Introduction
Pancreatic cancer is a lethal disease due to
late-stage diagnosis and a lack of effective treatment strategies.
The prognosis of patients with pancreatic cancer is very poor, with
a median survival of only 3–5 months and 1-year survival of less
than 10% (1,2). As with the majority of solid tumors,
surgery is the best choice for treating pancreatic cancer; however,
up to 80% of pancreatic cancer patients are diagnosed at an
advanced stage, which makes surgery difficult and ineffective. To
date, curative resection of pancreatic cancer occurs in only 10–15%
of patients (3). Moreover,
chemotherapy is only palliative to improve quality of life and gain
a modest survival benefit, and is used when patients are not
suitable for surgery. Accumulating evidence suggests that
successful surgical resection is one of the most crucial factors in
the effective treatment of pancreatic cancer (4), while chemotherapy and radiotherapy
are most effective in the treatment of locally unresectable and
recurrent pancreatic cancer (5).
Therefore, novel strategies that aid in the early detection,
disease prevention, effective treatment and prognosis prediction of
this deadly disease are required.
Pancreatic cancer development is likely associated
with the silencing of tumor suppressor genes and the activation of
oncogenes, although the underlying molecular mechanisms remain to
be defined. The altered expression of these genes may not only
trigger the development of pancreatic cancer but also promote tumor
progression, leading to a poor prognosis. Indeed, there have been a
number of studies published that associate the development and
prognosis of pancreatic cancer with a variety of factors (6). For example, a recent Japanese study
calculated the Onodera's prognostic nutrition index (PNI), based on
serum albumin and three other constitutive indices, to be an
independent prognostic factor useful in the prediction of survival
of pancreatic cancer patients (7).
In addition, other studies have focused on utilizing the
characteristics of the tumor phenotype, such as the number of
metastatic lymph nodes (8), tumor
invasion or adhesion to peripancreatic blood vessels and positive
margins following pancreatoduodenectomy (9,10) as
prognostic factors for pancreatic cancer. However, to date, there
are no studies found to associate the clinicopathological
characteristics with pancreatic cancer prognosis. Furthermore,
there have been no reports of the selection of pancreatic cancer
treatment with varying prognoses. Therefore, this study
retrospectively evaluated the clinicopathological features,
treatment selection and laboratory test data for pancreatic cancer
to guide its future management and to predict its prognosis.
Materials and methods
Patient population
In this study, we retrospectively reviewed data from
pancreatic cancer patients from the Cancer Hospital Affiliated to
Fudan University, Minhang Branch, The First Affiliated Hospital of
Suzhou University and the Jinshan Hospital Affiliated to Fudan
University, between January 2003 and December 2009. A total of 415
patients were identified and cytohistologically diagnosed to have
pancreatic cancer; 302 of them received a follow-up to ensure
survival via a phone interview. The overall survival was defined as
the period from the cytohistological diagnosis to the date of
mortality or the most recent follow-up. The institutional review
boards at our institutions approved this study and all patients or
their legal guardians signed an informed consent form.
Clinical data
The data of clinicopathological characteristics were
retrieved from the patients' medical records and follow-up data
were also obtained via phone interview. Of these 302 pancreatic
cancer patients, 189 (63%) were male and 113 (37%) were female, and
the median age was 63 years with a range of 28–89 years. A total of
140 patients had a pathological diagnosis determined from surgical
specimens, 85 patients were diagnosed through tissue biopsy of
metastatic or primary lesions, 32 cases via tissue biopsy from
liver metastasis puncture, 18 patients via cytological examination
of pleural effusion or ascites and 27 patients failed to provide
definitive pathological diagnosis. Moreover, 251 patients had
pancreatic adenocarcinoma, 5 had other types of cancer and 46 did
not provide definitive cytological results to diagnose the type of
cancer. In total, 189 cancers were located at the head or neck of
the pancreas, 110 cases at the body and tail of the pancreas and 3
cases had spread to the entire pancreas. In addition, 8 cases were
diagnosed as Stage I, 34 cases as Stage II, 94 as Stage IV and 166
cases as Stage V, according to the 2002 guidelines of the American
Joint Committee on Cancer (AJCC). A total of 67 patients did not
receive any treatment or only supportive treatment following
diagnosis, 140 patients underwent surgical treatment (47 patients
underwent radical surgery, 74 underwent palliative surgery and 19
did not have definitive surgical modalities), 115 patients
underwent chemotherapy, 17 underwent biliary drainage, 57 underwent
arterial interventional chemotherapy, 3 underwent local
radiotherapy and 86 underwent comprehensive treatment.
Statistical analyses
Survival curves were constructed by the Kaplan-Meier
method. Cox survival univariate and multivariate analyses were
performed to identify potential prognostic factors based on the
determination of the most significant variables that may contribute
to survival. Two-sided P-values of <0.05 were considered to
indicate a statistically significant difference. The association
between different clinicopathological characteristics or their
significance to survival was analyzed using the Chi-square test.
All statistical analyses were performed using the SPSS statistical
software program package (SPSS version 13.0 for windows; SPSS Inc.,
Chicago, IL, USA).
Results
Identification of prognostic factors for
pancreatic cancer patients
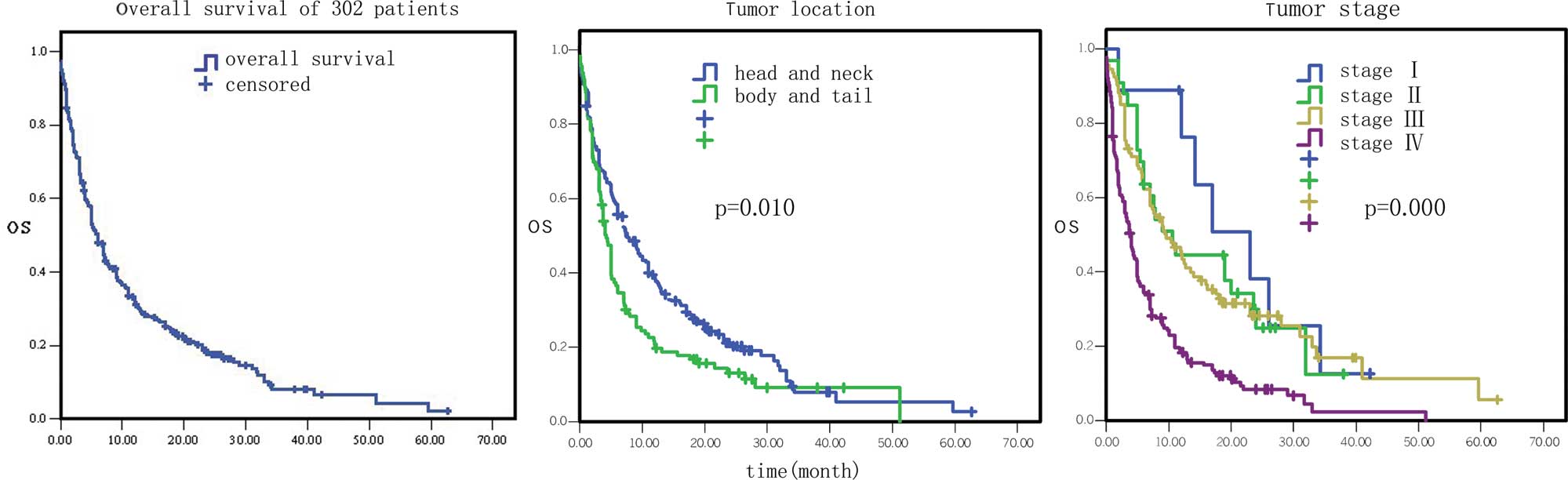
Among these 302 pancreatic cancer patients, 252 had
succumbed to the disease since their last follow-up and the
mortality rate was 83.4%. The median survival period for these 302
patients was 6.1 months (Fig. 1),
with 1-, 2- and 3-year survival rates of 30.1 (91/302), 10.6
(32/302) and 2.6% (8/302), respectively.
