Modern cancer immunotherapy has been proposed to
involve four primary promising strategies: i) Active vaccination of
tumor antigens, ii) passive vaccination with antibodies specific to
cancer antigens, iii) adoptive transfer of cancer-specific T cells,
and iv) manipulation of the patient's immune response by inhibiting
immune checkpoints. Additional emerging strategies include other
antigen-non-specific interventions, including the applications of
oncolytic or immune-enhancing viruses, innate immunity stimulators
and immunogenic cell death (ICD) inducers (1). The focus of the present review was to
describe the treatments that employ ICD to enhance the immunity of
patients with gastrointestinal (GI) cancers.
The daily death of billions of ordinary cells from
the human body goes essentially unrecognized by the immune system.
This is crucial since the conservation of the entire bodies
homeostasis includes the continuous turnover of various cell
compartments. As such, the initiation of an immune response against
dead-cell antigens would have detrimental outcomes. Conversely, the
death of a few cells infected by a microorganism can trigger a
potent antigen-specific immune reaction, which is associated with
the clearance of the invading pathogen from the body and also
enables the establishment of long-term immunological memory
(2). The first proposal of the
‘danger theory’ in 1994 by Matzinger (3) was that the immune system can
distinguish between dangerous and innocuous endogenous signaling.
In her famous essay, Matzinger suggested that ‘unprogrammed cell
death’ could give rise to the unusual release of internal molecules
from the cytoplasm, nucleus or membrane to activate dendritic cells
(DCs). The dying, stressed or injured cells release or present
molecules on the cell surface, which can function as either
adjuvants or danger signals for detection by the innate immune
system. These molecules are now termed ‘damage-associated molecular
patterns’ (DAMPs) (4). The term
‘ICD’ was introduced to indicate a type of cell death that triggers
an immune response against dead-cell antigens, particularly those
derived from cancer cells, including DAMPs. This model was
initially proposed with regard to anticancer chemotherapy, in view
of clinical proof demonstrating that tumor-specific immune
responses reflect the efficacy of anticancer treatments using
conventional cytotoxic drugs (5).
Currently, various routinely employed anticancer
agents include doxorubicin, epirubicin, idarubicin, mitoxantrone,
bleomycin, bortezomib, cyclophosphamide (CY) and oxaliplatin. The
list also includes certain anticancer agents that are currently
under preclinical or clinical development, such as some
microtubular inhibitors of the epothilone family. Certain drugs,
including digoxin, digitoxin and zoledronic acid, act to convert
otherwise non-immunogenic events of cell death into bona
fide ICD inducers, and may thus be used as adjuvants in
combinatorial immunotherapy regimens (6). The known clinically applied or
experimental anticancer agents that induce ICD act via one or
several of the following mechanisms: Inducing apoptosis, causing a
severe focused stress of the endoplasmic reticulum, overcoming
loss-of-function mutations that hide danger signals during
tumorigenesis and downregulating the cancer-based induction of
pro-inflammatory transcription factors (4). In addition, one important
consideration is the complex interactions with DAMPs and their
receptors, known as the pattern recognition receptors. Attempts
have been made to identify and detect multiple DAMPs in order to
facilitate the development of next-generation anticancer regimens,
which, in addition to killing cancer cells, can simultaneously
convert them into a cancer-specific therapeutic vaccine (7).
GI cancers are amongst the malignancies most
frequently diagnosed in European patients. These include gastric
cancer (GC), colorectal cancer (CRC), as well as cancers affecting
the liver, particularly hepatocellular carcinoma (HCC), the biliary
tract, such as cholangiocarcinoma (CCA), and the pancreas
(pancreatic cancer; PC). The frequency with which these conditions
are diagnosed presents a significant challenge for public health
systems in Europe and worldwide (8).
Most commonly reported in patients in Asia, GC is
notable for its particularly poor survival rates. The condition is
associated with certain bacterial infections, such as
Helicobacter pylori (H. pylori) infection, and the
effects of other pathogens, including Epstein-Barr virus (9).
The annual number of new CRC diagnoses falls in the
range of 1-2 million cases, placing CRC third in terms of the most
frequently occurring cancers, and fourth amongst the most common
causes of cancer-related mortality. The main CRC risk factors
include age and history of chronic disease, as well as various
aspects of patient lifestyles. There are three different pathogenic
mechanisms that can lead to the onset of CRC: Microsatellite
instability, chromosomal instability and a CpG island methylator
phenotype (10,11).
The most common type of liver cancer is HCC, which
originates from hepatocytes and accounts for ~4 in 5 liver cancer
diagnoses, with an increased prevalence in China and Eastern Africa
(12). The onset of HCC is often a
consequence of the interaction between genetic characteristics and
environmental factors. In particular, patients diagnosed with liver
cirrhosis, or infection with the hepatitis B virus (HBV) or the
hepatitis C virus (HCV), are more likely to develop HCC, while
other risk factors include alcohol abuse, the ingestion of
aflatoxin B1 or non-alcoholic steatohepatitis (13,14).
CCA is the second most frequently occurring primary
hepatic cancer after HCC. CCA has been most commonly reported
across Asia, although in recent years it has become increasingly
more widespread in North America and Europe (15,16).
CCA originates in the biliary tract and is subdivided by location
into three different subtypes, namely perihilar, intrahepatic and
distal CCA. Several risk factors, both common and rare, have been
associated with CCA, including hepatobiliary parasites, Caroli
disease, HBV and HCV infection, and exposure to toxins (17-19).
PC is the 14th most prevalent type of cancer and the
seventh largest cause of annual cancer-associated deaths globally.
PC risk factors include obesity, alcohol consumption and smoking,
as well as H. pylori infection (20).
Several potential treatments are currently being
developed for GI cancers. A number of these are targeted approaches
that make use of biological properties to achieve their objectives,
and can be employed alone or as components of combination or
adjuvant treatments. The most widely applied treatments at present
include surgery, as a means of resecting solid tumors; radiation
therapy, as a means of managing localized solid tumors;
chemotherapy, which involves the use of cytotoxic agents to
eliminate cancerous cells; and hormonal therapy, which serves as a
systematic approach with the aim of targeting all cancerous cells
found in the body (21-23).
Patients diagnosed with GI cancers are typically
subjected to a combination of treatments, including surgery,
chemotherapy and/or radiation therapy; however, the survival rates
remain poor, particularly when the cancer has reached an advanced
stage, or in the case of metastatic disease (24,25).
For this reason, it is imperative to develop more effective, novel
techniques to address the problem, and immunotherapy appears to
hold promise for this purpose. To date, a number of cytokines,
including IFN-γ or IL-2, have been used to limit the activity of
certain types of cancer, such as renal cell carcinoma and melanoma,
and a moderate level of inhibitory activity has been reported
(26). However, the development of
cancer vaccines has been less successful, with none generating
statistically significant responses in test patients (23).
The progress in immunotherapy shows great potential
in the context of GI cancers, whereas further therapies involving
the administration of immunostimulatory monoclonal antibodies to
treat GI malignancies are currently in their developmental phase.
Immune checkpoint blockade is the primary type of immunotherapy
currently used in GI cancer treatment. It can be anticipated that
the vaccination approach will be streamlined with the lessons
learned from initial successes, and the most suitable
tumor-associated antigens will be identified for targeting.
Adoptive cell therapies are now at an advanced stage of development
and appear to hold significant promise for GI cancers. An improved
understanding of the prevalent suppressive factors in patients with
GI cancers may enable the development of superior strategies to
limit immune suppression and promote endogenous immunity in
patients. It is likely that deeper knowledge of the tumor
microenvironment and the field of immunology will lead to the
successful development of more efficacious treatments in the near
future.
Various cancer vaccines have been developed to date
by using different technologies, including recombinant
microorganisms, recombinant antigen cocktails, oncolytic viruses,
DNA and gene therapy-based treatments, and anti-idiotypic
antibodies. In addition, personalized vaccines have also been
devised, including those based on adoptive cell transfer, or
autologous cells and antigens. These may be more complex, and
require specialized manufacturing approaches and expertise
(27). However, although several
trials have been conducted, approval has only been granted for one
vaccine, which acts against metastatic castration-resistant
prostate cancer. This vaccine is Dendreon's Provenge®
(Sipuleucel-T), which was approved by the Food and Drug
Administration in 2010 (28,29).
Furthermore, two additional cancer vaccines, Vitespen®
(30) and Melacine®
(31), were approved in Russia and
Canada, but not in the United States. These cancer vaccines rely
upon the activation and strengthening of antitumor responses that
target cancer. The dendritic cell-based cancer vaccine presents
antigens and serves a critical role in formulating the immune
response. They can also activate B cells, natural killer (NK)
cells, as well as naïve and memory T cells, through the
presentation of tumor antigens associated with major
histocompatibility complex (MHC) molecules. When patients with
cancer have higher numbers of DCs penetrating the tumors, this is a
sign of reduced lymph node metastases and improved chances of
survival (32). A number of
approaches have been employed to create vaccines by loading DCs
with tumor antigens. These include the use of synthetic peptides
pulsed on DCs (33), DCs engineered
with plasmid DNA (34), RNA
(35) or viruses (36), tumor cell lysates combined with
immature DCs (37) and, finally,
DCs combined with whole tumor cells through polyethylene glycol or
electroporation (38). The
technique that uses DCs pulsed with MHC-restricted peptides, which
are obtained from antigens known to be associated with tumors, is
the most common type of vaccine approach (39-41).
