Introduction
Acute kidney injury (AKI), formerly known as acute
renal failure, is a common clinical problem which occurs in
critically ill patients (1–3).
Sepsis is now recognized as the most important contributing factor
to AKI in this population (3). For
example, acute renal failure occurs in approximately 19% of
patients with moderate sepsis, in 23% with severe sepsis and in 51%
with septic shock when blood cultures are positive (1,2). In
the US, an estimated 700,000 cases of sepsis occur each year,
resulting in more than 210,000 deaths (4). The combination of acute renal failure
and sepsis is associated with a 70% mortality, as compared to a 45%
mortality among patients with acute renal failure alone. Thus, the
combination of sepsis and acute renal failure constitutes a
particularly serious medical problem in the US (5).
In clinical practice, a reliable marker for the
extent of AKI would be a valuable asset for the management of
patients with septic AKI in the critical care setting. In adults,
research has focused on the use of biochemical markers to detect
and define the extent of AKI and to predict adverse outcome after
AKI. These research findings have improved our understanding of the
values of urinary markers for the early detection of AKI before
there is a noticeable increase in serum creatinine. Regrettably,
only a few clinical studies have focused on the prognostic utility
of kidney injury markers in patients with established AKI.
Among the potential biochemical markers, certain
studies have explored urine neutrophil gelatinase-associated
lipocalin (uNGAL) and the urine kidney injury molecule-1 (uKIM-1)
as diagnostic and prognostic indices of AKI. Human NGAL was
originally identified as a 25-kDa protein covalently bound to
gelatinase from neutrophils (5–7).
Although NGAL is expressed only at very low levels in several human
tissues, it is markedly induced in injured epithelial cells,
including the kidney (8). uKIM-1
is a more recently described type 1 cell membrane glycoprotein that
is expressed in humans and rodents when the injured renal proximal
tubule assumes a dedifferentiated phenotype (9). NGAL and KIM-1 are increased in urine
very early (2 h) after injury, followed by IL-18 at 12 h, and hence
may serve as early detection biomarkers, at least in well-defined
clinical settings. Both NGAL and KIM-1 performed well in predicting
delayed graft function after renal transplantation; a study of both
together may show significant synergy.
The aim of this study was to test the hypothesis
that uNGAL and uKIM-1 are associated with measures of disease
severity and with adverse clinical outcomes in patients with
established septic AKI of mixed cause and severity.
Patients and methods
Patient recruitment
Over the period from March 2008 to January 2009, we
conducted a prospective observational study in intensive care units
in Changsha, China. The study was approved by the institutional
ethics committee. Informed consent was obtained from all patients
or from their guardians prior to inclusion. We enrolled 92 septic
patients with AKI and an expected stay in intensive care units
(ICUs) of >24 h. Inclusion criteria were age ≥18 years, AKI and
sepsis. Exclusion criteria were prior kidney transplant, end-stage
kidney disease (K/DOQI stages), renal replacement therapy (RRT)
prior to ICU admission, or confirmed and/or suspected acute
glomerulonephritis, interstitial nephritis, renal vasculitis or
obstructive etiology for AKI. AKI was defined according to the
risk-injury-failure-loss-ESRD (RIFLE) criteria (10). Worsening and/or progressive AKI was
defined as transition from RIFLE class-risk to class-injury,
failure or RRT initiation during the 5 days following enrollment.
Sepsis was defined according to consensus guidelines (11). Shock was defined as a mean arterial
pressure (MAP) <60 mmHg and/or need for vasoactive support.
Preexisting co-morbid illnesses were defined by the Charlson index
(12).
Clinical assessment and follow-up
Patients were identified by daily surveillance of
the participating ICUs. Eligible patients underwent a medical
record review. Data were extracted on standardized data forms.
Clinical data included demographics, co-morbidities, mechanical
ventilation, RRT details and clinical outcomes. Physiologic and
laboratory data included weight, hemodynamics, vasoactive drugs,
illness severity scores and details of pre-morbid and enrollment
kidney function. With this information, the Acute Physiology and
Chronic Health Evaluation II (APACHE II) score was calculated for
all patients. All had indwelling urinary catheters. Patients had
urine and blood drawn at enrollment. At the end of the hospital
stay, the length of hospital stay and vital status were recorded.
Finally, 180 days after AKI we contacted each patient’s general
practitioner to obtain information on vital status and hospital
admissions. Our primary endpoint was 6-month mortality.
Laboratory methods
Urine samples for uNGAL testing were centrifuged at
1,500 rpm × 10 min, and the supernatant was stored at −70°C for
batched analysis. uNGAL was measured by a chemiluminescent
microparticle assay using the ARCHITECT platform (Abbott
Diagnostics Inc., Abbott Park, IL, USA) (13). uKIM-1 measurements were performed
using microsphere-based Luminex xMAP technology with polyclonal
antibodies raised against the human KIM-1 ectodomain. This
technique is an adaptation of the sandwich ELISA assay. For
measurements, 30-μl urine samples were analyzed in duplicate.
Urinary creatinine levels were determined by a colorimetric method
based on the Jaffe reaction (14).
The urinary NGAL and KIM-1 levels were normalized to the urinary
creatinine concentration and expressed as ng/mg creatinine, to
standardize and correct for changes in urine concentration. Four
investigators blinded to the patients’ clinical characteristics
performed all of the urinary biomarker measures.
