Introduction
Gliomas account for half of all primary intracranial
tumors (1). High-grade gliomas are
those gliomas of grades III–IV, also known as malignant gliomas
with poor prognosis. Glioblastoma multiforme is the most malignant
of the astrocytic tumors, which belong to the grade IV gliomas. The
goal of therapy in malignant gliomas is dependent on available
techniques and on the nature of the malignant glioma itself, and
the final objective of malignant glioma therapy is cytoreduction.
Multimodality therapy including surgery, radiotherapy and
chemotherapy can treat malignant gliomas, but rarely cures them.
Surgery can establish a diagnosis and remove the tumor, improving
the symptoms, but the role of surgical resection in treatment of
malignant gliomas remains controversial even after 75 years of
experience (2). There is evidence
that surgical reduction of the tumor to minimal residual amounts is
associated with prolonged survival. In one Brain Tumor Cooperative
Group study, CT scans from brain tumor patients were studied
several times over the course of their illness and compared to
their ultimate outcomes (3). There
was a marked inverse correlation between postoperative tumor size
and survival. This was especially notable in patients with minimal
or no residual enhancing tumor. The beneficial effect of surgery
was less marked where the aim was de-bulking as opposed to leaving
a minimal amount of residual tumor. A trend toward longer survival
was observed in patients whose tumors were reduced by 75% or more.
A similar result was reported in a study carried out by MRI
(4). Retrospective reviews have
indicated that surgery increases survival time in malignant glioma
patients (5). Radiation Therapy
Oncology Group data have indicated that surgical resection was
associated with statistically significantly longer survival and
median survival time (6).
Radiotherapy is a key treatment for malignant
gliomas. The Brain Tumor Study Group first reported in controlled
studies that whole-brain radiation therapy increases the survival
time of patients over those following surgery alone (7). Other data showed that patients
receiving 55–60 Gy survive for significantly longer than those
receiving 50 Gy or less (8).
Andersen et al reported that postoperative radiotherapy
improved the 6-month and 1-year survival rates of glioblastoma
patients (9). Kristiansen et
al studied 118 patients with supratentorial astrocytoma of
grades III–IV and revealed that postoperative radiotherapy
prolonged the median survival time to 10.8 months vs. 5.2 months in
the control group (10).
Laperriere et al reviewed systemic trials of postoperative
radiotherapy on malignant gliomas and carried out a meta-analysis.
Their results revealed that six randomized trials detected a
significant survival benefit favoring post-operative radiotherapy
compared with no radiotherapy (11).
Temozolomide (TMZ) is an oral preparation used in
newly diagnosed grade III and IV gliomas as adjuvant and
concomitant therapy to surgery and radiotherapy. It has the
advantages of being administered orally and exhibiting effective
blood-brain barrier (BBB) penetration, and may have low toxicity
(12). Watkins et al
reported that among glioblastoma patients, TMZ provided a
statistically significant survival improvement over no chemotherapy
(median survival 12.7 vs. 7.5 months; P=0.0058) (13). Stupp et al reported the
overall survival was 27.2% (95% CI, 22.2–32.5) at 2 years, 16.0%
(12.0–20.6) at 3 years, 12.1% (8.5–16.4) at 4 years, and 9.8%
(6.4–14.0) at 5 years with TMZ plus radiotherapy, versus 10.9%
(7.6–14.8), 4.4% (2.4–7.2), 3.0% (1.4–5.7), and 1.9% (0.6–4.4) with
radiotherapy alone (HR 0.6; 95% CI, 0.5–0.7; P<0.0001) (14).
Nimotuzumab is a humanized monoclonal antibody that
inhibits tumor cells and enhances chemoradiosensitivity, and has
already been used in combination with radiotherapy in unresectable
head and neck cancer patients (15,16).
A trend towards survival benefit for nimotuzumab-treated subjects
has been identified. Malignant gliomas are resistant to
radiotherapy and chemotherapy, and since the majority of patients
with malignant gliomas experience local recurrence, the prognosis
of patients with this tumor remains dismal. Therefore, we designed
randomly controlled trials to investigate the effect of nimotuzumab
on sensitization to the effect of radiochemotherapy on malignant
gliomas.
Materials and methods
Patient selection
Between June 2008 and February 2011, 41 patients
with malignant gliomas confirmed by pathological diagnosis
according to the World Health Organization criteria (17) who had not received prior treatment
were eligible to take part in the study. They were divided into the
nimotuzumab + radiochemotherapy (treatment group; 20 cases) and
placebo + radiochemotherapy (control group; 21 cases) groups. All
patients provided written informed consent. The protocols were
approved by the Institutional Research Review Board at Xiangya
Hospital of South Central University, Changsha, China. Eligibility
criteria comprised the following: age ≥18 years; Karnofsky
performance status (KPS) score ≥60%; grade III–IV glioma confirmed
by histopathology; predictive survival time ≥6 months; normal
function of major organs; bone marrow function: hemoglobin ≥10g/l,
white blood cell count ≥4x109/l, platelet count
≥100x109/l, normal renal function (serum creatinine, 1.2
mg/dl); existing lesions measurable by MRI; and no allergic
reaction to biological agents. Clinical data of the patients are
shown in Table I.
 | Table I.Clinical data of patients in the
treatment group and control group. |
Table I.
