Introduction
Infantile hemangiomas (IHs) are the most common
benign tumors in infancy affecting 5–10% of the population, and are
largely composed of densely packed over-proliferating capillaries
with high cellular density and the absence of an open lumen. These
lesions are most prevalent in Caucasian children and are three
times more common in female infants than male. The head and neck
region is the most frequently involved area (60%), followed by the
trunk (25%) and the extremities (15%), and these tumors exhibit a
non-random distribution largely correlating with regions of
embryological fusion (1). IHs have
a predictable natural history, arising soon after birth to undergo
a significant proliferative phase during the first year of life,
followed by gradual involution over several years. Regression is
complete in 50% of 5-year-old patients and 90% of 9-year-old
patients. Because these tumors spontaneously regress and (for the
majority of lesions) produce no long-term scarring, most children
with IHs require no treatment. Despite their self-limiting course,
in approximately 10% of cases depending on their anatomical site
and/or size, there can be serious or life threatening complications
requiring immediate intervention. The classical approaches for
treating complicated IHs include the use of systemic or
intralesional corticosteroids, chemotherapeutic agents such as
vincristine, laser therapy, surgical resection or a combination of
these treatments. The recent serendipitous discovery of β blockers
as an effective therapy for IHs has revolutionized management of
IHs to become the current gold standard (2).
Propranolol, which is administered systemically in
pediatric patients with IHs, is a non-selective β-adrenergic
receptor antagonist that blocks the action of epinephrine and
norepinephrin. This drug has been shown to suppress angiogenesis
via inhibition of proliferation, migration, barrier function, and
induction of apoptosis in primary cultures of normal epithelial
cells (3–6). The molecular mechanism of action for
propranolol includes disrupting the epinephrine and norpinephrine
regulation of cyclic AMP production, actin cytoskeletal dynamics
and release of atherogenesis regulators (7–9).
Only recently have investigations into the precise roles of
propranolol in IHs revealed that this therapy blocks hemangioma
endothelial growth and this effect may be through suppressing the
production of nitric oxide and HIF1α regulation of vascular
endothelial growth factor (VEGF) expression (10,11).
Perplexingly, it is unknown how propranolol preferentially inhibits
the growth of IHs, while spares the formation of new blood vessels
necessary for growth and development of the infant. In this study,
we sought to further evaluate the molecular mechanisms by which
propranolol exerts its effects on human IH endothelial cells
(HemECs). Furthermore, we compared the biological response of
HemECs treated with propranolol to that of normal human endothelial
cells treated with propranolol. Our data indicate that propranolol
disrupts cell proliferation through modulation of key cell cycle
regulators and blocks cell migration via alterations in the
activation status of proteins essential for cytoskeletal dynamics.
We further showed via microarray analysis that propranolol leads to
large-scale changes in global gene expression, particularly in
genes involved in lipid/sterol metabolism, cell cycle regulation,
angiogenesis and post-translational modification. Interestingly,
our data indicate that the effects of propranolol on HemECs are
similar to that observed in normal endothelial cells, suggesting
that this drug is not specific to HemECs.
Materials and methods
Cell lines and culture conditions
HemECs were previously isolated from
proliferating-phase IH specimens collected from female infants
(12). Primary cultures of
neonatal human dermal microvascular endothelial cells (HDMVECs) and
human coronary artery endothelial cells (HCAECs) were purchased
from ATCC. These cell lines were cultured in vascular cell basal
media (ATCC #PCS-100-030) and supplemented with 0.2% bovine brain
extract, 5 ng/ml human epidermal growth factor, 10 mM L-glutamine,
0.75 U/ml heparin sulfate, 1 μg/ml hydrocortisone, 50 μg/ml
ascorbic acid, 2% fetal bovine serum and penicillin/streptomycin.
For all experiments cell lines were used at <10 passages.
RT-PCR
RNA was isolated from cells using the Ambion
Purelink Mini kit according to the manufacturer’s directions.
qRT-PCR was performed on an ABI7900HT RT-PCR system using TaqMan
assays with predesigned primer sets for the genes of interest
(Invitrogen). All RT-PCR experiments were performed in triplicate.
Data shown are the average RQ value ± standard deviation of 4
replicates.
Western blot analysis
Cell lysates were collected after 48 h treatment and
subjected to SDS-PAGE on gradient (4–15%) gels and subsequently
transferred to PVDF for western blotting. p-vascular endothelial
growth factor receptor-2 (VEGFR-2) (Cell Signaling #2478), VEGFR-2
(Cell Signaling #2479), p-p38 (Cell Signaling #4511), p-p44/42
(Cell Signaling #4370), p-SAPK/JNK (Cell Signaling #4668), p-ATF2
(Cell Signaling #5112), actin (Santa Cruz #SC47778), cyclin A1
(Abcam #ab13337), cyclin A2 (Abcam #7956), cyclin B2 (Abcam
#18250), cyclin D1 (Cell Signaling #2978), cyclin D2 (Cell
Signaling #3741), cyclin D3 (Cell Signaling #2936), cyclin E1 (Cell
Signaling #4129), p15 (Cell Signaling #4822), p21 (Cell Signaling
#2947), p27 (Cell Signaling #3698), cleaved caspase-9 (Cell
Signaling #9509), cleaved caspase-3 (Cell Signaling #9664), p-FAK
(Cell Signaling #3283), p-cofilin (Cell Signaling #3313), cofilin
(Cell Signaling #3318), p-ERM (Cell Signaling #3149), ERM (Cell
Signaling #3142), p-MYPT1 (Cell Signaling #4563) and MYPT1 (Cell
Signaling #2634) antibodies were used at a 1:1000 dilution,
followed by incubation with 1:1000 HRP-conjugated anti-mouse or
anti-rabbit antibodies (as appropriate). Proteins were detected
using Supersignal West Dura Extended Duration Substrate (Thermo
Scientific) and digitally captured using a GE Image Quant LAS4000
imaging system.
Proliferation assay
Cells were plated at subconfluent density and
subjected to the indicated treatments for 48 h. Images from 5
independent areas were collected at 1-h intervals using a Nikon
Biostation CT time lapse imaging robot. Changes in cell density
were calculated every 24 h by counting the number of cells in the
selected field of vision. Data shown represent the average of 5
independent areas ± the standard deviation.
Flow cytometry
Cells were treated as indicated, trypsinized, and
fixed in 70:30 ethanol:phosphate-buffered saline overnight. Cells
were then stained with 200 μg/ml ethidium bromide plus 20 μg/ml
RNase A and incubated overnight. DNA content was analyzed using an
Accuri C6 flow cytometer. Data shown are representative of at least
3 independent experiments. Quantitative analysis of DNA content was
performed using CFlow Plus software (Accuri) and is the average of
triplicate data points.
Live/dead assay
Cells were treated as indicated, stained for 10 min
with 5 μg/ml Hoechst and 5 μg/ml propidium iodide, and washed 3
times in PBS. A Nikon C2SI scanning laser confocal microscope was
used to image the red and blue channels. Percent apoptosis (A) was
calculated by the following formula: A = (number of red
cells/number of blue cells) x 100. The data presented is the
average of triplicates.
Migration assay
Confluent cultures were treated as indicated,
scratch wounded, and the progress of ‘healing’ of the wound was
monitored using a Nikon Biostation CT time lapse imaging robot.
Migration speed was calculated by monitoring the movement of the
‘wound’ toward its center at each hour over a 12-h period.
Immunofluorescence and cytoskeletal
organization calculations
Cells were grown on glass coverslips, treated as
indicated and fixed in 4% paraformaldehyde. Then, the coverslips
were blocked in 5% bovine serum albumin plus 0.5% Tween-20,
incubated with 1:200 of the p-FAK antibody and detected with
fluorescently conjugated secondary antibodies. Actin microfilaments
were detected by staining with Rhodamine-conjugated phalloidin, and
cell nuclei were detected with 4′,6-diamidino-2-phenylindole
(DAPI). Immunofluorescent images were captured as z-stacks using a
Nikon C2SI scanning laser confocal microscope. Image analysis of
cytoskeletal organization included calculating the actin stress
fiber correlation and binarizing this correlation image to
determine fiber lengths using the FiberScore algorithm (13).
Microarray analysis
Total RNA was amplified and biotin-labeled using
Illumina TotalPrep RNA Amplification kit (Ambion). A total amount
of 750 ng of biotinylated aRNA was then briefly heat-denatured and
loaded onto expression arrays to hybridize overnight. Following
hybridization, arrays were labeled with Cy3-streptavidin and imaged
on the Illumina ISCAN. Intensity values were transferred to Agilent
GeneSpring GX microarray analysis software and data were filtered
based on the quality of each call. Statistical relevance was
determined using ANOVA with a Benjamini Hochberg FDR multiple
testing correction (p<0.05). Data were then limited by fold
change analysis to statistically relevant data points demonstrating
a 2-fold or more change in expression.
