Introduction
Intravesical bacillus Calmette-Guérin (BCG)
immunotherapy is considered more effective than intravesical
chemotherapy and is advocated as the first treatment choice in
patients with carcinoma in situ or with pT1G3 (1). However, not all patients benefit from
intravesical BCG (2). In fact,
30–50% of patients undergoing intravesical BCG treatment have
recurring tumours following therapy (3–5),
with common side-effects that can be life threatening (6). Patients refractory to BCG therapy are
subjected to salvage cystectomy as standard treatment (2), though may show a poor prognosis
(7). Therefore, the patient
failing BCG therapy is a challenge to the urologist and predictors
of BCG response should be investigated (2). Although several authors have proposed
molecular markers to predict the clinical outcome of patients with
non-muscle invasive bladder cancer (NMIBC) following treatment with
intravesical BCG (8–9), no marker has yet proven to be valid
in everyday clinical practice (2).
Zhang et al demonstrated the induction of cytokine
production by BCG, particularly interleukin-6 (IL-6) (10). Recently, Luo et al showed
the inhibitory role of interleukin-10 (IL-10) in BCG-induced
macrophage cytotoxicity, suggesting that the blockage of IL-10 may
potentially enhance the effect of BCG in the treatment of bladder
cancer patients (11). Chen et
al demonstrated that BCG increases IL-6 messenger RNA and
protein in a time-and dose-dependent manner via an immediate early
pathway (12). Furthermore, we
highlighted the feasible role of IL-6 and IL-10 ratio (IL-6/IL-10)
as a prognostic marker of recurrence in patients affected by NMIBC
(9). Urinary interleukins could
consequently be used as prognosticators to better assess the
outcome of NMIBC patients following BCG therapy. The present study
aimed to evaluate the role of IL-6/IL-10 in predicting patient
response to BCG therapy.
Materials and methods
Study design
To evaluate the prognostic role of urinary
IL-6/IL-10, all consecutive patients who had undergone
transurethral resection of bladder tumours (TUR-BT) at the same
urological unit (Department of Urology, University of Florence,
Florence, Italy) between January 2005 and May 2006 were selected
for this prospective study. As controls, 49 subjects were enrolled
from among patients attending the clinic in the same period for
other non-malignant urological diseases. Since this study was
designed to establish the role of IL-6/IL-10 as a predictor of the
response to BCG and not as a diagnostic tool, patients with other
urological malignant diseases were excluded. Outcome measures were
time to first recurrence following treatment and recurrence rate.
Disease progression was not included among the main outcomes due to
the small number of patients who experienced stage or grade
progression, though these data are reported in Results. Response to
BCG was confirmed by negative urinary cytology and cystoscopy after
6 months’ follow-up (13).
According to Herr and Dalbagni, patients were defined as
BCG-refractory if the recurrence occurred within 6 months of
starting BCG treatment (14).
Urine samples for the urine dipstick test and interleukin analyses
were collected before TUR-BT and 6 subsequent weekly BCG
instillations. Depending on laboratory results, all patients
enrolled in the study were divided into 2 groups: group A with
IL-6/IL-10 ≤0.09 and group B with IL-6/IL-10 >0.10. The controls
constituted group C. Follow-up data were compared and analysed.
Patients with no further information available at follow-up were
excluded from the study. The local research ethics committee
approved the study and written informed consent was obtained from
all patients.
Eligibility for the study
Inclusion criteria were the presence of
cystoscopically demonstrated bladder tumours, normal pre-operative
blood tests and compliance with instillation and follow-up
schedules. We enrolled only patients affected by high-risk NMIBC,
according to the European Association of Urology Guidelines
criteria (13). Exclusion criteria
were evidence of locally infiltrative or metastatic bladder tumours
(pT ≥2), presence of upper urinary tract tumours, lesions that
could not be completely removed transurethrally and presence of
other neoplastic, lower urinary tract or major concomitant
diseases. Patients who had undergone surgery for benign prostatic
obstruction at the same time as surgical treatment for NMIBC were
also excluded, along with patients with histologically documented
urothelial carcinoma in situ. Only those with a tumour
recurrence of the same stage and grade of the initial tumour at
diagnosis were enrolled. We enrolled only patients with recurrent
urothelial cancer in order to obtain a homogeneous group for
analysis. Patients with histologically confirmed pT1G3 were
excluded, since management decisions in these patients are critical
(15). A recurrent bladder tumour
within 3 months of receiving TUR-BT was also a criterion for
exclusion. Patients who had previously received intravesical
treatment were included, provided this treatment had been
administered >6 months before TUR-BT. No patient underwent early
single intravesical instillation, as suggested by Cai et al
(16).