The overall survival data by Cox univariate
regression analysis are presented in Table I. The most influential factors
predicting the survival of these patients were the site of primary
cancer, tumor stage, treatment selection, the levels of serum
glutamic-pyruvic transaminase (GPT), serum albumin, serum lactate
dehydrogenase (LDH) and hemoglobin, and white blood cell (WBC)
counts (P<0.05). In particular, the mortality risk was increased
for pancreatic cancer masses located at the body and tail of the
pancreas compared to the tumors located at the head and neck of the
pancreas [hazard ratio (HR)=1.37, 95% CI 1.08–1.75, P=0.01;
Fig. 1). The mortality risk was
also increased in pancreatic cancer that was in advanced stages
compared to early stages (HR=1.64, 95% CI 1.37–1.96, P=0.000;
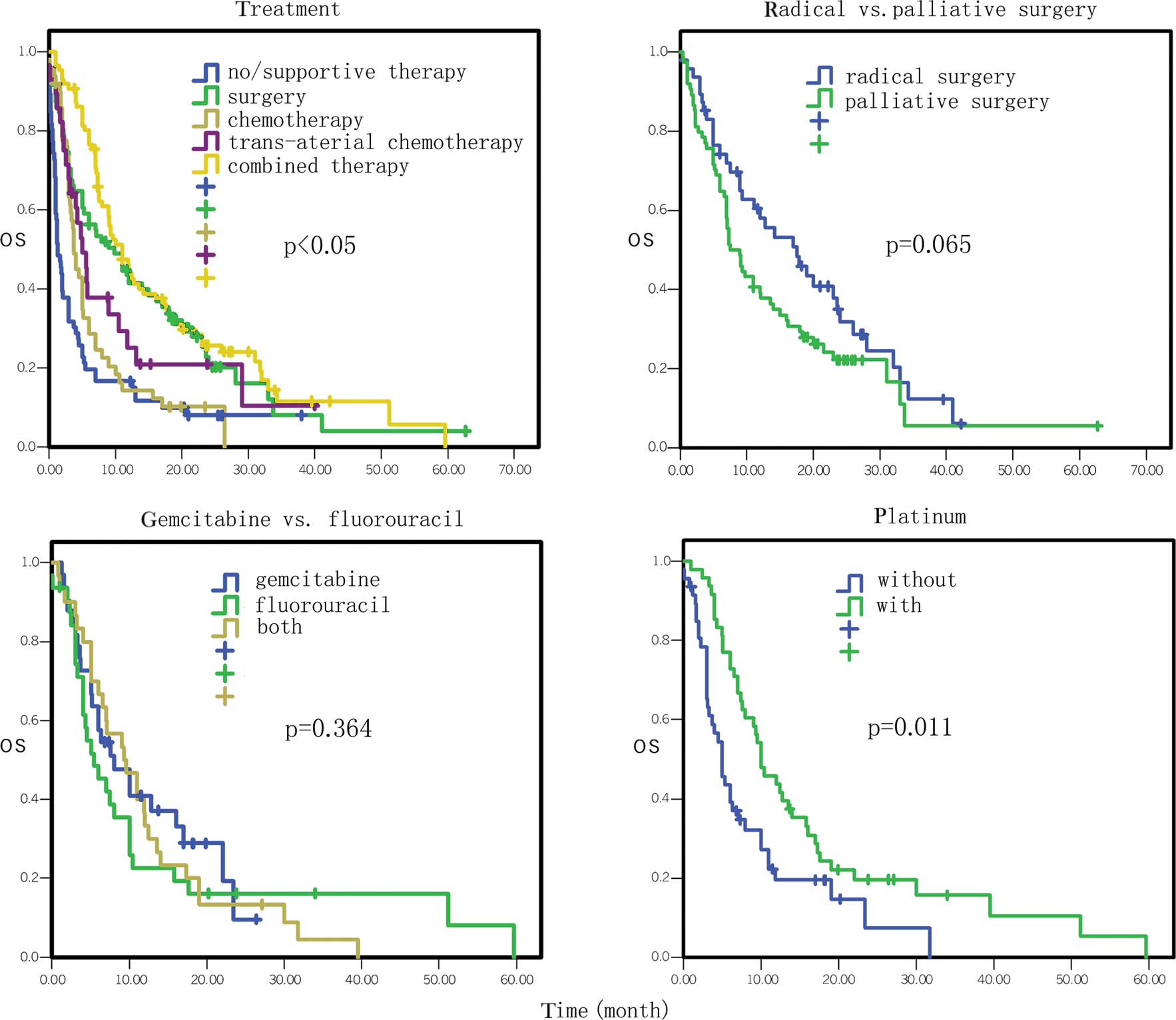
Fig. 1). However, the mortality
risk of patients who underwent surgery, chemotherapy, biliary
drainage, arterial interventional chemotherapy or comprehensive
treatment was reduced compared to the patients who did not receive
any treatment or who just received supportive treatment (HR=0.84,
95% CI 0.77–0.91, P=0.000; Fig.
