Introduction
Mesothelioma is an aggressive tumor arising from the
mesothelium, a membrane lining various body cavities, including the
pleura, peritoneum and pericardium, and is usually associated with
asbestos exposure.
Due to the long incubation period and the short
survival time after the onset of asbestos-induced malignant
mesothelioma (MM), an early diagnostic system for individuals with
a history of asbestos exposure is critically required. Recently,
soluble mesothelin-related protein (1) and serum mesothelin have been reported
to be potentially useful markers for the early diagnosis of MM
(2,3).
A 71-kDa precursor protein of human ERC/mesothelin
can be cleaved into a 40-kDa C-terminal fragment as a surface
GPI-anchored glycoprotein and a 31-kDa N-terminal fragment as a
secreted protein. We focused on this N-ERC/mesothelin, as it is
physiologically secreted into the blood, and as a specific ELISA
system has been developed for N-ERC/mesothelin (2,3).
In the present study, to develop a pre-clinical
diagnostic system for the early detection of MM, the levels of
N-ERC/mesothelin, the N-terminal 31-kDa fragment of mesothelin, in
blood samples was measured by ELISA as a primary screening method.
Chest radiography, chest CT and positron emission tomography (PET)
examinations, and also histopathology, were then used as secondary
screening examinations for individuals with a history of exposure
to asbestos and consequently, a high risk of developing of MM.
Materials and methods
Establishment of ELISA for
N-ERC/mesothelin and measurement of blood samples
The sandwich ELISA system used in this report were
established as described previously (3). The 7E7 MoAb was used as the capture
antibody and the 16K16 MoAb was used as the detecting antibody
after conjugation with horseradish peroxidase. Recombinant
N-ERC/mesothelin was used as the standard. The protein in the ELISA
system was purified from culture supernatants of CHO-K1 cells
transfected with ERC/mesothelin cDNA using an anti-ERC/mesothelin
PoAb. EDTA plasma was used for this ELISA.
The present study was approved by the Institutional
Review Board of Juntendo University School of Medicine, its
hospital and Immuno-Biological Laboratories. Written informed
consent for participation in the study was obtained from all of the
subjects.
Results
Case reports of three patients
Patient A: clinical history
The subject was a 71-year-old male who had a history
of smoking for 58 years. He did not have any clinical complaints or
significant past medical history. The patient had an occupational
history of employment as a plumber using asbestos for pipe
insulation since the age of 24 years.
History of present illness
The subject underwent a physical examination in June
2007, at which time his plasma N-ERC/mesothelin level was 8.62
ng/ml, which was higher than the cutoff value (3).
He subsequently underwent secondary screening.
Although a chest CT revealed bilateral pleural thickening with
calcification, no abnormal findings in the abdominal area or
