Other
significant differences were found in the rates of hypertension (9
vs. 2; P<0.191) complications and HBeAg-positive (3 vs. 8;
P=0.0240). Conversely, no significant differences were found in the
other baseline characteristics amongst the two groups.
 | Table IBaseline characteristics of patients
receiving NA treatment. |
Table I
Baseline characteristics of patients
receiving NA treatment.
|
Parameterc | Total, n=33 | Long-term group,
n=19 | Short-term group,
n=14 |
P-valued |
|---|
| Age, years, | 62±9 | 61±10 | 62±9 | 0.9564 |
| Male: | 23 (70%): | 13 (68%): | 10 (71%): | 1.0000 |
| female (%) | 10 (30%) | 6 (32%) | 4 (29%) | |
| BMI,
kg/m2 | 21.8±2.9 | 21.7±2.3 | 22.0±3.6 | 0.7987 |
| With cirrhosis | 1 (3%) | 1 (5%) | 0 (0%) | 1.0000 |
| With
hypertension | 9 (27%) | 2 (11%) | 7 (50%) | 0.0191a |
| With diabetes
mellitus | 5 (15%) | 3 (16%) | 2 (14%) | 1.0000 |
| Latest NA regimen
for TAF-based therapy n (%) | | | | |
|
ADV
single | 1 (3%) | 1 (5%) | 0 (0%) | 1.0000 |
|
TDF
single | 11 (33%) | 2 (11%) | 9 (64%) | 0.0023a |
|
LAM
single | 0 (0%) | 0 (0%) | 0 (0%) | |
|
ETV
single | 0 (0%) | 0 (0%) | 0 (0%) | |
|
ADV +
LAM | 6 (18%) | 6 (32%) | 0 (0%) | 0.0272a |
|
ADV +
ETV | 2 (6%) | 1 (5%) | 1 (7%) | 1.0000 |
|
TDF +
LAM | 7 (21%) | 7 (37%) | 0 (0%) | 0.0126a |
|
TDF +
ETV | 6 (18%) | 2 (11%) | 4 (29%) | 0.3631 |
| Past NA treatment
before TAF-based therapy, n (%) | | | | |
|
ADV | 21 (64%) | 19 (100%) | 2 (14%) |
<0.0001b |
|
TDF | 24 (73%) | 11 (58%) | 13 (93%) | 0.0466 |
|
LAM | 19 (58%) | 19 (100%) | 0 (0%) |
<0.0001b |
|
ETV | 12 (36%) | 3 (16%) | 9 (64%) | 0.0091 |
| Duration of all NA
treatments, years | 11.2±6.3 | 16.1±2.4 | 4.6±2.7 |
<0.001b |
| Duration of prior
NA treatment, years | | | | |
|
ADV | 9.8±3.0 | 10.5±2.1 | 3.3±0.4 | 0.027a |
|
TDF | 2.0±0.8 | 1.8±0.8 | 2.2±0.8 | 0.2124 |
|
LAM | 13.5±4.0 | 13.5±4.0 | 0 |
<0.0001b |
|
ETV | 4.7±2.8 | 4.8±3.8 | 4.7±2.6 | 1.0000 |
| HBeAg-positive | 11 (33%) | 3 (33%) | 8 (57%) | 0.0240a |
| HBV DNA positive,
>1.3 Log IU/ml, n (%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| HBsAg, IU/ml | 1,126±1,724 | 590±641 | 1,853±2,400 | 0.0974 |
| AST, U/l | 24.9±7.7 | 25.5±9.5 | 24.1±4.3 | 0.7288 |
| ALT, U/l | 23.1±11.1 | 24.6±13.5 | 21.1±6.4 | 0.8695 |
| ALP, U/l | 320±126 | 324±141 | 298±86 | 0.7021 |
| BAP, µg/l | 19.7±9.0 | 21.1±11.0 | 17.9±5.1 | 0.6358 |
| Total bilirubin,
mg/dl | 0.9±0.3 | 0.9±0.3 | 0.9±0.4 | 0.8979 |
| Platelets,
x103/mm3 | 189±60 | 183±63 | 197±58 | 0.5599 |
| Creatinine,
mg/dl | 0.8±0.2 | 0.9±0.3 | 0.8±0.2 | 0.2743 |
| eGFR, ml/min/1.73
m2 | 73.4±13.7 | 68.4±17.5 | 77.9±18.1 | 0.1837 |
| Serum Ca,
mmol/l | 9.3±0.4 | 9.4±0.4 | 9.3±0.2 | 0.3158 |
| Serum P,
mmol/l | 3.1±0.5 | 3.1±0.6 | 3.1±0.5 | 0.9274 |
| U-BMG/Cr,
µg/g·Cre | 5,224±17,471 | 8,636±23,026 | 951±1,455 | 0.0558 |
| U-NAG/Cr,
U/g·Cre | 9.2±8.9 | 10.8±11.5 | 7.2±3.1 | 0.8698 |
| %TRP, % | 85.0±9.3 | 82.5±11.4 | 88.1±4.5 | 0.1719 |
| TmP/GFR, mg/dl | 2.6±0.6 | 2.6±0.7 | 2.7±0.5 | 0.5478 |
Time course observation of virological
markers and hepatobiliary enzymes
Table II shows the
time course of virological markers and hepatobiliary enzymes in all
33 cases after 3 and 6 months after switching to TAF. Regarding
virological markers, HBsAg significantly decreased after 6 months
(1,126±1,724 to 1,001±1,591 IU/ml; P<0.0001). As for
hepatobiliary enzymes, the serum ALP levels significantly improved
(320±126 to 283±124 U/l; P=0.028). In addition, the serum bone
specific alkaline phosphatase (BAP) level, an ALP isozyme derived
from bone (25,26), also improved after 6 months (19.7±9.0
to 17.7±8.0 µg/l; P=0.0006). Other virological markers and
hepatobiliary enzymes did not show any significant changes.