Clinical data of patients in the
treatment group and control group.
|
Characteristics | Treatment n
(%) | Control n (%) | Z | P-value |
|---|
| Total | 20 (100) | 21 (100) | | |
| Gender | | | | |
| Male | 14 (70) | 12 (57.1) | −0.111 | 0.912 |
| Female | 6 (30) | 9 (42.9) | | |
| Age | | | | |
| <40 years | 7 (35) | 9 (42.9) | −0.146 | 0.990 |
| 40–60 years | 12 (60) | 11 (52.4) | | |
| >60 years | 1 (1) | 1 (4.7) | | |
| Lesion
location | | | | |
| Temporal
lobe | 3 (15) | 5 (23.8) | 0.227 | 0.821 |
| Parietal
lobe | 5 (25) | 6 (28.6) | | |
| Frontal lobe | 5 (25) | 4 (19.0) | | |
| Occipital
lobe | 4 (20) | 3 (14.3) | | |
| Brain stem | 2 (10) | 3 (14.3) | | |
| Two or more than
two locations | 1 (5) | 0 (0) | | |
| Lesion side | | | | |
| Left | 6 (30) | 10 (47.6) | −0.776 | 0.438 |
| Right | 12 (60) | 8 (38.1) | | |
| Both sides | 2 (10) | 3 (14.3) | | |
| Extent of surgical
resection | | | | |
| Total
resection | 4 (20) | 6 (28.6) | −0.495 | 0.621 |
| Subtotal
resection | 13 (65) | 12 (57.1) | | |
| Biopsy | 3 (15) | 3 (14.3) | | |
| Interval between
surgery and radiotherapy | | | | |
| ≤1 month | 10 (50) | 8 (38) | −0.483 | 0.629 |
| >1 month | 10 (50) | 13 (62) | | |
| Histological
grade | | | | |
| III | 9 (45) | 8 (38.1) | −0.814 | 0.415 |
| IV | 4 (20) | 3 (14.3) | | |
| III–IVa | 7 (35) | 10 (47.6) | | |
| Modality of
radiotherapy | | | | |
| 3D-CRT | 2 (10) | 4 (19) | −0.809 | 0.418 |
| IMRT | 18 (90) | 17 (81) | | |
| Dose of
radiotherapy | | | | |
| <54 Gy | 3 (15) | 6 (28.6) | −0.637 | 0.524 |
| 54–60 Gy | 10 (50) | 9 (42.8) | | |
| >60 Gy | 7 (35) | 6 (28.6) | | |
Nimotuzumab treatment
In the radiotherapy period, the patients in the
treatment group received 200 mg intravenous nimotuzumab by drip,
once per week, continuing for six weeks. Nimotuzumab (200 mg) was
dissolved in 250 ml physiological saline. Infusion time was >60
minutes. Diphenhydramine (20 mg) was injected intramuscularly and
dexamethasone (10 mg) was infused intravenously to patients prior
to nimotuzumab infusion for the first time. In the absence of an
allergic reaction, diphenhydramine and dexamethasone were not
administered in subsequent doses. In the control group, patients
were administered placebo instead of nimotuzumab.
Chemotherapy
TMZ was used in conjunction with radiotherapy (RT)
and was administered in two phases. During RT, a daily dose of 75
mg/m2 was administered. On completion of RT, there was a
28-day treatment break, followed by a second phase of up to six
28-day cycles of maintained (adjuvant) TMZ treatment. Dosage was
150 mg/m2 once daily for 5 days followed by 23 days
without treatment. At the start of cycle 2, the dose was escalated
to 200 mg/m2/day if haematological toxicity was within
prescribed limits.
Radiotherapy
All patients were treated with intensity modulated
radiotherapy (IMRT) or three-dimensional conformal radiotherapy
(3D-CRT). Each patient was positioned and immobilized with an
individualized thermoplastic mask with treatment-planning CT.
Slices of 0.3 cm were obtained through the regions of interest.
Gross tumor volume (GTV), clinical tumor volume (CTV), and planning
tumor volume (PTV) were defined based on the treatment-planning CT,
with registration to MRI when possible, in accordance with the
International Commission on Radiation Units and Measurements 62
report (1999), according to pre- and postoperative MRI. Gross tumor
volume (GTV) or gross tumor volume tumor bed (GTVtb) were
delineated on contrasted MRI images. GTV or GTVtb with a 2.5–3.0 cm
margin were defined as clinical tumor volume (CTV). CTV with
0.3–0.5 cm margins were defined as planning tumor volume (PTV); GTV
or GTVtb with a 0.5-cm margin were defined as planning GTV (PGTV)
or planning GTVtb (PGTVtb); 3D-CRT or IMRT were delivered as
DT = 46–50 Gy/26–28 fractions to PTV or DT =
54–66 Gy/26–30 fractions to PGTV or PGTVtb; dose was in part
determined by critical structure tolerance.