Results
β-adrenergic receptor expression in
HemECs and IHs
The presence of β-adrenergic receptors on normal
human endothelial cells has been previously confirmed (14). However, despite the extensive use
of systemic propranolol as an anti-IH agent, the expression of the
three known β-adrenergic receptors in endothelial cells isolated
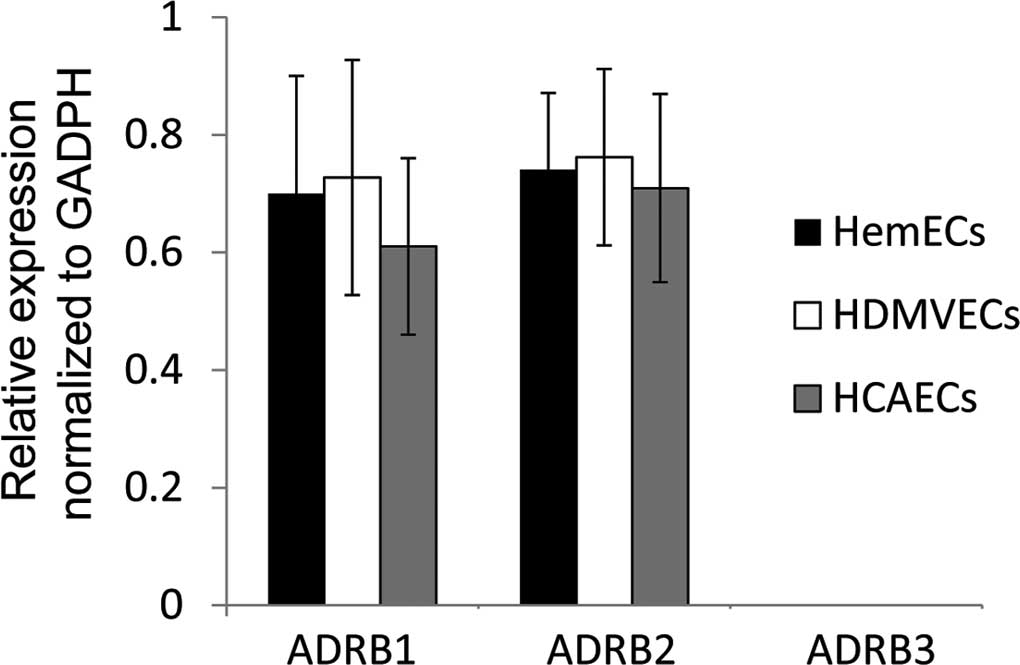
from these benign tumors is unknown. Using RT-PCR, we evaluated the
steady state mRNA expression of the three known β-adrenergic
receptors (ADRB1, ADRB2 and ADRB3) in cultured HemECs. Our data
revealed that ADRB1 and 2, although not ADRB3, were expressed in
HemECs (Fig. 1). Moreover, similar
results were observed for both HDMVECs and HCAECs, with equivalent
levels of each receptor across the three endothelial cell
lines.
Propranolol disrupts cell cycle
progression
Despite the extensive use of propranolol, many of
the mechanisms of action of this drug on IHs have been inferred
from its effects on normal endothelial cells (7–9).
Recent studies have suggested that propranolol may inhibit IHs by
suppressing production of nitric oxide and HIF1α signaling
(10,11). However, the signaling intermediates
and many of the downstream effectors which modulate its action on
IHs are largely unknown. To elucidate the molecular components at
play following propranolol-induced inhibition of HemEC
proliferation, we first examined the growth rates of HemECs,
HDMVECs and HCAECs after treatment with a dose curve of
propranolol. Our data indicate that the IC50 for
propranolol-induced inhibition of proliferation was ∼50 μM for all
three cell types (Fig. 2A and B),
therefore for all subsequent experiments in this study we continued
to use this concentration. Moreover, cell cycle analysis on the
panel of endothelial cells using flow cytometry revealed that
propranolol indiscriminately induced an increase in the proportion
of cells in the G1 phase of the cell cycle, while reducing the
proportion of cells in the S and G2/M phases (Fig. 2C, Table I). Equivalent results were observed
in HDMVECs and HCAECs (Table I).
To address the effects of propranolol on HIHEC proliferation, we
analyzed the expression/activation status of a number of proteins
involved in regulating proliferation. VEGFR-2 is a strong mitogenic
regulator of endothelial cells that shows aberrant constitutive
activation in HemECs (15), and
its phosphorylation is reportedly blocked following propranolol
treatment (5). Indeed, the 24-h
treatment of HemECs with 50 mM propranolol resulted in sharply
decreased VEGFR-2 phosphorylation (Fig. 2D). The mitogen activated protein
kinases (MAPKs) are direct downstream effectors of VEGFR-2
regulating VEGF-induced endothelial proliferation. We tested the
activation status of p38, p44, p42, SAPK, JNK, and the downstream
effector ATF4 in HemECs experiencing 24 h of propranolol treatment.
Of the proteins tested, the stress activated p38 (but not the
stress activated SAPK or JNK) was the only one that exhibited a
significant change in phosphorylation following propranolol
treatment of HemECs (Fig. 2D).
These data suggest that despite the inhibition of VEGFR-2 noted
following the treatment, the major proliferative MAPKs such as p44
and p42 were not affected by propranolol treatment in HemECs. As
flow cytometry analysis indicated that propranolol induced
alterations in cell cycle progression, we performed western blot
analysis on a panel of cell cycle regulators, discovering that this
drug decreases the expression of key cyclin proteins (cyclins A1,
A2, B2, D2 and D3) and increases the expression of important cell
cycle inhibitors (p15, p21 and p27) (Fig. 2E). No change in the expression of
Cdk2 or Cdk4 was observed following the treatment. These
alterations in key cell cycle regulators likely account for
propranolol-induced alterations in HemEC proliferation.
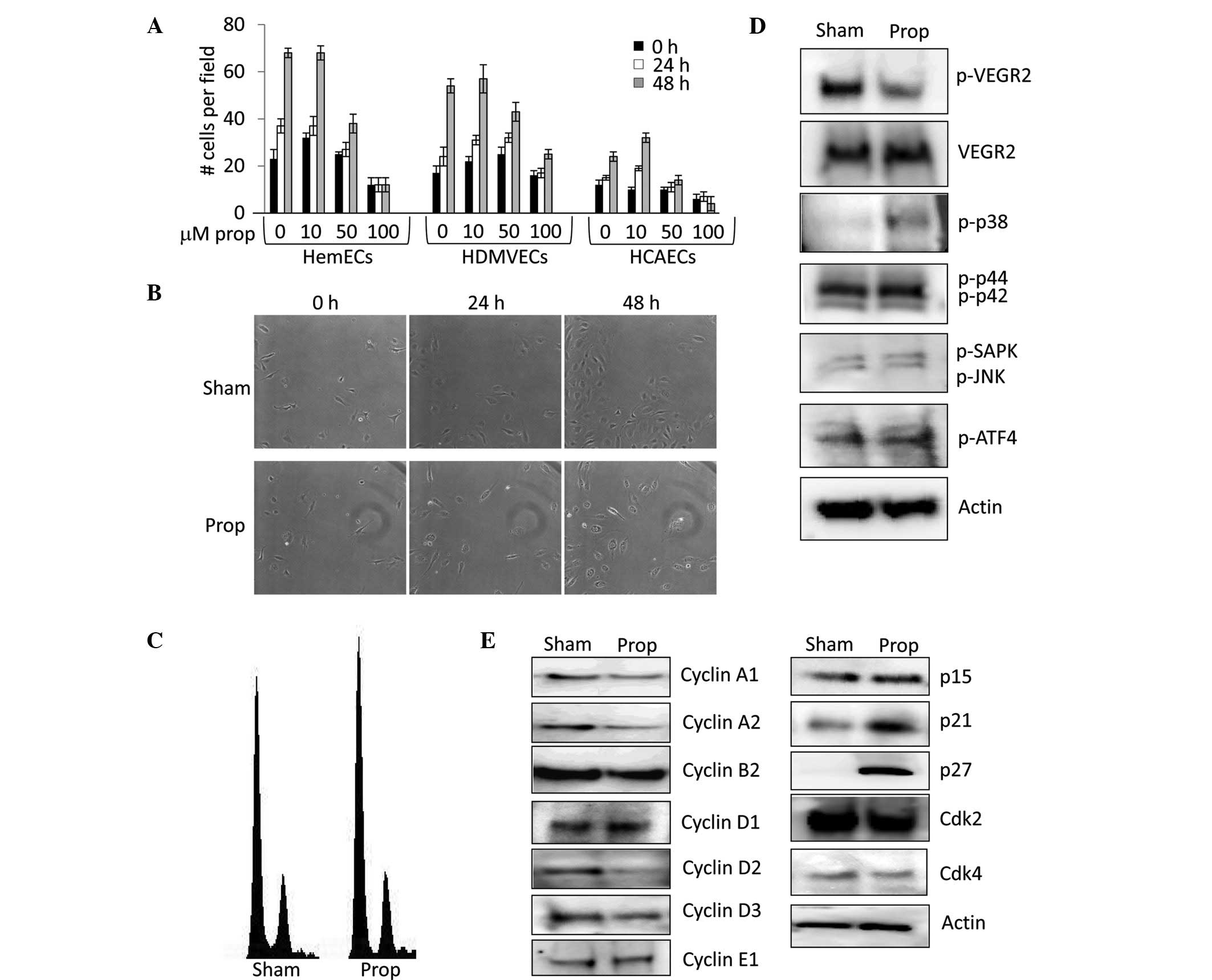 | Figure 2Propranolol decreases the
proliferation of human infantile hemangioma endothelial cells
(HemECs). (A) HemECs, human dermal microvascular endothelial cells
(HDMVECs), and human coronary artery endothelial cells (HCAECs)
were treated with a dose curve of propranolol (0 to 100 μM) and
cell proliferation was measured by counting changes in the number
of cells/defined vision field over a 48-h period. (B) Time lapse
microscopy image of sham and 50 μM propranolol treated HemECs over
a 48-h period. (C) DNA content analysis of propidium iodide stained
HemECs treated with sham or 50 μM propranolol for 48 h. (D) Western
blot analysis detecting the levels of phosphorylated and total
vascular endothelial growth factor receptor-2 (p-VEGFR-2 and
VEGFR-2, respectively) and the phosphorylated forms of p38 (p-p38),
p44 (p-p44), p42 (p-p42), stress activated protein kinase (p-SAPK),
c-jun N-terminal kinase (p-JNK), and activating transcription
factor 4 (p-ATF4) in HemECs treated for 24 h with sham or 50 μM
propranolol. Actin levels were used as a loading control. (E)
Western blot analysis detecting the levels of cyclins, cyclin
dependent kinases, and cyclin dependent kinase inhibitors in HemECs
treated for 24 h with sham or 50 μM propranolol. Actin levels were
used as a loading control. Prop, propranolol. |
 | Table IPercentage of endothelial cells in
each cell cycle phase. |
Table I
Percentage of endothelial cells in
each cell cycle phase.
