Introduction
Since Carney et al reported a rare thyroid
lesion termed hyalinizing trabecular adenoma (HTA) presenting with
characteristics of a trabecular growth pattern and hyalinizing
stroma in 1987, controversies concerning the classification of this
entity have arisen (1). Most
believe it to be a unique entity, whereas others have argued that
it is a variant of papillary carcinoma. To make it even more
complicated, the majority of the reported cases were benign, while
a few, which were accompanied by metastasis in the lymph nodes or
the lung, were named hyalinizing trabecular carcinoma (HTC)
(2). Due to the uncertain
malignant potential and entity of this tumor, a more general term,
hyalinizing trabecular tumor (HTT), has been adopted by most
pathologists and the World Health Organization classification,
which reflects such controversy.
In clinical and pathological practice, HTT is
frequently misdiagnosed and is managed as other thyroid neoplasms
due to the similarity in morphology, mimicking papillary thyroid
carcinoma (PTC) and medullary thyroid carcinoma (MTC). Although HTT
has attracted the interest of pathologists, according to our
knowledge such enthusiasm has not been stimulated in clinicians. In
fact, it is crucial for surgeons to recognize the features of this
lesion to ensure effective treatment and management of HTT. For
example, currently, lobectomy is recommended for HTTs, but
mistreatment may result in cases where total thyroidectomy has been
undertaken. Herein, we present the diagnosis and management of a
typical HTT case and general information concerning HTT is also
presented.
Case report
A female patient 42 years of age presented with a
single lump in the right side of the neck. Ultrasonography revealed
a solid cold nodule, which was regarded as a thyroid adenoma. Thus,
the intact neoplasm was surgically removed for pathological
examination.
Gross investigation showed an encapsulated mass of
5×3.5×2.5 cm. The cut surface was homogeneously pale and rigid.
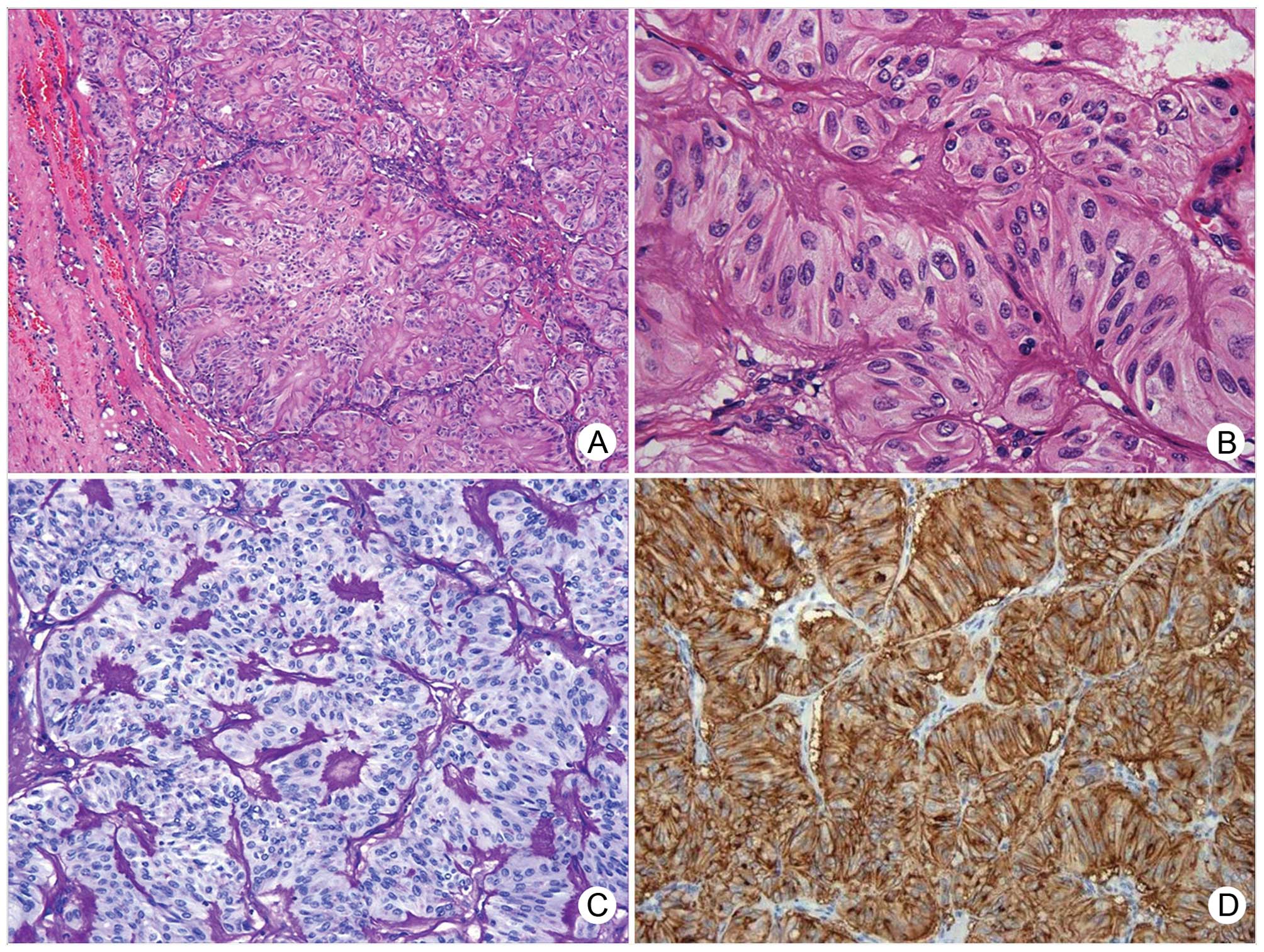
Microscopically, the lump was surrounded by a thin capsule, and no
malignant morphological features, including capsular or vascular
invasions, were observed (Fig.
1A). The tumor was characterized by trabecular structures
separated by minimal fibrous stroma. The intratrabecular hyalin and
colloid was prominent, which consisted of basement membrane
material rather than amyloid with PAS positivity (Fig. 1C) and Congo Red negativity.