Evaluation response
All patients were surgically treated with
exploratory craniotomy, tumorectomy and/or biopsy, and the extent
of surgical resection was evaluated by preoperative MRI, the
patient surgical record and the results of the last three-day
postoperative MRI. Based on this, patients were allocated total
resection, subtotal resection or biopsy procedures. Total resection
represented the complete removal of the visible tumor, subtotal
resection involved a 50–99% volume reduction and a biopsy indicated
a <50% resection. Objective response rates of the treatment
group and control group were evaluated using the Response
Evaluation Criteria in Solid Tumors (18). Complete response (CR) was defined
as disappearance of all target lesions. Partial response (PR) was
defined as a decrease of at least 30% in the sum of diameters of
target lesions, taking as reference the baseline sum diameters.
Progressive disease (PD) was defined as an increase of at least 20%
in the sum of diameters of target lesions, taking as reference the
smallest sum on study. Stable disease (SD) was defined as neither
sufficient shrinkage to qualify for PR nor sufficient increase to
qualify for PD, taking as reference the smallest sum diameters
while on study. Surgical resection extent and response rate were
determined by comparing the disease lesion of the enhancing tumor
on gadolinium-enhanced T1-weighted MR images at points preoperative
and postoperative (within 3 days following surgery) or after
completion of the radiotherapy. Response rate included complete
response and partial response. Enhanced disease lesion in
gadolinium-enhanced T1-weighted MR images was regarded as the basis
of tumor residual and tumor recurrence. The follow-up period began
on completion of radiotherapy. The MRI was scanned every three
months following radiotherapy to evaluate tumor relapse.
Statistical analysis
SPSS 13.0 was used to carry out the statistical
analysis. The mean and median survival times and 1-year survival
rate were calculated using the Kaplan-Meier method. Mean and median
survival times and 1-year survival rate between the treatment group