However, it can be challenging to use DCs for clinical purposes, as
these cells have a relatively short life span (42). To date, vaccines have shown little
effectiveness in preventing GI cancers. The vaccines developed thus
far have targeted melanoma-associated antigen (MAGE)-A3(43), HER2 p369 peptide (44), gastrin-17 diphtheria toxoid
(45), URLC10 or VEGFR1 epitopes
(46) and heat shock protein (HSP)
gp96(47) in patients with GI
cancers. Furthermore, chemotherapy has been tested alongside
adjuvant Bacillus Calmette-Guérin (48). In cases of PC, a number of specific
antigens serve as targets, including carcinoembryonic antigen
(CEA), EGFR, Wilms' tumor 1 and VEGF, whereas GVAX® is a
whole-cell vaccine that has been tested in trials in the
metastatic, neoadjuvant and adjuvant settings. Positive outcomes
have been reported in the metastatic setting when combined with
ipilimumab, with a reported survival rate of 27% after 1 year
(49).
In the case of HCC, vaccines have shown no efficacy
thus far. However, immune responses have been reported in phase I
trials involving peptide vaccines (50), DC vaccines and tumor-associated
antigens targeting oncolytic viruses, such as AFP (51), GPC-3(52) and human telomerase reverse
transcriptase (53). DC-based
vaccines have been included in trials on CCA, whereas a phase II
study was conducted in the adjuvant setting in order to target
mucin 1 (MUC1) in the biliary tract and in PC via DC vaccination,
and the tolerability was reported to be good, although it was not
possible to draw definitive conclusions regarding the immune
response (54). Further phase II
clinical trials involving CRC-specific peptide vaccines were
performed with patients diagnosed with HLA-A*2402-positive stage
III CRC, with the findings suggesting that an immune response would
be generated by the vaccine, leading to higher survival rates
(55). For patients with PC, 13-mer
mutant ras peptide vaccines were not only shown to be safe, but to
also generate the appropriate immune response (56). Additionally, the p53 synthetic long
peptide vaccine has been shown to be safe for patients with
metastatic CRC in whom specific T-cell responses were induced
(57). However, several issues must
be addressed if a novel cancer vaccine is to be approved, including
commercial, clinical, manufacturing, operational and regulatory
concerns. Risk evaluation must also be conducted to make full use
of the expertise available. Moreover, a number of clinical studies
revealed that some patients may not benefit from the cancer vaccine
treatment (primary resistance), and some responders may relapse
after a period of response (acquired resistance). For example, PC
is associated with the presence of a highly immunosuppressive
microenvironment, which is characterized by a dense desmoplastic
stroma that impedes blood flow to the area, inhibits drug delivery
and suppresses antitumor immune response (58). In CRC and GC, it has been shown that
only patients with the subset of mismatch-repair-deficient or
microsatellite instability-high tumors are likely to respond to
immunotherapy (59,60). Once these issues have been
addressed, ICD may prove to be the answer for vaccine
development.
DC maturation is a crucial step for immune
activation. Once in the lymph nodes, DCs activate T cells via three
canonical signals: Binding of T-cell receptors, co-stimulatory
receptor engagement, and the provision of cytokines and chemokines
to facilitate T-cell polarization and differentiation. The ICD
complementarily activates DCs. High mobility group box 1 (HMGB1)
and HSP activate pro-inflammatory DCs through the Toll-like
receptor (TLR)2/4-MyD88-NF-κB signaling pathway (61). Moreover, dying cancer cells also
express calreticulin (CRT) on their plasma membrane, which signals
to facilitate engulfment by DCs. The exposed CRT on the cell
membrane can bind to CD91, the low-density
lipoprotein-receptor-related protein 1, which promotes the
engulfment of cellular compartments and debris by a mechanism that
depends on the Rac family small GTPase 1(61). Hence, the original concept for using
the combination treatment of ICD stimulation and DC-based
anticancer vaccines originated from significant evidence that
cancer treatments, such as chemotherapy, radiation, phototherapy,
phytotherapy and immunotherapy, could elicit danger signals from
dying cancer cells. Notably, chemoradiotherapy is known to elevate
serum HMGB1 in patients with esophageal squamous cell carcinoma,
and the levels of HMGB1 were found to be positively correlated with
patient survival (62). Moreover,
oxaliplatin and mitoxantrone induced cancer cell death accompanied
by an exposure of CRT and a release of HMGB1, HSP70 and ATP,
thereby strongly inducing in vitro immune responses of DCs
(63,64). Interestingly, it has been
demonstrated that pretreatment with the oxaliplatin nanoparticle
followed by a rechallenge by tumor inoculation in PC-bearing mice
can enhance therapeutic efficacy by increasing the numbers of
tumor-infiltrating activated cytotoxic T cells (64). In addition to the use of
chemotherapy, botanical cancer therapy has also been introduced.
Treatment with Hemidesmus indicus was shown to induce CRC
cell apoptosis characterized by surface expression of CRT,
increased HSP70 expression, and a release of ATP and HMGB1. This
immunogenic agent is promising when combined with a DC-based
anticancer vaccine (Table I)
(65). Recently, our group
demonstrated that a potent bioactive compound, honokiol, can induce
CCA cell apoptosis, which is associated with the release of HMGB1
and HSP90. Incubation of DCs with CCA cells that were pretreated
with honokiol induced DC maturation, and thus enhanced the priming
of cytotoxic T cells to kill cancer cells (37). Therefore, the priming of DCs with
immunogenic agents may maximize antitumor responses though DC
stimulation.
Radiation as a cancer treatment also induces ICD,
which may pave the way for anticancer vaccines in such patients.
For example, in large orthotopic HCC, synergistic antitumor effects
may be obtained when radiation is combined with the administration
of IL-12. This has been shown to be associated with the activation
of tumor-infiltrating DCs, CD8+ T cells and NK cells, as
well as the suppression of tumor-infiltrating myeloid-derived
suppressor cells (MDSCs) (66).
Similar to radiation, phototherapy has been suggested to be a new
platform for enhancing the immunogenicity of cancer. Photodynamic
and photothermal therapies proficiently promote immunotherapy via
the induction of ICD. In addition, phototherapy combined with
oxygenation boosters can promote CRC cell apoptosis and induce ICD,
thus facilitating DC maturation and inhibiting tumor growth and
recurrence in animal models (67).
Plasma-treated PBS, which is physical cold atmospheric plasma
consisting of reactive oxygen and nitrogen species, has
demonstrated cytotoxic activity against PC cells with immunogenic
features. This increases the potential of phagocytosing DCs and DC
maturation, which may hold promise for combinations with DC cancer
vaccines (68).
Several clinical studies have corroborated the
concept that ICD-inducing pretreatment may act as an
immunomodulator (Table I). There
are ~50 trials currently investigating the benefit of ICD in
vaccines against cancer, mostly PC and CRC. A phase I/II trial
study, in which 22 patients with HCC have been enrolled, is
investigating treatment interventions comprising pre-infusion of CY
and vaccination using a multi-peptide-based HCC vaccine (IMA970A)
plus CV8102 adjuvant (RNAdjuvant®). This trial is
investigating whether IMA970A and CV8102 are safe and whether they
can trigger an immune response against the tumor under
pre-conditioning by induction of ICD (NCT03203005). Moreover,
mFOLFOX6, which is a formulation of 5-fluorouracil (5-FU),
leucovorin and oxaliplatin, has been used in combination with
nivolumab and vaccination with a CV301 peptide vaccine in patients
with advanced CRC (NCT03547999). Another clinical trial including
patients with PC used CY followed by vaccination with a GVAX
peptide cancer vaccine. However, pretreatment with CY did not
improve overall survival or disease-free survival when compared
with the uncombined intervention (NCT00727441). Collectively, the
majority of preclinical and clinical data have demonstrated that
combining the immunogenic potential of ICD with cancer vaccination
is a promising approach that could achieve future translational
success.
The field of immuno-oncology has witnessed
significant advances with regard to immune checkpoint inhibitors
(ICIs). Immune checkpoints are the mechanisms through which T-cell
immune responses are regulated (69). Tumor cells are considered to be able
to avoid host immune clearance when T-cell immune responses are
downregulated. If immune checkpoints can be targeted, the
endogenous response of the immune system to tumors may be used as a
means of addressing the risk of disease. A number of antibodies
have been shown to be effective against immune checkpoints, and
more are under examination (69).
These antibodies most commonly serve to target cytotoxic T
lymphocyte-associated protein 4 (CTLA-4), programmed death-1 (PD-1)
and programmed death-ligand 1 (PD-L1). CTLA-4 acts as a receptor
capable of inhibiting the activation of T cells (70). Accordingly, when CTLA-4 is blocked,
the T cells will proliferate and become activated. PD-1 is
expressed on T cells and other immune cells, and PD-L1 serves as
one of its ligands. PD-1 and PD-L1 binding creates an inhibitory
signal affecting T cells; by contrast, if the binding is inhibited,
the T cells will become activated, leading to a heightened response
from cold tumor (non-inflammatory T-cell) to hot tumor
(inflammatory T-cell) immune response (71-73).