| Cells | Sham | Propranolol |
|---|
| HemECs | | |
| G1 | 68±2.3 | 74±2.2 |
| S | 8±0.6 | 5±0.3 |
| G2/M | 24±2.7 | 21±1.1 |
| HDMVECs | | |
| G1 | 69±3.0 | 75±1.6 |
| S | 8±4.1 | 4±0 |
| G2/M | 22±3.9 | 20±4.5 |
| HCAECs | | |
| G1 | 71±1.4 | 76±1.7 |
| S | 5±1.6 | 3±1.3 |
| G2/M | 23±3.3 | 20±2.5 |
It is speculated that propranolol may
increase apoptosis of IHs
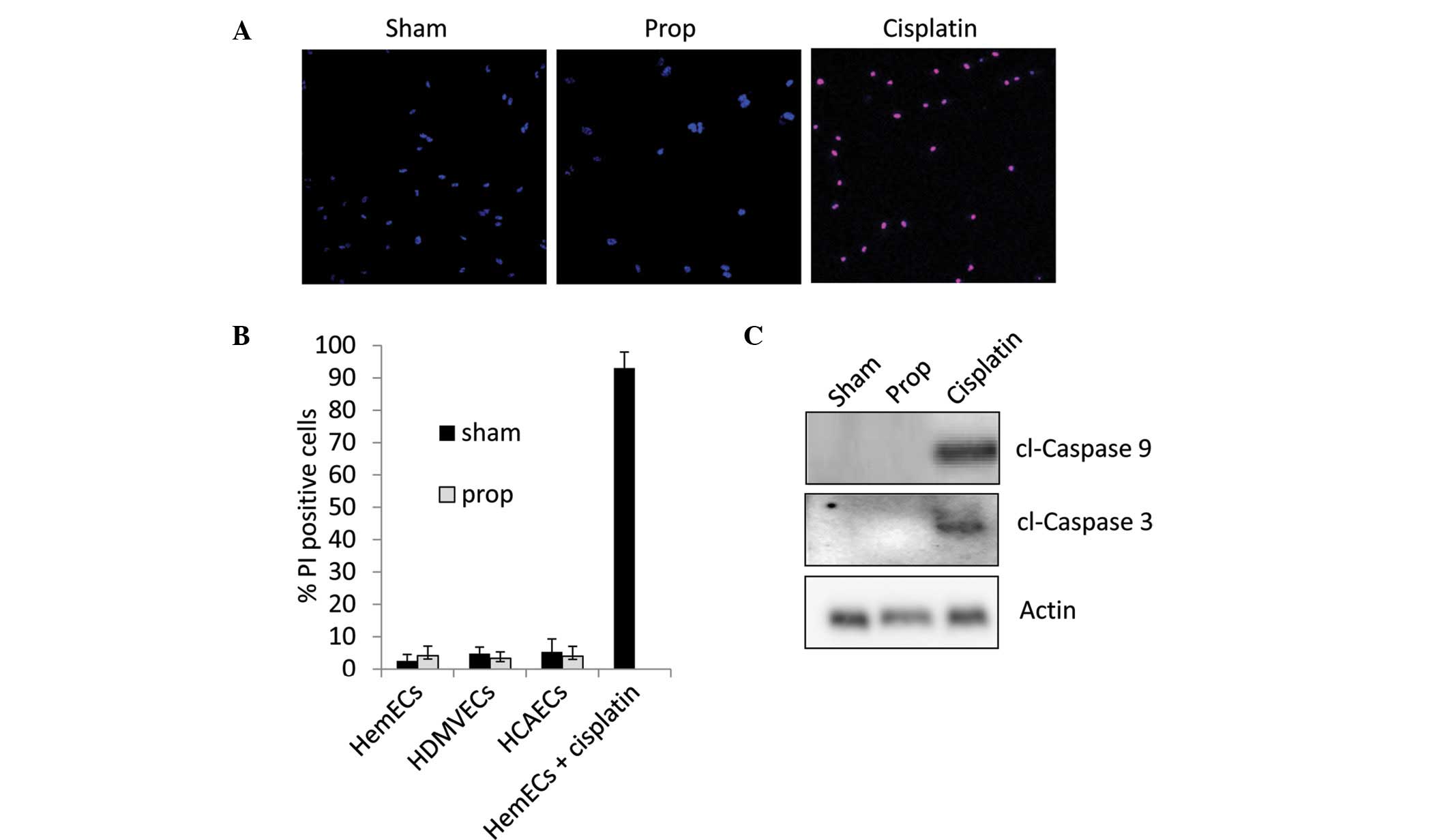
To determine whether this drug affects apoptosis, we
treated HemECs, HDMVECs and HCAECs with 50 μM propranolol for 3
days. As a control we treated HemECs with 5 μM cisplatin for an
equivalent amount of time. Cells were co-stained with propidium
iodide (which only stains the nuclei of dead cells) and Hoechst dye
(which stains the nuclei of both live and dead cells). Calculation
of the apoptotic index from each treatment revealed that 50 μM
propranolol did not induce apoptosis of any of the cell lines
tested, while 5 μM cisplatin resulted in almost 100% apoptosis
(Fig. 3A and B). We did observe
significant apoptosis in all of our cell lines at concentrations of
propranolol higher than 150 μM (data not shown). To confirm our
observations, we utilized western blotting to detect the cleavage
products of the apoptotic initiator caspase-9 and the apoptotic
effector caspase-3. Our data indicate that while 5 μM cisplatin
strongly induced caspase cleavage, 50 μM propranolol failed to
induce apoptotic signaling (Fig.
3C).