Alveolar and Zellballen structures were also present, partitioned
by sinus vascular network, similar to those noted in
paragangliomas. The tumor cells were polygonal, oval, or high
columnar with an acidophilic or clear cytoplasm. The nuclei were
round or oval with inconspicuous small nucleoli, with prominent
grooves and less frequent pseudoinclusions (Fig. 1B). Mitosis and psammoma bodies were
rare or absent.
Immunohistochemical study of these tumors showed
positivity for thyroglobulin, thyroid transcription factor-1
(TTF-1) and gelactin-3, and negativity for calcitonin,
cytokeratin-19, synaptophysin and chromogranin A. Staining with the
MIB-1 antibody showed a distinctive membranous pattern (Fig. 1D), whereas other clones of Ki-67,
such as SP2 or 7B11, showed a common nuclear pattern, with an index
of <1%. Staining for the anti-P53 antibody was negative. After a
follow-up of 4 years the patients was alive without local
recurrence or metastasis.
Discussion
HTT is a rare and controversial thyroid lesion,
prevalent in females between the fourth and fifth decades of age.
The entity remains controversial as HTT was originally believed to
be a distinct neoplasm, but others regard it as a variant of PTC as
some similarities are noted in nuclear features. RET/PTC
rearrangements, which are characteristic of a specific molecular
event of PTC, were noted in HTT samples by immunohistochemistry
staining and reverse transcription-polymerase chain reaction, and
the ratio was nearly identical to that of PTC (3,4). All
of these observations reinforced the fact that HTT is a variant of
PTC. However, as previously pointed out, the conclusion was
arbitrary as RET rearrangements may also occur in other thyroid
lesions, such as lymphocytic thyroiditis which is frequently
associated with HTT. Moreover, cytokeratin-19 and gelactin-3, which
are expressed strongly in PTC, were expressed at weak levels in
HTT. MIB-1 staining of HTT samples exhibits a distinctive
membrane-positive pattern rather than nuclear positivity; however,
this finding has not been observed in PTC samples. In contrast to
the high prevalence for mutations of the BRAF and N-ras genes in
PTC, such have not been detected in HTT patients (5). The five microRNAs, which have been
found to be upregulated in PTC, were verified to be downregulated
in HTT (6). These provide evidence
that HTT is distinct from PTC. Thus, to date, HTT is diagnosed as
an independent neoplasm, rather than one variant of PTC.