and control group were compared using the log-rank method. The
Wilcoxon rank sum test was used to apply the equilibrium analysis
of the two groups’ data. The difference in objective response rate
between the treatment and control groups was evaluated using the
Pearson Chi-square test. A p-value <0.05 was considered to
indicate statistical significance in all statistical analyses.
Results
Survival in the treatment and control
groups
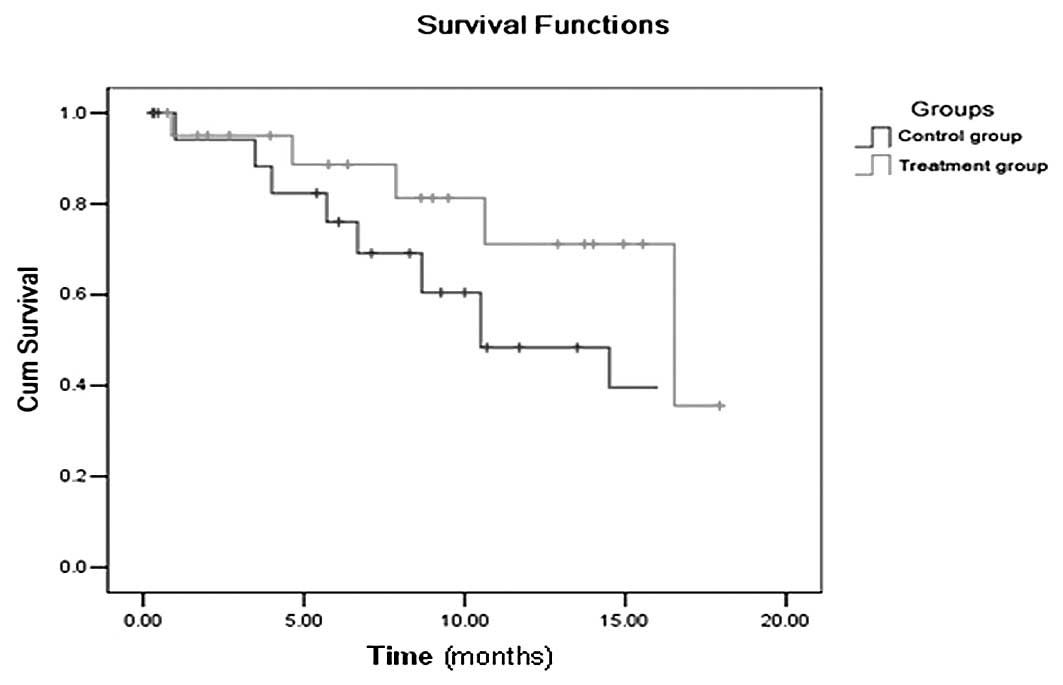
Mean survival times of the treatment and control
groups were 14.3 and 10.4 months, respectively. Median survival
times of the treatment and control groups were 16.5 and 10.5
months, respectively. The 1-year survival rates of the treatment
and control groups were 81.3 and 69.1%, respectively. Mean and
median survival times of the treatment group were longer than those
of control group, and the 1-year survival rate of the treatment
group was higher than that of the control group. There was no
significant differences between the treatment and control groups
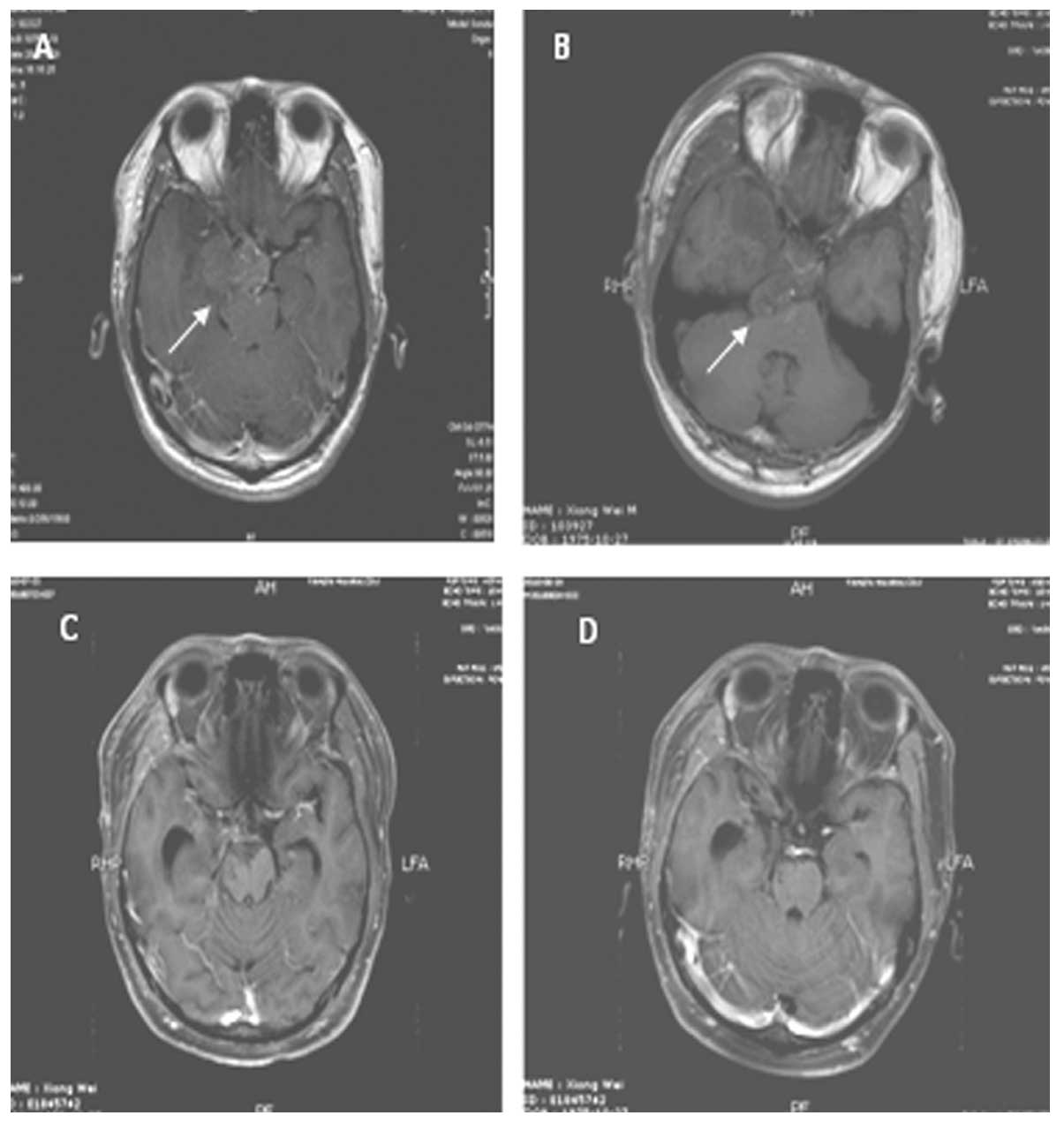
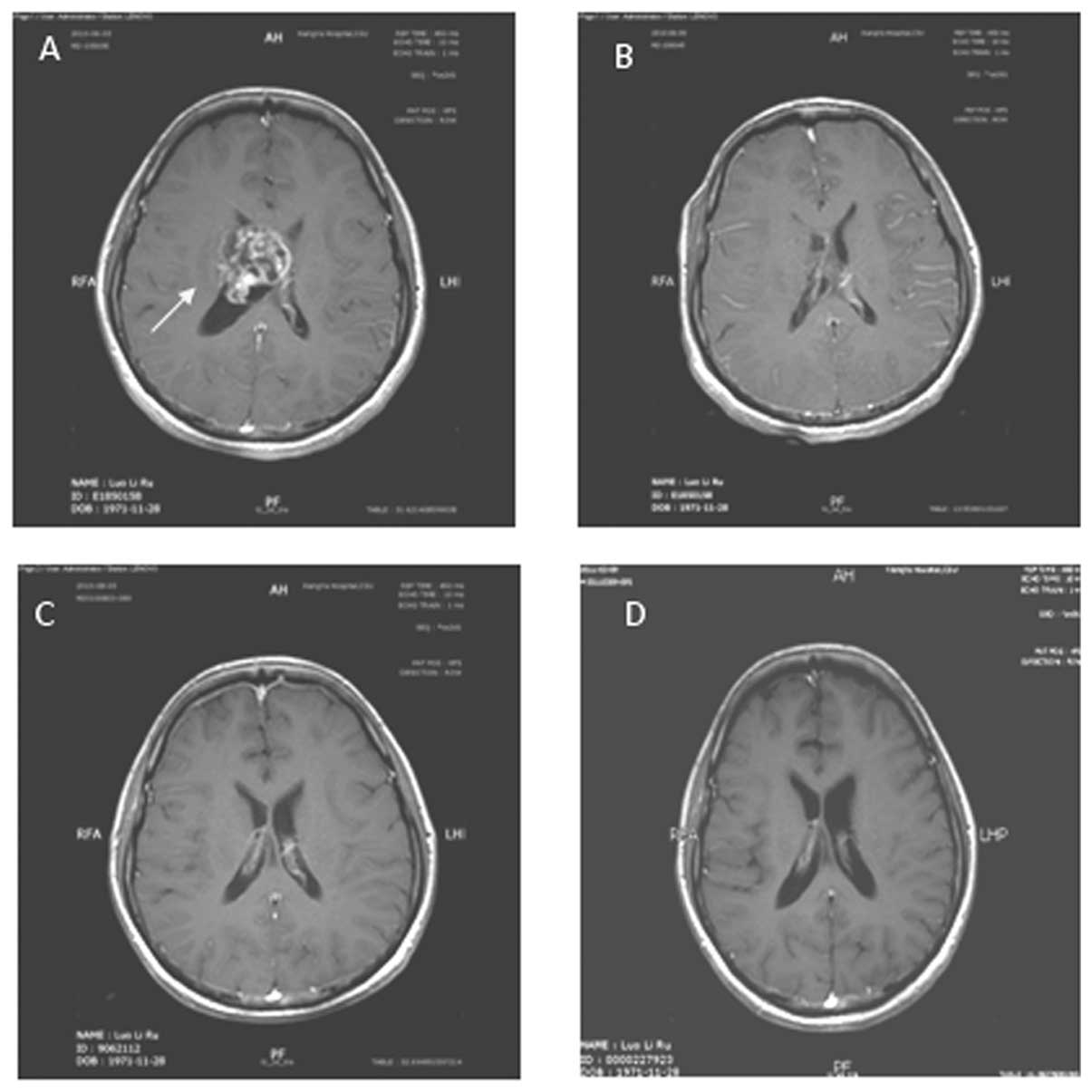
(P=0.094, Fig. 1). The
gadolinium-enhanced T1-weighted MR images of representative
patients are shown in Fig.
2–5.
Objective response rate of patients in
the treatment and control groups
Objective response rates of the treatment and
control groups were 70.0 and 52.4%, respectively, and the
difference between the treatment group and control group was not
statistically significant (P=0.248, Table II).
| Table II.Objective response rate of patients
in treatment and control groups. |
Table II.
Objective response rate of patients
in treatment and control groups.
| Group | CR | PR | SD | PD | RR (%) |
|---|
| Treatment | 3 | 11 | 4 | 2 | 70.0 |
| Control | 2 | 9 | 7 | 3 | 52.4 |
Discussion
Malignant gliomas are aggressive and incurable brain
tumors, and the aim of treatment is to increase survival while
improving quality of life. Median survival is approximately one
year for patients with grade IV tumors and 2–3 years for those with
grade III tumors. More than 80% of high-grade gliomas recur within