Propranolol disrupts cell migration and
actin cytoskeleton dynamics
Several reports have presented mixed results for the
role of β-adrenergic receptor signaling in wound healing and cell
migration, with evidence that inhibition of this class of receptors
delays (16–19) or promotes (20–22)
wound healing. Moreover, in cultured bovine aortic endothelial
cells, β-adrenergic blockade with propranolol reportedly inhibits
norepinephrine-induced induction of actin stress fibers (8), thus we sought to determine if similar
effects on cell migration and cytoskeletal organization could be
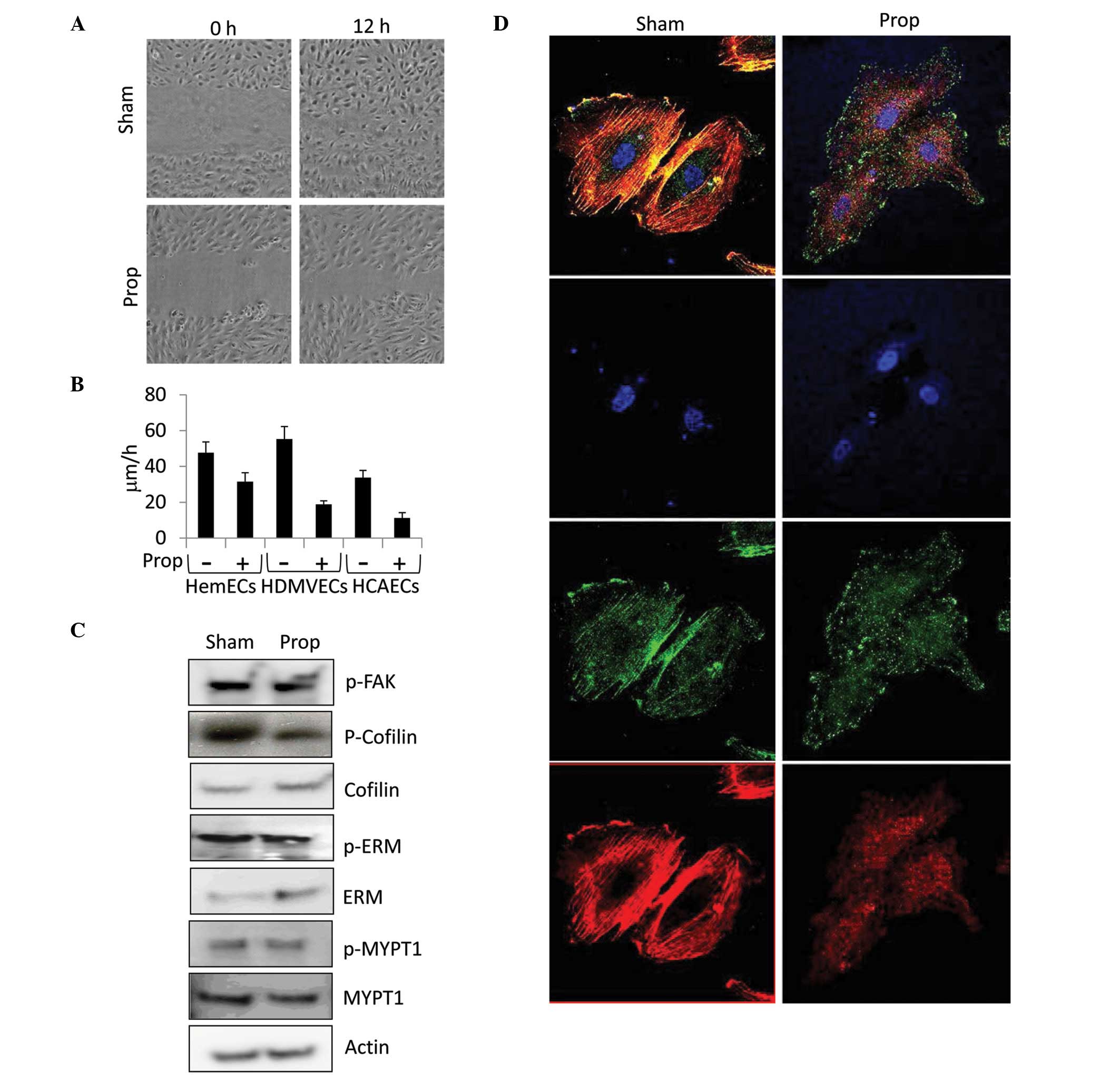
observed in HemECs treated with propranolol. HemECs, HDMVECs and
HCAECs were grown to confluence, manually scratch wounded with a
micropipette tip, and imaged using time lapse microscopy over a
period of 12 h. As illustrated in Fig.
4A, treatment of HemECs with 50 μM propranolol resulted in a
significant reduction in ‘wound’ closure compared to the control.
Quantification of the time lapse images taken from the scratch
migration assay revealed that propranolol dramatically reduced the
migratory speed of HemECs (34% reduction), HMVECs (66% reduction)
and HCAECs (67% reduction) (Fig.
4B), suggesting that propranolol is more effective at blocking
proliferation of normal endothelial cells than HemECs. To identify
signaling events that might shed light on how propranolol disrupts
migration, we performed western blot analysis to detect the
activation status of several known regulators of actin cytoskeletal
dynamics including focal adhesion kinase (FAK), cofilin,
ezrin/radixin/moesin (ERM), and myosin phosphatase (MYPT1),
revealing that this drug effectively decreases the inhibitory
phosphorylation of cofilin (an actin severing protein) at serine-3
(Fig. 4C). Given the increased
activation of cofilin following propranolol treatment, we suspected
that changes in the actin microfilament cytoskeleton would ensue.
Indeed, immunofluorescent detection of actin stress fibers revealed
that propranolol markedly inhibits actin polymerization in HemECs
(Fig. 4D) and normal endothelial
cells (data not shown) consistent with that expected from
activation of cofilin. Computational analysis of actin stress fiber
length using the FiberScore algorithm (Lichtenstein) demonstrated
that propranolol-treated HemECs exhibit a greater than 1.5-fold
reduction in average fiber length compared to the sham treatment
(data not shown). Similar observations were observed for
non-hemangioma endothelial cells (data not shown). In addition to
altering actin stress fiber polymerization, propranolol shifted the
subcellular localization of p-FAK from regions of colocalization
with actin stress fibers in sham-treated cells to diffuse punctuate
regions located throughout the cytoplasm in propranolol-treated
cells (Fig. 4D). Despite
alterations in p-FAK subcellular localization, no changes in the
levels of p-FAK were observed in response to propranolol (Fig. 4C).
Propranolol disrupts global gene
expression patterns in endothelial cells
Propranolol has been shown to affect the expression
of cyclins across multiple cell types (5,23),
gluconeogenic and glycolytic enzymes in the liver (24), epidermal growth factor 1 in
cardiomyocytes (25) and pigment
epithelial derived factor in the retina (26). However, these studies have focused
on small subsets of genes and did not look at large-scale changes
in genomic expression patterns. To evaluate the global gene
expression changes in HemECs in response to propranolol and to
examine how the identified changes compared with those observed in
propranolol-treated normal human endothelial cells, we performed
whole genome microarrays providing coverage for more than 47,000
transcripts and known splice variants across the human
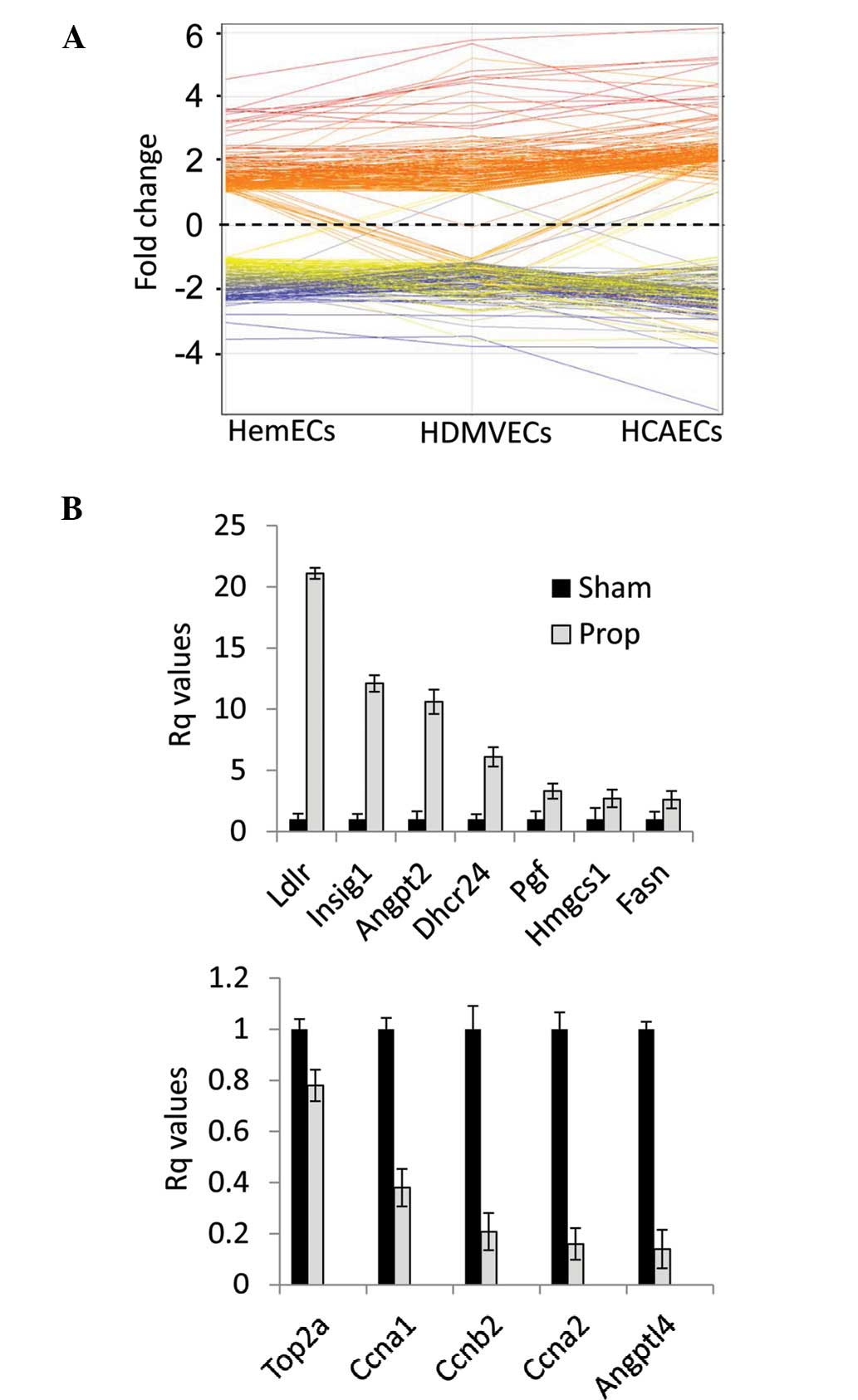
transcriptome. Our analysis identified 89 genes whose expression in
HemECs was altered greater than 2-fold (p<0.05) in response to
propranolol (32 genes significantly upregulated and 57 genes
downregulated) (Table II). Several
functional groupings of genes were identified included those
involved in lipid and sterol metabolism (21% of total gene
expression changes: HMGCS1, MSMO1, LDLR,
DHCR7, SCD, ACAT2, LSS, FASN,
MSMO1, SQLE, DHCR24, FDFT1,
IDI1, FADS2, ACSS2, EBP, SC5DL,
NSDHL and LPIN1), cell cycle regulation (14% of total
gene expression changes: CDC2, CDCA8, CDKN3,
PRC1, MCM4, CDC20, CDC45L,
CCNA1, CCNB2, CCNA2, TOP2A and
CDCA7), angiogenesis (5% of total gene expression changes:
PGF, ANGPT2, ANGPTL4 and RGS4) and
ubiquitin modifications (3% of total gene expression changes:
UBE2T, UBE2C and UHRF1). Comparative analysis
of genes whose expression was statistically altered by propranolol
treatment in any of the three endothelial cell line tests revealed
a strong correlation between cell lines (Fig. 5A). This data indicate that
propranolol-induced gene expression changes are endothelial
cell-type independent. Quantitative RT-PCR validation of ∼14% of
the propranolol-responsive genes in HemECs revealed comparable
alterations in gene expression similar to that revealed by
microarray analysis, thus corroborating our microarray data through
independent analysis (Fig.
5B).
| Table IIAlterations in gene expression
(fold-change) induced by propranolol treatment. |
Table II
Alterations in gene expression
(fold-change) induced by propranolol treatment.