| Table IITime course observation of
virological markers and hepatobiliary enzyme levels. |
Table II
Time course observation of
virological markers and hepatobiliary enzyme levels.
|
Parametersd | Baseline | 3 months | 6 months |
P-valuee |
|---|
| Total, n=33 | | | | |
|
HBeAg-positive | 11 (33%) | 10 (30%) | 10 (30%) | 1.0000 |
|
HBV DNA
positive, >1.3 Log IU/ml | 0 (0%) | 0 (0%) | 0 (0%) | |
|
HBsAg,
IU/ml | 1,126±1,724 | 1,032±1,648 | 1,001±1,591 | 0.0001c |
|
AST,
U/l | 24.9±7.7 | 23.5±6.6 | 26.6±14.2 | 0.7459 |
|
ALT,
U/l | 23.1±11.1 | 22.6±12.4 | 24.5±14.5 | 0.5044 |
|
ALP,
U/l | 320±126 | 295±135 | 283±124 | 0.028a |
|
BAP,
µg/l | 19.7±9.0 | N/A | 17.7±8.0 | 0.0006c |
|
Total
bilirubin, mg/dl | 0.9±0.3 | 0.9±0.3 | 0.9±0.3 | 0.9821 |
| Long-term group,
n=19 | | | | |
|
HBsAg
IU/ml | 590±641 | 523±613 | 537±598 | 0.0108a |
|
AST,
U/l | 25.5±9.5 | 23.9±6.7 | 24.0±7.1 | 0.2982 |
|
ALT,
U/l | 24.6±13.5 | 23.5±15.3 | 22.2±12.4 | 0.1329 |
|
ALP,
U/l | 324±141 | 310±159 | 302±151 | 0.0281a |
|
BAP,
µg/l | 21.1±11.0 | N/A | 19.2±9.7 | 0.0678 |
| Total bilirubin,
mg/dl | 0.9±0.3 | 0.9±0.3 | 0.9±0.3 | 0.1221 |
| Short-term group,
n=14 | | | | |
|
HBsAg,
IU/ml | 1,853±2,400 | 1,796±2,350 | 1,631±2,235 | 0.004b |
|
AST,
U/l | 24.1±4.3 | 23.0±6.6 | 30.1±20.2 | 0.4121 |
|
ALT,
U/l | 21.1±6.4 | 21.2±6.1 | 27.6±16.9 | 0.5093 |
|
ALP,
U/l | 298±86 | 255±73 | 257±69 | 0.005b |
|
BAP,
µg/l | 17.9±5.1 | N/A | 15.5±4.6 | 0.0016b |
|
Total
bilirubin, mg/dl | 0.9±0.4 | 0.9±0.4 | 0.9±0.3 | 0.1016 |
Time course of observation of renal
and tubular function and phosphorus metabolism
Table III shows the
time course of renal and tubular functions and phosphorus
metabolism in all 33 cases. U-BMG/Cr, which is associated with
tubular function, was significantly improved after 6 months
(5,224±17,471 to 3,547±14,652 µg/g x Cre; P=0.002). Regarding other
renal and tubular functions, no significant changes in phosphorus
metabolism were noted, and no problematic adverse reactions were
observed after switching treatment regimens.
| Table IIITime course observation of renal and
tubular function, and phosphorus metabolism. |
Table III
Time course observation of renal and
tubular function, and phosphorus metabolism.