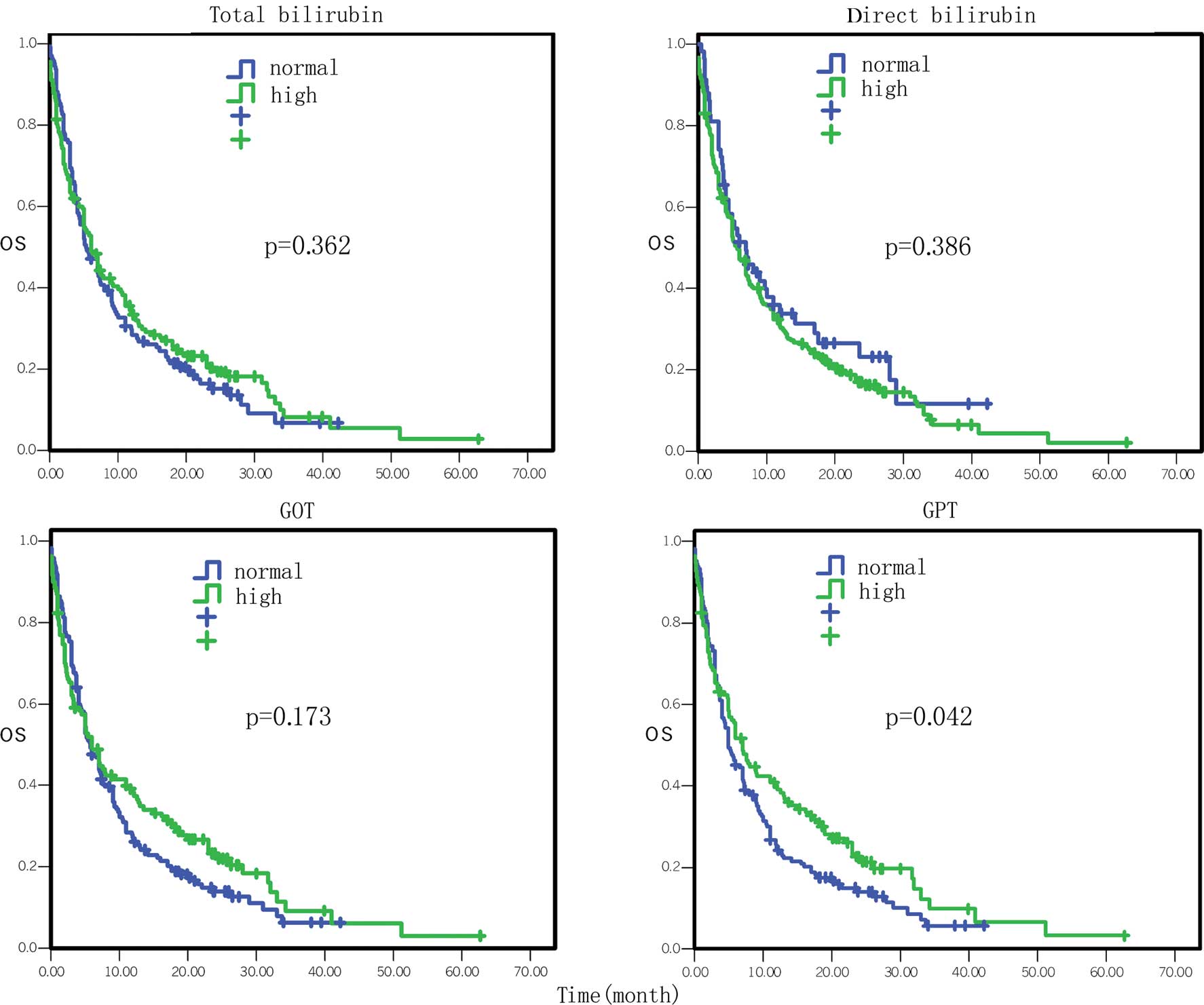
2). The mortality risk of patients with high GPT levels was
also reduced compared to the patients with normal levels (HR= 0.77,
95% CI 0.59–0.99, P= 0.042; Fig.
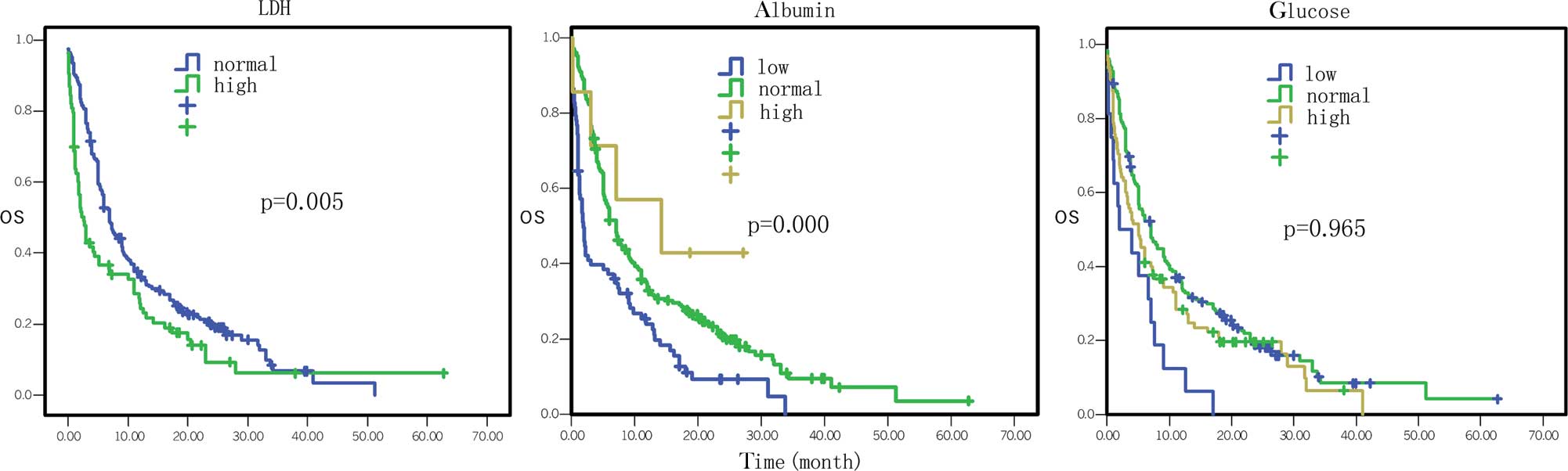
3). The mortality risk of the patients with high or normal
albumin levels was reduced compared to the patients with low levels
(HR=0.60, 95% CI 0.46–0.79, P=0.000; Fig. 4). In addition, the mortality risk
of the patients with high serum LDH levels was increased compared
to the patients with normal levels (HR=1.50, 95% CI 1.13–1.99,
P=0.005; Fig. 4). The mortality
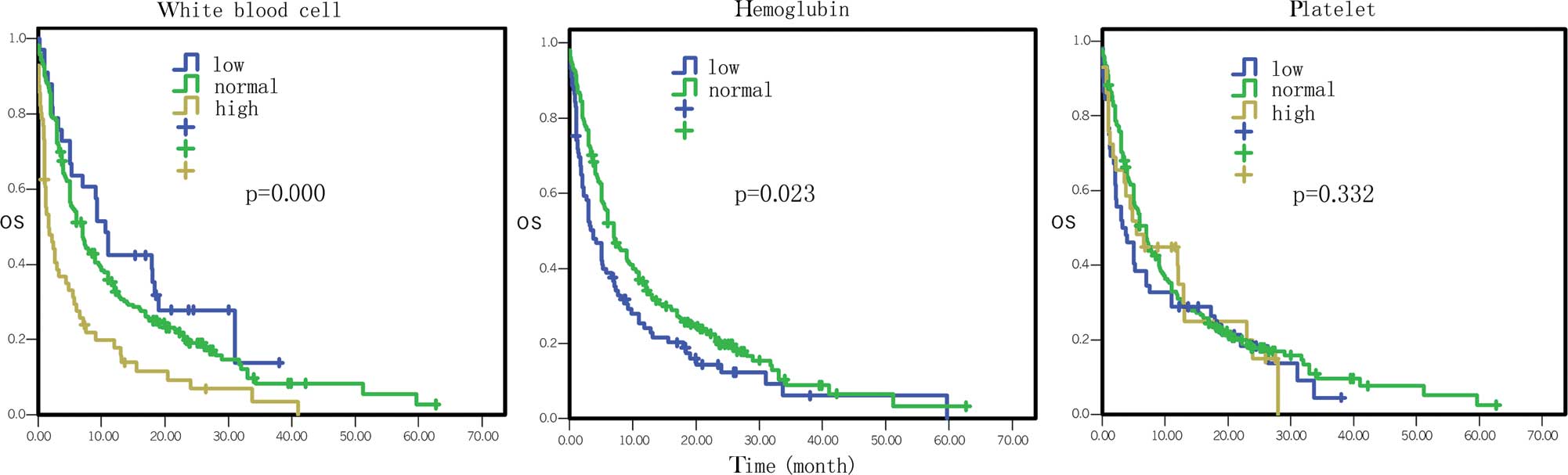
risk of patients with normal hemoglobin levels was reduced compared
to the patients with low levels (HR=0.73, 95% CI 0.55–0.96, P=
0.023; Fig. 5). The mortality risk
of patients with high WBC counts was increased compared to patients
with normal or low counts (HR=1.63, 95 %CI 1.27–2.09, P=0.000;
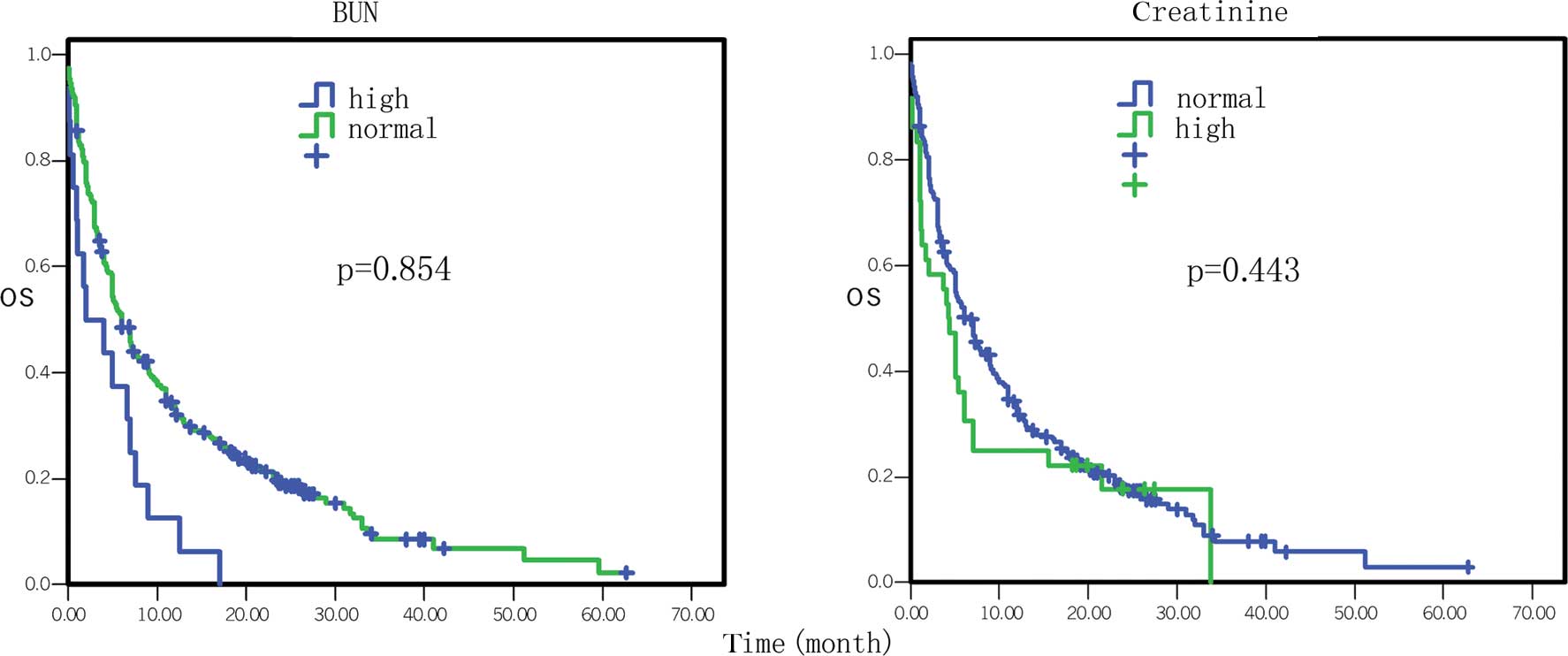
Fig. 5). Other factors, such as
gender, age, the levels of serum total bilirubin (TB), serum direct
bilirubin (DB), serum glutamic-oxalacetic transaminase (GOT)
(Fig. 3), blood urea nitrogen
(BUN), serum creatinine (Fig. 6),
blood glucose (Fig. 4) and
platelet counts, had no association with patient survival
(P>0.05).
 | Table I.Cox univariate regression analysis of
302 pancreatic cancer patients. |
Table I.
Cox univariate regression analysis of
302 pancreatic cancer patients.
| Parameter | No. | Median survival
(months; 95% CI) | P-value | Hazard ratio (95%
CI) |
|---|
| Gender | | | | |
| Male | 189 | 6.0 (5.0–7.4) | | |
| Female | 113 | 5.1 (3.7–8.0) | 0.342 | 1.13
(0.88–1.47) |
| Age (years) | | | | |
| ≤60 | 119 | 7.1 (5.3–10.4) | | |
| >60 | 183 | 5.0 (4.0–7.0) | 0.331 | 1.01
(0.99–1.02) |
| Site of primary
cancer | | | | |
| Head and
neck | 189 | 7.6 (6.0–10.6) | | |
| Body and
tail | 110 | 4.0 (3.3–5.0) | | |
| Whole
pancreas | 3 | 1.7 (1.1–3.0) | 0.010 | 1.37
(1.08–1.75) |
| Stage | | | | |
| I | 8 | 20.0 (12–34.3) | | |
| II | 34 | 10.6
(6.0–20.0) | | |
| III | 94 | 10.4
(7.0–14.0) | | |