interior of the pelvis were observed in an examination performed in
October 2007.
In January 2008, a thoracoabdominal CT revealed an
anterior mediastinal node and a small amount of pleural effusion,
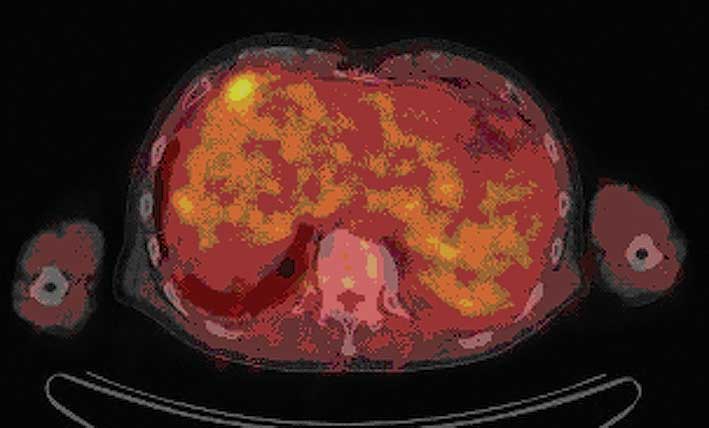
and the amount of ascites was noted to have increased. In May 2008,
a PET-CT examination was performed and an accumulation was detected
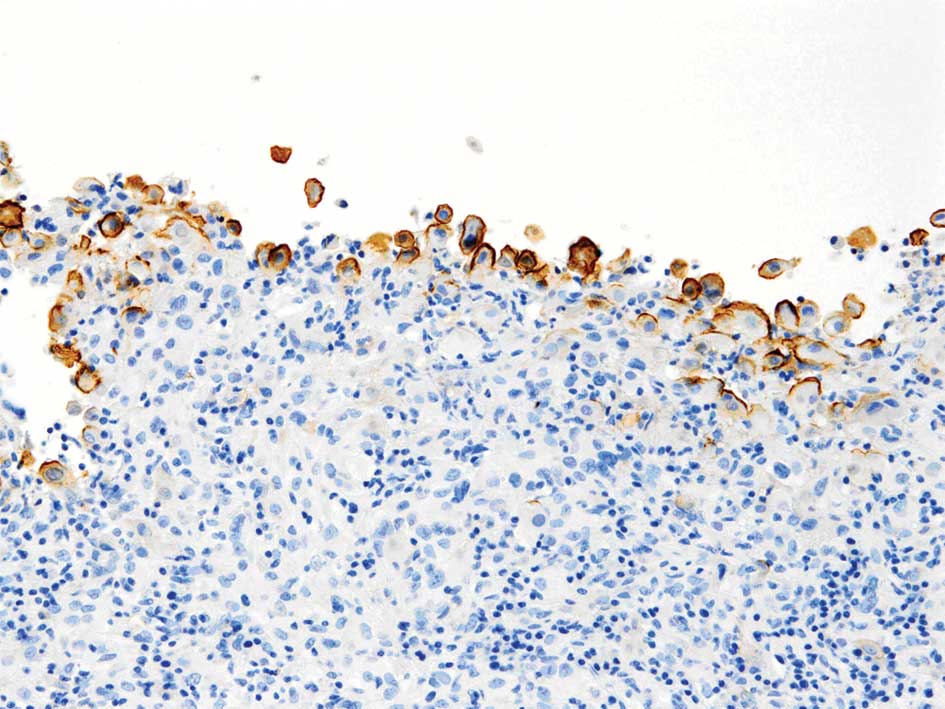
in the anterior mediastinal node and abdominal cavity (Fig. 1). A laparoscopic biopsy was
performed in June 2008 and numerous white nodes were detected in
the abdominal cavity. A pathological examination confirmed the
diagnosis of MM, epithelioid-type (Fig. 2).
During this time period, the patient’s blood
N-ERC/mesothelin levels increased from 8.62 ng/ml in June 2007 to
13.59 ng/ml in October 2007 and 31.49 ng/ml in April 2008.
Patient B: clinical history
The subject was a 68-year-old male. He had suffered
from glaucoma since the age of 42, gout since the age of 50 and
high blood pressure and hyperlipidemia since the age of 55 years.He
had an occupational history of employment as a quality control
supervisor in charge of electric machinery that was stored in
heat-insulating material (asbestos) in his 20s, in an electrical
construction company where spraying with asbestos was carried out
in his immediate environment in his 30s, and in a building
custodial service using asbestos for caulking projects around pumps
from the age of 40.
History of present illness
The subject underwent a physical examination each
year. In 2007, an abnormality was detected on a plain chest
roentgenogram. In November 2008, an abnormality was again perceived
on a plain chest roentgenogram. In December 2008, a pleural
effusion was detected at a local hospital. In February 2009,
thoracentesis was performed, and a cytological examination of the
pleural fluid revealed class V cytology.
The patient subsequently visited the clinic of
Juntendo University Hospital in the same month, at which time his
plasma N-ERC/mesothelin level was 15.6 ng/ml, which was in excess
of the cutoff value (3). In April
2009, a pleural biopsy was performed. Histopathological examination
confirmed a diagnosis of MM, epithelioid-type. The TNM class was
evaluated as pT1bN0M0 and the clinical stage as stage IB. In June,
the patient was admitted to the hospital. Surgical removal of the
pericardium and diaphragm and left extrapleural pneumonectomy were
performed immediately. On day 3 after the surgery, the thoracostomy
tube was removed. On day 11, as he was making satisfactory
progress, he was discharged from the hospital, at which time his
plasma N-ERC/mesothelin level was 1.63 ng/ml, lower than the cutoff
value. After discharge from the hospital, he visited the clinic
again in June, July, August and December 2009, and February 2010,
and no evidence of recurrence was detected. In December 2009, the
plasma N-ERC/mesothelin level was 2.64 ng/ml, which was within the
normal range.