|
Parametersb | Baseline | 3 months | 6 months |
P-valuec |
|---|
| Total, n=33 | | | | |
|
Creatinine,
mg/dl | 0.8±0.2 | 0.8±0.2 | 0.8±0.2 | 0.0744 |
|
eGFR,
ml/min/1.73 m2 | 73.4±13.7 | 75.2±21.7 | 75.8±20.9 | 0.1047 |
|
Serum Ca,
mmol/l | 9.3±0.4 | 9.2±0.4 | 9.3±0.4 | 0.4241 |
|
Serum P,
mmol/l | 3.1±0.5 | 3.1±0.4 | 3.1±0.5 | 0.9165 |
|
U-BMG/Cr,
µg/g·Cre | 5,224±17,471 | 3,702±13,769 | 3,547±14,652 | 0.002a |
|
U-NAG/Cr,
U/g·Cre | 9.2±8.9 | 8.8±10.2 | 9.2±9.5 | 0.8068 |
|
%TRP | 85.0±9.3 | 84.0±10.0 | 85.8±8.8 | 0.3750 |
|
TmP/GFR,
mg/dl | 2.6±0.6 | 2.6±0.5 | 2.6±0.6 | 0.8476 |
| Long-term group,
n=19 | | | | |
|
Creatinine,
mg/dl | 0.9±0.3 | 0.9±0.2 | 0.8±0.2 | 0.0890 |
|
eGFR,
ml/min/1.73 m2 | 68.4±17.5 | 69.9±17.8 | 70.9±17.4 | 0.1719 |
|
Serum Ca,
mmol/l | 9.4±0.4 | 9.3±0.4 | 9.3±0.3 | 0.4880 |
|
Serum P,
mmol/l | 3.1±0.6 | 3.1±0.4 | 3.0±0.4 | 0.7553 |
|
U-BMG/Cr,
µg/g·Cre | 8,636±23,026 | 6,191±17,858 | 5,815±19,200 | 0.0017a |
|
U-NAG/Cr,
U/g·Cre | 10.8±11.5 | 11.1±13.1 | 10.8±12.1 | 0.7575 |
|
%TRP | 82.5±11.4 | 81.2±12.0 | 85.0±10.7 | 0.0602 |
|
TmP/GFR,
mg/dl | 2.6±0.7 | 2.5±0.6 | 2.6±0.5 | 0.8673 |
| Short-term group,
n=14 | | | | |
|
Creatinine,
mg/dl | 0.8±0.2 | 0.8±0.2 | 0.7±0.2 | 0.5409 |
|
eGFR,
ml/min/1.73 m2 | 77.9±18.1 | 79.0±22.2 | 82.5±24.0 | 0.3997 |
|
Serum Ca,
mmol/l | 9.3±0.2 | 9.2±0.4 | 9.2±0.4 | 0.7471 |
|
Serum P,
mmol/l | 3.1±0.5 | 3.1±0.4 | 3.1±0.7 | 0.5535 |
|
U-BMG/Cr,
µg/g·Cre | 951±1,455 | 262±179 | 469±549 | 0.0052a |
|
U-NAG/Cr,
U/g·Cre | 7.2±3.1 | 5.6±2.1 | 7.0±3.5 | 1.0000 |
|
%TRP | 88.1±4.5 | 87.5±3.9 | 87.0±5.4 | 0.2958 |
|
TmP/GFR,
mg/dl | 2.7±0.5 | 2.7±0.4 | 2.7±0.7 | 0.9875 |
Comparison based on the duration of NA
administration
Changes in viral markers, hepatobiliary enzymes,
renal and tubular functions, and phosphorus metabolism between the
long-term and short-term administration groups were compared and
assessed. The results of each group are shown in Tables II and III. In the long-term group, the serum
HBsAg levels were 590±641 and 537±598 IU/ml before switching to TAF
and 6 months after switching, respectively (P=0.0108), and those of
the short-term group were 1,853±2,400 and 1,631±2,235 IU/ml,
respectively (P=0.0040). In the long-term group, the serum ALP
levels were 324±141 and 302±151 U/l before switching and 6 months
after switching, respectively (P=0.0281), and those of the
short-term group were 298±86 and 257±69 U/l, respectively
(P=0.0050). In the long-term group, the serum BAP levels were
21.1±11.0 and 19.2±9.7 µg/l before switching and 6 months after,
respectively (P=0.0678), whereas in the short-term group, the
values were 17.9±5.1 and 15.5±4.6 µg/l, respectively (P=0.0016). In
the long-term group, the U-BMG/Cr ratios before switching and 6
months after switching were 8,635±23,026 and 5,815±19,200 µg/g·Cre,
respectively (P=0.0017), whereas in the short-term group they were
951±1,455 and 469±549 µg/g·Cre, respectively (P=0.0052).