2–3 cm of the margin of the original tumor following surgery
(19). Recurrence can be defined
clinically or radiologically, based on patients presenting with
certain progressive symptoms (20).
The benefit of radiotherapy for malignant gliomas
has been demonstrated. A postoperative 6-week course of external
beam radiotherapy using linear accelerators is recommended as
standard treatment (11). A
systematic review of radiotherapy showed a 3–4-month survival
advantage for postoperative radiotherapy compared with supportive
care or chemotherapy (21).
However, the outcome of simple postoperative radiotherapy in
malignant gliomas is poor.
TMZ has been used for malignant gliomas. It has the
advantage of being administered orally, has marked BBB penetration
and may have low toxicity. TMZ
(8-carbamoyl-3-methylimidazo[5,1-d]-1,2,3,5-tetrazin-4
(3H)-1) is an oral prodrug, i.e., it is converted within the
body into an active agent. In the case of TMZ, the substance
produced is monomethyl triazenoimidazole carboxamide (MTIC). The
effect of MTIC is believed to be the methylation of DNA in a manner
that prevents the proliferation of tumor cells (12). It has been suggested that patients
with reduced MGMT activity may derive particular benefit from TMZ,
as their DNA is less capable of repairing the cytotoxic damage
inflicted by the drug, thus preserving its effect (22–24).
Surgery followed by RT with concomitant TMZ as a standard regimen
has been used for malignant gliomas.
Nimotuzumab is a humanized anti-epidermal growth
factor receptor (EGFR) monoclonal antibody (mAb) obtained by
complementarity determining region grafting of a murine mAb to a
human framework. Nimotuzumab binds to domain III of the
extracellular region of the EGFR. Studies have shown that
nimotuzumab mediates anti-tumor effects due to its capacity to
inhibit proliferation, survival and angiogenesis and to induce
apoptosis to cause antibody-dependent cell-mediated cytotoxicity
and complement-dependent cytotoxicity (25). Malignant gliomas have been found to
overexpress EGFR and to amplify the EGFR gene (26–28).