Treatment plan
At least 21 days after TUR-BT, all patients
underwent weekly BCG instillations for 6 weeks (5×108
colony-forming units in 50 ml saline; OncoTice® BCG,
Organon USA Inc.). In accordance with Lamm et al (17), boosters of BCG were given at 3, 6,
12, 18, 24, 30 and 36 months. This protocol schedule is the current
standard treatment for NMIBC (13). All patients were instructed to
retain the drug solution in the bladder for 1 h.
Sample collection and storage
Urine samples were collected from each subject by
using a clean catch. A spontaneous morning void urine sample was
collected by the patients before TUR-BT and by the controls on
enrolment. The urine sample was collected from each subject in
order to obtain a basal IL-6 and IL-10 mean value. All samples were
stored in aliquots at −80°C until analysis after testing for the
presence of inflammatory cells or bacteriuria by using urine
dipstick test for nitrites and leukocyte esterase (Multistik
Pro®), as shown by Cai et al (18–19).
A positive test result was indicative of urinary tract
infection.
Interleukin measurements
At the time of the analysis, urine aliquots were
defrosted and centrifuged for 10 min at 800 rpm and the urinary
IL-6 and IL-10 levels were measured in the supernatants. Natural
human-produced IL-6 and IL-10 concentrations were determined in the
urine of all patients and controls by solid phase ELISA Quantikine
IL-6 Immunoassay and IL-10 Immunoassay, respectively (R&D
Systems, Minneapolis, MN, USA). All samples were measured in
duplicate in accordance with the manufacturer’s recommendations
(www.rndsystems.com/productdetailobjectnameQuantikine.aspx).
The median minimal detectable dose of the IL-6 assay was 0.70 pg/ml
and 3.9 pg/ml for IL-10. Values were considered normal if under the
lowest IL-6 and IL-10 standards, 3.12 pg/ml and 7.8 pg/ml,
respectively. All samples were tested in duplicate by using
independent analysis to avoid errors.
IL-6/IL-10
The IL-6 to IL-10 ratio was calculated as a fraction
between urinary IL-6 and IL-10 values, expressed as a number or
fraction ranging from 0 to 1. The cut-off value was determined
according to Cai et al (9).
Histopathology
Tumour stage and grade were classified following the
1998 WHO classification and the 2002 TNM classification of
malignant tumours, as defined by the International Union Against
Cancer. A single genito-urinary pathologist performed the
pathological evaluation.
Patient follow-up
Each patient underwent urinary cytology,
ultrasonography and cystoscopy every 3 months for the first 12
months following TUR and then every 6 months. Recurrence was
determined by papillary formations protruding into the bladder
lumen and detected on cystoscopy, or by the presence of neoplastic
tissue diagnosed following vesical biopsy. Every recurrence was
pathologically confirmed. Time to the first recurrence was defined
as the time from randomisation to the date of the first recurrence.
Progression was defined as an increase in tumour stage or grade
(13).
Statistical analysis
As the null hypothesis, we assumed that there was no
difference among the groups in terms of recurrence-free time or
recurrence rate and that the IL-6/IL-10 had no impact on predicting
the response to BCG therapy. The Fisher’s exact test and the
Chi-square χ2 test were used to assess the significance
of all parameters, and p<0.05 was considered to indicate a
statistically significant difference. Kaplan-Meier survival curves
and the log-rank test were also used to evaluate survival in NMIBC
cases. The 95% confidence intervals (CI) were calculated for the
probability of survival for Kaplan-Meier estimates. The
Mann-Whitney test was also used to compare different parameter
means. Univariate and multivariate relative risk was calculated by
using Cox’s proportional hazards regression. Statistical analysis
was performed using StatPlus for Apple Macintosh (Analyst Soft,
2001–2009).