Patient C: clinical history
The subject was a 68-year-old female. She had a
previous history of undergoing surgical removal of a chocolate cyst
in the right ovary. She had an occupational history of employment
as a teacher in a school building with asbestos insulation.
History of present illness
The patient visited a local hospital with the chief
complaint of dyspnea on exertion and was diagnosed as having a
bloody pleural effusion on the left side.
A tumor mass on the chest wall was detected by chest
CT. A lung biopsy was performed. Cytological examination of the
pleural fluid revealed class III cytology, and biochemical
examination revealed a markedly elevated level of hyaluronic acid
(646,000 ng/ml). Cytological examination of the lacteal gland
discharge revealed class V cytology. In April 2009, the patient
visited the clinic of Juntendo University Hospital. A pleural
biopsy was performed. Histopathological examination confirmed the
diagnosis of malignant pleural mesothelioma. The TNM classification
was evaluated as pT4N2M0 and the clinical stage as IV. She was
discharged from the hospital, but was re-admitted in May of the
same year because of re-accumulation of the pleural fluid, which
was treated by drainage. A pleurosclerosis was performed using
OK-432 and 5KE. She was discharged from the hospital, but was again
admitted in June 2009, at which time her plasma N-ERC/mesothelin
level reached 117.50 ng/ml, markedly higher than the cutoff value.
A left extrapleural pneumonectomy was performed. On day 3 after the
surgery, the thoracostomy tube was removed. On day 9, as she was
making satisfactory progress, she was discharged from the hospital.
After the surgery, her plasma N-ERC/mesothelin levels were 14.46
ng/ml in December 2009, 7.13 ng/ml in February 2010 and 8.36 ng/ml
in April 2010. She showed no evidence of recurrence until February
2010. In July 2010, she was found to have a tumor recurrence on the
chest wall and a metastasis in the contralateral lung, and was
re-admitted to the hospital for chemotherapy, at which time her
plasma N-ERC/mesothelin level had again increased to 36.03
ng/ml.
Relationship between the plasma level
of N-ERC/mesothelin and the pathogenesis of MM
Patient A was detected during a large-scale
screening of approximately 30,000 subjects affiliated with the
Tokyo Doken National Health Insurance Association who had worked at
construction sites, and who had undergone a physical examination
and submitted blood samples for laboratory analysis. The
N-ERC/mesothelin level in each blood sample was measured using our
novel ELISA method.
Approximately 80 subjects were identified as
belonging to a high-risk group based on the previously reported
cutoff value for N-ERC/mesothelin (3). Of these subjects, 30 individuals
underwent secondary screening, and one man (patient A) was
diagnosed as having MM based on the results of a PET study and
histopathology. It is noteworthy that, in this case, although no
abnormal findings were observed on a thoracoabdominal CT performed
in October 2007, the plasma N-ERC/mesothelin level was already
elevated at this time. Thus, this is the first report of the
pre-clinical diagnosis of MM based on a blood test.
The two additional cases reported here were not
detected to have MM in the large-scale screening study, but they
represent appropriate examples to demonstrate the effectiveness of
N-ERC/mesothelin as a blood marker for the diagnosis of MM. Patient
B was a 68-year-old male who was detected to have an abnormality on
a plain chest X-ray during a medical check-up. A histopathological
examination confirmed the diagnosis of MM, epithelioid-type.
Surgical removal of the pericardium and diaphragm and a left
extrapleural pneumonectomy were performed. Before the surgery, the
plasma N-ERC/mesothelin level was 15.6 ng/ml; however, following
the surgery it decreased to 1.63 ng/ml. There has been no evidence
of recurrence since.
Patient C was a 68-year-old female working as a
teacher in a school building with asbestos insulation. She had a
previous history of surgical removal of a chocolate cyst in the
right ovary. She visited our hospital because of dyspnea on
exertion, and was diagnosed as having a bloody pleural effusion on
the left side. Histopathologic examination of a pleural biopsy
confirmed the diagnosis of malignant pleural mesothelioma. A left
extrapleural pneumonectomy was performed. Before the surgery, the
plasma N-ERC/mesothelin level was 117.50 ng/ml, while after the
surgery it decreased to 7.13 ng/ml. However, 11 months later, the
patient developed a tumor recurrence on the chest wall and a
metastasis in the contralateral lung, at which time her plasma
N-ERC/mesothelin level had again increased to 36.03 ng/ml.