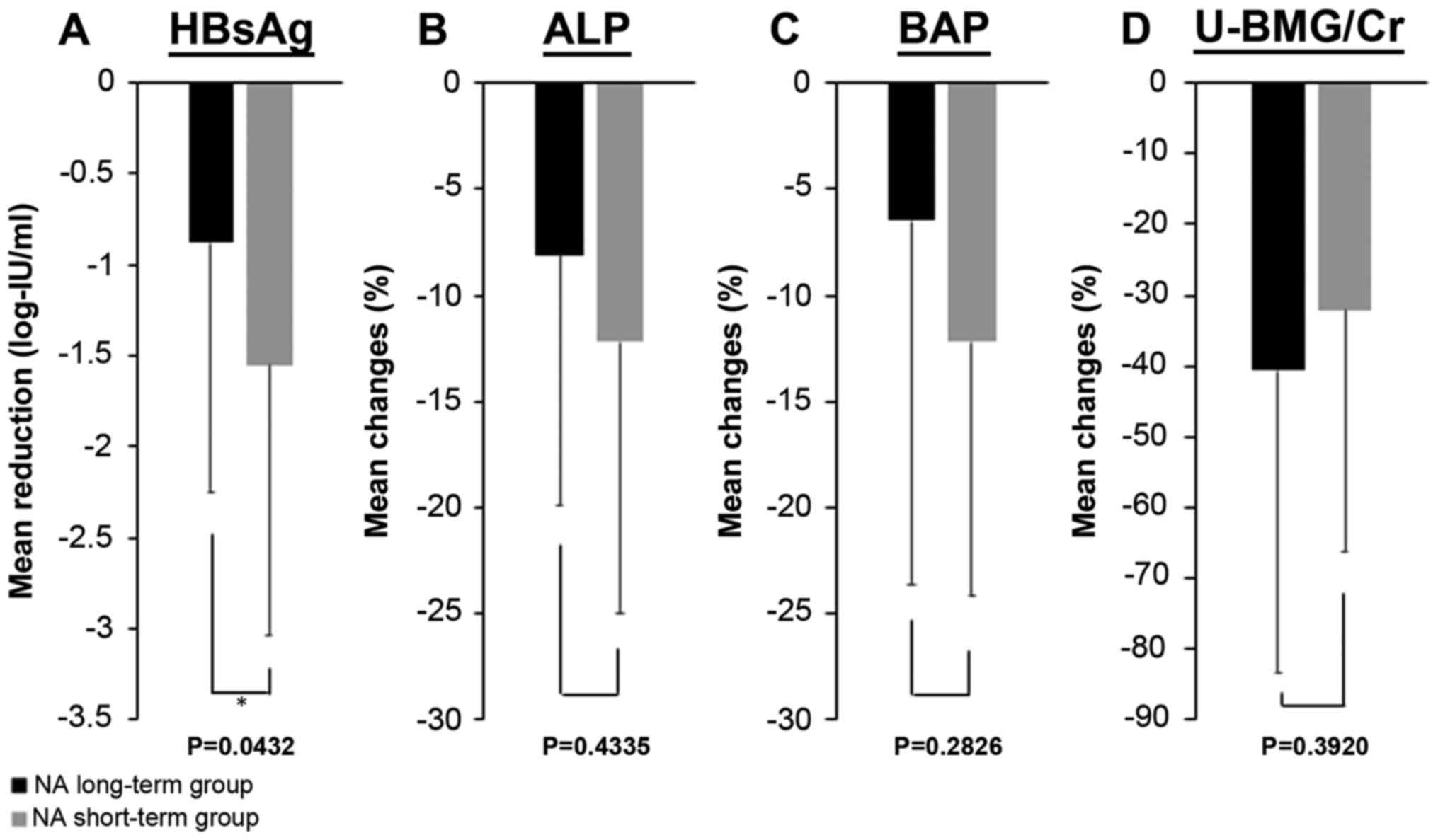
Fig. 1 shows the
reduction in the HBsAg levels and the improvements in serum ALP,
serum BAP and U-BMG/Cr levels in each group. The HBsAg levels
decreased by 0.88±1.37 log-IU/ml in the long-term group and by
1.55±1.49 log-IU/ml in the short-term group, whereas the serum ALP
levels improved by 8.1±11.9% in the long-term group and 12.2±12.8%
in the short-term group. The serum BAP levels improved by 6.5±17.1%
in the long-term group and 12.2±12.0% in the short-term group.
U-BMG/Cr improved by 40.6±42.9% in the long-term group and by
32.1±34.3% in the short-term group. In summary, similar to the
results seen in all 33 cases, a significant decrease in serum HBsAg
levels and a significant improvement in serum ALP and U-BMG/Cr
levels were observed in both groups. The serum BAP improved in both
groups, but a significant improvement was observed only in the
short-term group. HBsAg was significantly reduced in the short-term
group compared with the long-term group (P=0.0432). No significant
differences were found between the two groups in the other
comparisons.
Discussion
The present study evaluated changes in biochemical
(particularly renal and tubular functions and phosphorus
metabolism) and virological markers in patients with CHB who
switched from treatment with ADV or TDF therapy to TAF therapy. The
results from the whole sample showed that the serum HBsAg and ALP
levels and the U-BMG/Cr ratio were significantly decreased 6 months
after switching. Within this period, no cases were found to have
inadequate disease control due to a decrease in the antiviral
effect and exacerbation of hepatobiliary enzymes.
Regarding the reduction in the HBsAg levels,
Hagiwara et al (27) reported
that it was particularly prominent in patients with serum HBsAg
levels <800 IU/ml after switching from ETV to TAF. Uchida et
al (28) found that the degree
of reduction in serum HBsAg levels after switching from ETV to TAF
was significantly higher, particularly in patients with cirrhosis,
genotype B HBV infection and serum hepatitis B core related antigen
levels <3.0 log U/ml. As mentioned above, some studies reported
on factors contributing to the reduction in the serum HBsAg levels
after switching from other NAs to TAF. In patients with low levels
of HBV DNA who had a low risk of HCC, serum HBsAg levels were
identified as an independent risk factor for the development of HCC
(29). In addition, patients who
received TDF treatment exhibit a reduced risk of developing HCC
compared with those who received ETV treatment (30,31).