Results
Among 196 consecutive patients undergoing TUR-BT, 81
were enrolled, of which 72 were found to be eligible for the
present study. This trial ultimately included 72 patients and 49
controls. Patient characteristics, clinical and laboratory data are
described in Table I.
 | Table ISummary of clinical and pathological
patient and control data. |
Table I
Summary of clinical and pathological
patient and control data.
| A, Patient and
control characteristics |
|
| No. of patients | 72 |
| No. of controls | 49 |
| Median patient age
(range) | 71.3 (52–79) |
| Median control age
(range) | 68.7 (57–75) |
| Gender
(patients) | |
| Male | 70 (97.2) |
| Female | 2 (2.8) |
| Gender
(controls) | |
| Male | 49 (100.0) |
| Female | 0 (0.0) |
|
| B, Patient
anamnestic, pathological and clinical data |
|
| Number of
recurrences/year | |
| 1 | 8 (11.1) |
| 2 | 15 (20.9) |
| ≥3 | 49 (68.0) |
| Number of
lesions | |
| 1 | 11 (15.2) |
| 2 | 25 (34.7) |
| ≥3 | 36 (50.1) |
| Diameter of lesion
(if multiple, diameter of the largest) | |
| <3 cm | 44 (61.1) |
| ≥3 cm | 28 (38.9) |
| Stage | |
| pTa | 49 (68.0) |
| pT1 | 23 (32.0) |
| Grade | |
| G1 | 8 (11.1) |
| G2 | 26 (36.2) |
| G3 | 38 (52.7) |
| Previous
intravesical therapy | |
| No treatment | 11 (15.2) |
| BCG | 25 (34.7) |
|
Chemotherapya | 36 (50.1) |
|
| C, Control clinical
data |
|
| Urological
diseases | |
| TUR-P | 49 (100) |
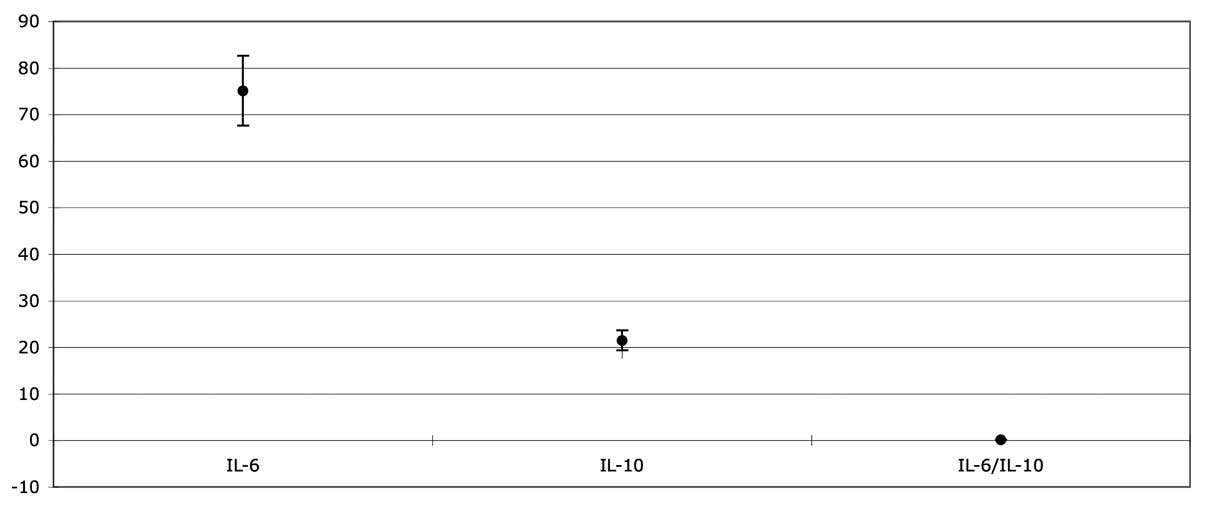
Results at enrolment
No patient tested positive in the urine dipstick
test. IL-6 and IL-10 were 74.13 pg/ml (22.84 ± SD) and 196.28 pg/ml
(36.59 ± SD), respectively, among the patients, while IL-6 and
IL-10 were 3.11 pg/ml (1.13 ± SD) and 5.78 pg/ml (2.17 ± SD),
respectively, in the control group. The IL-6/IL-10 mean value was
0.13 (0.13 ± SD) among the patients (Fig. 1). At the baseline, 38 out of 72
(52.7%) patients showed an IL-6/IL-10 of ≤0.09 while 34 (47.3%)
showed an IL-6/IL-10 of >0.10. The IL-6/IL-10 ratio was not
calculated in the control group. All patients were then split into
2 groups: 38 patients to group A (IL-6/IL-10 ≤0.09) and 34 to group
B (IL-6/IL-10 >0.10). In group A the IL-6/IL-10 mean value was
0.05 (0.01 ± SD) while in group B it was 0.17 (0.11 ± SD).