Another targeted checkpoint receptor protein is the lymphocyte
activation gene-3, which may control the activity of T cells
through its binding with MHC class II-molecules (74). However, earlier studies examining
such checkpoint inhibitors in CRC were not very successful, phase
II trials involving the CTLA-4 inhibitor, tremelimumab, in patients
diagnosed with metastatic CRC have shown no significant levels of
efficacy (75,76).
As a consequence of tumor heterogeneity, along with
the complexity of immunosuppression, treatment of GC, as has been
the case with CRC, has shown little success in the area of
immunotherapy, for reasons possibly related to mechanisms that are
incompletely understood. Previous findings have revealed that a
certain level of checkpoint inhibition can be achieved, often in
correlation with enhanced classification and characterization of GC
and an improved understanding of its histopathology (48). PC presents the greatest challenge
amongst all types of GI cancer in the context of immunotherapy,
most likely as a result of inadequate immunogenicity, along with a
low mutational burden and a unique vascular and stromal
microenvironment. These conditions make it very difficult for the
immune cells and molecules to penetrate into the tumors,
particularly compared with the conditions in other types of cancer
(77). If the microenvironment
exhibits immunosuppressive qualities, checkpoint inhibition may
represent a suitable goal for HCC immunotherapy, although success
has been limited to date in the case of single-agent checkpoint
blockade (78).
In this decade, antibodies directed against immune
checkpoints have been intensely investigated in patients with
cancer following the discovery by the Nobel prize winners James P.
Allison and Tasuku Honjo, who demonstrated that cancer therapy can
be enhanced by the inhibition of negative immune regulation
(79). CTLA-4 and PD-1 are the
receptors that are commonly found on the surface of activated T
cells. The interaction of CTLA-4 and PD-1 with their ligands
inhibits activated T cells and converts them into exhausted T
cells, which abrogates the antitumor response. The targeting of
CTLA-4 and PD-1 molecules has demonstrated durable response rates,
increased survival time of responders and a manageable safety
profile. Recently, checkpoint inhibition plus chemotherapy has been
considered for use in the first-line setting for the treatment of
CRC (11). The potential clinical
responses may be associated with the induction therapy with ICD
inducers and cancer immunotherapy.
It has been reported that calmodulin-binding peptide
(CBP)501, a CBP that can induce ICD when combined with cisplatin
treatment, can induce cell membrane exposure of CRT and the release
of HMGB1. Treatment of CRC-bearing mice with CBP501 and cisplatin,
and subsequently with anti PD-1 or PD-L1 antibodies, significantly
enhanced the antitumor activity of immune blockade via upregulating
the percentage of tumor-infiltrating CD8+ T cells
(80). Similarly, in CRC-bearing
mouse models, the combination treatment of PARP and PI3K inhibitors
induced radio-sensitization and the induction of ICD. Thus,
subsequent anti-CTLA-4 treatment strongly inhibited tumor growth
and increased the numbers of tumor-infiltrating lymphocytes (TILs)
(81). The induction treatment of
not only CRC, but also HCC, has been investigated using immunogenic
chemotherapy, through oxaliplatin promoting the exposure of CRT and
the release of HMGB1. In HCC, oxaliplatin combined with anti PD-1
antibodies achieved marked tumor suppression, activation of
CD8+ T cells and stimulation of DCs (82). Moreover, radiation and phototherapy
are additional examples of immunogenic cancer therapies that
sensitize the immune checkpoint blockade. CD44-targeted
near-infrared photoimmunotherapy combined with anti CTLA-4 and PD-1
antibodies was shown to inhibit tumor growth and prolong the
survival of CRC-bearing mice via a mechanism associated with the
induction of ATP and the release of HMGB1(83).
The ICD inducer-enhancing immune blockade has been
proven in several clinical reports (Table I), but has not been well established
in GI cancers. Current phase II trials have been investigating the
ICD-inducing effect of 5-FU, leucovorin and oxaliplatin (FOLFOX)
and FOLFOX plus irinotecan (FOLFOXIRI) to enhance the efficacy of
ICIs. Patients with unresectable metastatic CRC have been treated
with either FOLFOX/FOLFOXIRI or anti-PD-L1/CTLA-4 antibodies. After
each treatment cycle, the safety, disease progression, death and
intolerable toxicity will be continuously recorded (84,85).
Furthermore, the use of 5-FU and cisplatin is encouraged owing to
their safety and strong enhancement of the antitumor response in
advanced GC when combined with pembrolizumab (86).
The insight into the mechanism of ICD-sensitized
immune blockade inhibitors is under investigation. Two possible
effects have been proposed, depending on the type of ICD inducer.
The first effect is the direct consequence of the chemotherapeutic
agents proficiently upregulating PD-L1 expression. Those that exert
this effect include 5-FU, gemcitabine, cisplatin, oxaliplatin,
doxorubicin and paclitaxel (87).
This is an important method for increasing the sensitivity to
blockade inhibitors. Treatment with FOLFOX can activate the
secretion of IFN-γ from PD-1+ CD8+ T cells,
which is associated with the overexpression of PD-L1 on tumor
cells. Hence, the combination treatment of FOLFOX with anti
PD-1/PD-L1 antibodies has achieved complete cure in CRC-bearing
mice, while monotherapy was unsuccessful (88). Similarly, the anthracycline drug,
epirubicin, could upregulate PD-L1 expression in HCC, which causes
sensitization to immune blockade therapy (89). The other effect would be due to the
indirect function of ICD inducer agents via modulating the tumor
microenvironment. This may be associated with the depletion of
regulatory T cells and MDSCs that potentiates stronger antitumor
responses (66). Taken together,
these results from preclinical and clinical studies have indicated
that the concept of priming treatment with ICD inducer agents prior
to checkpoint blockade treatment could elicit a stronger antitumor
response.
A potential approach to cancer treatment is
harnessing the properties of T cells and NK cells to attack tumor
cells. NK cells and TILs are of both predictive and prognostic
value in GI cancers (90). These
properties can be applied through the various modalities of
adoptive cell therapies, typically involving the isolation of
immune cells obtained from patients diagnosed with cancer,
whereupon they can be genetically modified in order to strengthen
their capacity to identify and kill cancerous cells. By expanding
these isolated cells ex vivo, they can then be re-introduced
to the patient, in a form of treatment which can theoretically be
effective for all patients with cancer who do not demonstrate
adequate cancer immunity without assistance, and would therefore be
incapable of responding to ICIs. Adoptive cell therapy as a cancer
treatment can involve various strategies, which have either been
previously examined in clinical settings, or are undergoing trials
to assess their suitability against GI cancers (91). One particular approach of adoptive
cell therapy makes use of the immunotherapeutic properties of
cytokine-induced killer cells (CIK), which can be obtained through
the treatment of peripheral blood lymphocytes using IFN-γ. This is
a type of monoclonal antibody that counteracts the CD3 molecule,
along with IL-2. CIK cells are predominantly expansions of
CD3+/CD8+/CD56- cells to become
terminally differentiated CD56-positive NK cells. These are
uniquely able to identify the tumor cells regardless of the
presence or absence of antibodies and MHC molecules and,
accordingly, have the ability to identify any tumor cells lacking
MHC molecules on their surface (92). In addition to T-cell adoptive
transfer, NK cell-based immunotherapy has shown promising antitumor
effects in a number of studies (93-95).
Adoptive transfer is being used to increase the infiltration of NK
cells in the tumor site by using NK cells from different origins,
such as autologous cells, allogeneic peripheral blood mononuclear
cells, umbilical cord blood, human embryonic stem cells and induced
pluripotent stem cells (90).
However, although preclinical data indicate high efficacy of NK
cell adoptive transfer in in vitro and in vivo
studies, there is little information on the clinical efficiency of
this method. A phase I clinical trial demonstrated that
HSP70-induced activation of autologous NK cells was achieved in
patients without any treatment-related negative side effects, but
no significant clinical response was observed due to the high tumor
burden and limited sample size (96). Moreover, adoptive macrophage
transfer has recently become a hot research field (97,98).
Due to their innate immune function and more prominent penetrating
ability, macrophages may kill tumor cells when T-cell therapy fails
(99). However, sufficient clinical
evidence is urgently needed to support pre-clinical data,
particularly in the field of GI cancer treatment.