Moreover, one additional controversy is whether HTT
is a benign or malignant neoplasm. In early reports, malignant
phenotypes such as vascular or capsular invasion, or a high index
of mitoses were not observed in histological studies. However, the
benign nature of these tumors has been challenged in subsequent
descriptions of vascular invasion in aggressive cases or with
metastases to the lymph nodes and lung (2). In his most recent report, Carney
et al investigated 119 cases of HTT for invasion, recurrence
and metastasis, and obtained follow-up for 96% of the cases
(7). In their biggest series to
date, only one case showed vascular and capsular invasion and
pulmonary metastasis. Thus, it was confirmed that the overwhelming
majority of HTTs behave as benign neoplasms. Thus in clinical
practice, sufficient dissection and careful observation of
vascular, capsular and parenchymal invasion is essential to
eliminate the minute possibility of malignancy.
Despite the fact that the entity of HTT is not
entirely clear, it is frequently misdiagnosed as a malignant
thyroid lesion. Surgeons should be aware that HTT can be mistaken
for PTC or MTC following pathological evaluation, particulary when
using cytological or frozen sections, whereas it may be considered
as a benign lesion in ultrasonography (8,9).
Preoperative cytology using fine needle aspiration biopsy of
thyroid nodules is the most effective and widely used method to
distinguish the nature of these lesions. However, the features of
hypercellularity and grooves, pseudoinclusions and
hyperchromaticity of the nuclei, which are the main diagnostic
clues for HTT, are also often observed in patients with classical
PTC (10–13). In most reported cases, these tumors
are diagnosed as ‘suspicious or even diagnostic for PTC’ in
cytological evaluations, and few tumors are diagnostic or
suspicious for HTT, partly since cytologists are not familiar with
HTT. Similarly, frozen sections are seldom useful for the diagnosis
of HTT. In our experience with the 42-year-old patient, we
initially diagnosed the patient as ‘suspicious for PTC’ based on
the nuclear features observed in the frozen section, but we made no
recommendations for further treatment until we had obtained a
definite pathological diagnosis. Thus, surgeons should be aware
that the preoperative cytological or frozen sectional diagnosis may
not necessarily agree with the final pathological diagnosis due to
the overlapping nature between HTT and PTC. In addition, surgeons
can inform the patients that most cases of HTT are benign and are
associated with a much more favorable outcome than PTC.
The differentiation of HTT from other thyroid
tumors, such as MTC or PTC and occasionally, primary thyroid
paraganglioma with trabecular architecture, can be achieved by
histochemistry and immunohistochemistry besides morphology. HTT
usually stains positive for thyroid follicular epithelial markers,
such as thyroglobulin and TTF-1, and negative for calcitonin, NSE,
chromogranin A or synaptophysin. The hyalinizing material is
PAS-positive and Congo Red-negative in special staining, and is
positive for collagen type IV in immunostaining, which has been
demonstrated for basal lamina-like substance ultrastructurally
(14). On the contrary, MTC often
expresses calcitonin and neuroendocrine markers and exhibits
positive staining for Congo Red. Thyroid paraganglioma is a rare
lesion which expresses neuroendocrine markers.
Differentiating HTT from PTC is more challenging due
to the similarities in cellular morphology and origin. PTC often
displays strong positive staining for CK19 and galectin-3, whereas
these markers are weakly expressed in HTT (15). MIB-1 staining pattern is useful as
the membrane-positive reactivity is a distinctive feature of HTT,
however, no such pattern appears in PTC. Notably, it has been
reported that the membrane-positive pattern is observed for the
MIB-1 clone only but not other clones of Ki-67, which was also
confirmed in our present study (16).
To date, the etiology of HTT remains to be fully
clarified. This tumor may arise in the background of chronic
lymphocytic thyroiditis and multinodular goiter, or in association
with PTC. The link between HTT and lymphocytic thyroiditis may be
significant due to similarities in molecular genetics and age or
gender distribution. However, this remains to be addressed in
future studies. The prognosis of most HTT cases is favorable,
therefore, lobectomy treatment is sufficient; however, when HTT is
accompanied by metastasis, we require further knowledge regarding
treatment and prognosis.