Follow-up results
All patients correctly underwent BCG intravesical
therapy. Nineteen patients had mild adverse effects, which did not
require treatment suspension and which were cured with antibiotic
and anti-inflammatory drugs. At the end of the follow-up period
(mean, 53.7 months; ranging from 49 to 58 months), all patients
were alive, 39 (54.1%) without recurrence, while 33 (45.9%) had at
least one recurrence. Three patients showed progression in stage
and/or grade: 2 pTaG2 to pT1G3 (time to progression, 8 months) and
1 pTaG1 to pT1G3.
Results according to the groups
Group A (IL-6/IL-10 ≤0.09). Among patients
with IL-6/ IL-10 ≤0.09, 23 out of 38 (60.5%) showed at least one
recurrence (mean, 6.2 months; ranging from 3 to 16 months), while
15 (39.5%) experienced no recurrence (mean, 13.1 months; ranging
from 11 to 16 months). Among the patients with at least one
recurrence at follow-up, 2 patients showed progression in stage and
grade (2 pTaG2 to pT1G3).
Group B (IL-6/IL-10 >0.10). Among patients
with IL-6/ IL-10 >0.10, 10 out of 34 (29.4%) showed at least one
recurrence (mean, 12.3 months; ranging from 10 to 14 months) while
24 (70.6%) had no recurrence (mean, 16.1 months’ ranging 11 from to
17 months). Among the patients with at least one recurrence at
follow-up, one patient showed grade progression (1 pT1G1 to pT1G3).
All follow-up data pertaining to the groups are detailed in
Table II.
| Table IIFollow-up results according to
IL-6/IL-10 value. |
Table II
Follow-up results according to
IL-6/IL-10 value.
| Group | IL-6/IL-10 | Status at follow-up
| Total |
|---|
| VNED | VREC with
progression | VREC without
progression |
|---|
| A | ≤0.09 | 15 | 2 | 21 | 38 |
| B | >0.10 | 24 | 1 | 9 | 34 |
| Total | | 39 | 3 | 30 | 72 |
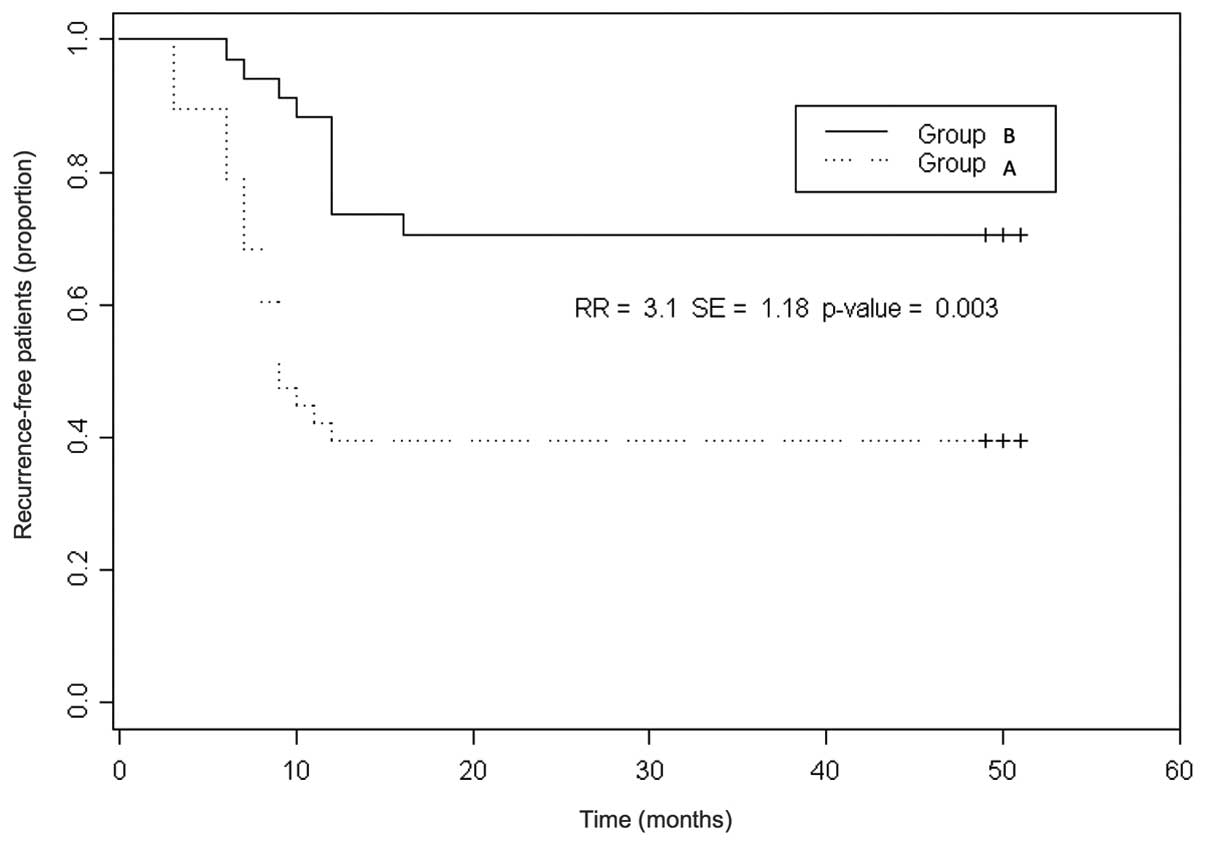
Statistical difference between
IL-6/IL-10, other clinical or pathological factors and follow-up
results
No correlation between anamnestic or pathological
factors and the IL-6/IL-10 value was reported. A statistically
significant difference between the IL-6/IL-10 value and the
response to BCG therapy (as status at follow-up) was found
(p=0.016, df=1, χ2=5.800). The Kaplan-Meier analysis
demonstrated a significant difference in terms of response to BCG
between the 2 groups [p=0.003; recurrence rate (RR)=3.1; standard
error (SE)=1.18] (Fig. 2).
Univariate and multivariate
analysis
No clinical or anamnestic parameter had any
significant impact on BCG response, as shown by univariate
analysis. At multivariate analysis, the IL-6/IL-10 value (p=0.002)
[IL-6/IL-10 value; hazard ratio (HR), 4.09; 95% CI, 2.59–6.28] and
number of lesions (p=0.03) (3 lesions; HR, 3.31; 95% CI, 1.38–3.35)