In order to make adoptive cell therapy more readily
applicable and more effective in destroying tumor cells, relatively
more recent approaches have sought to introduce antitumor antigen
receptors to regular T cells, which may have promising therapeutic
applications. It is possible to eliminate the requirement for MHC
interaction and co-stimulatory molecules when T cells are
engineered to include chimeric antigen receptors (CAR), in which
the B-cell receptor-derived and T-cell receptor domains are
combined (100,101). To date, the antitumor qualities
from the adoptive transfer of CAR-T cells has been evident in the
case of advanced hematological malignancies, but in the case of
solid tumors the results have been less promising (102,103). It may be possible to explain this
as a consequence of the expression of heterogeneous tumor antigens,
the immunosuppressive network activity within the microenvironment
of the tumor, the T-cell trafficking into solid tumors, which is
less than optimal, and the absence of the necessary co-stimulatory
signals to achieve CAR-T cell persistence following infusion
(100,101). The affinity of HER2-directed CAR-T
cells for cancer cells of the GI tract is high, even for cells
exhibiting low levels of HER2 expression. Moreover, CAR-T-HER2
cells may offer the potential to inhibit disease recurrence of
metastasis. Specific CAR-T-HER2 cells have been developed, which
are consistently active within the cardiovascular system, and which
can accumulate within and inhibit tumors (104). In the context of PC, CAR-T-cell
therapy has been the subject of a number of studies. The
tumor-specific antigens of PC can be targeted by CAR-T-cell
therapy. In particular, antigens that are overexpressed, such as
CEA (NCT02349724), mesothelin (NCT02159716), HER2 (NCT02713984) and
MUC1 (NCT02587689), are promising targets. In HCC, there have been
no complete CAR-T-cell tests, but there is some evidence that the
antigens CEA, MUC1 and glypican-3 could be effectively targeted
(105,106). For GC, only a few studies have
examined CAR-T-cell therapy to date (107,108), but the results are cautiously
optimistic when developing CAR-T cells to target 3H11(109), despite an inability to overcome
the biological obstacles presented by solid tumors. A further study
based on the overexpression of the folate 1 receptor (FOLR1) in GC
compared with healthy tissue showed that FOLR1 CAR-T cells display
antitumor properties by recognizing FOLR1-positive GC cells
(110). In the case of
hepatobiliary cancer, small-scale trials have reported positive
outcomes of immunotherapy, and recent work has assessed the
potential of CAR-T cells when treating cancers of the biliary tract
(111). The suggested targets
include EGFR, mesothelin and HER2, due to their propensity to be
overexpressed in the aforementioned malignancies (112-114).
Although adoptive transfer therapy is promising and
intensely under review, the major obstacle of this approach in GI
cancer treatment is the heterogeneity of solid tumor, particularly
in colon and GC. The heterogenicity is caused by genomic
instability, which contributes to clonal evolution and immune
evasion resulting in immune-resistance and tumor recurrence.
Interestingly, combination treatment of cellular adoptive transfer
and chemotherapy can improve clinical outcomes and may prevent
recurrence in patients with advance GC that may be attributed to
the synergistic effect of ICD (115). Moreover, multiclonal elimination
of tumor cells could be improved by using multi-peptide vaccine or
broad-array tumor antigen (116,117). Overall, these would be the
solution for immune exhaustion in clinical settings of adoptive
therapies.
The implications of adoptive transfer of cytotoxic T
cells or CAR-T cells with ICD has not been extensively studied in
the context of GI cancer treatment. However, it has been shown that
the antitumor immune response of cytotoxic T cells may lead to
immunogenic tumor cell death, improving their own tumor
cell-killing capacity (118).
Interestingly, treatment with mitochondria-targeted small
molecules, including ATP, CRT and HMGB1, can induce upregulation of
ICD in both in vitro and in vivo models. This is
surprising, as priming by an ICD inducer effectively suppressed
tumor growth and lung metastasis by enhancing the adoptive T-cell
therapy against colon cancer in a mouse model (119). Moreover, it has been demonstrated
that the mitochondrial DAMPs could play a role as immunomodulators
through activation of γδ-T cells. Mitochondrial DAMPs induced
expression of TLR2 and TLR4, which may positively regulate the
antitumor response (120,121). TLR/type I IFN/CXCL10 has been
proposed as the signaling pathway implicated in the recruitment of
CXCR3+ T cells and the activation of γδ-T cells
(122). Hence, not only the direct
impact from activated antigen-presenting cells, but also
T-cell-based anticancer therapy may be targeted when considering
ICD (Table I). However, although
the implications of T-cell therapy and ICD appear to be very
promising, sufficient evidence is currently lacking.
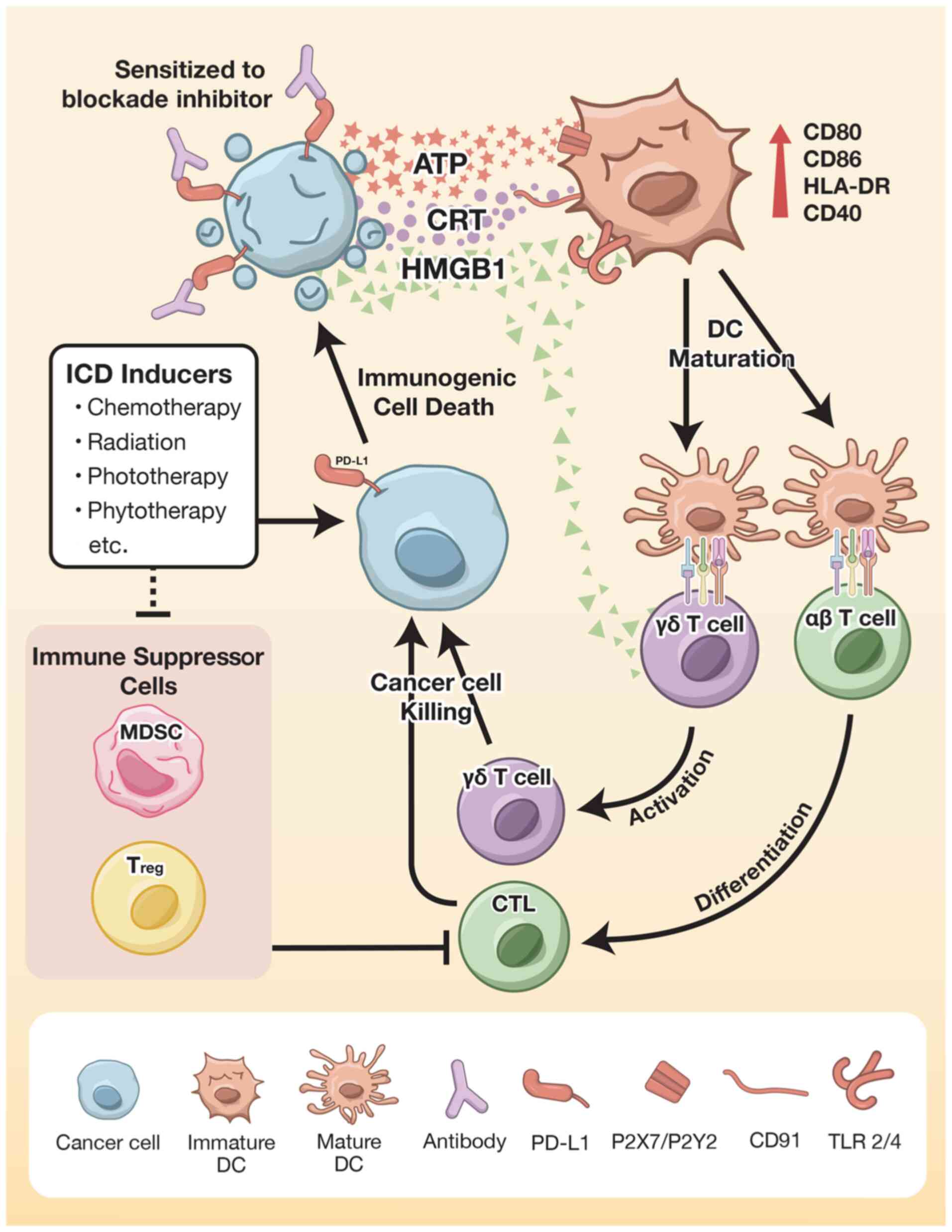
ICD plays a key role in enhancing the efficacy of
immunotherapy. DC-based anticancer vaccines directly activate and
strengthen the co-stimulatory signal through DAMPs to further
stimulate the immune response. The treatment outcomes from both the
immune checkpoint blockade and adoptive transfer cell therapy may
be enhanced by using ICD inducer agents. The mechanisms involving
ICD-enhanced immunotherapy in GI cancer treatment are demonstrated
in Fig. 1. These findings confirm
the effectiveness of induction therapies combined with
immunotherapy. Intervention may be implemented at only one or a few
cycles at effectively low doses to avoid adverse effects and to
obtain optimal ICD induction. Neoadjuvant chemotherapy can induce
either cancer cell apoptosis or necrosis, which effectively
promotes ICD induction, particularly HMGB1 release. In addition to
the HSP family, CRT and S100 protein expression is elicited by
chemotherapy and may be the primary DAMP molecules strengthening
the efficacy of immunotherapy. However, the use of ICD inducers in
immunotherapy for GI cancers has been limited due to a lack of
research evidence, accounting for only 5-10% of all clinical
trials. Further investigation should yield more positive outcomes
regarding the induction of ICD in immunotherapy for GI cancer.
Not applicable.
The present study was supported by the National Science Research
and Innovation Fund (NSRF) (grant nos. R2564B011, R2564B012,
R2563C029 and R2564B015) and the Thailand Science Research and
Innovations (TSRI) (grant no. BRG6180010).
Not applicable.
WS wrote the paper. CN designed and created the
graphic figure. SP and AJ wrote and edited the paper. All authors
have read and approved the final manuscript. Data authentication is
not applicable.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Rammensee HG: From basic immunology to new
therapies for cancer patients. In: Cancer Immunotherapy Meets.