EGFR has been associated with high malignant degree and poor
outcomes in malignant gliomas. The BBB prevents certain
chemotherapy drugs and large molecular substances from penetrating
the brain tissue, and surgery, radiotherapy and the tumor itself
disrupt BBB integrity (29–31).
Radioimmunoscintigraphy with 99mTc-labelled nimotuzumab exhibits a
high sensitivity, specificity and accuracy in in vivo
detection of gliomas in patients (32). In a clinical trial involving
high-grade gliomas treated with nimotuzumab combined with
radiotherapy, radioimmunoscintigraphy with 99mTc-labelled
nimotuzumab showed patients achieving CR according to standard
imaging methods and no murine anti-EGFR antibody uptake, whereas
patients showing PR, SD or PD exhibited positive uptake of the
murine anti-EGFR antibody in the known tumor areas (33). The above study indicated that
nimotuzumab was capable of penetrating the BBB when it was
disrupted by surgery, radiotherapy and/or the tumor itself, and of
combining with EGFR to a certain extent and inhibiting its
biological function. EGFR expression has been correlated with
alterations in cell cycle progression (34), promotion of cell proliferation,
enhancement of angiogenesis (35,36),
promotion of DNA radiation damage repair and decrease in apoptosis
of tumor cells (37). When human
cancer cells are exposed to ionizing radiation, the epidermal
growth factor receptor (EGFR) is activated. This in turn mediates a
cytoprotective response that reduces the sensitivity of the cells
to ionizing radiation (38–40).
Our study revealed that the mean and median survival
times of the patients with malignant gliomas were longer in those
patients treated with nimotuzumab-combined radiochemotherapy.
However, mean and median survival time and the one-year survival
rate exhibited no significant difference between the treatment and
control groups. The objective response rate between the treatment
and control groups also exhibited no significant difference. We
postulate that the sample size enrolled in our study was too small
to detect any statistically significant difference in median
survival time or objective response rate between the treatment and
control groups. Although the patient numbers were small, there was
a trend towards survival benefit with nimotuzumab and
radiochemotherapy.
We hypothesize that the mechanism by which
nimotuzumab enhances sensitivity of malignant gliomas to
radiotherapy is the inhibition of proliferation and induction of
apoptosis in malignant glioma cells. Diaz et al reported
that exposure to nimotuzumab can inhibit proliferation and induce
apoptosis in U87MG brain tumors, and observed enhancement of
radiosensitivity of these tumors (41). Furthermore, certain studies have
shown that anti-EGFR mAb inhibits angiogensis, downregulates
vascular endothelial growth factor (VEGF) expression and enhances
the radiosensitivity of tumor cells (35,42,43).
Anti-EGFR mAb also mediates radiosensitivity through DNA repair
pathways. Anti-EGFR mAb triggered a specific physical interaction
between internalized EGFR and DNA protein kinase (DNA-PK) in the
cytosol, significantly reduced the level of DNA-PK in the nucleus
and raised the level of DNA-PK in the cytosol. DNA-PK in the
nucleus repairs double-strand DNA breakage, therefore it is
proposed that anti-EGFR mAb-induced reduction of the DNA-PK in the
nucleus sensitized the tumors to radiotherapy (44,45).
The capacity of anti-EGFR mAb to modulate tumor cell-cycle phase
distribution may play an important role in enhancement of
radiosensitivity. Anti-EGFR mAb may enhance radiosensitivity by
inducing accumulation of cells in the more radiosensitive cell
cycle G1 and G2/M phases and reducing the size of the
radioresistant S-phase fraction (46–48).
Acknowledgements
This work was supported by Hunan
Province Development and Reform Committee Science Research Fund
(2010-1060), Hunan Province Science and Technology Program
(2011SK3223), the Project of New Clinic Techniques of Central South
University, China and the National Natural Scientific Foundation of
China (Nos. 30670990, 30871189 and 81071718).
References
|
1
|
Counsell CE and Grant R: Incidence studies
of primary and secondary intracranial tumors: a systematic review
of their methodology and results. J Neurooncol. 37:241–250. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nazzaro JM and Neuwelt EA: The role of
surgery in the management of supratentorial intermediate and
high-grade astrocytomas in adults. J Neurosurg. 73:331–344. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wood JR, Green SB and Shapiro WR: The
prognostic importance of tumor size in malignant gliomas: a
computed tomographic scan study by the Brain Tumor Cooperative
Group. J Clin Oncol. 6:338–343. 1988.PubMed/NCBI
|
|
4
|
Albert FK, Forsting M, Sartor K, Adams HP
and Kunze S: Early postoperative magnetic resonance imaging after
resection of malignant glioma: objective evaluation of residual
tumor and its influence on regrowth and prognosis. Neurosurgery.