Statistical analysis
Analysis was performed using SPSS version 13.0 (SPSS
Inc., Chicago, IL, USA). Continuous variables are expressed as the
means ± SD and categorical variables as frequency (%). Comparision
of parameters of the two groups (survivors and non-survivors) was
carried out using the Student’s t-test and the Fisher’s exact test.
uKIM-1 and uNGAL levels were adjusted for the APACHE II score since
the APACHE II score represents a composite illness-severity score
that takes into consideration several demographic, physiologic and
laboratory variables, and the presence of sepsis. The performance
characteristics of uNGAL levels and KIM-1 activity in predicting
the composite outcome were described using the area under a
receiver operator characteristic (ROC) curve and compared to the
performance of more traditional clinical severity indices of kidney
injury, including serum creatinine, urinary output and APACHE II
score. Survival probabilities were calculated by the Kaplan-Meier
method and comparisons were made using the log-rank test to
identify potential prognostic factor. Variables found to be
statistically significant at the P<0.05 level were entered into
a multivariate model using Cox regression analysis to identify the
most statistically significant model. All P values are two sided,
the level of significance is P<0.05 and confidence intervals
(CI) refer to 95% boundaries.
Results
The demographic and clinical characteristics of the
92 patients on inclusion are shown in Tables I and II. The cases of septic AKI were
classified into two groups (survivors and non-survivors) on the
basis of 180-day death. The gender, length of ICU stay and
admission for emergence between the two groups were not different.
The survivor group had a longer length of stay in the hospital.
However, a higher percentage of patients exercised oliguria, shock
and need for RRT in the non-survivor group. They also had a higher
need for mechanical ventilation (P<0.009), more failed organs
(P<0.000) and higher mean values of the APACHE II score than the
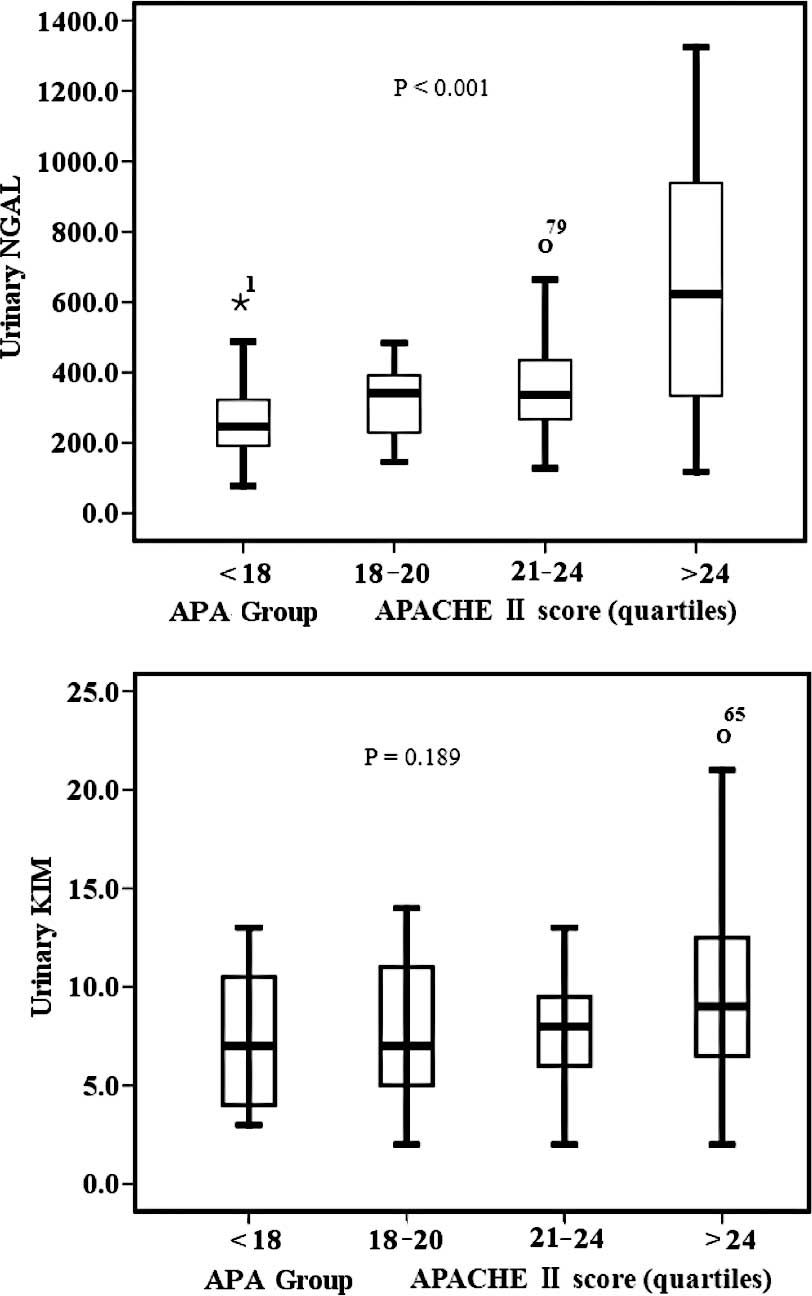
survival patient group (P<0.000). Urinary concentration of KIM-1
and NGAL increased significantly in the non-survivor group and
there was clear difference in the urinary concentrations between
those in the survivor group and the non-survivor group. uNGAL and
uKIM-1 concentrations increased in tandem with APACHE II score
quartiles (P<0.001; Figs. 1 and
2). The overall mortality among
patients studied was 39.1% (36 out of 92 patients). The primary
source of sepsis was intra-abdominal (45.7%) and pulmonary thoracic
(31.5%).