were identified as independent prognostic factors of BCG response
probability (Table III).
| Table IIIMultivariate analysis results of
factors affecting recurrence risk in all enrolled patients. |
Table III
Multivariate analysis results of
factors affecting recurrence risk in all enrolled patients.
| Categories
(variables) | No. of
recurrence-free patients/Total no. of patients (%) | Multivariate
analysis HR (95% CI) (p) |
|---|
| Age | | 0.74 |
| <65 years | 23/42 (54.7) | 0.77
(0.60–1.43) |
| ≥65 years | 16/30 (53.3) | 0.62
(0.15–1.16) |
| Gender | | 0.71 |
| Male | 38/70 (54.2) | 1.00
(0.18–1.55) |
| Female | 1/2 (50.0) | 1.21
(0.75–1.16) |
| Number of
recurrences/year | | 0.25 |
| 1 | 5/8 (62.5) | 0.99
(0.12–1.67) |
| 2 | 6/15 (40.0) | 0.74
(0.10–1.19) |
| ≥3 | 28/49 (57.1) | 1.15
(0.47–2.00) |
| Diameter of
lesions | | 0.89 |
| <3 cm | 29/44 (65.9) | 1.01
(0.15–1.23) |
| ≥3 cm | 10/28 (35.7) | 2.21
(2.10–3.02) |
| Grade | | 0.09 |
| G1 | 3/8 (37.5) | 0.97
(0.12–1.13) |
| G2 | 16/26 (61.5) | 1.10
(0.23–1.24) |
| G3 | 20/38 (52.6) | 1.99
(0.78–2.32) |
| Number of
lesions | | 0.03 |
| 1 | 10/11 (90.9) | 0.62
(0.24–1.08) |
| 2 | 13/25 (52.0) | 1.29
(0.61–1.99) |
| ≥3 | 16/36 (44.4) | 4.22
(2.62–3.95) |
| IL-6 levels | | 0.62 |
| Normal (≤3.12
pg/ml) | 21/37 (56.7) | 1.68
(1.50–2.87) |
| Abnormal | 18/35 (51.4) | 1.12
(0.20–2.12) |
| IL-10 levels | | 0.71 |
| Normal (≤7.8
pg/ml) | 16/21 (76.1) | 0.87
(0.74–1.09) |
| Abnormal | 23/51 (45.0) | 1.09
(0.19–1.20) |
| IL-6/IL-10 | | 0.002 |
| ≤0.09 | 15/38 (39.4) | 0.65
(0.29–1.19) |
| >0.10 | 24/34 (70.5) | 3.87
(2.81–4.98) |
Discussion
In his review on the management of BCG failures in
NMIBC patients, Witjes stated that the response to BCG therapy
cannot be accurately predicted on an individual basis (2). In previous years, however, several
molecular markers, such as urinary cytokines (20), p53 and pRb expression (6) and loss of heterozygosis on INF-α
locus (9), have been proposed as
prognosticators of BCG response, even if their clinical usefulness
remains to be proven (2). Cai
et al recently demonstrated that IL-6/IL-10 predicts the
risk of recurrence in NMIBC patients (9). In the present study, we have shown
that IL-6/IL-10 is an independent prognostic factor of BCG response
probability. The rationale of this approach is based on the fact
that IL-6 and IL-10 are cytokines overexpressed in bladder
carcinoma, and with a role in the interaction between cancer cells
and the evironment (21). IL-6 is
a multifunctional cytokine produced by cells in response to several
inflammatory conditions (22) and
has been recognised as a growth factor for the final maturation of
B cells and the differentiation of T cells (23). IL-6 is crucial in supporting