| Gene symbol | Gene name | Accession no. | HIHEC | HDMVEC | HCAEC |
|---|
| HMGCS1 |
3-Hydroxy-3-methylglutaryl-CoA synthase
1 | NM_002130.6 | 4.6 | 5.8 | 6.2 |
| MSMO1 | Methylsterol
monooxygenase 1, TV2 | NM_001017369.2 | 4.5 | 4.0 | 5.8 |
| INSIG1 | Insulin induced
gene 1 | NM_198336.2 | 4.3 | 4.6 | 4.9 |
| LDLR | Low density
lipoprotein receptor | NM_000527.4 | 3.6 | 3.8 | 3.9 |
| MVD | Mevalonate
decarboxylase | NM_002461.1 | 3.6 | 5.7 | 3.4 |
| DHCR7 |
7-Dehydrocholesterol reductase | NM_001360.2 | 3.6 | 4.7 | 3.4 |
| SCD | Stearoyl-CoA
desaturase | NM_005063.4 | 3.3 | 3.2 | 5.0 |
| ACAT2 | Acetyl-CoA
acetyltransferase 2 | NM_005891.2 | 3.2 | 4.6 | 5.2 |
| LSS | Lanosterol
synthase | NM_002340.5 | 3.2 | 4.5 | 5.1 |
| TM7SF2 | Transmembrane 7
superfamily member 2 | NM_003273.2 | 3.0 | 4.8 | 5.2 |
| HMGCR |
3-Hydroxy-3-methylglutaryl-CoA
reductase | NM_000859.2 | 2.9 | 3.1 | 3.8 |
| FASN | Fatty acid
synthase | NM_004104.4 | 2.8 | 4.6 | 4.3 |
| MSMO1 | Methylsterol
monooxygenase 1, TV1 | NM_006745.4 | 2.8 | 2.0 | 3.0 |
| SQLE | Squalene
epoxidase | NM_003129.3 | 2.7 | 2.6 | 3.6 |
| PSG4 | Pregnancy specific
β-1-glycoprotein 4 | NM_002780.3 | 2.6 | 1.3 | 4.5 |
| DHCR24 |
24-Dehydrocholesterol reductase | NM_014762.3 | 2.5 | 2.4 | 3.3 |
| FDFT1 |
Farnesyl-diphosphate farnesyltransferase
1 | NM_004462.3 | 2.5 | 2.2 | 3.2 |
| IDI1 |
Isopentenyl-diphosphate δ isomerase 1 | NM_004508.2 | 2.4 | 2.3 | 3.4 |
| FADS2 | Fatty acid
desaturase 2 | NM_004265.2 | 2.4 | 4.2 | 2.8 |
| NPC1 | Niemann-Pick
disease, type C1 | NM_000271.4 | 2.3 | 2.3 | 3.8 |
| PFKFB4 |
Fructose-2,6-biphosphatase 4 | NM_004567.2 | 2.2 | 2.8 | 2.3 |
| ACSS2 | Acyl-CoA synthetase
family member 2, TV2 | NM_001076552.2 | 2.2 | 2.6 | 3.5 |
| ACSS2 | Acyl-CoA synthetase
family member 2, TV1 | NM_018677.3 | 2.2 | 2.7 | 3.2 |
| EBP | Emopamil binding
protein | NM_006579.2 | 2.1 | 2.4 | 2.3 |
|
LOC100129668 | LOC100129669 | XM_001713607.1 | 2.1 | 2.2 | 2.5 |
| HMOX1 | Heme oxygenase
(decycling) 1 | NM_002133.2 | 2.1 | 2.1 | 3.5 |
| SC5DL |
Sterol-C5-desaturase-like | NM_006918.4 | 2.1 | 1.4 | 2.4 |
| NSDHL | NAD(P) dependent
steroid dehydrogenase-like | NM_015922.2 | 2.1 | 2.3 | 2.2 |
| P2RX4 | Purinergic receptor
P2X, 4 | NM_002560.2 | 2.1 | 1.7 | 1.8 |
| LPIN1 | Lipin 1 | NM_145693.1 | 2.0 | 1.6 | 2.9 |
| PGF | Placental growth
factor | NM_002632.5 | 2.0 | 1.7 | 2.3 |
| ANGPT2 | Angiopoietin 2 | NM_001147.2 | 2.0 | 1.0 | 2.1 |
|
LOC729009 | LOC729010 | XR_042330.1 | 2.0 | 1.6 | 2.6 |
| IL8 | Interleukin 8 | NM_000584.3 | −2.0 | −2.9 | −3.1 |
| CDK1 | Cyclin-dependent
kinase 1 | NM_001786.4 | −2.0 | −1.8 | −2.1 |
| TUBB2C | Tubulin, β 4B
Ivb | NM_006088.5 | −2.0 | −1.4 | −2.5 |
| PTTG1 | Pituitary
tumor-transforming 1 | NM_004219.2 | −2.0 | −2.0 | −2.0 |
| OIP5 | Opa interacting
protein 5 | NM_007280.1 | −2.0 | −2.3 | −2.1 |
| CDCA8 | Cell division cycle
associated 8 | NM_018101.3 | 2.0 | −1.4 | −2.3 |
| TAGLN | Transgelin | NM_003186.3 | −2.0 | −1.7 | −2.9 |
| CDKN3 | Cyclin-dependent
kinase inhibitor 3 | NM_005192.3 | −2.0 | −1.7 | −1.6 |
| ANLN | Anillin, actin
binding protein | NM_018685.2 | −2.0 | −1.8 | −1.7 |
| HJURP | Holliday junction
recognition protein | NM_018410.3 | −2.0 | −1.2 | −2.0 |
| PBK | PDZ binding
kinase | NM_018492.2 | −2.0 | −1.6 | −2.5 |
| UBE2T |
Ubiquitin-conjugating enzyme E2T
(putative) | NM_014176.3 | −2.0 | −1.4 | −1.5 |
| STEAP1 | 6-Transmembrane
epithelial antigen of the prostate 1 | NM_012449.2 | −2.0 | −1.8 | −1.8 |
| UBE2C |
Ubiquitin-conjugating enzyme E2C, TV3 | NM_181800.1 | −2.0 | −1.9 | −2.8 |
| CKS1B | CDC28 protein
kinase regulatory subunit 1B | NM_001826.2 | −2.0 | −1.6 | −1.9 |
| TACC3 | Transforming,
acidic coiled-coil containing protein 3 | NM_006342.2 | −2.0 | −1.4 | −1.8 |
| NCAPG | Non-SMC condensin I
complex, subunit G | NM_022346.3 | −2.0 | −1.7 | −1.6 |
| PCDH7 | Protocadherin
7 | NM_002589.2 | −2.0 | −1.2 | −2.2 |
| FAM64A | Family with
sequence similarity 64, member A | NM_019013.2 | −2.1 | −1.2 | −2.0 |
| PRC1 | Protein regulator
of cytokinesis 1 | NM_199413.1 | −2.1 | −1.5 | −2.3 |
| MELK | Maternal embryonic
leucine zipper kinase | NM_014791.3 | −2.1 | −1.8 | −2.1 |
| TPX2 | TPX2,
microtubule-associated | NM_012112.4 | −2.1 | −1.4 | −2.2 |
| MCM4 | Minichromosome
maintenance complex CMPT 4, TV2 | NM_182746.2 | −2.1 | −1.6 | −1.9 |
| ZWINT | ZW10
interactor | NM_001005413.1 | −2.1 | −1.5 | −2.0 |
| KIFC1 | Kinesin family
member C1 | NM_002263.2 | −2.1 | −1.4 | −2.2 |
| CDC20 | Cell division cycle
20 | NM_001255.2 | −2.2 | −2.0 | −4.0 |
| UBE2C |
Ubiquitin-conjugating enzyme E2C, TV6 | NM_181803.1 | −2.2 | −1.8 | −2.4 |
| NCAPG2 | Non-SMC condensin
II complex, subunit G2 | NM_017760.5 | −2.2 | −1.3 | −1.4 |
|
SERPIND1 | Serpin peptidase
inhibitor, clade D, member 1 | NM_000185.3 | −2.2 | −1.8 | −2.6 |
| CDC45L | Cell division cycle
45 | NM_003504.3 | −2.2 | −1.8 | −3.0 |
| LYAR | Ly1 antibody
reactive | NM_017816.2 | −2.2 | −1.6 | −1.3 |
| CCNA1 | Cyclin A1 | NM_003914.3 | −2.2 | −2.2 | −1.9 |
| TRIP1 | Thyroid hormone
receptor interactor 13 | NM_004237.3 | −2.2 | −1.9 | −2.6 |
| MPZL2 | Myelin protein
zero-like 2, TV2 | NM_144765.2 | −2.2 | −1.3 | −2.4 |
| CEP55 | Centrosomal protein
55kDa | NM_018131.4 | −2.2 | −2.0 | −2.1 |
| CXCL1 | Chemokine (C-X-C
motif) ligand 1 | NM_001511.3 | −2.2 | −2.5 | −2.8 |
| CCNB2 | Cyclin B2 | NM_004701.3 | −2.2 | −2.2 | −2.3 |
| KIF20A | Kinesin family