 | Table IMain source of sepsis in patients with
septic AKI. |
Table I
Main source of sepsis in patients with
septic AKI.
| Source of sepsis | No. (%) |
|---|
| Intra-abdominal | 42 (45.7) |
| Pulmonary
thoracic | 29 (31.5) |
| Skin/sofe
tissue/bone | 13 (14.1) |
| Urogenital | 8 (8.7) |
| Table IIBaseline demographic characteristics
of the patient population by vital status at 180 days. |
Table II
Baseline demographic characteristics
of the patient population by vital status at 180 days.
| Survival (n=56) | Non-survival
(n=36) | P-value |
|---|
| Age (years) | 55.0±7.7 | 59.5±8.3 | 0.090 |
| Males/females | 25/31 | 21/15 | 0.285 |
| Stage at diagnosis
(RIFLE) | | | |
| R, risk of renal
dysfunction | 16 | 3 | 0.000 |
| I, Injury to the
kidney | 28 | 14 | 0.000 |
| F, failure of
kidney function | 8 | 23 | 0.000 |
| Length of ICU
stay | 9.0±7.2 | 7.7±3.8 | 0.323 |
| Length of hospital
stay | 36.3±15.6 | 18.4±6.7 | 0.000 |
| Emergence | 18 (32.1%) | 17 (47.2%) | 0.188 |
| Shock | 28 (50.0%) | 29 (80.6%) | 0.004 |
| Mechanical
ventilation | 18 (32.1%) | 23 (63.9%) | 0.005 |
| APACHE II
score | 18.5±4.1 | 23.9±4.9 | 0.000 |
| Oliguria | 24 (42.9%) | 23 (63.9%) | 0.057 |
| RRT | 2 (3.6%) | 7 (19.4%) | 0.026 |
| Failure of organs
≥2 | 22 (39.3%) | 24 (66.7%) | 0.018 |
| Serum creatinine
(mmol/l) | 218.7±66.5 | 258.3±77.1 | 0.010 |
| CrCL | 30.2±10.2 | 24.3±9.2 | 0.007 |
| KIM-1 (ng/mg) | 7.9±4.1 | 8.9±4.9 | 0.288 |
| NGAL (ng/mg) | 308.9±155.2 | 539.0±287.6 | 0.000 |
To test whether uKIM and uNGAL levels predicts
180-day mortality, we initially performed univariate Cox
proportional hazards analyses incorporating multiple demographic,
clinical and laboratory variables (Table III). All variables found to be
statistically significant at a 5% level in the univariate analysis
(APACHE II score, oliguria, failure of organs ≥2, RRT, Cr, uKIM,
uNGAL, CrCL and Shock) were subjected to multivariate Cox
regression analysis. As a result, the APACHE II score (P= 0.014)
and uNGAL (P= 0.015) were identified as independent predictors of
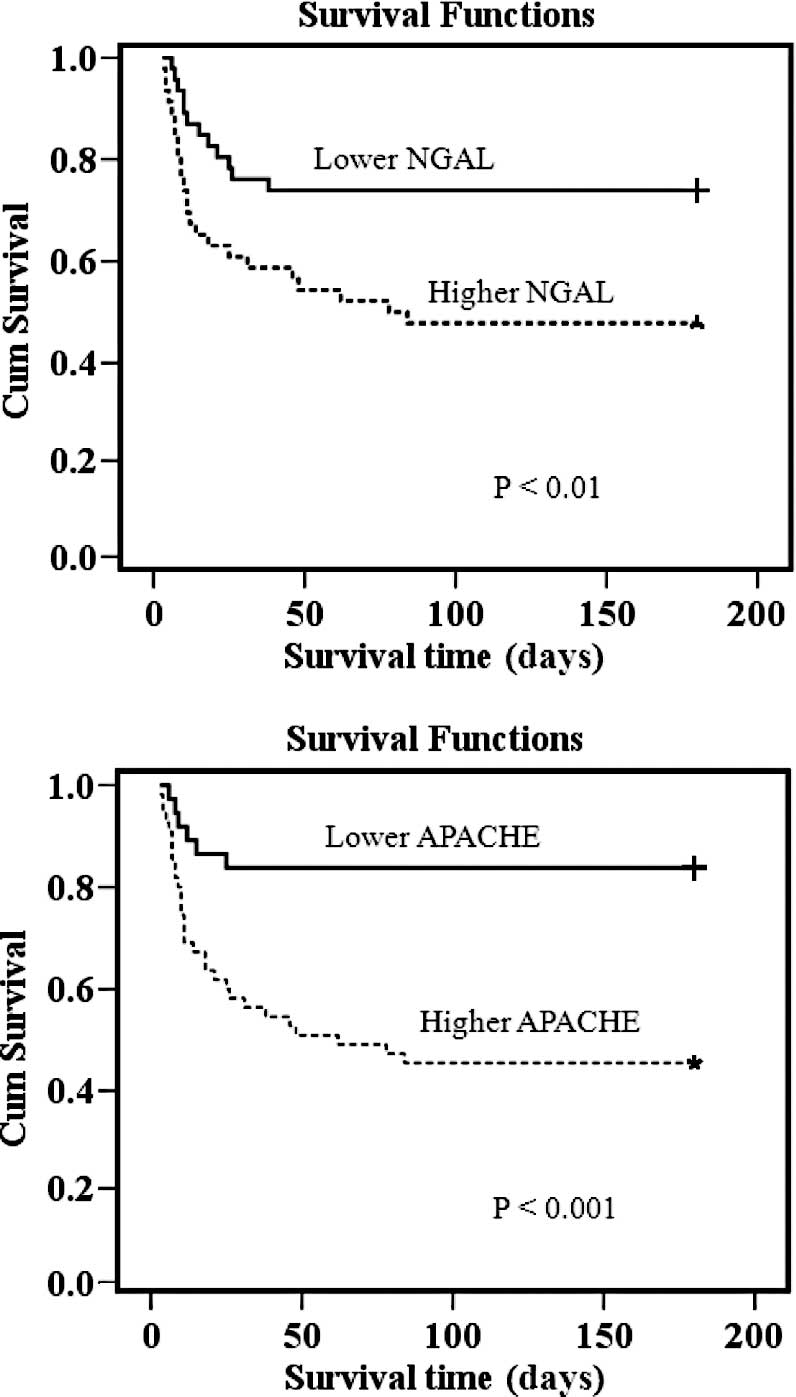
180-day mortality. When visualized by Kaplan-Meier curves, lower
event-free survival was shown in patients with higher uNGAL
concentrations compared to those with lower uNGAL concentrations
(Fig. 3). A similar phenomenon was
observed in the APACHE II score (Fig.