systemic host response to tissue injury (24). Mulé et al described the
anti-tumour effect of IL-6 on lung cancer in mice, confirming that
the induction of host immunological response is central in the
reaction to cancer (25).
Moreover, several studies have demonstrated that IL-10 has the
physiological role of downregulating cell-mediated immunity,
resulting in the improvement of tumour immune escape (26). Nadler et al reported that
IL-10 is an important modulator of immune-mediated events in
vivo and suggested that efforts to downmodulate this inhibitory
cytokine may be of therapeutic value (27). The theory that IL-6/IL-10 is a good
prognostic marker for use in clinical practice was based on the
following reasons: i) high levels of IL-10, with consequent
decrease in IL-6/IL-10, indicate tumour immunosuppression,
eliminating the ability of immunocompetent cells to respond to the
tumour (26); ii) IL-10 is known
to be a promoter of immune dysregulation, with the enhancement of
Th2 cells (27). Indeed, patients
with bladder cancer appear to develop a Th2 dominant status with a
deficient-type immune response due to an increase in IL-10 levels
(27). This immune dysregulation
should be proved by altered IL-6/IL-10; iii) the decrease in IL-6
levels and increase in IL-10 levels are evidence of an altered host
immune response to the tumour, confirmed by cell activation due to
BCG (26). The release of
immunosuppressive IL-10 during BCG therapy reduces inflammation and
anticancer response (28). In
addition, IL-6 and IL-10 are promoters of two different immune
response pathways, i.e. Th1 and Th2, and allow the evaluation of
host immunological response to the tumour (26,29).
The present study, even though conducive for a better understanding
of the correlation between urothelial bladder cancer cells and the
host immune system, had a number of limitations that should be
taken into account. First of all, the number of the patients
enrolled was small, even if a statistical significance was
obtained. Secondly, a group of patients undergoing alternative
intravesical therapies, i.e. mitomycin or epirubicin, was lacking.
Future studies are mandatory to confirm the present findings.
The current study highlights the role of IL-6/IL-10
in predicting the response to BCG therapy in NMIBC patients. We put
forward the feasibility and usefulness of IL-6/IL-10 as a clinical
marker, in association with traditional clinico-pathological
factors, in planning a more appropriate follow-up schedule for
NMIBC patients.
Acknowledgements
Special thanks to Professor John
Denton for manuscript language revision and to all members of the
Santa Maria Annunziata Hospital STDs Center, for their
excellent laboratory assistance.