34:45–61. 1994. View Article : Google Scholar
|
|
5
|
Devaux BC, O’Fallon JR and Kelly PJ:
Resection, biopsy, and survival in malignant glial neoplasms. A
retrospective study of clinical parameters, therapy, and outcome. J
Neurosurg. 78:767–775. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Curran WJ Jr, Scott CB, Horton J, et al:
Does extent of surgery influence outcome for astrocytoma with
atypical or anaplastic foci (AAF)? A report from three Radiation
Therapy Oncology Group (RTOG) trials. J Neurooncol. 12:219–227.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Walker MD, Alexander E Jr, Hun WE, et al:
Evaluation of BCNU and/or radiotherapy in the treatment of
anaplastic gliomas. A cooperative clinical trial. J Neurosurg.
49:333–343. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Walker MD, Strike TA and Sheline GE: An
analysis of dose-effect relationship in the radiotherapy of
malignant gliomas. Int J Radiat Oncol Biol Phys. 5:1725–1731. 1979.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Andersen AP: Postoperative irradiation of
glioblastomas. Results in a randomized series. Acta Radiol Oncol
Radiat Phys Biol. 17:475–484. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kristiansen K, Hagen S, Kollevold T, et
al: Combined modality therapy of operated astrocytomas grade III
and IV. Confirmation of the value of postoperative irradiation and
lack of potentiation of bleomycin on survival time: a prospective
multicenter trial of the Scandinavian Glioblastoma Study Group.
Cancer. 47:649–652. 1981. View Article : Google Scholar
|
|
11
|
Laperriere N, Zuraw L and Cairncross G:
Radiotherapy for newly diagnosed malignant glioma in adults: a
systematic review. Radiother Oncol. 64:259–273. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Friedman HS, Kerby T and Calvert H:
Temozolomide and treatment of malignant glioma. Clin Cancer Res.
6:2585–2597. 2000.PubMed/NCBI
|
|
13
|
Watkins JM, Marshall DT, Patel S, et al:
High-dose radiotherapy to 78 Gy with or without temozolomide for
high grade gliomas. J Neurooncol. 93:343–348. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Stupp R, Hegi ME, Mason WP, et al: Effects
of radiotherapy with concomitant and adjuvant temozolomide versus
radiotherapy alone on survival in glioblastoma in a randomised
phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet
Oncol. 10:459–466. 2009.
|
|
15
|
Crombet T, Osorio M, Cruz T, et al: Use of
the humanized anti-epidermal growth factor receptor monoclonal
antibody h-R3 in combination with radiotherapy in the treatment of
locally advanced head and neck cancer patients. J Clin Oncol.
22:1646–1654. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rodriguez MO, Rivero TC, del Castillo Bahi
R, et al: Nimotuzumab plus radiotherapy for unresectable
squamous-cell carcinoma of the head and neck. Cancer Biol Ther.
9:343–349. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
World Health Organization Classification
of Tumours. Pathology and genetics of tumours of the central
nervous system. World Health Organization, IARC Press; Lyon:
2000
|
|
18
|
Eisenhauer EA, Therasse P, Bogaerts J, et
al: New response evaluation criteria in solid tumours: revised
RECIST guideline (version 1.1). Eur J Cancer. 45:228–247. 2009.
View Article : Google Scholar
|
|
19
|
Behin A, Hoang-Xuan K, Carpentier AF and
Delattre JY: Primary brain tumours in adults. Lancet. 361:323–331.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Macdonald DR, Cascino TL, Schold SC Jr and
Cairncross JG: Response criteria for phase II studies of
supratentorial malignant glioma. J Clin Oncol. 8:1277–1280.
1990.PubMed/NCBI
|
|
21
|
Berg G, Blomquist E and Cavallin-Stahl E:
A systematic overview of radiation therapy effects in brain
tumours. Acta Oncol. 42:582–588. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hegi ME, Diserens AC, Godard S, et al:
Clinical trial substantiates the predictive value of
O-6-methylguanine-DNA methyltransferase promoter methylation in
glioblastoma patients treated with temozolomide. Clin Cancer Res.
10:1871–1874. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Paz MF, Yaya-Tur R, Rojas-Marcos I, et al:
CpG island hypermethylation of the DNA repair enzyme
methyltransferase predicts response to temozolomide in primary
gliomas. Clin Cancer Res. 10:4933–4938. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hegi ME, Diserens AC, Gorlia T, et al:
MGMT gene silencing and benefit from temozolomide in glioblastoma.
N Engl J Med. 352:997–1003. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Diaz MA, Blanco R, Garcia B, et al:
Biological activity in vitro of anti-epidermal growth factor
receptor monoclonal antibodies with different affinities. Hybridoma
(Larchmt). 26:423–431. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ekstrand AJ, James CD, Cavenee WK, Seliger
B, Pettersson RF and Collins VP: Genes for epidermal growth factor
receptor, transforming growth factor alpha, and epidermal growth
factor and their expression in human gliomas in vivo. Cancer Res.
51:2164–2172. 1991.PubMed/NCBI
|
|
27
|
Bredel M, Pollack IF, Hamilton RL and
James CD: Epidermal growth factor receptor expression and gene
amplification in high-grade non-brainstem gliomas of childhood.