In summary, HTT represents a rare and controversial
thyroid tumor. It has a characteristic trabecular growth pattern
and hyalinizing stroma. The differentiation of HTT from other
thyroid tumors such as PTC and MTC can be achieved using
histochemistry and immunohistochemistry in addition to morphology.
In general, the prognosis of HTT is favorable, whereas a few cases
may be accompanied by morphological malignant features or
metastases.
References
|
1.
|
Carney JA, Ryan J and Goellner JR:
Hyalinizing trabecular adenoma of the thyroid gland. Am J Surg
Pathol. 11:583–591. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Gowrishankar S, Pai SA and Carney JA:
Hyalinizing trabecular carcinoma of the thyroid gland.
Histopathology. 52:529–531. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Papotti M, Volante M, Giuliano A, Fassina
A, Fusco A, Bussolati G, Santoro M and Chiappetta G: RET/PTC
activation in hyalinizing trabecular tumors of the thyroid. Am J
Surg Pathol. 24:1615–1621. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Cheung CC, Boerner SL, MacMillan CM,
Ramyar L and Asa SL: Hyalinizing trabecular tumor of the thyroid: a
variant of papillary carcinoma proved by molecular genetics. Am J
Surg Pathol. 24:1622–1626. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Salvatore G, Chiappetta G, Nikiforov YE,
Decaussin-Petrucci M, Fusco A, Carney JA and Santoro M: Molecular
profile of hyalinizing trabecular tumours of the thyroid: high
prevalence of RET/PTC rearrangements and absence of B-raf and N-ras
point mutations. Eur J Cancer. 41:816–821. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Sheu SY, Vogel E, Worm K, Grabellus F,
Schwertheim S and Schmid KW: Hyalinizing trabecular tumour of the
thyroid – differential expression of distinct miRNAs compared with
papillary thyroid carcinoma. Histopathology. 56:632–640. 2010.
|
|
7.
|
Carney JA, Hirokawa M, Lloyd RV, Papotti M
and Sebo TJ: Hyalinizing trabecular tumors of the thyroid gland are
almost all benign. Am J Surg Pathol. 32:1877–1889. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Casey MB, Sebo TJ and Carney JA:
Hyalinizing trabecular adenoma of the thyroid gland: cytologic
features in 29 cases. Am J Surg Pathol. 28:859–867. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Lee S, Han BK, Ko EY, Oh YL, Choe JH and
Shin JH: The ultrasonography features of hyalinizing trabecular
tumor of the thyroid are more consistent with its benign behavior
than cytology or frozen section readings. Thyroid. 21:253–259.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Gupta S, Modi S, Gupta V and Marwah N:
Hyalinizing trabecular tumor of the thyroid gland. J Cytol.
27:63–65. 2010. View Article : Google Scholar
|
|
11.
|
Santosh KV, Raychaudhuri S, Subramanya H
and Naveen Kumar BJ: Cytology of hyalinising trabecular
adenoma-like variant of medullary thyroid carcinoma. J Cancer Res
Ther. 7:189–191. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Bishop JA and Ali SZ: Hyalinizing
trabecular adenoma of the thyroid gland. Diagn Cytopathol.
39:306–310. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Kim T, Oh YL, Kim KM and Shin JH:
Diagnostic dilemmas of hyalinizing trabecular tumours on fine
needle aspiration cytology: a study of seven cases with BRAF
mutation analysis. Cytopathology. 22:407–413. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Ohtsuki Y, Kimura M, Murao S, Okada Y,
Teratani Y, Matsumoto M, Kurabayashi A, Iguchi M, Lee GH and
Furihata M: Immunohistochemical and electron microscopy studies of
a case of hyalinizing trabecular tumor of the thyroid gland, with
special consideration of the hyalinizing mass associated with it.
Med Mol Morphol. 42:189–194. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Lee S, Hong S and Koo JS:
Immunohistochemical subclassification of thyroid tumors with a
prominent hyalinizing trabecular pattern. APMIS. 119:529–536. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Leonardo E, Volante M, Barbareschi M,
Cavazza A, Dei Tos AP, Bussolati G and Papotti M: Cell membrane
reactivity of MIB-1 antibody to Ki67 in human tumors: fact or
artifact? Appl Immunohistochem Mol Morphol. 15:220–223. 2007.
View Article : Google Scholar : PubMed/NCBI
|