| IV | 166 | 4.0 (3.0–5.0) | 0.000 | 1.64
(1.37–1.96) |
| Treatment
selection | | | | |
| Supportive
treatment | 67 | 1.3 (1.0–3.0) | | |
| Surgery, chemo-
or interventional therapy | 235 | 7.4 (6.0–9.3) | 0.000 | 0.84
(0.77–0.91) |
| Total
bilirubin | | | | |
| Normal | 144 | 5.3 (4.3–7.3) | | |
| High | 158 | 6.0 (5.0–9.0) | 0.362 | 0.89
(0.69–1.15) |
| Direct
bilirubin | | | | |
| Normal | 58 | 7.0 (4.0–11.0) | | |
| High | 244 | 5.7 (5.0–7.0) | 0.386 | 1.16
(0.83–1.61) |
| Glutamic-pyruvic
transaminase | | | | |
| Normal | 164 | 5.0 (4.0–7.0) | | |
| High | 136 | 7.0 (5.1–11.0) | 0.042 | 0.77
(0.59–0.99) |
| Glutamic-oxalacetic
transaminase | | | | |
| Normal | 170 | 5.7 (5.0–7.3) | | |
| High | 130 | 6.0 (4.2–11.0) | 0.173 | 0.84
(0.65–1.08) |
| Albumin | | | | |
| Low | 82 | 1.8 (1.23–5.0) | | |
| Normal | 210 | 7.0 (5.4–9.0) | | |
| High | 7 | 14.2
(3.0–27.1) | 0.000 | 0.60
(0.46–0.79) |
| Blood urea
nitrogen | | | | |
| Normal | 270 | 6.0 (5.0–7.1) | | |
| High | 29 | 1.7 (0.9–13.1) | 0.854 | 0.96
(0.61–1.50) |
| Serum
creatinine | | | | |
| Normal | 263 | 6.6 (5.0–8.0) | | |
| High | 36 | 4.3 (1.2–6.0) | 0.443 | 1.17
(0.78–1.75) |
| Lactate
dehydrogenase | | | | |
| Normal | 200 | 7.0 (5.8–9.0) | | |
| High | 83 | 4.3 (1.7–4.4) | 0.005 | 1.50
(1.13–1.99) |
| Blood glucose | | | | |
| Low | 16 | 3.0 (1.0–7.0) | | |
| Normal | 185 | 7.0 (5.0–9.3) | | |
| High | 96 | 5.0 (3.2–7.3) | 0.965 | 0.99
(0.77–1.28) |
| Hemoglobin | | | | |
| Low | 89 | 3.7 (2.2–5.7) | | |
| Normal | 212 | 7.0 (5.4–9.0) | 0.023 | 0.73
(0.55–0.96) |
| White blood
cells | | | | |
| Low | 33 | 10.6
(5.3–18.4) | | |
| Normal | 212 | 7.0 (5.1–8.0) | | |
| High | 56 | 1.7 (1.0–3.3) | 0.000 | 1.63
(1.27–2.09) |
| Platelets | | | | |
| Low | 52 | 3.5 (2.0–7.0) | | |
| Normal | 220 | 7.0 (5.1–8.0) | | |
| High | 29 | 5.4 (2.2–13.0) | 0.332 | 0.88
(0.68–1.14) |
| CEA | | | | |
| Normal | 130 | 5.0 (4.0–6.0) | | |
| High | 67 | 2.0 (1.3–3.0) | 0.030 | 1.43
(1.04–1.98) |
| CA19-9 | | | | |
| Normal | 52 | 5.0 (3.0–9.1) | | |
| High | 153 | 3.8 (2.5–5.0) | 0.060 | 1.41
(0.99–2.02) |
| CA125 | | | | |
| Normal | 22 | 10.1
(6.0–18.0) | | |