A possible mechanism underlying the difference in
HCC risk is the induction of IFN-λ activity in patients treated
with NAs, such as TDF and TAF, which would lead to the inhibition
of HBsAg production and activation of an antitumor effect (32). As mentioned above, since the
inhibitory effect of TFV on HCC development has been reported, it
is necessary to examine not only the effect of reducing serum HBsAg
levels in TAF but also the effect of reducing HCC risk in the
future, but this was not evaluated in the present study. Moreover,
renal and tubular functions were considered. Mitochondrial
dysfunction of the proximal tubule cells is presumed to be a
mechanism of renal dysfunction and the onset of ADV-related Fanconi
syndrome (33). Fanconi syndrome is
a disease that causes disorders of glucose, amino acid, phosphorus,
and bicarbonate reabsorption in the proximal tubule of the kidney,
and is often associated with osteomalacia (34). Renal tubular injury is characterized
by a decrease in serum phosphorus and uric acid levels, an increase
in U-BMG, and osteomalacia combined with elevation of the serum ALP
levels (34,35). Previously, genetic polymorphisms of
multidrug resistance-associated protein 2, which is involved in the
excretion of ADV from the renal tubule, have been reported as
factors contributing to renal impairment by ADV (36,37).
Although ADV was changed to TDF in ADV-related Fanconi syndrome,
TDF is structurally similar to ADV, and renal dysfunction and
Fanconi syndrome due to TDF have also been reported. Therefore, as
in ADV treatment, monitoring of renal and tubular functions is also
required (17,18,38).
As an important clinical premise, tubular
dysfunction may precede the decline in glomerular function. Tubular
proteinuria implies the presence of increased amounts of
small-sized proteins in the urine that are freely filtered in the
glomerulus but reabsorbed by the proximal tubules (39,40).
β2-microglobulinuria is prevalent amongst TFV-treated patients,
even with normal GFR (39,40). In the present study, the mean overall
eGFR was 73.4±13.7 ml/min/1.73 m2; although various
patients had normal kidney function or mild CKD, the mean U-BMG/Cr
was elevated (>300 µg/g·Cre was defined as abnormal) (41), indicating that tubular damage was
already present. Primary tubular abnormalities, even severe, may be
missed until they affect the glomerular function; thus, specific
and early screening is necessary to prevent abnormalities.
Blood biochemical examination alone is insufficient
to assess tubular dysfunction, and a regular urine test is
recommended in patients undergoing NA treatment. This is also
useful for evaluating phosphorous metabolism. Thus, how the
duration of NA administration affected the transition of
biochemical data was assessed with a focus on renal and tubular
function after switching to TAF between the long-term and
short-term groups. The U-BMG/Cr findings indicate that tubular
injury was already present even in the short-term group. Similar to
the whole-sample results, switching to TAF showed a significant
improvement in serum ALP levels and in the U-BMG/Cr ratio in both
groups. As shown in Fig. 1, an
improvement in serum ALP levels and in the U-BMG/Cr ratio can be
expected after this switch.
The important points of the present study were that
these improvements were obtained regardless of the duration of the
previous NA administration and that the effect was observed within
6 months after switching therapy. The incidence of tubular
dysfunction has been reported to increase dramatically 8 years
after the start of ADV administration (42). Thus, it is notable that the tubular
dysfunction caused by long-term administration of NA, including
ADV, is improved by switching to TAF. A real-world study also
reported that switching from TDF to TAF significantly reduced
tubular dysfunction markers, including the U-BMG/Cr and
retinol-binding protein-creatinine ratio in 3 months (43). A previous study also reported that
not only tubular dysfunction markers, but also eGFR, significantly
improved 1 and 6 months after switching from TDF to TAF (44).
Most patients treated with NA combination therapy
have already been treated for years or even decades. Furthermore,
since complete eradication of HBV is exceedingly difficult with
current treatments, continuous treatment is required. Based on
previous reports and the present study, which found an improvement
in a short period of time, switching to TAF in patients with renal
and tubular dysfunction appears to be effective regardless of
previous NA administration duration (43,44).
Therefore, switching to TAF should be considered, even in patients
treated with NAs who have not experienced side effects. Although a
detailed examination was not performed in the present study,
including analysis of changes in bone density, the improvement in
serum ALP and BAP levels may reflect an improvement in bone
metabolism. In fact, clinical trials and real-world studies have
shown superior bone safety in patients treated with TAF compared
with those treated with TDF (4-6,43).
The limitations of the present study are the small
sample size, the short-term follow-up period, and the lack of a
control group. The effects on serum HBsAg level reduction, renal
tubular function and bone metabolism by switching from NA to TAF
should be investigated in a larger cohort over a period of time.