References
|
1.
|
Sylvester RJ, van der Meijden AP,
Oosterlinck W, Witjes JA, Bouffioux C, Denis L, Newling DW and
Kurth K: Predicting recurrence and progression in individual
patients with stage Ta T1 bladder cancer using EORTC risk tables: a
combined analysis of 2596 patients from seven EORTC trials. Eur
Urol. 49:466–465. 2006. View Article : Google Scholar
|
|
2.
|
Witjes JA: Management of BCG failures in
superficial bladder cancer: a review. Eur Urol. 49:790–797. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Punnen SP, Chin JL and Jewett MA:
Management of bacillus Calmette-Guerin (BCG) refractory superficial
bladder cancer: results with intravesical BCG and Interferon
combination therapy. Can J Urol. 10:1790–1795. 2003.
|
|
4.
|
Kim JC and Steinberg GD: Medical
management of patients with refractory carcinoma in situ of the
bladder. Drugs Aging. 18:335–344. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Herr HW, Wartinger DD, Fair WR and Oettgen
HF: Bacillus Calmette-Guerin therapy for superficial bladder
cancer: a 10-year followup. J Urol. 147:1020–1023. 1992.PubMed/NCBI
|
|
6.
|
Esuvaranathan K, Chiong E, Thamboo TP,
Chan YH, Kamaraj R, Mahendran R and Teh M: Predictive value of p53
and pRb expression in superficial bladder cancer patients treated
with BCG and interferon-alpha. Cancer. 109:1097–1105. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Huguet J, Crego M, Sabate S, Salvador J,
Palou J and Villavicencio H: Cystectomy in patients with high risk
superficial bladder tumours who fail intravesical BCG therapy:
pre-cystectomy prostate involvement as a prognostic factor. Eur
Urol. 48:53–59. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Ahirwar D, Kesarwani P, Manchanda PK,
Mandhani A and Mittal RD: Anti- and proinflammatory cytokine gene
polymorphism and genetic predisposition: association with smoking,
tumor stage and grade, and bacillus Calmette-Guérin immunotherapy
in bladder cancer. Cancer Genet Cytogenet. 184:1–8. 2008.PubMed/NCBI
|
|
9.
|
Cai T, Nesi G, Dal Canto M, Tinacci G,
Mondaini N, Piazzini M, Geppetti P and Bartoletti R: Loss of
heterozygosis on IFN-alpha locus is a prognostic indicator of
bacillus Calmette-Guerin response for nonmuscle invasive bladder
cancer. J Urol. 183:1738–1743. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Zhang Y, Mahendran R, Yap LL,
Esuvaranathan K and Khoo HE: The signalling pathway for BCG-induced
interleukin-6 production in human bladder cancer cells. Biochem
Pharmacol. 63:273–282. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Luo Y, Han R, Evanoff DP and Chen X:
Interleukin-10 inhibits Mycobacterium bovis bacillus
Calmette-Guérin (BCG)-induced macrophage cytotoxicity against
bladder cancer cells. Clin Exp Immunol. 160:359–368. 2010.
|
|
12.
|
Chen FH, Crist SA, Zhang GJ, Iwamoto Y and
See WA: Interleukin-6 production by human bladder tumor cell lines
is up-regulated by bacillus Calmette-Guérin through nuclear
factor-kappaB and Ap-1 via an immediate early pathway. J Urol.
168:786–97. 2002.PubMed/NCBI
|
|
13.
|
Oosterlinck W, Lobel B, Jakse G, Malmström
P, Stöckle M and Sternberg C; European Association of Urology (EAU)
Working Group on Oncological Urology: Guidelines on bladder cancer.
Eur Urol. 41:105–112. 2002. View Article : Google Scholar
|
|
14.
|
Herr HW and Dalbagni G: Defining bacillus
Calmette-Guerin refractory superficial bladder tumors. J Urol.
169:1706–1708. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Thalmann GN, Markwalder R, Shahin O,
Burkhard FC, Hochreiter WW and Studer UE: Primary T1G3 bladder
cancer: organ preserving approach or immediate cystectomy? J Urol.