Oncology. In Honor of Christoph Huber. Britten CM, Kreiter S, Diken
M and Rammensee HG (eds). Springer International Publishing, Cham,
pp3-11, 2014.
|
|
2
|
Galluzzi L, Buqué A, Kepp O, Zitvogel L
and Kroemer G: Immunogenic cell death in cancer and infectious
disease. Nat Rev Immunol. 17:97–111. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Matzinger P: Tolerance, danger, and the
extended family. Annual Rev Immunol. 12:991–1045. 1994.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Krysko DV, Garg AD, Kaczmarek A, Krysko O,
Agostinis P and Vandenabeele P: Immunogenic cell death and DAMPs in
cancer therapy. Nat Rev Cancer. 12:860–875. 2012.PubMed/NCBI View
Article : Google Scholar
|
|
5
|
Kroemer G, Galluzzi L, Kepp O and Zitvogel
L: Immunogenic cell death in cancer therapy. Annu Rev Immunol.
31:51–72. 2013.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Pol J, Vacchelli E, Aranda F, Castoldi F,
Eggermont A, Cremer I, Sautès-Fridman C, Fucikova J, Galon J,
Spisek R, et al: Trial Watch: Immunogenic cell death inducers for
anticancer chemotherapy. Oncoimmunology. 4(e1008866)2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kepp O, Senovilla L, Vitale I, Vacchelli
E, Adjemian S, Agostinis P, Apetoh L, Aranda F, Barnaba V, Bloy N,
et al: Consensus guidelines for the detection of immunogenic cell
death. Oncoimmunology. 3(e955691)2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Toomey PG, Vohra NA, Ghansah T, Sarnaik AA
and Pilon-Thomas SA: Immunotherapy for gastrointestinal
malignancies. Cancer Control. 20:32–42. 2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Rawla P and Barsouk A: Epidemiology of
gastric cancer: Global trends, risk factors and prevention.
Gastroenterol Rev. 14:26–38. 2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Grady WM and Carethers JM: Genomic and
epigenetic instability in colorectal cancer pathogenesis.
Gastroenterology. 135:1079–1099. 2008.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Morse MA, Hochster H and Benson A:
Perspectives on treatment of metastatic colorectal cancer with
immune checkpoint inhibitor therapy. Oncologist. 25:33–45.
2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Mittal S and El-Serag HB: Epidemiology of
hepatocellular carcinoma: Consider the population. J Clin
Gastroenterol. 47 (Suppl):S2–S6. 2013.PubMed/NCBI View Article : Google Scholar
|
|
14
|
McGlynn KA and London WT: The global
epidemiology of hepatocellular carcinoma: Present and future. Clin
Liver Dis. 15:223–243. 2011.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kamsa-Ard S, Luvira V, Suwanrungruang K,
Kamsa-Ard S, Luvira V, Santong C, Srisuk T, Pugkhem A,
Bhudhisawasdi V and Pairojkul C: Cholangiocarcinoma trends,
incidence, and relative survival in Khon Kaen, Thailand from 1989
through 2013: A population-based cancer registry study. J
Epidemiol. 29:197–204. 2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Bertuccio P, Malvezzi M, Carioli G, Hashim
D, Boffetta P, El-Serag HB, La Vecchia C and Negri E: Global trends
in mortality from intrahepatic and extrahepatic cholangiocarcinoma.
J Hepatol. 71:104–114. 2019.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Blechacz B: Cholangiocarcinoma: Current
knowledge and new developments. Gut Liver. 11:13–26.
2017.PubMed/NCBI View
Article : Google Scholar
|
|
18
|
Banales JM, Marin JJG, Lamarca A,
Rodrigues PM, Khan SA, Roberts LR, Cardinale V, Carpino G, Andersen
JB, Braconi C, et al: Cholangiocarcinoma 2020: The next horizon in
mechanisms and management. Nat Rev Gastroenterol Hepatol.
17:557–588. 2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Sripa B and Pairojkul C:
Cholangiocarcinoma: Lessons from Thailand. Curr Opin Gastroenterol.
24:349–356. 2008.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Pereira NP and Corrêa JR: Pancreatic
cancer: Treatment approaches and trends. J Cancer Metastasis Treat.
4(18)2018.
|
|
21
|
Matsuoka T and Yashiro M: Precision
medicine for gastrointestinal cancer: Recent progress and future
perspective. World J Gastrointest Oncol. 12:1–20. 2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Abdul-Latif M, Townsend K, Dearman C, Shiu
KK and Khan K: Immunotherapy in gastrointestinal cancer: The
current scenario and future perspectives. Cancer Treat Rev.
88(102030)2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Tannapfel A and Reinacher-Schick A:
Immunotherapy in gastrointestinal cancer: Where Do We Stand? Visc
Med. 35:1–2. 2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Suntharalingam M, Winter K, Ilson DH,
Dicker A, Kachnic LA, Chakravarthy AAK, Gaffney DK, Thakrar HV,
Horiba MN, Deutsch M, et al: The initial report of RTOG 0436: A
phase III trial evaluating the addition of cetuximab to paclitaxel,
cisplatin, and radiation for patients with esophageal cancer
treated without surgery. J Clin Oncol. 32:LBA6. 2014.
|
|
25
|
O'Connell MJ, Colangelo LH, Beart RW,
Petrelli NJ, Allegra CJ, Sharif S, Pitot HC, Shields AF, Landry JC,
Ryan DP, et al: Capecitabine and oxaliplatin in the preoperative
multimodality treatment of rectal cancer: Surgical end points from
national surgical adjuvant breast and bowel project trial R-04. J
Clin Oncol. 32:1927–1934. 2014.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Mortara L, Balza E, Bruno A, Poggi A,
Orecchia P and Carnemolla B: Anti-cancer therapies employing il-2
cytokine tumor targeting: Contribution of innate, adaptive and
immunosuppressive cells in the anti-tumor efficacy. Front Immunol.
9(2905)2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Hollingsworth RE and Jansen K: Turning the
corner on therapeutic cancer vaccines. NPJ Vaccines.
4(7)2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Cheever MA and Higano CS: PROVENGE
(Sipuleucel-T) in prostate cancer: The first FDA-approved
therapeutic cancer vaccine. Clin Cancer Res. 17:3520–3526.
2011.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Kudrin A: Overview of cancer vaccines:
Considerations for development. Hum Vaccin Immunother. 8:1335–1353.
2012.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Reitsma DJ and Combest AJ: Challenges in
the development of an autologous heat shock protein based
anti-tumor vaccine. Hum Vaccin Immunother. 8:1152–1155.
2012.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Ozao-Choy J, Lee DJ and Faries MB:
Melanoma vaccines: Mixed past, promising future. Surg Clin North
Am. 94:1017–1030. 2014.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Niccolai E, Taddei A, Prisco D and Amedei
A: Gastric cancer and the epoch of immunotherapy approaches. World
J Gastroenterol. 21:5778–5793. 2015.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Morse MA, Deng Y, Coleman D, Hull S,
Kitrell-Fisher E, Nair S, Schlom J, Ryback ME and Lyerly HK: A
Phase I study of active immunotherapy with carcinoembryonic antigen
peptide (CAP-1)-pulsed, autologous human cultured dendritic cells
in patients with metastatic malignancies expressing
carcinoembryonic antigen. Clin Cancer Res. 5:1331–1338.
1999.PubMed/NCBI
|
|
34
|
Li J, Valentin A, Beach RK, Alicea C,
Felber BK and Pavlakis GN: DNA is an efficient booster of dendritic
cell-based vaccine. Hum Vaccin Immunother. 11:1927–1935.
2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Maeda Y, Yoshimura K, Matsui H, Shindo Y,
Tamesa T, Tokumitsu Y, Hashimoto N, Tokuhisa Y, Sakamoto K, Sakai
K, et al: Dendritic cells transfected with heat-shock protein 70
messenger RNA for patients with hepatitis C virus-related
hepatocellular carcinoma: A phase 1 dose escalation clinical trial.
Cancer Immunol Immunother. 64:1047–1056. 2015.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Song W, Kong HL, Carpenter H, Torii H,
Granstein R, Rafii S, Moore MA and Crystal RG: Dendritic cells
genetically modified with an adenovirus vector encoding the cDNA
for a model antigen induce protective and therapeutic antitumor
immunity. J Exp Med. 186:1247–1256. 1997.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Jiraviriyakul A, Songjang W, Kaewthet P,
Tanawatkitichai P, Bayan P and Pongcharoen S: Honokiol-enhanced
cytotoxic T lymphocyte activity against cholangiocarcinoma cells
mediated by dendritic cells pulsed with damage-associated molecular
patterns. World J Gastroenterol. 25:3941–3955. 2019.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Gottfried E, Krieg R, Eichelberg C,
Andreesen R, Mackensen A and Krause SW: Characterization of cells
prepared by dendritic cell-tumor cell fusion. Cancer Immun.
2(15)2002.PubMed/NCBI
|
|
39
|
Kavanagh B, Ko A, Venook A, Margolin K,
Zeh H, Lotze M, Schillinger B, Liu W, Lu Y, Mitsky P, et al:
Vaccination of metastatic colorectal cancer patients with matured
dendritic cells loaded with multiple major histocompatibility
complex class I peptides. J Immunother. 30:762–772. 2007.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Vonderheide RH, Domchek SM, Schultze JL,
George DJ, Hoar KM, Chen DY, Stephans KF, Masutomi K, Loda M, Xia
Z, et al: Vaccination of cancer patients against telomerase induces
functional antitumor CD8+ T lymphocytes. Clin Cancer Res.