Considering the association between renal and bone dysfunction,
long-term administration of ADV and TDF, and the increase in
compliance due to the convenience of administration timing compared
with ETV (45), if the antiviral
effect is not inferior in the long term and is safer, it is
expected that switching to TAF therapy will become more frequently
recommended in the future. Further randomized clinical trials are
required for selecting appropriate NAs.
In conclusion, switching from ADV or TDF to TAF
confirmed a decrease in serum HBsAg and improvement in serum ALP
levels and the U-BMG/Cr ratio after 6 months in patients regardless
of length of NA administration history.
Supplementary Material
Treatment history with NAs in all
cases.
Acknowledgements
The authors would like to thank Dr T. Kawaguchi, Dr
T. Nakamura, Dr M. Nakano, Dr S. Okamura, Dr M. Abe and Dr S.
Shimose, Division of Gastroenterology, Department of Internal
Medicine, Kurume University School of Medicine for their
contribution to this study.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
TS, KA, TI, TK, RK, TAH, HK, RK and TT obtained the
biological samples. TS, KA, and TI analyzed the data. TS wrote the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was performed in accordance with the
ethical principles of the Declaration of Helsinki and was approved
by the Clinical Research Ethics Committee of Kurume University
Hospital (approval no. 17209). Written informed consent was
obtained from all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Trépo C, Chan HLY and Lok A: Hepatitis B
virus infection. Lancet. 384:2053–2063. 2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kwon H and Lok AS: Hepatitis B therapy.
Nat Rev Gastroenterol Hepatol. 8:275–284. 2011.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lo AO and Wong GL: Current developments in
nucleoside/nucleotide analogues for hepatitis B. Expert Rev
Gastroenterol Hepatol. 8:607–622. 2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Buti M, Gane E, Seto WK, Chan HL, Chuang
WL, Stepanova T, Hui AJ, Lim YS, Mehta R, Janssen HL, et al:
Tenofovir alafenamide versus tenofovir disoproxil fumarate for the
treatment of patients with HBeAg-negative chronic hepatitis B virus
infection: A randomised, double- blind, phase 3, non-inferiority
trial. Lancet Gastroenterol Hepatol. 1:196–206. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Chan HL, Fung S, Seto WK, Chuang WL, Chen
CY, Kim HJ, Hui AJ, Janssen HL, Chowdhury A, Tsang TY, et al:
Tenofovir alafenamide versus tenofovir disoproxil fumarate for the
treatment of HBeAg-positive chronic hepatitis B virus infection: A
randomised, double-blind, phase 3, non-inferiority trial. Lancet
Gastroenterol Hepatol. 1:185–195. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Agarwal K, Brunetto M, Seto WK, Lim YS,
Fung S, Marcellin P, Ahn SH, Izumi N, Chuang WL, Bae H, et al: 96
weeks treatment of tenofovir alafenamide vs. tenofovir disoproxil
fumarate for hepatitis B virus infection. J Hepatol. 68:672–681.
2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Wong GL, Chan HL, Mak CW, Lee SK, Ip ZM,
Lam AT, Iu HW, Leung JM, Lai JW, Lo AO, et al: Entecavir treatment
reduces hepatic events and deaths in chronic hepatitis B patients
with liver cirrhosis. Hepatology. 58:1537–1547. 2013.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Gordon SC, Lamerato LE, Rupp LB, Li J,
Holmberg SD, Moorman AC, Spradling PR, Teshale EH, Vijayadeva V,
Boscarino JA, et al: Antiviral therapy for chronic hepatitis B
virus infection and development of hepatocellular carcinoma in a US
population. Clin Gastroenterol Hepatol. 12:885–893. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Lok AS, McMahon BJ, Brown RS Jr, Wong JB,
Ahmed AT, Farah W, Almasri J, Alahdab F, Benkhadra K, Mouchli MA,
et al: Antiviral therapy for chronic hepatitis B viral infection in
adults: A systematic review and meta-analysis. Hepatology.
63:284–306. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Mak LY, Seto WK, Lai CL and Yuen MF: DNA
polymerase inhibitors for treating hepatitis B: A safety
evaluation. Expert Opin Drug Saf. 15:383–392. 2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Wong GL, Tse YK, Wong VW, Yip TC, Tsoi KK
and Chan HL: Long-term safety of oral nucleos(t)ide analogs for
patients with chronic hepatitis B: A cohort study of 53,500
subjects. Hepatology. 62:684–693. 2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Cathcart AL, Chan HL, Bhardwaj N, Liu Y,
Marcellin P, Pan CQ, Shalimar Buti M, Cox S, Parhy B, et al: No
resistance to tenofovir alafenamide detected through 96 Weeks of
treatment in patients with chronic hepatitis B infection.
Antimicrob Agents Chemother. 62:e01064–18. 2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Sax PE, Wohl D, Yin MT, Post F, DeJesus E,
Saag M, Pozniak A, Thompson M, Podzamczer D, Molina JM, et al:
Tenofovir alafenamide versus tenofovir disoproxil fumarate,
coformulated with elvitegravir, cobicistat, and emtricitabine, for
initial treatment of HIV-1 infection: Two randomised, double-blind,
phase 3, non-inferiority trials. Lancet. 385:2606–2615.