As described above, the plasma level of
N-ERC/mesothelin may be a useful blood marker for the early
diagnosis of MM, and may be particularly effective for monitoring
patients for relapse after surgery.
Early diagnosis of MM may become possible by
measurement of the blood N-ERC/mesothelin level as a routine
laboratory test in high-risk populations with a history of exposure
to asbestos.
Discussion
This study showed the effectiveness of
N-ERC/mesothelin as a blood marker for MM. At present, two lines of
clinical studies for mesothelin-bearing tumors are ongoing: a phase
I trial of the anti-mesothelin immunotoxin SS1P in patients with
mesothelioma, ovarian and pancreatic cancer (4), and a phase I clinical trial of
MORAb-009, which is a chimeric antibody targeting tumor-associated
mesothelin (5,6). Additionally, Inami et al
reported the antitumor activity of the anti-C-ERC/mesothelin
monoclonal antibody in vivo (7), and Yoshida et al reported on
the use of PET imaging of 64Cu-labeled Fab for detecting
ERC/mesothelin in a mesothelioma mouse model (8).
It would be most useful to combine immunotherapy
using an anti-mesothelin antibody directed against
mesothelinbearing tumors and a blood test for ERC/mesothelin.
The screening protocol reported herein is very
promising for the early diagnosis of MM in subjects with a history
of exposure to asbestos. In addition, measurement of the plasma
level of N-ERC/mesothelin may also be useful in the follow-up of
patients after surgery for MM.
Acknowledgements
This study was supported by a
Grant-in-Aid for Cancer Research and Grants-in Aid for Scientific
Research from the Ministry of Education, Culture, Sports, Science,
and Technology of Japan, and the Ministry of Health, Labor, and
Welfare of Japan.
References
|
1.
|
Robinson BWS, Creaney J, Lake R, Nowak A,
Musk AW and De Klerk N: Mesothelin-family proteins and diagnosis of
mesothelioma. Lancet. 362:1612–1616. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Shiomi K, Miyamoto H, Segawa T, Hagiwara
Y, Ota A and Hino O: Novel ELISA system for detection of
NERC/mesothelin in the sera of mesothelioma patients. Cancer Sci.
97:928–932. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Shiomi K, Hagiwara Y, Sonoue K, et al:
Sensitive and specific new enzyme-linked immunosorbent assay for
N-ERC/mesothelin increases its potential as a useful serum tumor
marker for mesothelioma. Clin Cancer Res. 14:1431–1437. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Hassan R, Bullock S, Premkumar A, Kreitman
RJ, Kindler H, Willingham M and Pastan I: Phase I study of SS1P, a
recombinant anti-mesothelin immunotoxin for targeted therapy of
mesothelin-expressing mesotheliomas, ovarian and pancreatic cancer.
J Clin Oncol. 25:35532007.PubMed/NCBI
|
|
5.
|
Hassan R, Ebel W, Routhier E, et al:
Preclinical evaluation of MORAb-009, a chimeric antibody targeting
tumor-associated mesothelin. Cancer Immun. 7:20–29. 2007.PubMed/NCBI
|
|
6.
|
Hassan R and Ho M: Mesothelin-targeted
cancer immunotherapy. Eur J Cancer. 44:46–53. 2008. View Article : Google Scholar
|
|
7.
|
Inami K, Abe M, Takeda K, Hagiwara Y,
Maeda M, Segawa T, Suyama M, Watanabe S and Hino O: Antitumor
activity of anti-C-ERC/mesothelin monoclonal antibody in vivo.
Cancer Sci. 101:969–974. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Yoshida C, Sogawa C, Tsuji A, Sudo H,
Sugyo A, Uehara T, Hino O, Yoshii Y, Fujibayashi Y, Fukumura T,
Koizumi M, Arano Y and Saga T: Development of positron emission
tomography imaging by 64Cu-labeled Fab for detecting ERC/mesothelin
in mesothelioma mouse model. Nucl Med Commun. 31:380–388.
2010.PubMed/NCBI
|