10:828–839. 2004.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Rosalia RA, Quakkelaar ED, Redeker A, Khan
S, Camps M, Drijfhout JW, Silva AL, Jiskoot W, van Hall T, van
Veelen PA, et al: Dendritic cells process synthetic long peptides
better than whole protein, improving antigen presentation and
T-cell activation. Eur J Immunol. 43:2554–2565. 2013.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Medema JP, Schuurhuis DH, Rea D, van
Tongeren J, de Jong J, Bres SA, Laban S, Toes RE, Toebes M,
Schumacher TN, et al: Expression of the serpin serine protease
inhibitor 6 protects dendritic cells from cytotoxic T
lymphocyte-induced apoptosis: Differential modulation by T helper
type 1 and type 2 cells. J Exp Med. 194:657–667. 2001.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Zhang QM, He SJ, Shen N, Luo B, Fan R, Fu
J, Luo GR, Zhou SF, Xiao SW and Xie XX: Overexpression of MAGE-D4
in colorectal cancer is a potentially prognostic biomarker and
immunotherapy target. Int J Clin Exp Pathol. 7:3918–3927.
2014.PubMed/NCBI
|
|
44
|
Kono K, Takahashi A, Sugai H, Fujii H,
Choudhury AR, Kiessling R and Matsumoto Y: Dendritic cells pulsed
with HER-2/neu-derived peptides can induce specific T-cell
responses in patients with gastric cancer. Clin Cancer Res.
8:3394–3400. 2002.PubMed/NCBI
|
|
45
|
Smith AM, Justin T, Michaeli D and Watson
SA: Phase I/II study of G17-DT, an Anti-gastrin immunogen, in
advanced colorectal cancer. Clin Cancer Res. 6:4719–4724.
2000.PubMed/NCBI
|
|
46
|
Higashihara Y, Kato J, Nagahara A, Izumi
K, Konishi M, Kodani T, Serizawa N, Osada T and Watanabe S: Phase I
clinical trial of peptide vaccination with URLC10 and VEGFR1
epitope peptides in patients with advanced gastric cancer Int J.
Oncol. 44:662–668. 2014.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Mazzaferro V, Coppa J, Carrabba MG,
Rivoltini L, Schiavo M, Regalia E, Mariani L, Camerini T, Marchianò
A, Andreola S, et al: Vaccination with autologous tumor-derived
heat-shock protein gp96 after liver resection for metastatic
colorectal cancer. Clin Cancer Res. 9:3235–3245. 2003.PubMed/NCBI
|
|
48
|
Dolcetti R, De Re V and Canzonieri V:
Immunotherapy for gastric cancer: Time for a Personalized Approach?
Int J Mol Sci. 19(1602)2018.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Le DT, Lutz E, Uram JN, Sugar EA, Onners
B, Solt S, Zheng L, Diaz LA Jr, Donehower RC, Jaffee EM and Laheru
DA: Evaluation of ipilimumab in combination with allogeneic
pancreatic tumor cells transfected with a GM-CSF gene in previously
treated pancreatic cancer. J Immunother. 36:382–389.
2013.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Ikeda M, Okusaka T, Ohno I, Mitsunaga S,
Kondo S, Ueno H, Morizane C, Gemmoto K, Suna H, Ushida Y and Furuse
J: Phase I studies of peptide vaccine cocktails derived from GPC3,
WDRPUH and NEIL3 for advanced hepatocellular carcinoma.
Immunotherapy. 13:371–385. 2021.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Butterfield LH, Ribas A, Meng WS, Dissette
VB, Amarnani S, Vu HT, Seja E, Todd K, Glaspy JA, McBride WH and
Economou JS: T-cell responses to HLA-A*0201 immunodominant peptides
derived from alpha-fetoprotein in patients with hepatocellular
cancer. Clin Cancer Res. 9:5902–5908. 2003.PubMed/NCBI
|
|
52
|
Tsuchiya N, Yoshikawa T, Fujinami N, Saito
K, Mizuno S, Sawada Y, Endo I and Nakatsura T: Immunological
efficacy of glypican-3 peptide vaccine in patients with advanced
hepatocellular carcinoma. Oncoimmunology.
6(e1346764)2017.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Zhang Q, Chen G, Peng L, Wang X, Yang Y,
Liu C, Shi W, Su C, Wu H, Liu X, et al: Increased safety with
preserved antitumoral efficacy on hepatocellular carcinoma with
dual-regulated oncolytic adenovirus. Clin Cancer Res. 12:6523–6531.
2006.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Lepisto AJ, Moser AJ, Zeh H, Lee K,
Bartlett D, McKolanis JR, Geller BA, Schmotzer A, Potter DP,
Whiteside T, et al: A phase I/II study of a MUC1 peptide pulsed
autologous dendritic cell vaccine as adjuvant therapy in patients
with resected pancreatic and biliary tumors. Cancer Ther.
6:955–964. 2008.PubMed/NCBI
|
|
55
|
Kawamura J, Sugiura F, Sukegawa Y,
Yoshioka Y, Hida JI, Hazama S and Okuno K: Multicenter, phase II
clinical trial of peptide vaccination with oral chemotherapy
following curative resection for stage III colorectal cancer.
Oncology Lett. 15:4241–4247. 2018.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Rahma OE, Hamilton JM, Wojtowicz M,
Dakheel O, Bernstein S, Liewehr DJ, Steinberg SM and Khleif SN: The
immunological and clinical effects of mutated ras peptide vaccine
in combination with IL-2, GM-CSF, or both in patients with solid
tumors. J Transl Med. 12(55)2014.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Quandt J, Schlude C, Bartoschek M, Will R,
Cid-Arregui A, Schölch S, Reissfelder C, Weitz J, Schneider M,
Wiemann S, et al: Long-peptide vaccination with driver gene
mutations in p53 and Kras induces cancer mutation-specific effector
as well as regulatory T cell responses. Oncoimmunology.
7(e1500671)2018.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Hessmann E, Patzak MS, Klein L, Chen N,
Kari V, Ramu I, Bapiro TE, Frese KK, Gopinathan A, Richards FM, et
al: Fibroblast drug scavenging increases intratumoural gemcitabine
accumulation in murine pancreas cancer. Gut. 67:497–507.
2018.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Scarpa M, Ruffolo C, Canal F, Scarpa M,
Basato S, Erroi F, Fiorot A, Dall'Agnese L, Pozza A, Porzionato A,
et al: Mismatch repair gene defects in sporadic colorectal cancer
enhance immune surveillance. Oncotarget. 6:43472–43482.
2015.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Marabelle A, Le DT, Ascierto PA, Di
Giacomo AM, De Jesus-Acosta A, Delord JP, Geva R, Gottfried M,
Penel N, Hansen AR, et al: Efficacy of Pembrolizumab in patients
with noncolorectal high microsatellite Instability/Mismatch
Repair-deficient cancer: Results from the phase II KEYNOTE-158
Study. J Clin Oncol. 38:1–10. 2019.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Fucikova J, Kepp O, Kasikova L, Petroni G,
Yamazaki T, Liu P, Zhao L, Spisek R, Kroemer G and Galluzzi L:
Detection of immunogenic cell death and its relevance for cancer
therapy. Cell Death Dis. 11(1013)2020.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Suzuki Y, Mimura K, Yoshimoto Y, Watanabe
M, Ohkubo Y, Izawa S, Murata K, Fujii H, Nakano T and Kono K:
Immunogenic tumor cell death induced by chemoradiotherapy in
patients with esophageal squamous cell carcinoma. Cancer Res.
72:3967–3976. 2012.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Ratschker T, Egenberger L, Alev M,
Zschiesche L, Band J, Schreiber E, Frey B, Derer A, Alexiou C and
Janko C: Mitoxantrone-loaded nanoparticles for magnetically
controlled tumor therapy-induction of tumor cell death, release of
danger signals and activation of immune cells. Pharmaceutics.
12(923)2020.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Zhao X, Yang K, Zhao R, Ji T, Wang X, Yang
X, Zhang Y, Cheng K, Liu S, Hao J, et al: Inducing enhanced
immunogenic cell death with nanocarrier-based drug delivery systems
for pancreatic cancer therapy. Biomaterials. 102:187–197.
2016.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Turrini E, Catanzaro E, Muraro MG, Governa
V, Trella E, Mele V, Calcabrini C, Morroni F, Sita G, Hrelia P, et
al: Hemidesmus indicus induces immunogenic death in human
colorectal cancer cells. Oncotarget. 9:24443–24456. 2018.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Wu CJ, Tsai YT, Lee IJ, Wu PY, Lu LS, Tsao
WS, Huang YJ, Chang CC, Ka SM and Tao MH: Combination of radiation
and interleukin 12 eradicates large orthotopic hepatocellular
carcinoma through immunomodulation of tumor microenvironment.
Oncoimmunology. 7(e1477459)2018.PubMed/NCBI View Article : Google Scholar
|
|
67
|
He H, Liu L, Liang R, Zhou H, Pan H, Zhang
S and Cai L: Tumor-targeted nanoplatform for in situ
oxygenation-boosted immunogenic phototherapy of colorectal cancer.
Acta Biomaterialia. 104:188–197. 2020.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Van Loenhout J, Flieswasser T, Freire
Boullosa L, De Waele J, Van Audenaerde J, Marcq E, Jacobs J, Lin A,
Lion E, Dewitte H, et al: Cold atmospheric plasma-treated PBS
eliminates immunosuppressive pancreatic stellate cells and induces
immunogenic cell death of pancreatic cancer cells. Cancers.