2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Mills A, Arribas JR, Andrade-Villanueva J,
DiPerri G, Van Lunzen J, Koenig E, Elion R, Cavassini M, Madruga
JV, Brunetta J, et al: Switching from tenofovir disoproxil fumarate
to tenofovir alafenamide in antiretroviral regimens for
virologically suppressed adults with HIV-1 infection: A randomised,
active-controlled, multicentre, open-label, Phase 3,
non-inferiority study. Lancet Infect Dis. 16:43–52. 2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Agarwal K, Fung SK, Nguyen TT, Cheng W,
Sicard E, Ryder SD, Flaherty JF, Lawson E, Zhao S, Subramanian GM,
et al: Twenty-eight days safety, antiviral activity, and
pharmacokinetics of tenofovir alafenamide for treatment of chronic
hepatitis B infection. J Hepatol. 62:533–540. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ha NB, Ha NB, Garcia RT, Trinh HN, Vu AA,
Nguyen HA, Nguyen KK, Levitt BS and Nguyen MH: Renal dysfunction in
chronic hepatitis B patients treated with adefovir dipivoxil.
Hepatology. 50:727–734. 2009.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Jung YK, Yeon JE, Choi JH, Kim CH, Jung
ES, Kim JH, Park JJ, Kim JS, Bak YT and Byun KS: Fanconi's Syndrome
associated with prolonged adefovir dipivoxil therapy in a hepatitis
B virus patient. Gut Liver. 4:389–393. 2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Viganò M, Brocchieri A, Spinetti A,
Zaltron S, Mangia G, Facchetti F, Fugazza A, Castelli F, Colombo M
and Lampertico P: Tenofovir-induced Fanconi syndrome in chronic
hepatitis B monoinfected patients that reverted after tenofovir
withdrawal. J Clin Virol. 61:600–603. 2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Mauss S, Berger F, Filmann N, Hueppe D,
Henke J, Hegener P, Athmann C, Schmutz G and Herrmann E: Effect of
HBV polymerase inhibitors on renal function in patients with
chronic hepatitis B. J Hepatol. 55:1235–1240. 2011.PubMed/NCBI View Article : Google Scholar
|
|
20
|
World Medical Association Declaration of
Helsinki. Ethical principles for medical research involving human
subjects. JAMA. 310:2191–2194. 2013.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Drafting Committee for Hepatitis
Management Guidelines and the Japan Society of Hepatology. JSH
Guidelines for the management of hepatitis B virus infection.
Hepatol Res. 44 (Suppl S1):S1–S58. 2014.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Committee of the Japan Diabetes Society on
the Diagnostic Criteria of Diabetes Mellitus. Seino Y, Nanjo K,
Tajima N, Kadowaki T, Kashiwagi A, Araki E, Ito C, Inagaki N,
Iwamoto Y, et alReport of the committee on the classification and
diagnostic criteria of diabetes mellitus. J Diabetes Investig.
1:212–228. 2010.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Levey AS, Stevens LA, Schmid CH, Zhang Y,
Castro AF III, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene
T, et al: A new equation to estimate glomerular filtration rate.
Ann Intern Med. 150:604–612. 2009.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Barth JH, Jones RG and Payne RB:
Calculation of renal tubular reabsorption of phosphate: The
algorithm performs better than the nomogram. Ann Clin Biochem.
37:79–81. 2000.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Bervoets AR, Spasovski GB, Behets GJ, Dams
G, Polenakovic MH, Zafirovska K, Van Hoof VO, De Broe ME and
D'Haese PC: Useful biochemical markers for diagnosing renal
osteodystrophy in predialysis end-stage renal failure patients. Am
J Kidney Dis. 41:997–1007. 2003.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Ureña P, Hruby M, Ferreira A, Ang KS and
de Vernejoul MC: Plasma total versus bone alkaline phosphatase as
markers of bone turnover in hemodialysis patients. J Am Soc
Nephrol. 7:506–512. 1996.PubMed/NCBI
|
|
27
|
Hagiwara S, Nishida N, Ida H, Ueshima K,
Minami Y, Takita M, Komeda Y and Kudo M: Switching from entecavir
to tenofovir alafenamide versus maintaining entecavir for chronic
hepatitis B. J Med Virol. 91:1804–1810. 2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Uchida Y, Nakao M, Tsuji S, Uemura H,
Kouyama JI, Naiki K, Motoya D, Sugawara K, Nakayama N, Imai Y, et
al: Significance of switching of the nucleos(t)ide analog used to
treat Japanese patients with chronic hepatitis B virus infection
from entecavir to tenofovir alafenamide fumarate. J Med Virol.
92:329–338. 2020.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Tseng TC, Liu CJ, Yang HC, Su TH, Wang CC,
Chen CL, Kuo SF, Liu CH, Chen PJ, Chen DS and Kao JH: High levels
of hepatitis B surface antigen increase risk of hepatocellular
carcinoma in patients with low HBV load. Gastroenterology.