| High | 26 | 3.1 (1.4–5.0) | 0.018 | 2.06
(1.13–3.76) |
| CA15-3 | | | | |
| Normal | 47 | 2.4 (1.6–5.0) | | |
| High | 26 | 3.2 (1.2–7.8) | 0.564 | 0.86
(0.50–1.46) |
| CA72-4 | | | | |
| Normal | 40 | 1.4 (1.0–2.5) | | |
| High | 13 | 1.6 (0.8–2.0) | 0.429 | 1.33
(0.66–2.69) |
| CA50 | | | | |
| Normal | 31 | 1.7 (0.8–4.3) | | |
| High | 29 | 1.3 (0.8–1.6) | 0.258 | 1.40
(0.78–2.49) |
| CA242 | | | | |
| Normal | 15 | 1.2 (0.6–2.4) | | |
| High | 27 | 1.6 (0.8–3.7) | 0.312 | 0.70
(0.35–1.40) |
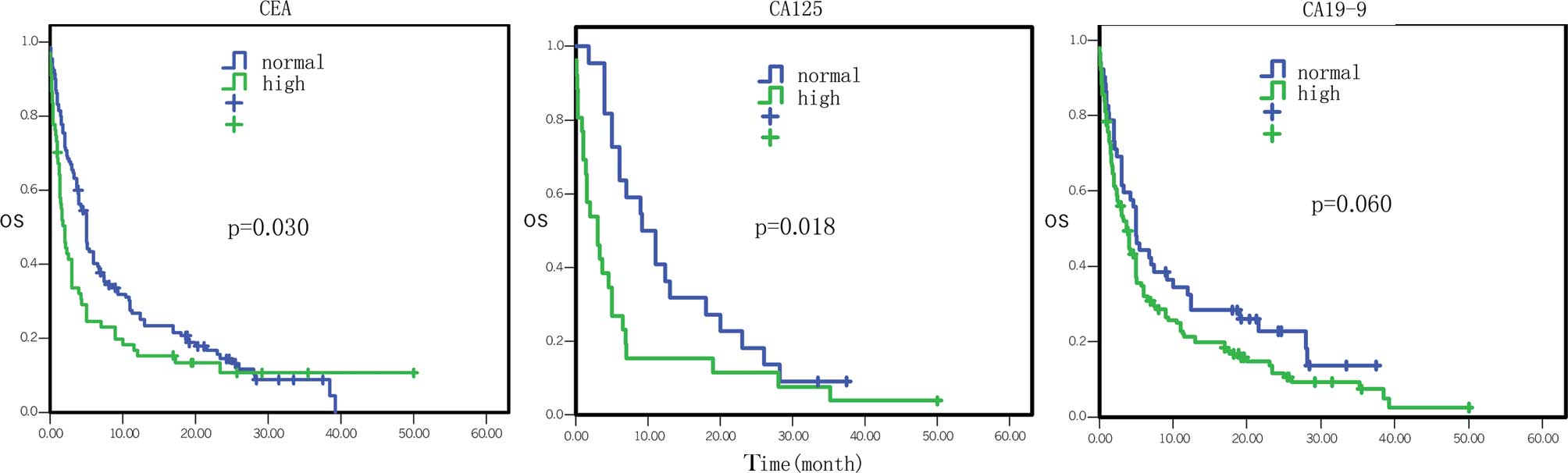
Analysis of tumor markers indicated that the
patients with high serum CEA levels had a median survival of 2.0
vs. 5.0 months in patients with normal levels, which was
statistically significant (HR=1.43, 95% CI 1.04–1.98, P=0.030;
Fig. 7). Patients with high serum
CA125 levels had a median survival of 3.1 vs. 10.1 months in
patients with normal levels (HR=2.06, 95% CI 1.13–3.76, P=0.018;
Fig. 7). Patients with high serum
CA19–9 levels had a median survival of 3.8 months vs. 5.0 months in
patients with normal levels (HR=1.41, 95% CI 0.99–2.02, P= 0.060;
Fig. 7). However, the serum levels
of CA15-3, CA72-4, CA50 and CA242 were not associated with survival
(P>0.05).
Cox multivariate regression analysis data of the
overall survival are presented in Table II. The most influential factors
were tumor stage, treatment selection, levels of serum albumin and
BUN (Fig. 6), WBC and platelet
counts, and serum CA19-9 levels (P<0.05). In brief, the
mortality risk of patients with advanced stage disease was
increased by 46% (HR=1.46, 95% CI 1.19-1.78, P= 0.000). The
mortality risk of patients who underwent surgery, chemotherapy,
interventional therapy, biliary drainage or comprehensive treatment
was reduced by 49% compared to patients who did not undergo
treatment or only received supportive treatment (HR= 0.51, 95% CI
0.36–0.73, P=0.000). The mortality risk of patients with high
levels of serum albumin, BUN, platelets and CA19-9 was reduced by
38, 57, 27 and 53%, respectively, and the mortality risk of
patients with high WBC counts was increased by 49% (P<0.05).