172:70–75. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Cai T, Nesi G, Tinacci G, Zini E, Mondaini
N, Boddi V, Mazzoli S and Bartoletti R: Can early single dose
instillation of epirubicin improve bacillus Calmette-Guerin
efficacy in patients with nonmuscle invasive high risk bladder
cancer? Results from a prospective, randomized, double-blind
controlled study. J Urol. 180:110–115. 2008. View Article : Google Scholar
|
|
17.
|
Lamm DL and Crawford ED, Blumenstein B,
Crismann JD, Montie JE, Gottesman JE, Lowe BA, Sarosdy MF, Bohl RD,
Grossman HB, Beck TM, Leimers JT and Crawford ED: Maintenance BCG
immunotherapy for recurrent Ta, T1 and Tis transitional cell
carcinoma of the bladder: a randomized prospective Southwest
Oncology Group study. J Urol. 163:1124–1129. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Cai T, Mazzoli S, Meacci F, Nesi G,
Geppetti P, Malossini G and Bartoletti R: Human papillomavirus and
non-muscle invasive urothelial bladder cancer: Potential
relationship from a pilot study. Oncol Rep. 25:485–489.
2011.PubMed/NCBI
|
|
19.
|
Cai T, Piazzini M, Nesi G, Taddei I, Sardi
I, Detti B, Mondaini N, Dal Canto M and Bartoletti R: E-cadherin
mRNA expression analysis in evaluating the natural history of
urothelial bladder cell carcinoma: Results from a long-term
follow-up study. Oncol Rep. 17:925–930. 2007.PubMed/NCBI
|
|
20.
|
Thalmann GN, Sermier A, Rentsch C, Mohrle
K, Cecchini MG and Studer UE: Urinary interleukin-8 and 18 predict
the response of superficial bladder cancer to intravesical therapy
with bacillus Calmette-Guerin. J Urol. 164:2129–2133. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Watanabe E, Matsuyama H, Matsuda K, Ohmi
C, Tei Y, Yoshihiro S, Ohmoto Y and Naito K: Urinary interleukin-2
may predict clinical outcome of intravesical bacillus
Calmette-Guerin immunotherapy for carcinoma in situ of the bladder.
Cancer Immunol Immunother. 52:481–486. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Barton BE: Interleukin-6 and new
strategies for the treatment of cancer, hyperproliferative diseases
and paraneoplastic syndromes. Expert Opin Ther Targets. 9:737–752.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Liang B, Gardner DB, Griswold DE, Bugelski
PJ and Song X: Anti-interleukin-6 monoclonal antibody inhibits
autoimmune responses in a murine model of systemic lupus
erythematosus. Immunology. 119:296–305. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Seguchi T, Yokokawa K, Sugao H, Nakano E,
Sonoda T and Okuyama A: Interleukin-6 activity in urine and serum
in patients with bladder carcinoma. J Urol. 148:791–794.
1992.PubMed/NCBI
|
|
25.
|
Mulé JJ, McIntosh JK, Jablons DM and
Rosenberg SA: Antitumor activity of recombinant interleukin 6 in
mice. J Exp Med. 171:629–636. 1990.
|
|
26.
|
Sabat R and Asadullah K: Interleukin-10 in
cancer immunity. Cancer Immune Therapy: Experiences and Future
Strategies. Stuhler G and Walden P: Wiley-VCH Verlag GmbH;
Weinheim, Germany: pp. 223–231. 2002
|
|
27.
|
Nadler R, Luo Y, Zhao W, Ritchey JK,
Austin JC, Cohen MB, O’Donnell MA and Ratliff TL: Interleukin 10
induced augmentation of delayed-type hypersensitivity (DTH)
enhances Mycobacterium bovis bacillus Calmette-Guérin (BCG)
mediated antitumour activity. Clin Exp Immunol. 131:206–216. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Agarwal A, Verma S, Burra U, Murthy NS,
Mohanty NK and Saxena S: Flow cytometric analysis of Th1 and Th2
cytokines in PBMCs as a parameter of immunological dysfunction in
patients of superficial transitional cell carcinoma of bladder.
Cancer Immunol Immunother. 55:734–743. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Suttmann H, Jacobsen M, Reiss K, Jocham D,
Bohle A and Brandau S: Mechanisms of bacillus Calmette-Guerin
mediated natural killer cell activation. J Urol. 172:1490–1495.
2004. View Article : Google Scholar : PubMed/NCBI
|