142:1140–1149.e3; quiz e13-4. 2012.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Choi J, Kim HJ, Lee J, Cho S, Ko MJ and
Lim YS: Risk of hepatocellular carcinoma in patients treated with
entecavir vs. tenofovir for chronic hepatitis B: A Korean
nationwide cohort study. JAMA Oncol. 5:30–36. 2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Yip TC, Wong VW, Chan HL, Tse YK, Lui GC
and Wong GL: Tenofovir is associated with lower risk of
hepatocellular carcinoma than entecavir in patients with chronic
HBV infection in China. Gastroenterology. 158:215–225.e6.
2019.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Murata K, Asano M, Matsumoto A, Sugiyama
M, Nishida N, Tanaka E, Inoue T, Sakamoto M, Enomoto N, Shirasaki
T, et al: Induction of IFN-λ3 as an additional effect of
nucleotide, not nucleoside, analogues: A new potential target for
HBV infection. Gut. 67:362–371. 2018.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Tanji N, Tanji K, Kambham N, Markowitz GS,
Bell A and D'agati VD: Adefovir nephrotoxicity: Possible role of
mitochondrial DNA depletion. Hum Pathol. 32:734–740.
2001.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Izzedine H, Launay-Vacher V, Isnard-Bagnis
C and Deray G: Drug-induced Fanconi's syndrome. Am J Kidney Dis.
41:292–309. 2003.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Sun L, Yi D, Sun W and Wang C:
Retrospective analysis of the clinical characteristics of adefovir
dipivoxil-induced Fanconi's syndrome in the Chinese population. J
Clin Pharm Ther. 45:722–728. 2020.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Servais A, Lechat P, Zahr N, Urien S,
Aymard G, Jaudon MC, Deray G and Isnard Bagnis C: Tubular
transporters and clearance of adefovir. Eur J Pharmacol.
540:168–174. 2006.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Sanyal A, Bass N, Mullen K, Poordad F,
Shaw A, Merchant K, Bortey E, Forbes WP and Huang S: A drug
transporter gene polymorphism predicts renal tubular toxicity in
patients with chronic hepatitis B on long-term adefovir and
lamivudine combination. J Hepatol. 52(S7)2010.
|
|
38
|
Fernandez-Fernandez B, Montoya-Ferrer A,
Sanz AB, Sanchez-Niño MD, Izquierdo MC, Poveda J, Sainz-Prestel V,
Ortiz-Martin N, Parra-Rodriguez A, Selgas R, et al: Tenofovir
nephrotoxicity: 2011 update. AIDS Res Treat.
2011(354908)2011.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Papaleo A, Warszawski J, Salomon R,
Jullien V, Veber F, Dechaux M and Blanche S: Increased beta-2
microglobulinuria in human immunodeficiency virus-1-infected
children and adolescents treated with tenofovir. Pediatr Infect Dis
J. 26:949–951. 2007.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Gatanaga H, Tachikawa N, Kikuchi Y, Teruya
K, Genka I, Honda M, Tanuma J, Yazaki H, Ueda A, Kimura S and Oka
S: Urinary beta2-microglobulin as a possible sensitive marker for
renal injury caused by tenofovir disoproxil fumarate. AIDS Res Hum
Retroviruses. 22:744–748. 2006.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Dauchy FA, Lawson-Ayayi S, de La Faille R,
Bonnet F, Rigothier C, Mehsen N, Miremont-Salamé G, Cazanave C,
Greib C, Dabis F and Dupon M: Increased risk of abnormal proximal
renal tubular function with HIV infection and antiretroviral
therapy. Kidney Int. 80:302–309. 2011.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Shimizu M, Furusyo N, Ikezaki H, Ogawa E,
Hayashi T, Ihara T, Harada Y, Toyoda K, Murata M and Hayashi J:
Predictors of kidney tubular dysfunction induced by adefovir
treatment for chronic hepatitis B. World J Gastroenterol.
21:2116–2123. 2015.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Fong TL, Lee BT, Tien A, Chang M, Lim C,
Ahn A and Bae HS: Improvement of bone mineral density and markers
of proximal renal tubular function in chronic hepatitis B patients
switched from tenofovir disoproxil fumarate to tenofovir
alafenamide. J Viral Hepat. 26:561–567. 2019.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Kaneko S, Kurosaki M, Tamaki N, Itakura J,
Hayashi T, Kirino S, Osawa L, Watakabe K, Okada M, Wang W, et al:
Tenofovir alafenamide for hepatitis B virus infection including
switching therapy from tenofovir disoproxil fumarate. J
Gastroenterol Hepatol. 34:2004–2010. 2019.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Tamaki N, Kurosaki M, Nakanishi H, Itakura
J, Inada K, Kirino S, Yamashita K, Osawa L, Sekiguchi S, Hayakawa
Y, et al: Comparison of medication adherence and satisfaction
between entecavir and tenofovir alafenamide therapy in chronic
hepatitis B. J Med Virol. 92:1355–1358. 2020.PubMed/NCBI View Article : Google Scholar
|