However, other factors, such as gender, age, site of primary
cancer, the levels of TB, DB, GPT, GOT, serum creatinine, serum
LDH, blood glucose and hemoglobin, were not associated with
mortality risk (P>0.05).
| Table II.Cox multivariate regression analysis
of 302 pancreatic cancer patients. |
Table II.
Cox multivariate regression analysis
of 302 pancreatic cancer patients.
| Parameter | DF | Wald Chi-square
test | P-value | Hazard ratio (95%
CI) |
|---|
| Gender | 1 | 0.03 | 0.855 | 1.03
(0.75–1.41) |
| Age | 1 | 0.42 | 0.517 | 0.91
(0.69–1.21) |
| Site of primary
cancer | 1 | 2.38 | 0.123 | 1.25
(0.94–1.66) |
| Stage | 1 | 13.60 | 0.000 | 1.46
(1.19–1.78) |
| Treatment | 1 | 13.93 | 0.000 | 0.51
(0.36–0.73) |
| Total
bilirubin | 1 | 0.17 | 0.678 | 0.93
(0.65–1.33) |
| Direct
bilirubin | 1 | 2.45 | 0.117 | 1.38
(0.92–2.06) |
| Glutamic-pyruvic
transaminase | 1 | 0.05 | 0.825 | 0.94
(0.56–1.58) |
| Glutamic-oxalacetic
transaminase | 1 | 0.00 | 0.970 | 0.99
(0.60–1.63) |
| Albumin | 1 | 6.10 | 0.014 | 0.62
(0.42–0.91) |
| Blood urea
nitrogen | 1 | 9.81 | 0.002 | 0.43
(0.25–0.73) |
| Serum
creatinine | 1 | 0.60 | 0.437 | 0.83
(0.53–1.32) |
| Lactate
dehydrogenase | 1 | 2.57 | 0.109 | 1.31
(0.94–1.82) |
| Blood glucose | 1 | 3.59 | 0.058 | 0.57
(0.31–1.02) |
| Hemoglobin | 1 | 1.10 | 0.295 | 0.82
(0.56–1.20) |
| White blood
cells | 1 | 6.92 | 0.009 | 1.49
(1.11–2.01) |
| Platelets | 1 | 3.94 | 0.047 | 0.73
(0.53–1.00) |
| CEA | 1 | 0.32 | 0.573 | 1.11
(0.77–1.59) |
| CA19-9 | 1 | 4.54 | 0.033 | 1.53
(1.04–2.25) |
| CA125 | 1 | 1.88 | 0.171 | 1.86
(0.77–4.50) |
| CA15-3 | 1 | 0.32 | 0.574 | 1.22
(0.61–2.41) |
| CA72-4 | 1 | 0.70 | 0.404 | 0.68
(0.27–1.69) |
| CA50 | 1 | 0.01 | 0.924 | 0.96
(0.45–2.05) |
| CA242 | 1 | 0.81 | 0.370 | 0.63
(0.24–1.72) |
Effects of treatment selection on overall
survival of pancreatic cancer patients
The survival of the patients who underwent
supportive treatment or no treatment was used as the control and
the various treatment selections vs. the survival of the patients
are presented in Table III and
Fig. 2. In particular, the median
survival of patients who did not receive any treatment or just
received supportive treatment was 1.3 months, while the median
overall survival of patients who underwent surgery, chemotherapy,
biliary drainage therapy, arterial interventional chemotherapy and
comprehensive treatment was 11.0, 7.3, 3.5, 9.0 and 11.0 months,
respectively. The mortality risk for these treatments decreased by
61% (95% CI 0.28–0.55, P=0.000), 52% (95% CI 0.35–0.68, P=0.000),
52% (95% CI 0.24–0.94, P=0.031), 57% (95% CI 0.29–0.63, P=0.000)
and 72% (95% CI 0.26–0.54, P=0.000), respectively.
| Table III.Treatment selections and survival of
pancreatic cancer patients. |
Table III.
Treatment selections and survival of
pancreatic cancer patients.
| Parameter | No. | Median survival
(months; 95% CI) | P-value | Hazard ratio (95%
CI) |
|---|
| Supportive or no
therapy | 67 | 1.3 (1.0–3.0) | | |
| Surgery | 140 | 11.0
(7.8–13.5) | 0.000 | 0.39
(0.28–0.55) |
| Chemotherapy | 115 | 7.3 (6.0–9.3) | 0.000 | 0.48
(0.35–0.68) |
| Endoscopic
retrograde biliary drainage | 17 | 3.5 (2.2–8.8) | 0.031 | 0.48
(0.24–0.94) |
| Transcatheter
arterial infusion chemotherapy | 57 | 9.0 (7.3–12.8) | 0.000 | 0.43
(0.29–0.63) |
| Combined
therapy | 86 | 11.0
(9.0–14.2) | 0.000 | 0.38
(0.26–0.54) |
A comparison of the overall survival between radical
surgery and palliative surgery treatment is presented in Table IV and Fig. 2. In brief, the median survival of
patients receiving radical surgery was 17.6 months vs. 8.3 months
in patients receiving palliative surgery; these data did not reach
statistical significance (HR=1.50; 95% CI 0.98–2.29, P=0.065).
| Table IV.Effect of surgical modalities on the
survival of pancreatic cancer patients. |
Table IV.
Effect of surgical modalities on the
survival of pancreatic cancer patients.
| Parameter | No. | Median survival
(months; 95% CI) | P-value | Hazard ratio (95%
CI) |
|---|
| Radical
surgery | 47 | 17.6
(9.3–23.6) | | |
| Palliative
surgery | 74 | 8.3 (7.0–12.1) | 0.065 | 1.50
(0.98–2.29) |
The data on the association of chemotherapy with the
survival of pancreatic cancer are presented in Table V. In particular, single-drug
chemotherapy had no statistically significant difference in
survival compared to the multi-drug regimen (P>0.05).
Chemotherapy using gemcitabine had no statistically significant
difference in survival compared to fluorouracil (P>0.05;
Fig. 2). However, the mortality
risk of patients who received platinum chemotherapy was decreased
(HR= 0.56, 95% CI 0.35–0.88, P= 0.011) compared to the patients who
did not receive drug therapy (Fig.
2), although there was no distinction among cisplatin,
carboplatin and oxaplatin (P>0.05).
| Table V.Effect of chemotherapy regimens on
the survival of pancreatic cancer patients. |
Table V.