member 20A | NM_005733.2 | −2.2 | −1.9 | −2.5 |
|
RAD51AP1 | RAD51 associated
protein 1 | NM_006479.4 | −2.2 | −1.6 | −2.2 |
| GINS2 | GINS complex
subunit 2 | NM_016095.2 | −2.2 | −1.7 | −2.9 |
| FAM83D | Family with
sequence similarity 83, member D | NM_030919.2 | −2.3 | −1.6 | −2.4 |
|
KIAA0101 | KIAA0101 | NM_014736.4 | −2.3 | −2.0 | −2.3 |
| DLGAP5 | Discs, large
(Drosophila) homolog-associated protein 5 | NM_014750.4 | −2.3 | −2.0 | −2.3 |
| CCNA2 | Cyclin A2 | NM_001237.3 | −2.3 | −2.2 | −2.8 |
|
LOC399942 | LOC399943 | XM_934471.1 | −2.3 | −2.4 | −3.4 |
| MPZL2 | Myelin protein
zero-like 2, TV1 | NM_005797.3 | −2.3 | −2.7 | −2.2 |
| TOP2A | Topoisomerase II α
170kDa | NM_001067.3 | −2.3 | −2.4 | −2.6 |
| RRM2 | Ribonucleotide
reductase M2 | NM_001034.3 | −2.3 | −1.5 | −2.8 |
| FBXO5 | F-box protein
5 | NM_012177.3 | −2.4 | −1.9 | −2.6 |
| CDCA7 | Cell division cycle
associated 7 | NM_031942.4 | −2.4 | −1.9 | −2.5 |
| MCM4 | Minichromosome
maintenance complex CMPT 4, TV1 | NM_005914.3 | −2.4 | −1.5 | −2.0 |
| MAD2L1 | MAD2 mitotic arrest
deficient-like 1 | NM_002358.3 | −2.4 | −2.3 | −2.1 |
| UHRF1 | Ubiquitin-like with
PHD and ring finger domains 1 | NM_001048201.1 | −2.5 | −1.6 | −2.6 |
| ANGPTL4 | Angiopoietin-like
4 | NM_139314.1 | −2.8 | −2.8 | −2.9 |
| RGS4 | Regulator of
G-protein signaling 4 | NM_005613.5 | −3.0 | −3.8 | −3.8 |
| IL1RL1 | Interleukin 1
receptor-like 1 | NM_003856.2 | −3.2 | 3.4 | −5.2 |
Discussion
IHs as a whole are largely understudied considering
the high prevalence of these lesions in children and the serious
threat to health they pose in certain instances. To date, there
remains a great deal of uncertainty as to the origin of these
tumors, with evidence suggesting they may be caused by aberrant
transplantation of placental endothelial cells (27), predisposing genetic factors
(28,29) and/or tumor stem cell components
(30). Despite the controversial
origin of these tumors, proliferating IHs are characterized by an
enhanced angiogenic capacity largely due to modulation of signaling
pathways that regulate the VEGF signaling axis, while involuting
IHs display a chronic inflammatory response and downregulation of
angiogenesis regulators (31). The
recent discovery that the β blocker propranolol is an effective
treatment for IHs suggests that the sympathetic nervous system may
play a key role in controlling IH growth. Epinephrine is a
sympathomimetic amine that increases the activity of noradrenaline
in post-synaptic cells, and is capable of enhancing vasodilation
through activation of β-adrenergic receptors. β-adrenergic
receptors have been shown to be expressed on normal capillary
endothelial cells (32) and it is
believed that β blockers, such as propranolol, inhibit epinephrine
signaling through inducing vasoconstriction of endothelial cells
and disruptions in key angiogenic processes (7–9,33).
Moreover, β blockers have been shown to reduce the expression of
VEGF in non-endothelial cells, thus leading to inhibition of
angiogenic paracrine signaling (34). Despite the extensive use of
propranolol in the treatment of IHs, very little has been done to
determine the molecular mechanisms of propranolol in IH tumors.
This drug is presumably believed to induce IH tumor regression
through mechanisms similar to that noted in normal endothelial
cells, and recent reports suggest that it may work in part through
suppressing production of nitric oxide and HIF1α regulation of VEGF
expression (10,11). In this study, we sought to
investigate how propranolol disrupts HIHEC function and compare
these effects to those seen in normal primary endothelial cell
lines. Our data demonstrated that β-adrenergic receptors are
expressed across a panel of HIHEC and normal endothelial cells. We
further showed that propranolol disrupts HIHEC and normal
endothelial cell cycle progression, migration, cytoskeletal
dynamics, and gene expression, and we elucidated multiple
downstream targets of propranolol including cell cycle progression
regulators, cytoskeletal modulators and gene expression
alterations.
The expression of β1- and β2-adrenergic receptors
has been extensively studied in the cardiovascular system, with
high expression occurring in cardiac myocytes and vascular smooth
muscle cells (35). Although
β3-knockout mice display increased hypotension in response to
isoproternol (36), these
receptors are suspected to play a lesser role in cardiovascular
function compared to β1- and β2- receptors as they are expressed
primarily in brown adipocytes, gallbladder and the colon (37). Our data indicate that both β1- and
β2- (but not β3-) adrenergic receptors are expressed on primary
cultures of HemECs. Interestingly, comparisons of the relative mRNA
expression levels of these receptors on primary cultures of
non-diseased endothelial cells revealed similar levels to that of
HemECs, causing us to question if propranolol is selective for
HemECs or if this drug demonstrates a similar level of inhibition
for diseased and normal endothelial cells. Indeed, comparisons of
the inhibitory effect of propranolol at its IC50 on
cultures of HemECs, HDMVECs, and HCAECs revealed that this drug
indiscriminately blocks proliferation, migration, and actin
polymerization in an endothelial cell-type independent manner. This
finding suggests that the mechanism of action for propranolol on
IHs may extend beyond simply blocking endothelial cell function.