4). On the other hand, there was no statistical difference in
event-free survival between patients with and without higher serum
creatinine, creatinine clearance and uKIM-1 (data not shown).
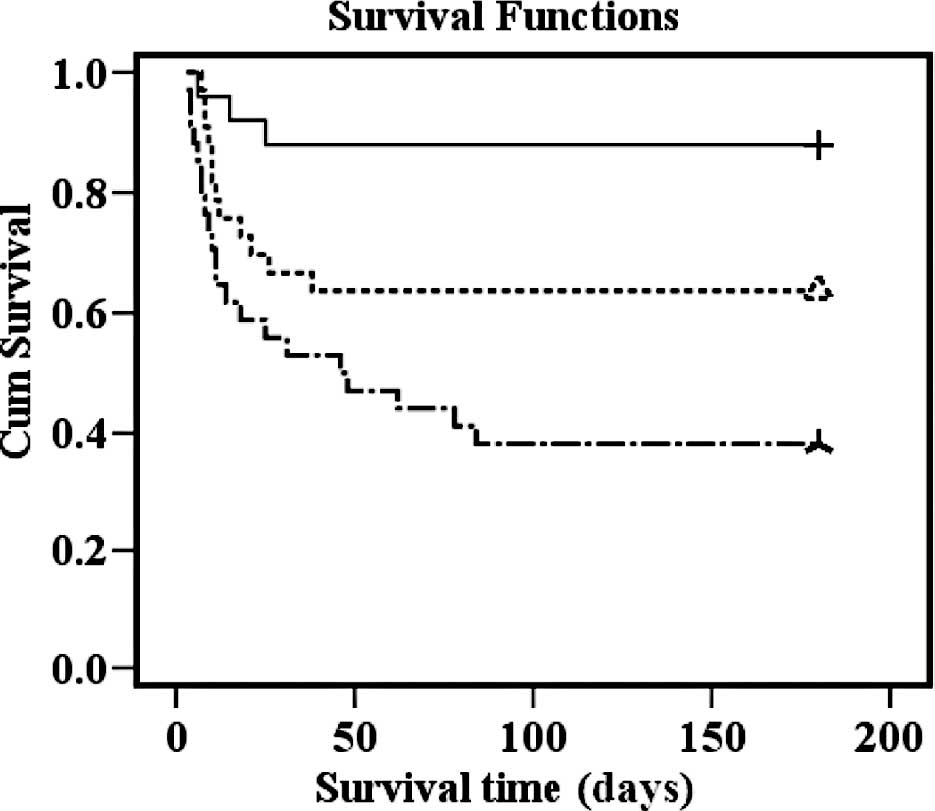
Moreover, after combining the uNGAL and APACHE II score, three
separate risk groups yielded low, medium and high 180-day mortality
(Fig. 4). Compared to the first
group, the risk of death increased significantly with each
group.
| Table IIIUnivariate and multivariable Cox
regression analysis for the 180-day mortality rate. |
Table III
Univariate and multivariable Cox
regression analysis for the 180-day mortality rate.