Effect of chemotherapy regimens on
the survival of pancreatic cancer patients.
| Parameter | No. | Median survival
(months; 95% CI) | P-value | Hazard ratio (95%
CI) |
|---|
| Multi-drug vs.
single-drug regimen | | | | |
| Multi-drug | 58 | 7.6 (6.0–10.0) | | |
| Single-drug | 35 | 7.6 (4.2–15.6) | 0.743 | 0.92
(0.57–1.49) |
| Gemcitabine,
fluorouracil and combined regimen | | | | |
| Gemcitabine | 50 | 7.6 (6.0–14.2) | | |
| Fluorouracil | 25 | 5.0 (3.7–10.0) | | |
| Combined | 18 | 9.3 (7.1–11.0) | 0.364 | 1.09
(0.90–1.32) |
| Gemcitabine | | | | |
| Yes | 68 | 9.0 (7.1–11.0) | | |
| No | 25 | 5.0 (3.7–10.0) | 0.956 | 0.99
(0.58–1.68) |
| Fluorouracil | | | | |
| Yes | 43 | 7.4 (4.5–10.0) | | |
| No | 50 | 7.6 (6.0–14.2) | 0.504 | 1.17
(0.74–1.84) |
| Platinum (1) | | | | |
| With | 48 | 10.0
(7.6–14.0) | | |
| Without | 47 | 5.0 (3.2–7.1) | 0.011 | 0.56
(0.35–0.88) |
| Platinum (2) | | | | |
| Cisplatin | 8 | 7.9 (5.1–17.0) | | |
| Carboplatin | 15 | 9.6 (6.0–17.3) | | |
| Oxaliplatin | 23 | 12.4
(10.0–19.0) | 0.093 | 0.70
(0.46–1.06) |
In addition, the overall survival of pancreatic
cancer patients with arterial cannula interventional chemotherapy
(Table VI) was not statistically
different between gemcitabine and fluorouracil (P>0.05).
| Table VI.Effect of transcatheter arterial
infusion chemotherapy on the survival of pancreatic cancer
patients. |
Table VI.
Effect of transcatheter arterial
infusion chemotherapy on the survival of pancreatic cancer
patients.
| Parameter | No. | Median survival
(months; 95% CI) | P-value | Hazard ratio (95%
CI) |
|---|
| Gemcitabine | 17 | 13.1
(5.8–31.0) | | |
| Fluorouracil | 29 | 7.3 (5.1–11.0) | | |
| Combined
regimen | 11 | 9.3 (7.6–30.0) | 0.672 | 0.94
(0.71–1.25) |
Discussion
To date, the survival of pancreatic cancer patients
remains very poor as it is usually diagnosed at the advanced
stages, which are unsuitable for surgery, and chemotherapy is
ineffective in the management of tumor progression and metastasis.
In the present study, we investigated the factors potentially
associated with the overall survival of patients, which may in turn
provide a novel strategy in increasing survival. Our data showed
that the median survival of the patients was 6.1 months, with 1-,
2- and 3-year survival rates of 30.1, 10.6 and 2.6%, respectively.
The Cox analysis showed that the site of primary cancer, tumor
stages, treatment selections, levels of serum GPT, albumin, BUN,
LDH and hemoglobin, CEA, CA19-9 and CA125, as well as WBC counts
were statistically associated with overall survival. Furthermore,
the median survival of patients who underwent surgery,
chemotherapy, biliary drainage therapy, arterial interventional
chemotherapy and comprehensive treatment with a variety of methods
was better that that of patients that only underwent supportive
treatment or no treatment. The mortality risk in patients who
received the platinum chemotherapy regimen was reduced compared to
that of patients who did not receive such a drug. The data from the
present study indicate that further study is required to confirm
these data, and that the use of platinum-based chemotherapy may
improve the overall survival of patients with pancreatic
cancer.
Previous studies demonstrated that the median
survival of pancreatic cancer patients with post-operative adjuvant
therapy was 11–23 months, and that the 5-year survival rate was
approximately 20%. The diagnosis rate of locally advanced disease
patients without distant metastasis was 15–20%, with a median
overall survival of 6–10 months (11,12).
The management of pancreatic cancer with a variety of comprehensive
combined treatments, including surgery, is the primary clinical
practice used presently (13). Our
current data showed that the median overall survival of these
patients without any treatment or only with supportive treatment
was only 1.3 months. The overall survival of the patients who
underwent surgery, chemotherapy, arterial interventional
chemotherapy, biliary drainage and comprehensive treatment
following diagnosis was increased to varying degrees. For example,
the median overall survival of pancreatic cancer patients with
surgery followed by other comprehensive treatments was 11.0 months,
which is compatible with previously published literature (10). Of the patients who underwent
surgery, those receiving radical tumor resection tended to have
longer survival rates than those who underwent palliative tumor
resection, although this did not reach a statistically significant
difference (HR=1.50, 95% CI 0.98–2.29, P= 0.065). Therefore,
radical resection should be recommended if the patient is capable
of undergoing it.
Moreover, the present study also demonstrated that
the median survival of the patients treated with chemotherapy was
7.3 months, which was longer than that of patients who did not
receive treatment or only received supportive treatment. In
addition, there was no statistical difference in survival between
single-drug and multi-drug chemotherapy regimens, and between
fluorouracil- and gemcitabine-containing regimens. However, a
previous study by Joo et al (14) found that chemotherapy was an
independent prognostic factor for the survival of pancreatic cancer
patients. Another study by Burris et al (15) compared the effect of gemcitabine
with fluorouracil regimens on locally advanced and metastatic
pancreatic cancer, and their data showed that the median survival
of the patients who received fluorouracil treatment was 4.41
months, while that of the patients who received gemcitabine therapy
was 5.65 months, but there was no statistical difference in overall
survival between these two treatments.
Another study using gemcitabine monotherapy as a
control, found that the combined therapy with platinum and
gemcitabine did improve the progression-free survival and overall
response rate in patients, but did not improve overall survival
(16). These data were similar to
our current findings suggesting that chemotherapy did not alter the
overall survival time of pancreatic cancer patients. However, our
data demonstrated that the median overall survival of the patients
who received platinum reduced the mortality risk by 44%. In other
words, it increased the survival rate of the patients, which
confirmed the data from a previous study reported by Heinemann
et al that patients with gemcitabine plus platinum treatment
had longer progression-free survival and overall survival than
patients receiving gemcitabine alone (17). This benefit was even greater in a
subgroup of patients with a performance status of 017.
Again, our current data indicated that there was no difference
among cisplatin, carboplatin and oxaplatin. The overall survival of
the patients who underwent arterial interventional chemotherapy was
prominently increased compared to the patients who received no
treatment or only supportive treatment, whereas patients who
underwent gemcitabine- and fluorouracil-containing treatments had
no difference in overall survival, and these data were similar to
the Burris et al study (18).
The prognosis of pancreatic cancer is associated
with a variety of factors, such as age, occupation, disease
history, tumor location, surgery method, post-operative
complication and TNM stage (6).
Indeed, the present study showed that the site of primary cancer,
tumor stages, treatments, serum levels of GPT, albumin, LDH and
hemoglobin and WBC counts were independent prognostic factors using
Cox univariate analysis, while Cox multivariate analysis revealed
that tumor site, stage and treatment were independent prognostic
factors. The poor prognosis of pancreatic cancer located in the
body and tail of the pancreas is due to the fact that these tumors
cause symptoms much later than those in other locations, such as
the head of the pancreas. Therefore, tumors in the body and tail of
the pancreas are usually at a more advanced stage at diagnosis and
commonly unresectable (19). By
contrast, tumors located at the head of the pancreas cause
obstructive jaundice at an early stage, which usually leads to
medical attention being sought much earlier, making them more
curable and thus leading to a more favorable prognosis (20).