For instance, IHs display a high pericyte density in the
proliferating stage (38) and
increased molecular markers of endothelial cell/pericyte
interactions (31). Primary
cultures of pericytes express functional adrenergic receptors and
respond to autonomic vasoactive substances in vivo (39). As pericytes are responsible for a
number of roles in the microvasculature including capillary
maturation and stabilization, further studies should examine if
propranolol inhibits IH growth through destabilization of
endothelial cell/pericyte interactions. Another possibility that
may account for the endothelial cell-type independent action of
propranolol may have to do with the limitations of in vitro
monolayer cell culture systems. Children undergoing systemic
propranolol treatment for IHs often undergo side effects including
bradycardia, hypotension and hypoglycemia (40), however significant disruptions of
their existing vascular beds have not been reported. This suggests
that propranolol may preferentially inhibit proliferating
endothelial vasculature while sparing the quiescent established
vasculature. However, this possibility is complicated by reports
suggesting that propranolol improves wound healing - a process
intimately dependent on neovascularization (20–22).
There is evidence that VEGFR-2 phosphorylation is
controlled by β-adrenergic signaling (5,41,42),
however the mechanisms underlying this effect remain to be
determined. As HemECs are characterized by aberrant constitutive
activation of VEGFR-2 signaling, we sought to determine whether
propranolol is capable of attenuating this process. Similar to data
reported in normal endothelial lines, propranolol effectively
blocks VEGFR-2 phosphorylation on HemECs. We tested the effects of
propranolol on known downstream targets of VEGF signaling revealing
propranolol-induced alterations in p38 signaling, decreased cyclin
expression and increased cyclin-dependent kinase inhibitor steady
state mRNA levels. Moreover, propranolol treatment of the panel of
endothelial cells resulted in reduced proliferation rates and
increased percentages of cells in the G1 cell cycle phase. These
alterations were coincident with significant changes in the levels
of key cyclins and cell cycle inhibitors. Interestingly, of the
panel of MAPK proteins that we tested, we saw increased
phosphorylation only in p38, which is known to be responsive to
stress stimuli such as cytokines, irradiation and shock. p38 plays
a central role in inflammation and regulates the production of
inflammatory mediators such as TNFα, IL1β, and COX2 (43), thus it is possible that increased
p38 activation in propranolol-treated IHs may mediate IH regression
through immune-mediated responses. A number of studies suggest that
propranolol may induce apoptosis of HemECs. No caspase cleavage or
apoptosis was observed at the IC50 (∼50 μM) for
propranolol in HemECs or normal endothelial cells, although we did
begin to see lethal effects of this treatment in all three
endothelial cell lines at upwards of 150 μM. These findings do not
rule out that propranolol-induced IH apoptosis plays a role in the
efficacy of this treatment, but it does suggest that basic
endothelial functions such as proliferation and migration display
greater susceptibility to lower doses of propranolol than does
apoptosis. We demonstrated that propranolol treatment of HemECs
results in abolished stress fiber formation, and this effect may be
due in part to decreased levels of phosphorylated cofilin following
propranolol treatment. Cofilin is a cytoskeletal-binding protein
critical for actin microfilament dynamics and reorganization by
severing and depolymerizing actin filaments (44). Cofilin phosphorylation is an
inhibitory event (45), thus the
absence of stress fiber formation observed in propranolol-treated
HemECs may be due in part to increased cofilin-mediated actin
severing. This effect would certainly disrupt cell migration, and
as the actin cytoskeleton is intimately tied to the regulation of
cell cycle progression (46), may
indirectly contribute to propranolol induced decreased cell
proliferation.
As propranolol appears to work with great efficacy
against IHs, similar inhibitory effects could potentially be
observed in other vascular tumors such as angiosarcomas and
Kaposi’s sarcomas. Indeed, propranolol has been tested in
preclinical and clinical models of malignant tumors, demonstrating
good efficacy in the treatment of melanoma (47), pancreatic (48), colorectal (49) and breast (50) cancer. Finally, given the cutaneous
nature of IHs and the endothelial cell type-independent effects of
propranolol observed in our study, topical delivery of β blockers
(as opposed to systemic delivery) should be aggressively pursued. A
controlled study of topical administration of the β blocker timolol
on non-life threatening IHs revealed consistently good to moderate
responses in 91.5% of infants (51), suggesting this therapy could
specifically treat the lesion area while preventing potential
collateral anti-vascular effects on the normal endothelium.
Acknowledgements
Support of this study was provided by
a National Heart, Lung, and Blood Institute grant HL098931 and
TTUHSC startup funds to BAB, a National Institute of Arthritis and
Musculoskeletal and Skin Diseases grant (AR048564) to JB, a NASA
EPSCoR award to NMSU, and internal support from NMSU to LB.
References
|
1
|
Waner M, North PE, Scherer KA, Frieden IJ,
Waner A and Mihm MC Jr: The nonrandom distribution of facial
hemangiomas. Arch Dermatol. 139:869–875. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Léauté-Labrèze C, Dumas de la Roque E,
Hubiche T, Boralevi F, Thambo JB and Taïeb A: Propranolol for
severe hemangiomas of infancy. N Engl J Med. 358:2649–2651.
2008.PubMed/NCBI
|
|
3
|
D’Angelo G, Lee H and Weiner RI:
cAMP-dependent protein kinase inhibits the mitogenic action of
vascular endothelial growth factor and fibroblast growth factor in
capillary endothelial cells by blocking Raf activation. J Cell
Biochem. 67:353–366. 1997.
|
|
4
|
Sommers Smith SK and Smith DM: Beta
blockade induces apoptosis in cultured capillary endothelial cells.
In Vitro Cell Dev Biol Anim. 38:298–304. 2002.PubMed/NCBI
|
|
5
|
Lamy S, Lachambre MP, Lord-Dufour S and
Béliveau R: Propranolol suppresses angiogenesis in vitro:
inhibition of proliferation, migration, and differentiation of
endothelial cells. Vascul Pharmacol. 53:200–208. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Spindler V and Waschke J: Beta-adrenergic
stimulation contributes to maintenance of endothelial barrier
functions under baseline conditions. Microcirculation. 18:118–127.
2011. View Article : Google Scholar
|
|
7
|
Makarski JS: Stimulation of cyclic AMP
production by vasoactive agents in cultured bovine aortic and
pulmonary artery endothelial cells. In Vitro. 17:450–458. 1981.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Welles SL, Shepro D and Hechtman HB:
Vasoactive amines modulate actin cables (stress fibers) and surface
area in cultured bovine endothelium. J Cell Physiol. 123:337–342.
1985. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Brehm BR, Bertsch D, von Fallois J and
Wolf SC: Beta-blockers of the third generation inhibit endothelin-1
liberation, mRNA production and proliferation of human coronary
smooth muscle and endothelial cells. J Cardiovasc Pharmacol.
36(Suppl 1): S401–S403. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dai Y, Hou F, Buckmiller L, Fan CY, Saad
A, Suen J and Richter GT: Decreased eNOS protein expression in
involuting and propranolol-treated hemangiomas. Arch Otolaryngol
Head Neck Surg. 138:177–182. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chim H, Armijo BS, Miller E, Gliniak C,
Serret MA and Gosain AK: Propranolol induces regression of
hemangioma cells through HIF-1alpha-mediated inhibition of VEGF-A.
Ann Surg. 256:146–156. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Boye E, Yu Y, Paranya G, Mulliken JB,
Olsen BR and Bischoff J: Clonality and altered behavior of
endothelial cells from hemangiomas. J Clin Invest. 107:745–752.
2001. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lichtenstein N, Geiger B and Kam Z:
Quantitative analysis of cytoskeletal organization by digital
fluorescent microscopy. Cytometry A. 54:8–18. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Howell RE, Albelda SM, Daise ML and Levine
EM: Characterization of beta-adrenergic receptors in cultured human
and bovine endothelial cells. J Appl Physiol. 65:1251–1257.
1988.PubMed/NCBI
|
|
15
|
Jinnin M, Medici D, Park L, Limaye N, Liu
Y, Boscolo E, Bischoff J, Vikkula M, Boye E and Olsen BR:
Suppressed NFAT-dependent VEGFR1 expression and constitutive VEGFR2
signaling in infantile hemangioma. Nat Med. 14:1236–1246. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Souza BR, Santos JS and Costa AM: Blockade
of beta1- and beta2-adrenoceptors delays wound contraction and
re-epithelialization in rats. Clin Exp Pharmacol Physiol.