| Variables | Univariate analysis
| Multivariate
analysis
|
|---|
| HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| APACHE II | 1.181
(1.112–1.254) | 0.000 | 1.088
(1.008–1.174) | 0.031 |
| Age (group) | 1.755
(1.185–2.600) | 0.005 | | |
| Gender | 1.570
(0.809–3.047) | 0.183 | | |
| Oliguria | 2.030
(1.027–4.011) | 0.042 | | |
| Failure of organs
≥2 | 2.308
(1.154–4.618) | 0.018 | | |
| Emergence | 1.584
(0.823–3.048) | 0.169 | | |
| RRT | 2.886
(1.253–6.644) | 0.013 | | |
| Cr | 1.005
(1.001–1.010) | 0.017 | | |
| KIM-1 | 1.039
(0.967–1.116) | 0.300 | | |
| NGAL | 1.003
(1.002–1.004) | 0.000 | 1.002
(1.001–1.004) | 0.006 |
| CrCL | 0.955
(0.922–0.989) | 0.011 | | |
| Shock | 3.112
(1.362–7.113) | 0.007 | | |
| MV | 2.573
(1.302–5.084) | 0.007 | | |
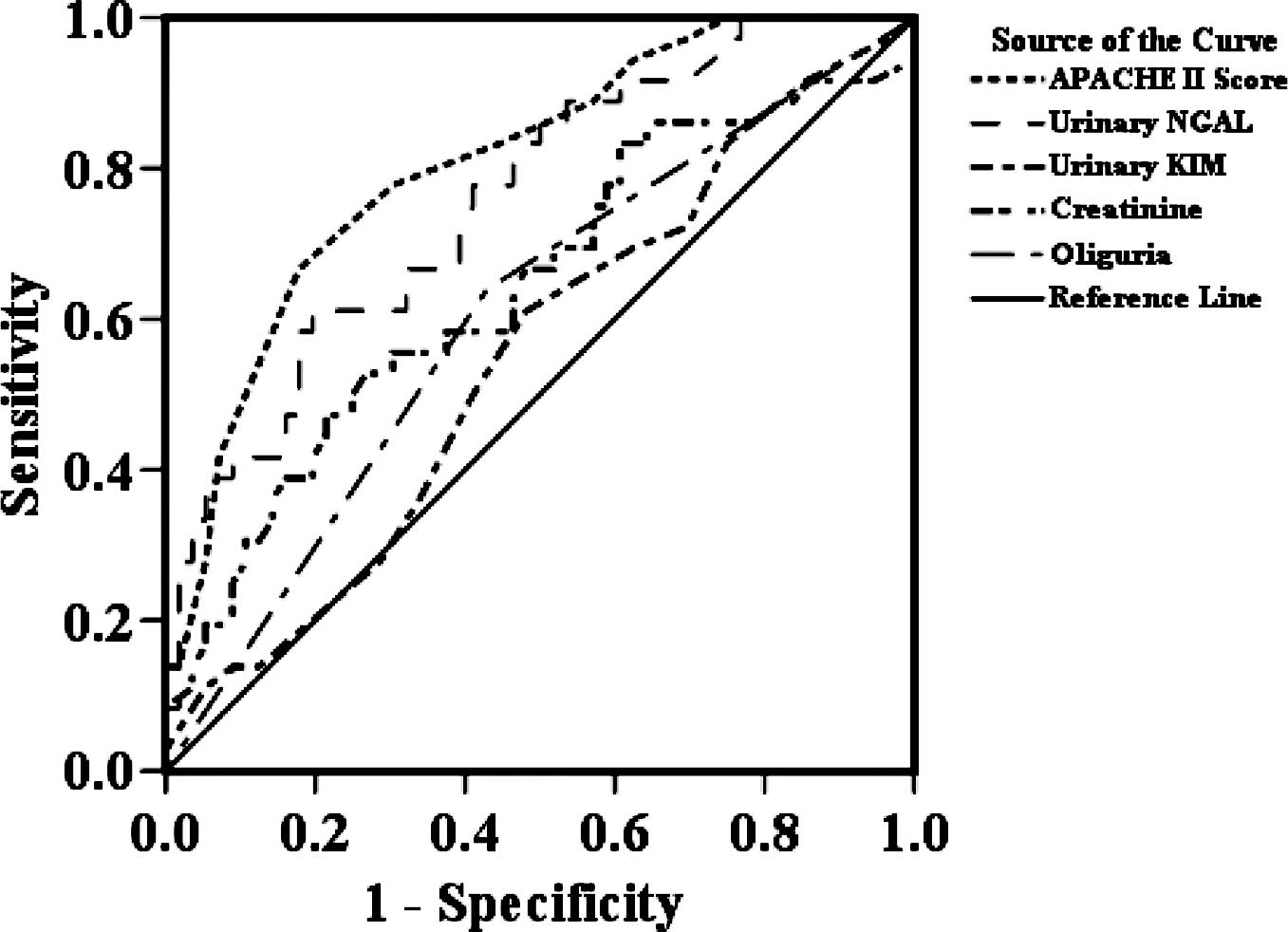
Table IV displays
the area under the ROC curve (AUC) of selected clinical and urinary
predictor variables for the 180-day death. The APACHE II score, a
composite score of 15 clinical variables, provided the best
discrimination compared to uNGAL for the 180-day death (0.785,
0.694–0.876). The uNGAL level performed better than serum
creatinine or oliguria, two traditional clinical parameters.
However, uKIM-1 showed slightly better discrimination compared to
serum creatinine.
| Table IVAUC of several variables for the
prediction of the outcome of 180-day mortality. |
Table IV
AUC of several variables for the
prediction of the outcome of 180-day mortality.
| Exp (B) 95% CI
|
|---|
| Parameter | AUC | P-value | Lower bound | Upper bound |
|---|
| APACHE II
score | 0.808 | 0.000 | 0.718 | 0.897 |
| NGAL | 0.759 | 0.000 | 0.660 | 0.858 |
| KIM-1 | 0.550 | 0.421 | 0.430 | 0.670 |
| Cr | 0.642 | 0.022 | 0.522 | 0.761 |
| Oliguria | 0.605 | 0.090 | 0.487 | 0.724 |
Discussion
Sepsis is an serious problem in ICU patients, not
only because of its high incidence, but also because of the high
mortality associated with this condition. It is a well-known fact
that sepsis is an important risk factor for the development of AKI,
and mortality in this specific subgroup of AKI patients is
considerably higher than in others (15–18).