11(1597)2019.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Pardoll DM: The blockade of immune
checkpoints in cancer immunotherapy. Nat Rev Cancer. 12:252–264.
2012.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Tivol EA, Borriello F, Schweitzer AN,
Lynch WP, Bluestone JA and Sharpe AH: Loss of CTLA-4 leads to
massive lymphoproliferation and fatal multiorgan tissue
destruction, revealing a critical negative regulatory role of
CTLA-4. Immunity. 3:541–547. 1995.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Borch TH, Donia M, Andersen MH and Svane
IM: Reorienting the immune system in the treatment of cancer by
using anti-PD-1 and anti-PD-L1 antibodies. Drug Discov Today.
20:1127–1134. 2015.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Schildberg FA, Klein SR, Freeman GJ and
Sharpe AH: Coinhibitory pathways in the B7-CD28 ligand-receptor
family. Immunity. 44:955–972. 2016.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Lee B, Hutchinson R, Wong HL, Tie J,
Putoczki T, Tran B, Gibbs P and Christie M: Emerging biomarkers for
immunomodulatory cancer treatment of upper gastrointestinal,
pancreatic and hepatic cancers. Semin Cancer Biol. 52:241–252.
2018.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Zhou G, Noordam L, Sprengers D, Doukas M,
Boor PPC, van Beek AA, Erkens R, Mancham S, Grünhagen D, Menon AG,
et al: Blockade of LAG3 enhances responses of tumor-infiltrating T
cells in mismatch repair-proficient liver metastases of colorectal
cancer. Oncoimmunology. 7(e1448332)2018.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Huyghe N, Baldin P and Van den Eynde M:
Immunotherapy with immune checkpoint inhibitors in colorectal
cancer: What is the future beyond deficient mismatch-repair
tumours? Gastroenterol Rep (Oxf). 8:11–24. 2020.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Chung KY, Gore I, Fong L, Venook A, Beck
SB, Dorazio P, Criscitiello PJ, Healey DI, Huang B, Gomez-Navarro J
and Saltz LB: Phase II study of the anti-cytotoxic
T-Lymphocyte-associated antigen 4 monoclonal antibody,
tremelimumab, in patients with refractory metastatic colorectal
cancer. J Clin Oncol. 28:3485–3490. 2010.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Torphy RJ, Zhu Y and Schulick RD:
Immunotherapy for pancreatic cancer: Barriers and breakthroughs.
Ann Gastroenterol Surg. 2:274–281. 2018.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Kudo M, Matilla A, Santoro A, Melero I,
Gracian AC, Acosta-Rivera M, Choo SP, El-Khoueiry AB, Kuromatsu R,
El-Rayes BF, et al: Checkmate-040: Nivolumab (NIVO) in patients
(pts) with advanced hepatocellular carcinoma (aHCC) and Child-Pugh
B (CPB) status. J Clin Oncol. 37(327)2019.
|
|
79
|
Ledford H, Else H and Warren M: Cancer
immunologists scoop medicine Nobel prize. Nature. 562:20–21.
2018.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Sakakibara K, Sato T, Kufe DW, VonHoff DD
and Kawabe T: CBP501 induces immunogenic tumor cell death and CD8 T
cell infiltration into tumors in combination with platinum, and
increases the efficacy of immune checkpoint inhibitors against
tumors in mice. Oncotarget. 8:78277–78288. 2017.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Landry MR, DuRoss AN, Neufeld MJ, Hahn L,
Sahay G, Luxenhofer R and Sun C: Low dose novel PARP-PI3K
inhibition via nanoformulation improves colorectal cancer
immunoradiotherapy. Materials today Bio. 8(100082)2020.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Zhu H, Shan Y, Ge K, Lu J, Kong W and Jia
C: Oxaliplatin induces immunogenic cell death in hepatocellular
carcinoma cells and synergizes with immune checkpoint blockade
therapy. Cell Oncol (Dordr). 43:1203–1214. 2020.PubMed/NCBI View Article : Google Scholar
|
|
83
|
Maruoka Y, Furusawa A, Okada R, Inagaki F,
Fujimura D, Wakiyama H, Kato T, Nagaya T, Choyke PL and Kobayashi
H: Near-infrared photoimmunotherapy combined with CTLA4 checkpoint
blockade in syngeneic mouse cancer models. Vaccines (Basel).
8(528)2020.PubMed/NCBI View Article : Google Scholar
|
|
84
|
Antoniotti C, Borelli B, Rossini D,
Pietrantonio F, Morano F, Salvatore L, Lonardi S, Marmorino F,
Tamberi S, Corallo S, et al: AtezoTRIBE: A randomised phase II
study of FOLFOXIRI plus bevacizumab alone or in combination with
atezolizumab as initial therapy for patients with unresectable
metastatic colorectal cancer. BMC Cancer. 20(683)2020.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Fumet JD, Isambert N, Hervieu A, Zanetta
S, Guion JF, Hennequin A, Rederstorff E, Bertaut A and Ghiringhelli
F: Phase Ib/II trial evaluating the safety, tolerability and
immunological activity of durvalumab (MEDI4736) (anti-PD-L1) plus
tremelimumab (anti-CTLA-4) combined with FOLFOX in patients with
metastatic colorectal cancer. ESMO Open. 3(e000375)2018.PubMed/NCBI View Article : Google Scholar
|
|
86
|
Bang YJ, Muro K, Fuchs CS, Golan T, Geva
R, Hara H, Jalal SI, Borg C, Doi T, Wainberg ZA, et al: KEYNOTE-059
cohort 2: Safety and efficacy of pembrolizumab (pembro) plus
5-fluorouracil (5-FU) and cisplatin for first-line (1L) treatment
of advanced gastric cancer. J Clin Oncol. 35(4012)2017.
|
|
87
|
Bailly C, Thuru X and Quesnel B: Combined
cytotoxic chemotherapy and immunotherapy of cancer: Modern times.
NAR Cancer. 2(zcaa002)2020.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Dosset M, Vargas TR, Lagrange A, Boidot R,
Végran F, Roussey A, Chalmin F, Dondaine L, Paul C, Lauret
Marie-Joseph E, et al: PD-1/PD-L1 pathway: An adaptive immune
resistance mechanism to immunogenic chemotherapy in colorectal
cancer. Oncoimmunology. 7(e1433981)2018.PubMed/NCBI View Article : Google Scholar
|
|
89
|
Chu TH, Chan HH, Hu TH, Wang EM, Ma YL,
Huang SC, Wu JC, Chang YC, Weng WT, Wen ZH, et al: Celecoxib
enhances the therapeutic efficacy of epirubicin for Novikoff
hepatoma in rats. Cancer Med. 7:2567–2580. 2018.PubMed/NCBI View Article : Google Scholar
|
|
90
|
Wang F, Lau JKC and Yu J: The role of
natural killer cell in gastrointestinal cancer: Killer or helper.
Oncogene. 40:717–730. 2021.PubMed/NCBI View Article : Google Scholar
|
|
91
|
Amedei A, Niccolai E and D'Elios MM: T
cells and adoptive immunotherapy: Recent developments and future
prospects in gastrointestinal oncology. Clin Dev Immunol.
2011(320571)2011.PubMed/NCBI View Article : Google Scholar
|
|
92
|
Guo Y and Han W: Cytokine-induced killer
(CIK) cells: From basic research to clinical translation. Chin J
Cancer. 34:99–107. 2015.PubMed/NCBI View Article : Google Scholar
|
|
93
|
Sakamoto N, Ishikawa T, Kokura S, Okayama
T, Oka K, Ideno M, Sakai F, Kato A, Tanabe M, Enoki T, et al: Phase
I clinical trial of autologous NK cell therapy using novel
expansion method in patients with advanced digestive cancer. J
Transl Med. 13(277)2015.PubMed/NCBI View Article : Google Scholar
|
|
94
|
Shiozawa M, Chang CH, Huang YC, Chen YC,
Chi MS, Hao HC, Chang YC, Takeda S, Chi KH and Wang YS:
Pharmacologically upregulated carcinoembryonic antigen-expression
enhances the cytolytic activity of genetically-modified chimeric
antigen receptor NK-92MI against colorectal cancer cells. BMC
Immunol. 19(27)2018.PubMed/NCBI View Article : Google Scholar
|
|
95
|
Liu B, Liu ZZ, Zhou ML, Lin JW, Chen XM,
Li Z, Gao WB, Yu ZD and Liu T: Development of c-MET-specific
chimeric antigen receptor-engineered natural killer cells with
cytotoxic effects on human liver cancer HepG2 cells. Mol Med Rep.