Clin Cancer Res. 5:1786–1792. 1999.PubMed/NCBI
|
|
28
|
Larysz D, Kula D, Kowal M, et al:
Epidermal growth factor receptor gene expression in high grade
gliomas. Folia Neuropathol. 49:28–38. 2011.PubMed/NCBI
|
|
29
|
Qin D, Ou G, Mo H, et al: Improved
efficacy of chemotherapy for glioblastoma by radiation-induced
opening of blood-brain barrier: clinical results. Int J Radiat
Oncol Biol Phys. 51:959–962. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Van Vulpen M, Kal HB, Taphoorn MJ and
El-Sharouni SY: Changes in blood-brain barrier permeability induced
by radiotherapy: Implications for timing of chemotherapy? (Review).
Oncol Rep. 9:683–688. 2002.PubMed/NCBI
|
|
31
|
Cao Y, Tsien CI, Shen Z, et al: Use of
magnetic resonance imaging to assess blood-brain/blood-glioma
barrier opening during conformal radiotherapy. J Clin Oncol.
23:4127–4136. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ramos-Suzarte M, Rodriguez N, Oliva JP, et
al: 99mTc-labeled antihuman epidermal growth factor receptor
antibody in patients with tumors of epithelial origin: Part III.
Clinical trials safety and diagnostic efficacy. J Nucl Med.
40:768–775. 1999.
|
|
33
|
Ramos TC, Figueredo J, Catala M, et al:
Treatment of high-grade glioma patients with the humanized
anti-epidermal growth factor receptor (EGFR) antibody h-R3: report
from a phase I/II trial. Cancer Biol Ther. 5:375–379. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Giordano A, Rustum YM and Wenner CE: Cell
cycle: molecular targets for diagnosis and therapy: tumor
suppressor genes and cell cycle progression in cancer. J Cell
Biochem. 70:1–7. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Petit AM, Rak J, Hung MC, et al:
Neutralizing antibodies against epidermal growth factor and
ErbB-2/neu receptor tyrosine kinases down-regulate vascular
endothelial growth factor production by tumor cells in vitro and in
vivo: angiogenic implications for signal transduction therapy of
solid tumors. Am J Pathol. 151:1523–1530. 1997.
|
|
36
|
Kerbel RS, Viloria-Petit A, Okada F and
Rak J: Establishing a link between oncogenes and tumor
angiogenesis. Mol Med. 4:286–295. 1998.PubMed/NCBI
|
|
37
|
Gibson S, Tu S, Oyer R, Anderson SM and
Johnson GL: Epidermal growth factor protects epithelial cells
against Fas-induced apoptosis. Requirement for Akt activation. J
Biol Chem. 274:17612–17618. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Lammering G, Hewit TH, Hawkins WT, et al:
Epidermal growth factor receptor as a genetic therapy target for
carcinoma cell radiosensitization. J Natl Cancer Inst. 93:921–929.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Lammering G: Anti-epidermal growth factor
receptor strategies to enhance radiation action. Curr Med Chem
Anticancer Agents. 3:327–333. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Damiano V, Melisi D, Bianco C, et al:
Cooperative antitumor effect of multitargeted kinase inhibitor
ZD6474 and ionizing radiation in glioblastoma. Clin Cancer Res.
11:5639–5644. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Diaz MA, Rolff J, Lemm M, Fichtner I,
Perez R and Montero E: Radiosensitisation of U87MG brain tumours by
anti-epidermal growth factor receptor monoclonal antibodies. Br J
Cancer. 100:950–958. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Gorski DH, Beckett MA, Jaskowiak NT, et
al: Blockage of the vascular endothelial growth factor stress
response increases the antitumor effects of ionizing radiation.
Cancer Res. 59:3374–3378. 1999.PubMed/NCBI
|
|
43
|
Perrotte P, Matsumoto T, Inoue K, et al:
Anti-epidermal growth factor receptor antibody C225 inhibits
angiogenesis in human transitional cell carcinoma growing
orthotopically in nude mice. Clin Cancer Res. 5:257–265.
1999.PubMed/NCBI
|
|
44
|
Coleman CN and Stevenson MA: Biologic
basis for radiation oncology. Oncology (Williston Park).
10:399–415. 1996.
|
|
45
|
Bandyopadhyay D, Mandal M, Adam L,
Mendelsohn J and Kumar R: Physical interaction between epidermal
growth factor receptor and DNA-dependent protein kinase in
mammalian cells. J Biol Chem. 273:1568–1573. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kwok TT and Sutherland RM: Cell cycle
dependence of epidermal growth factor induced radiosensitization.
Int J Radiat Oncol Biol Phys. 22:525–527. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Laderoute KR, Ausserer WA, Knapp AM, Grant
TD and Sutherland RM: Epidermal growth factor modifies cell cycle
control in A431 human squamous carcinoma cells damaged by ionizing
radiation. Cancer Res. 54:1407–1411. 1994.PubMed/NCBI
|
|
48
|
Huang SM and Harari PM: Modulation of
radiation response after epidermal growth factor receptor blockade
in squamous cell carcinomas: inhibition of damage repair, cell
cycle kinetics, and tumor angiogenesis. Clin Cancer Res.
6:2166–2174. 2000.
|