Such a high incidence and marked disparity in outcome implies a
need for increasing our understanding of the pathophysiology,
diagnosis and treatment options for septic AKI (19). Animal data indicate that septic AKI
may have distinct pathophysiologic features that differ from
ischemia/toxin-induced kidney injury (20). For example, in a mammalian model of
E. coli-induced hyperdynamic sepsis, renal blood flow was
increased nearly 300% from baseline at 48 h (21). This renal hyperemia was evident
despite severe reductions in kidney function. This phenomenon has
been similarly described in septic humans (22–24).
These observations may have implications for the
critically ill septic patient. Firstly, unique patterns of urine
biochemistry and/or biomarkers may exist in septic AKI that can be
detected early, guide therapy, aid in clinical decision-making
(early renal support) and/or provide prognostic information (renal
recovery) (25). Secondly,
emerging literature has challenged the conventional paradigm
concerning the value of urine biochemistry and derived indices in
septic AKI (26–28). This widely accepted paradigm for
classifying AKI (i.e., pre-renal azotemia or acute tubular
necrosis) may be flawed in septic AKI, and novel methods for
evaluation are required (25,28).
To the best of our knowledge, this is the first
study to investigate prognostic factors among patients with septic
AKI in China, especially using kidney injury makers, such as uNGAL
and uKIM-1. We found that the survival group patients with septic
AKI, when compared to the non-survival septic AKI group, had
considerable differences across numerous clinical, physiologic and
laboratory parameters. Non-survival patients were generally older,
had a shorter hospital stay, higher illness severity and organ
dysfunction, and were more likely to have undergone mechnical
ventilation therapy. These differences have likewise been described
in prior studies (29–31). We also found that the uNGAL level
increased in tandem with APACHE II score quartiles and was a strong
predictor of mortality compared to creatinine or uKIM-1. Mortality
increased significantly with every tertile of the compilation of
uNGAL and APACHE II score. Consequently, uNGAL enables
stratification of patients with septic AKI according to risk of
death, and may help in directing intensified treatment efforts to
high-risk groups.
NGAL is a 25-kDa protein that is expressed at very
low concentrations in several human tissues, including kidney,
lungs and gastrointestinal tract (6,32).
It is highly up-regulated in injured epithelial cells. The
detection of NGAL has been described in several studies as an early
sensitive biomarker of AKI that precedes the lag-time effect needed
to detect abnormalities in traditional measures of kidney function
(9,14,33–39).
Recent studies have demonstrated the utility of early NGAL
measurements for predicting clinical outcomes of AKI. In cardiac
surgery, the 2-h uNGAL levels measured by ARCHITECT®
analyzer highly correlated with duration and severity of AKI,
length of hospital stay, dialysis requirement and death (40). In a multicenter study of children
with diarrhea-associated hemolytic uremic syndrome, uNGAL obtained
early during the hospitalization predicted the severity of AKI and
dialysis requirement with high sensitivity (34). Early uNGAL levels were also
predictive of duration of AKI (AUC 0.79) in a heterogeneous cohort
of critically ill subjects (41).
Emerging literature suggests that uNGAL is also a marker of chronic
kidney disease (CKD) and its severity (42). In subjects with CKD, due to
glomerulonephritis, uNGAL levels were found to be elevated and
significantly correlated with serum creatinine, GFR and proteinuria
(43). In patients with autosomal
dominant polycystic kidney disease, uNGAL measurements correlated
with residual GFR and severity of cystic disease (44,45),
raising the possibility of NGAL representing a non-invasive
screening tool for the detection of tubulo-interstitial
disease.
Reliable identification of renal dysfunction is a
key issue in identifying patients at risk of death. In clinical
practice, however, assessment of renal function is dependent on
readily available methods. The relationship between creatinine and
GFR is non-linear and creatinine is an insensitive measure for
detecting small decreases in GFR (46). Creatinine concentrations are also
affected by factors, such as age, gender, muscle mass and diet. As
a sensitive marker of renal function, uNGAL probably overcomes many
of the shortcomings of the more commonly used measures of renal
function in the setting of AKI. Consequently, we suggest that the
preferred marker of renal function with the strongest prognostic
value for patients with AKI is uNGAL.
We acknowledge that increased mortality with higher
levels of NGAL largely reflects the association with renal
dysfunction. Whether the multivariable prognostic value of NGAL is
solely due to its superior ability to estimate the true renal
function and detect real changes in GFR is not clear. We consider
NGAL a possible marker of impaired renal perfusion that reflects
early end organ failure in patients with AKI. However, we cannot
exclude that NGAL affects prognosis by mechanisms unrelated to
renal function. Further studies are required to increase our
knowledge about the multivariable effect on mortality in septic AKI
and possible underlying mechanisms.
We demonstrated the ability of NGAL to distinguish
patients with septic AKI having low, median and high risk of death
in combination with the APACHE II score. The difference in
mortality between each group is marked and statistically highly
significant. This finding provides clinicians with a simple tool in
risk stratification, which is essential in the management of septic
AKI.