This study further showed that there was no survival
difference between patients with high and normal serum levels of TB
and DB, while the patients with high serum GPT levels had favorable
prognosis. The latter has not been previously reported. Moreover,
the median survival of the patients who had obstructive jaundice
and underwent biliary drainage treatment was 3.5 months, which was
2 months longer than that of patients who did not receive any
treatment or who received best supportive treatment. The reason may
be that obstructive jaundice can be easily identified as a tumor in
the head of the pancreas and, thus, a biliary drainage procedure
would be an effective palliative treatment for such patients.
In addition, our present data demonstrated that the
patients with high serum LDH levels had poor prognosis. A previous
study reported by Faruk et al (21) suggested that the serum LDH levels
correlated with tumor burden and reflected tumor growth and
invasion potential; thus, pancreatic cancer patients with elevated
serum LDH levels had shorter survival. Furthermore, in our study, 7
tumor-associated antigens were studied in connection with
pancreatic cancer, including CEA, CA19-9, CA125, CA15-3, CA72-4,
CA50 and CA242. Among these tumor markers, patients with high serum
levels of CEA, CA19-9 or CA125 had poor prognosis compared to the
patients with normal serum levels of these tumor markers. These
data are in agreement with data from previous studies (22,23).
However, in our study, low WBC counts were associated with
favorable patient survival, indicating that negative
immunoreactions may occur in pancreatic cancer.
In conclusion, this study investigated the
association of clinicopathological parameters, treatment selections
and laboratory test data with the prognosis of pancreatic cancer
patients. We found that these data are useful in assessing
prognosis and could guide future clinical practice in the
management of pancreatic cancer patients.
Acknowledgements
This study was sponsored in part by
grants from the Science and Technology Commission, Shanghai
Municipality and Minghang district, Shanghai Municipal Health
Bureau (Nos. 2008MW23, 2009MW17 and 2010MHZ042).
References
|
1.
|
D GoldsteinS CarrollM ApteModern
management of pancreatic carcinomaIntern Med
J34475481200410.1111/j.1444-0903.2004.00658.x15317546
|
|
2.
|
K HirataT SatoM MukaiyaResults of 1001
resections for invasive ductal adenocarcinoma of the pancreasArch
Surg132771776199710.1001/archsurg.1997.014303100850189230864
|
|
3.
|
A NakaoA HaradaT NonamiLymph node
metastasis in carcinoma of the body and tail of the pancreasBr J
Surg8410901092199710.1002/bjs.18008408139278647
|
|
4.
|
K ShimadaY SakamotoT SanoPrognostic
factors after distal pancreatectomy with extended lymphadenectomy
for invasive pancreatic adenocarcinoma of the body and
tailSurgery139288295200610.1016/j.surg.2005.08.00416546491
|
|
5.
|
JP NeoptolemosDD StockenH FriessA
randomized trial of chemoradiotherapy and chemotherapy after
resection of pancreatic cancerN Engl J
Med35012001210200410.1056/NEJMoa03229515028824
|
|
6.
|
QH ZhangQX LiClinical analysis of 2340
cases of pancreatic carcinomaNatl Med J
China84214218200415059537
|
|
7.
|
M KandaT FujiiY KoderaNutritional
predictors of postoperative outcome in pancreatic cancerBr J
Surg98268274201110.1002/bjs.730520960457
|
|
8.
|
Y MurakamiK UemuraT SudoNumber of
metastatic lymph nodes, but not lymph node ratio, is an independent
prognostic factor after resection of pancreatic carcinomaJ Am Coll
Surg211196204201010.1016/j.jamcollsurg.2010.03.03720670857
|
|
9.
|
U BoggiM del ChiaroC CrocePrognostic
implications of tumor invasion of adhesion to peripancreatic
vessels in resected pancreatic
cancerSurgery146869881200910.1016/j.surg.2009.04.02919744432
|
|
10.
|
J FatimaT SchnelldorferJ
BartonPancreatoduodenectomy for ductal adenocarcinoma: implications
of positive margin on survivalArch
Surg145167172201010.1001/archsurg.2009.28220157085
|
|
11.
|
V HeinemannPresent and future treatment of
pancreatic carcinomaSemin
Oncol292331200210.1053/sonc.2002.3426912094335
|
|
12.
|
YJ ChuaD CunninghamAdjuvant treatment for
respectable pancreatic cancerJ Clin
Oncol2345324537200510.1200/JCO.2005.17.95416002844
|
|
13.
|
D LiK XieR WolffPancreatic
cancerLancet36310491057200410.1016/S0140-6736(04)15841-8
|
|
14.
|
KP JooBY YongK Yong-TaeSurvival and
prognostic factors of unresectable pancreatic cancerJ Clin
Gastroenterol428691200810.1097/01.mcg.0000225657.30803.9d18097296
|
|
15.
|
V HeinemannGemcitabine in the treatment of
advanced pancreatic carcinoma: a comparative analysis of randomized
trialsSemin Oncol29916200210.1053/sonc.2002.3737212577228
|
|
16.
|
B EmilioM MicheleG AlainGemcitabine-based
combinations for inoperable pancreatic carcinoma: have we made real
progress? A meta-analysis of 20 phase 3
trialsCancer110525533200710.1002/cncr.2280917577216
|
|
17.
|
V HeinemannR LabiancaA HinkeIncreased
survival using platinum analog combined with gemcitabine as
compared to single-agent gemcitabine in advanced pancreatic cancer:
pooled analysis of two randomized trials, the GERCOR/GISCAD
intergroup study and a German multicenter studyAnn
Oncol1816521659200710.1093/annonc/mdm283
|
|
18.
|
HA Burris IIIMJ MooreMR GreenImprovements
in survival and clinical benefit with gemcitabine as first-line
therapy for patients with advanced pancreas cancer: a randomized
trialJ Clin Oncol152403241319979196156
|
|
19.
|
F TakeoN ToshioG NaotoEvaluation of the
prognostic factors and significance of lymph node status in
invasive ductal carcinoma of the body or tail of the
pancreasPancreas394854201010.1097/MPA.0b013e3181bd5cfa19910836
|
|
20.
|
W IchiroS SatoshiK MasaruOnset symptoms
and tumor locations as prognostic factors of pancreatic
carcinomaPancreas28160165200410.1097/00006676-200403000-0000715028948
|
|
21.
|
T FarukA FarukA SuleymanPrognostic factors
in pancreatic carcinoma serum LDH levels predict survival in
metastatic diseaseAm J Clin
Oncol24547550200110.1097/00000421-200112000-0000311801751
|
|
22.
|
J LouhimoH AlfthanUH StenmanSerum HCG beta
and CA72-4 are stronger prognostic factors than CEA, CA19-9 and
CA242 in pancreatic
cancerOncology66126131200410.1159/00007743815138364
|
|
23.
|
JE KimKT LeeJK LeeClinical usefulness of
carbohydrate antigen 19-9 as a screening test for pancreatic cancer
in an asymptomatic populationJ Gastroenterol
Hepatol19182186200410.1111/j.1440-1746.2004.03219.x14731128
|