20:2823–2831. 2019.PubMed/NCBI View Article : Google Scholar
|
|
96
|
Krause SW, Gastpar R, Andreesen R, Gross
C, Ullrich H, Thonigs G, Pfister K and Multhoff G: Treatment of
colon and lung cancer patients with ex vivo heat shock protein
70-peptide-activated, autologous natural killer cells: A clinical
phase i trial. Clin Cancer Res. 10:3699–3707. 2004.PubMed/NCBI View Article : Google Scholar
|
|
97
|
Andreesen R, Scheibenbogen C, Brugger W,
Krause S, Meerpohl HG, Leser HG, Engler H and Löhr GW: Adoptive
transfer of tumor cytotoxic macrophages generated in vitro from
circulating blood monocytes: A new approach to cancer
immunotherapy. Cancer Res. 50:7450–7456. 1990.PubMed/NCBI
|
|
98
|
Klichinsky M, Ruella M, Shestova O, Lu XM,
Best A, Zeeman M, Schmierer M, Gabrusiewicz K, Anderson NR, Petty
NE, et al: Human chimeric antigen receptor macrophages for cancer
immunotherapy. Nat Biotechnol. 38:947–953. 2020.PubMed/NCBI View Article : Google Scholar
|
|
99
|
Liu Y and Wang R: Immunotherapy targeting
tumor-associated macrophages. Front Med (Lausanne).
7(583708)2020.PubMed/NCBI View Article : Google Scholar
|
|
100
|
Fesnak AD, June CH and Levine BL:
Engineered T cells: The promise and challenges of cancer
immunotherapy. Nat Rev Cancer. 16:566–581. 2016.PubMed/NCBI View Article : Google Scholar
|
|
101
|
Mirzaei HR, Rodriguez A, Shepphird J,
Brown CE and Badie B: Chimeric antigen receptors T cell therapy in
solid tumor: Challenges and clinical applications. Front Immunol.
8(1850)2017.PubMed/NCBI View Article : Google Scholar
|
|
102
|
Neelapu SS, Locke FL, Bartlett NL, Lekakis
LJ, Miklos DB, Jacobson CA, Braunschweig I, Oluwole OO, Siddiqi T,
Lin Y, et al: Axicabtagene ciloleucel CAR T-cell therapy in
refractory large B-cell lymphoma. N Engl J Med. 377:2531–2544.
2017.PubMed/NCBI View Article : Google Scholar
|
|
103
|
Hou B, Tang Y, Li W, Zeng Q and Chang D:
Efficiency of CAR-T therapy for treatment of solid tumor in
clinical trials: A meta-analysis. Disease Markers.
2019(3425291)2019.PubMed/NCBI View Article : Google Scholar
|
|
104
|
Bebnowska D, Grywalska E,
Niedźwiedzka-Rystwej P, Sosnowska-Pasiarska B, Smok-Kalwat J,
Pasiarski M, Góźdź S, Roliński J and Polkowski W: CAR-T cell
therapy-an overview of targets in gastric cancer. J Clin Med.
9(1894)2020.PubMed/NCBI View Article : Google Scholar
|
|
105
|
Alrifai D, Sarker D and Maher J: Prospects
for adoptive immunotherapy of pancreatic cancer using chimeric
antigen receptor-engineered T-cells. Immunopharm Immunot. 38:50–60.
2016.PubMed/NCBI View Article : Google Scholar
|
|
106
|
Cheng X, Zhao G and Zhao Y: Combination
immunotherapy approaches for pancreatic cancer treatment. Can J
Gastroenterol Hepatol. 2018(6240467)2018.PubMed/NCBI View Article : Google Scholar
|
|
107
|
Song Y, Tong C, Wang Y, Gao Y, Dai H, Guo
Y, Zhao X, Wang Y, Wang Z, Han W and Chen L: Effective and
persistent antitumor activity of HER2-directed CAR-T cells against
gastric cancer cells in vitro and xenotransplanted tumors in vivo.
Protein Cell. 9:867–878. 2018.PubMed/NCBI View Article : Google Scholar
|
|
108
|
Tao K, He M, Tao F, Xu G, Ye M, Zheng Y
and Li Y: Development of NKG2D-based chimeric antigen receptor-T
cells for gastric cancer treatment. Cancer Chemother Pharmacol.
82:815–827. 2018.PubMed/NCBI View Article : Google Scholar
|
|
109
|
Han H, Wang S, Hu Y, Li Z, Yang W, Lv Y,
Wang L, Zhang L and Ji J: Monoclonal antibody 3H11 chimeric antigen
receptors enhance T cell effector function and exhibit efficacy
against gastric cancer. Oncol Lett. 15:6887–6894. 2018.PubMed/NCBI View Article : Google Scholar
|
|
110
|
Kim M, Pyo S, Kang CH, Lee CO, Lee HK,
Choi SU and Park CH: Folate receptor 1 (FOLR1) targeted chimeric
antigen receptor (CAR) T cells for the treatment of gastric cancer.
PLoS One. 13(e0198347)2018.PubMed/NCBI View Article : Google Scholar
|
|
111
|
DeLeon TT, Zhou YM, Nagalo BM, Yokoda RT,
Ahn DH, Ramanathan RK, Salomao MA, Aqel BA, Mahipal A, Bekaii-Saab
TS and Borad MJ: Novel immunotherapy strategies for hepatobiliary
cancers. Immunotherapy. 10:1077–1091. 2018.PubMed/NCBI View Article : Google Scholar
|
|
112
|
Xu JY, Ye ZL, Jiang DQ, He JC, Ding YM, Li
LF, Lv SQ, Wang Y, Jin HJ and Qian QJ: Mesothelin-targeting
chimeric antigen receptor-modified T cells by piggyBac transposon
system suppress the growth of bile duct carcinoma. Tumor Biol.
39(1010428317695949)2017.PubMed/NCBI View Article : Google Scholar
|
|
113
|
Guo Y, Feng K, Liu Y, Wu Z, Dai H, Yang Q,
Wang Y, Jia H and Han W: Phase I study of chimeric antigen
receptor-modified T cells in patients with EGFR-positive advanced
biliary tract cancers. Clin Cancer Res. 24:1277–1286.
2018.PubMed/NCBI View Article : Google Scholar
|
|
114
|
Yan M, Schwaederle M, Arguello D, Millis
SZ, Gatalica Z and Kurzrock R: HER2 expression status in diverse
cancers: Review of results from 37,992 patients. Cancer Metastasis
Rev. 34:157–164. 2015.PubMed/NCBI View Article : Google Scholar
|
|
115
|
Cui J, Li L, Wang C, Jin H, Yao C, Wang Y,
Li D, Tian H, Niu C, Wang G, et al: Combined cellular immunotherapy
and chemotherapy improves clinical outcome in patients with gastric
carcinoma. Cytotherapy. 17:979–988. 2015.PubMed/NCBI View Article : Google Scholar
|
|
116
|
El-Sayes N, Vito A and Mossman K: Tumor
heterogeneity: A great barrier in the age of cancer immunotherapy.
Cancers. 13(806)2021.PubMed/NCBI View Article : Google Scholar
|
|
117
|
Walter S, Weinschenk T, Stenzl A, Zdrojowy
R, Pluzanska A, Szczylik C, Staehler M, Brugger W, Dietrich PY,
Mendrzyk R, et al: Multipeptide immune response to cancer vaccine
IMA901 after single-dose cyclophosphamide associates with longer
patient survival. Nat Med. 18:1254–1261. 2012.PubMed/NCBI View Article : Google Scholar
|
|
118
|
Minute L, Teijeira A, Sanchez-Paulete AR,
Ochoa MC, Alvarez M, Otano I, Etxeberrria I, Bolaños E, Azpilikueta
A, Garasa S, et al: Cellular cytotoxicity is a form of immunogenic
cell death. J Immunother Cancer. 8(e000325)2020.PubMed/NCBI View Article : Google Scholar
|
|
119
|
Jiang Q, Zhang C, Wang H, Peng T, Zhang L,
Wang Y, Han W and Shi C: Mitochondria-targeting immunogenic cell
death inducer improves the adoptive T-cell therapy against solid
tumor. Front Oncol. 9(1196)2019.PubMed/NCBI View Article : Google Scholar
|
|
120
|
Schwacha MG, Rani M, Nicholson SE, Lewis
AM, Holloway TL, Sordo S and Cap AP: Dermal γδ T-cells can be
activated by mitochondrial damage-associated molecular patterns.
PLoS One. 11(e0158993)2016.PubMed/NCBI View Article : Google Scholar
|
|
121
|
Schwacha MG, Rani M, Zhang Q, Nunez-Cantu
O and Cap AP: Mitochondrial damage-associated molecular patterns
activate γδ T-cells. Innate immunity. 20:261–268. 2014.PubMed/NCBI View Article : Google Scholar
|
|
122
|
Gebremeskel S and Johnston B: Concepts and
mechanisms underlying chemotherapy induced immunogenic cell death:
Impact on clinical studies and considerations for combined
therapies. Oncotarget. 6:41600–41619. 2015.PubMed/NCBI View Article : Google Scholar
|
|
123
|
Xie W, Forveille S, Iribarren K, Sauvat A,
Senovilla L, Wang Y, Humeau J, Perez-Lanzon M, Zhou H,
Martínez-Leal JF, et al: Lurbinectedin synergizes with immune
checkpoint blockade to generate anticancer immunity.
Oncoimmunology. 8(e1656502)2019.PubMed/NCBI View Article : Google Scholar
|
|
124
|
Limagne E, Thibaudin M, Nuttin L, Spill A,
Derangère V, Fumet JD, Amellal N, Peranzoni E, Cattan V and
Ghiringhelli F: Trifluridine/Tipiracil plus Oxaliplatin improves
PD-1 blockade in colorectal cancer by inducing immunogenic cell
death and depleting macrophages. Cancer Immunol Res. 7:1958–1969.
2019.PubMed/NCBI View Article : Google Scholar
|