There are limitations to our study. First, this was
a prospective study with a small number of patients and relatively
short follow-up, which may be associated with the observed lack of
a significant difference between groups. Further studies with a
larger number of patients and longer follow-up are required to
evaluate the usefulness of the uNGAL level for predicting death
during follow-up after AKI. Second, we did not include a septic
non-AKI control group for comparison. We also did not study the
cause of death in our patients and therefore did not obtain data on
the mechanisms linking renal function impairment and outcomes.
In conclusion, our study provides evidence that
uNGAL is a sensitive marker of renal insufficiency in septic AKI
patients, correlates with APACHE II score and has an independent
prognostic significance for survival. Notably, its combination with
APACHE II score produces a prognostic model which separates
newly-diagnosed septic AKI patients into three risk groups: low-,
median- and high-risk groups. Therefore, its measurement provides
important information for septic AKI patients. According to our
data, routine assessment of uNGAL in septic AKI should be
recommended, while its combination with APACHE II score will be a
useful tool for the prognosis of septic AKI patients.
Acknowledgements
The authors gratefully acknowledge the
assistance of the medical and nursing staff of the ICU and of the
Nephrology Section of the Xiangya Hospital.
References
|
1
|
Riedemann NC, Guo RF and Ward PA: The
enigma of sepsis. J Clin Invest. 112:460–467. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rangel-Frausto MS, Pittet D, Costigan M,
et al: The natural history of the systemic inflammatory response
syndrome (SIRS): a prospective study. JAMA. 273:117–123. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Uchino S, Kellum JA, Bellomo R, et al:
Acute renal failure in critically ill patients: a multinational,
multicenter study. JAMA. 294:813–818. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Angus DC, Linde-Zwirble WT, Lidicker J, et
al: Epidemiology of severe sepsis in the United States: analysis of
incidence, outcome, and associated costs of care. Crit Care Med.
29:1303–1310. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Edelstein CL and Schrier RW:
Pathophysiology of ischemic acute renal failure. Schrier RW:
Diseases of the Kidney and Urinary Tract. 7th edition. 2.
Lippincott Williams & Wilkins; Philadelphia: pp. 1041–1069.
2001
|
|
6
|
Cowland JB and Borregaard N: Molecular
characterization and pattern of tissue expression of the gene for
neutrophil gelatinase-associated lipocalin from humans. Genomics.
45:17–23. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cowland JB, Sorensen OE, Schested M, et
al: Neutrophil gelatinase-associated lipocalin is up-regulated in
human epithelial cells by IL-1β but not by TNF-α. J Immunol.
171:6630–6639. 2003.
|
|
8
|
Mishra J, Mori K, Ma Q, et al:
Amelioration of ischemic acute renal injury by neutrophil
gelatinase-associated lipocalin. J Am Soc Nephrol. 15:3073–3082.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mishra J, Dent C, Tarabishi R, et al:
Neutrophil gelatinase-associated lipocalin (NGAL) as a biomarker
for acute renal injury after cardiac surgery. Lancet.
365:1231–1238. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Boldt J, Brenner T, Lehmann A, et al: Is
kidney function altered by the duration of cardiopulmonary bypass?
Ann Thorac Surg. 75:906–912. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bellomo R and Ronco C: Acute renal failure
– definition, outcome measures, animal models, fluid therapy and
information technology needs: the Second International Consensus
Conference of the Acute Dialysis Quality Initiative (ADQI) Group.
Crit Care. 8:R204–R212. 2004.
|
|
12
|
Levy MM, Fink MP, Marshall JC, et al: 2001
SCCM/ESICM/ ACCP/ATS/SIS international sepsis definitions
conference. Crit Care Med. 31:1250–1256. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Charlson ME, Pompei P, Ales KL, et al: A
new method of classifying prognostic comorbidity in longitudinal
studies: development and validation. J Chronic Dis. 40:373–383.
1987. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nickolas TL, O’Rourke MJ, Yang J, et al:
Sensitivity and specificity of a single emergency department
measurement of urinary neutrophil gelatinase-associated lipocalin
for diagnosing acute kidney injury. Ann Intern Med. 148:810–819.
2008. View Article : Google Scholar
|
|
15
|
Slot C: Plasma creatinine determination: a
new and specific Jaffe reaction method. Scand J Clin Lab Invest.
17:381–387. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Brivet F, Kleinknecht D, Loirat P, et al:
The French study group on acute renal failure: acute renal failure
in intensive care units – causes, outcome, and prognostic factors
on hospital mortality: a prospective, multicenter study. Crit Care
Med. 24:192–198. 1996.PubMed/NCBI
|
|
17
|
Liano F, Junco E, Pascual J, et al: The
spectrum of acute renal failure in the intensive care unit compared
to that seen in other settings. Kidney Int. 53(Suppl 66): 16–24.
1998.PubMed/NCBI
|
|
18
|
Neveu H, Kleinknecht D, Brivet F, et al:
Prognostic factors in acute renal failure due to sepsis. Results of
a prospective multicentre study. Nephrol Dial Transplant.
11:293–299. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cole L, Bellomo R, Silvester W, et al: A
prospective, multi-center study of the epidemiology, management,
and outcome of severe acute renal failure in a ‘closed’ ICU system.
Am J Respir Crit Care Med. 162:191–196. 2000.PubMed/NCBI
|
|
20
|
Wan L, Bagshaw SM, Langenberg C, et al:
Pathophysiology of septic acute kidney injury: what do we really
know? Crit Care Med. 36:S198–S203. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wan L, Bellomo R, di Giantomasso D, et al:
The pathogenesis of septic acute renal failure. Curr Opin Crit
Care. 9:496–502. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Langenberg C, Wan L, Egi M, et al: Renal
blood flow in experimental septic acute renal failure. Kidney Int.