33:421–430. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Romana-Souza B, Santos JS and
Monte-Alto-Costa A: beta-1 and beta-2, but not alpha-1 and alpha-2,
adrenoceptor blockade delays rat cutaneous wound healing. Wound
Repair Regen. 17:230–239. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Romana-Souza B, Porto LC and
Monte-Alto-Costa A: Cutaneous wound healing of chronically stressed
mice is improved through catecholamine blockade. Exp Dermatol.
19:821–829. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Romana-Souza B, Otranto M, Vieira AM,
Filgueiras CC, Fierro IM and Monte-Alto-Costa A: Rotational
stress-induced increase in epinephrine levels delays cutaneous
wound healing in mice. Brain Behav Immun. 24:427–437. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Romana-Souza B, Nascimento AP and
Monte-Alto-Costa A: Propranolol improves cutaneous wound healing in
streptozotocin-induced diabetic rats. Eur J Pharmacol. 611:77–84.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Romana-Souza B, Nascimento AP and
Monte-Alto-Costa A: Low-dose propranolol improves cutaneous wound
healing of burn-injured rats. Plast Reconstr Surg. 122:1690–1699.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mohammadi AA, Bakhshaeekia A, Alibeigi P,
Hasheminasab MJ, Tolide-ei HR, Tavakkolian AR and Mohammadi MK:
Efficacy of propranolol in wound healing for hospitalized burn
patients. J Burn Care Res. 30:1013–1017. 2009.PubMed/NCBI
|
|
23
|
Musumeci M, Maccari S, Sestili P, Signore
M, Molinari P, Ambrosio C, Stati T, Colledge WH, Grace AA, Catalano
L and Marano G: Propranolol enhances cell cycle-related gene
expression in pressure overloaded hearts. Br J Pharmacol.
164:1917–1928. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Erraji-Benchekroun L, Couton D, Postic C,
Borde I, Gaston J, Guillet JG and André C: Overexpression of
beta2-adrenergic receptors in mouse liver alters the expression of
gluconeogenic and glycolytic enzymes. Am J Physiol Endocrinol
Metab. 288:E715–E722. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Patrizio M, Musumeci M, Stati T, Fecchi K,
Mattei E, Catalano L and Marano G: Propranolol promotes Egr1 gene
expression in cardiomyocytes via beta-adrenoceptors. Eur J
Pharmacol. 587:85–89. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lashbrook BL and Steinle JJ:
Beta-adrenergic receptor regulation of pigment epithelial-derived
factor expression in rat retina. Auton Neurosci. 121:33–39. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Haggstrom AN, Beaumont JL, Lai JS, Adams
DM, Drolet BA, Frieden IJ, Garzon MC, Holland KE, Horii KA, Lucky
AW, et al: Measuring the severity of infantile hemangiomas:
instrument development and reliability. Arch Dermatol. 148:197–202.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Boye E and Olsen BR: Signaling mechanisms
in infantile hemangioma. Curr Opin Hematol. 16:202–208. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Grimmer JF, Williams MS, Pimentel R,
Mineau G, Wood GM, Bayrak-Toydemir P and Stevenson DA: Familial
clustering of hemangiomas. Arch Otolaryngol Head Neck Surg.
137:757–760. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Khan ZA, Boscolo E, Picard A, Psutka S,
Melero-Martin JM, Bartch TC, Mulliken JB and Bischoff J:
Multipotential stem cells recapitulate human infantile hemangioma
in immunodeficient mice. J Clin Invest. 118:2592–2599.
2008.PubMed/NCBI
|
|
31
|
Calicchio ML, Collins T and Kozakewich HP:
Identification of signaling systems in proliferating and involuting
phase infantile hemangiomas by genome-wide transcriptional
profiling. Am J Pathol. 174:1638–1649. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Iaccarino G, Ciccarelli M, Sorriento D,
Galasso G, Campanile A, Santulli G, Cipolletta E, Cerullo V, Cimini
V, Altobelli GG, et al: Ischemic neoangiogenesis enhanced by
beta2-adrenergic receptor overexpression: a novel role for the
endothelial adrenergic system. Circ Res. 97:1182–1189. 2005.
View Article : Google Scholar
|
|
33
|
Storch CH and Hoeger PH: Propranolol for
infantile haemangiomas: insights into the molecular mechanisms of
action. Br J Dermatol. 163:269–274. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Fredriksson JM, Lindquist JM, Bronnikov GE
and Nedergaard J: Norepinephrine induces vascular endothelial
growth factor gene expression in brown adipocytes through a
beta-adrenoreceptor/cAMP/protein kinase A pathway involving Src but
independently of Erk1/2. J Biol Chem. 275:13802–13811. 2000.
View Article : Google Scholar
|
|
35
|
Taylor MR: Pharmacogenetics of the human
beta-adrenergic receptors. Pharmacogenomics J. 7:29–37. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Rohrer DK, Chruscinski A, Schauble EH,
Bernstein D and Kobilka BK: Cardiovascular and metabolic
alterations in mice lacking both beta1- and beta2-adrenergic
receptors. J Biol Chem. 274:16701–16708. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Krief S, Lönnqvist F, Raimbault S, Baude
B, Van Spronsen A, Arner P, Strosberg AD, Ricquier D and Emorine
LJ: Tissue distribution of beta 3-adrenergic receptor mRNA in man.
J Clin Invest. 91:344–349. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Yuan SM, Jiang HQ, Ouyang TX and Xing X:
The distribution and evolution of pericytes in infantile
hemangioma. Zhonghua Zheng Xing Wai Ke Za Zhi. 23:322–324. 2007.(In
Chinese).
|
|
39
|
Ferrari-Dileo G, Davis EB and Anderson DR:
Effects of cholinergic and adrenergic agonists on adenylate cyclase
activity of retinal microvascular pericytes in culture. Invest
Ophthalmol Vis Sci. 33:42–47. 1992.
|
|
40
|
Siegfried EC, Keenan WJ and Al-Jureidini
S: More on propranolol for hemangiomas of infancy. N Engl J Med.
359:2846author reply 2846–2847, 2008.
|
|
41
|
Thaker PH, Han LY, Kamat AA, Arevalo JM,
Takahashi R, Lu C, Jennings NB, Armaiz-Pena G, Bankson JA, Ravoori
M, et al: Chronic stress promotes tumor growth and angiogenesis in
a mouse model of ovarian carcinoma. Nat Med. 12:939–944. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Yang H, Xu Z, Iuvone PM and Grossniklaus
HE: Angiostatin decreases cell migration and vascular endothelium
growth factor (VEGF) to pigment epithelium derived factor (PEDF)
RNA ratio in vitro and in a murine ocular melanoma model. Mol Vis.
12:511–517. 2006.
|
|
43
|
Schieven GL: The biology of p38 kinase: a
central role in inflammation. Curr Top Med Chem. 5:921–928. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Bamburg JR and Wiggan OP: ADF/cofilin and
actin dynamics in disease. Trends Cell Biol. 12:598–605. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Arber S, Barbayannis FA, Hanser H,
Schneider C, Stanyon CA, Bernard O and Caroni P: Regulation of
actin dynamics through phosphorylation of cofilin by LIM-kinase.
Nature. 393:805–809. 1998. View
Article : Google Scholar : PubMed/NCBI
|
|
46
|
Street CA and Bryan BA: Rho kinase
proteins – pleiotropic modulators of cell survival and apoptosis.
Anticancer Res. 31:3645–3657. 2011.
|
|
47
|
De Giorgi V, Gandini S, Grazzini M,
Benemei S, Marchionni N and Geppetti P: Beta-blockers: a new and
emerging treatment for melanoma. Recenti Prog Med. 103:11–16.
2012.(In Italian).
|
|
48
|
Lin X, Luo K, Lv Z and Huang J:
Beta-adrenoceptor action on pancreatic cancer cell proliferation
and tumor growth in mice. Hepatogastroenterology. 59:584–588.
2012.PubMed/NCBI
|
|
49
|
Jansen L, Below J, Chang-Claude J, Brenner
H and Hoffmeister M: Beta blocker use and colorectal cancer risk:
Population-based case-control study. Cancer. May 14–2012.(Epub
ahead of print).
|
|
50
|
Pérez Piñero C, Bruzzone A, Sarappa MG,
Castillo LF and Lüthy IA: Involvement of alpha2- and
beta2-adrenoceptors on breast cancer cell proliferation and tumour
growth regulation. Br J Pharmacol. 166:721–736. 2012.PubMed/NCBI
|
|
51
|
Chambers CB, Katowitz WR, Katowitz JA and
Binenbaum G: A controlled study of topical 0.25% timolol maleate
gel for the treatment of cutaneous infantile capillary hemangiomas.
Ophthal Plast Reconstr Surg. 28:103–106. 2012.
|