69:1996–2002. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Brenner M, Schaer GL, Mallory DL, et al:
Detection of renal blood flow abnormalities in septic and
critically ill patients using a newly designed indwelling
thermodilution renal vein catheter. Chest. 98:170–179. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lucas CE, Rector FE, Werner M, et al:
Altered renal homeostasis with acute sepsis. Clinical significance
Arch Surg. 106:444–449. 1973.PubMed/NCBI
|
|
25
|
Rector F, Goyal S, Rosenberg IK, et al:
Renal hyperemia is associated with clinical sepsis. Surg Forum.
23:51–53. 1972.
|
|
26
|
Bellomo R, Bagshaw S, Langenberg C, et al:
A flawed paradigm in critically ill septic patients? Contrib
Nephrol. 156:1–9. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bagshaw SM, Langenberg C, Haase M, et al:
Urinary biomarkers in septic acute kidney injury. Intensive Care
Med. 33:1285–1296. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bagshaw SM, Langenberg C, Wan L, et al: A
systematic review of urinary findings in experimental septic acute
renal failure. Crit Care Med. 35:1592–1598. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Schrier RW: Urinary indices and microscopy
in sepsis-related acute renal failure. Am J Kidney Dis. 48:838–841.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bagshaw SM, George C and Bellomo R: Early
acute kidney injury and sepsis: a multicentre evaluation. Crit
Care. 12:R472008. View
Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bagshaw SM, Uchino S, Bellomo R, et al:
Septic acute kidney injury in critically ill patients: clinical
characteristics and outcomes. Clin J Am Soc Nephrol. 2:431–439.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Bagshaw SM, Lapinsky S, Dial S, et al:
Acute kidney injury in septic shock: clinical outcomes and impact
of duration of hypotension prior to initiation of antimicrobial
therapy. Intensive Care Med. 35:871–881. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kjeldsen L, Cowland JB and Borregaard N:
Human neutrophil gelatinase-associated lipocalin and homologous
proteins in rat and mouse. Biochim Biophys Acta. 1482:272–283.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Bennett M, Dent CL, Ma Q, et al: Urine
NGAL predicts severity of acute kidney injury after cardiac
surgery: a prospective study. Clin J Am Soc Nephrol. 3:665–673.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Dent CL, Ma Q, Dastrala S, et al: Plasma
neutrophil gelatinase-associated lipocalin predicts acute kidney
injury, morbidity and mortality after pediatric cardiac surgery: a
prospective uncontrolled cohort study. Crit Care. 11:R1272007.
View Article : Google Scholar
|
|
36
|
Haase-Fielitz A, Bellomo R, Devarajan P,
et al: Novel and conventional serum biomarkers predicting acute
kidney injury in adult cardiac surgery: a prospective cohort study.
Crit Care Med. 37:553–560. 2009. View Article : Google Scholar
|
|
37
|
Mishra J, Mori K, Ma Q, et al: Neutrophil
gelatinase-associated lipocalin: a novel early urinary biomarker
for cisplatin nephrotoxicity. Am J Nephrol. 24:307–315. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Wagener G, Jan M, Kim M, et al:
Association between increases in urinary neutrophil
gelatinase-associated lipocalin and acute renal dysfunction after
adult cardiac surgery. Anesthesiology. 105:485–491. 2006.
View Article : Google Scholar
|
|
39
|
Bachorzewska-Gajewska H, Malyszko J,
Sitniewska E, et al: Neutrophil-gelatinase-associated lipocalin and
renal function after percutaneous coronary interventions. Am J
Nephrol. 26:287–292. 2006. View Article : Google Scholar
|
|
40
|
Haase M, Haase-Fielitz A, Bellomo R, et
al: Sodium bicarbonate to prevent increases in serum creatinine
after cardiac surgery: a pilot double-blind, randomized controlled
trial. Crit Care Med. 37:39–47. 2009. View Article : Google Scholar
|
|
41
|
Trachtman H, Christen E, Cnaan A, et al:
Urinary neutrophil gelatinase-associated lipocalcin in D+HUS: a
novel marker of renal injury. Pediatr Nephrol. 21:989–994.
2006.PubMed/NCBI
|
|
42
|
Zappitelli M, Washburn KM, Arikan AA, et
al: Urine NGAL is an early marker of acute kidney injury in
critically ill children. Crit Care. 11:R842007. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Nickolas TL, Barasch J and Devarajan P:
Biomarkers in acute and chronic kidney disease. Curr Opin Nephrol
Hypertens. 17:127–132. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Bolignano D, Coppolino G, Campo S, et al:
Urinary neutrophil gelatinase-associated lipocalin (NGAL) is
associated with severity of renal disease in proteinuric patients.
Nephrol Dial Transplant. 23:414–416. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Bolignano D, Coppolino G, Campo S, et al:
Neutrophil gelatinase-associated lipocalin in patients with
autosomal-dominant polycystic kidney disease. Am J Nephrol.
27:373–378. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Stevens LA, Coresh J, Greene T, et al:
Assessing kidney function measured and estimated glomerular
filtrationrate. N Engl J Med. 354:2473–2483. 2006. View Article : Google Scholar : PubMed/NCBI
|