Introduction
Multiple myeloma (MM) is a B cell
lymphoproliferative disorder characterized by monoclonal
proliferation of plasma cells with overproduction of a specific
monoclonal antibody (1).
Symptomatic MM patients usually present with at least one of the
following complications: anemia, hypercalcemia, renal insufficiency
or bone lesions. Anemia may be the most common single clinical
feature of MM, being present in appoximately 73% of patients at
diagnosis (2). The anemia in
patients with MM is usually normocytic and normochromic, with
normal to high serum iron levels and high serum ferritin levels
(3).
The main mediator of anemia in patients with chronic
disease is considered to be the regulatory hormone, hepcidin.
Hepcidin, an antimicrobial peptide (4), is produced predominantly by
hepatocytes (5). Cleavage of the
signal peptide from the hepcidin precursor protein yields the 60
amino acid prohepcidin molecule. The biologically active 25 amino
acid hepcidin molecule is generated by the removal of the proregion
by the prohormone convertase furin and other members of the furin
family (6). Mature hepcidin
regulates iron absorption and distribution by binding to
ferroportin, which is the exporter of iron in enterocytes and
macrophages (7). Hepcidin assays
based on mass spectroscopic techniques (8,9) or
immunoassays (10–12) have been developed, and ELISA is
available to measure serum levels of prohepcidin (13). However, there is no consensus on
which are the best assays for measuring hepcidin levels and it has
not been confirmed whether serum prohepcidin accurately reflects
active hepcidin levels.
Hepcidin synthesis is markedly increased by
infection and inflammation (14–16),
and these effects are mediated by inflammatory cytokines, including
interleukin (IL)-1 and IL-6 (16,17).
IL-6 levels are increased in MM (18). Hepcidin is also reported to be
upregulated in MM patients by IL-6-dependent and -independent
mechanisms, and may play a role in the development of anemia
(19). However, the associations
between serum prohepcidin and inflammation or iron metabolism are
controversial (14,20–22),
and the clinical significance of prohepcidin levels in MM patients
is not fully understood. In this study, we analyzed serum
prohepcidin levels to determine its significance in patients with
MM.
Materials and methods
Patients
A total of 39 patients with clinical Durie-Salmon
stage II or III MM (23) (mean
age, 66.7±10.9 years; 22 males, 17 females) were enrolled in this
retrospective study (Table I). All
patients were newly diagnosed prior to receiving chemotherapy
between April 2000 and May 2008. The clinical stage of patients
according to the Durie-Salmon Staging System and the International
Staging System (ISS) (24) are
shown in Table I. The prognostic
indicators of MM (24), including
age, platelet count, bone marrow plasma cell percentage, serum
levels of hemoglobin, lactate dehydrogenase (LDH), creatinine,
calcium, albumin, serum β2-microglobulin (sβ2M) and Eastern
Cooperative Oncology Group (ECOG) performance status at diagnosis
were examined. Creatinine clearance (CCr) and estimated glomerular
filtration rate (eGFR) were also examined. Eighteen healthy
subjects were enrolled as normal controls in the present study
(mean age, 51.9±10.4 years; 14 males, 4 females; mean CCr,
82.7±17.5 ml/min; range of CCr, 61.0–129.0). Prognosis was assessed
by the overall survival. The endpoint was considered as mortality,
the last available follow-up date or September 30, 2008. This study
was approved by the ethics committees of Kagoshima University
Medical and Dental Hospital, and National Hospital Organization
Kagoshima Medical Center (Kagoshima, Japan).
 | Table ICharacteristics of the patients with
multiple myeloma and healthy controls. |
Table I
Characteristics of the patients with
multiple myeloma and healthy controls.
| Variable | Multiple myeloma | Control |
|---|
| n | 39 | 18 |
| Age (years), mean ±
SD | 66.7±10.9 | 51.9±10.4 |
| Age range
(years) | 43–85 | 30–67 |
| Gender
(male/female) | 22/17 | 14/4 |
| Immunoglobulin
isotype | | |
| IgG | 23 | |
| IgA | 11 | |
| IgD | 1 | |
| BJP | 4 | |
| Clinical stage | | |
| Durie-Salmon | | |
| II | 7 | |
| III | 32 | |
| ISS | | |
| I | 15 | |
| II | 11 | |
| III | 13 | |
Serum prohepcidin, IL-1β, IL-6 and tumor
necrosis factor (TNF)-α measurement
The serum prohepcidin concentrations were determined
by ELISA using a commercially available kit (DRG Instruments,
Marburg, Germany) according to the manufacturer’s instructions. The
lower detection limit of this assay was 3.95 ng/ml.
The levels of IL-1β, IL-6 and TNF-α in available
serum samples were measured with ELISA kits (R&D Systems,
Minneapolis, MN, USA), with lower limits of detection at 3.9 pg/ml,
3.13 pg/ml and 15.6 pg/ml, respectively.
Statistical analysis
The values are expressed as means ± SD. The
differences between groups were analyzed with the Mann-Whitney U
test and the correlations between continuous variables were
calculated by Spearman’s rank correlation. The Kaplan-Meier method
was used to estimate survival and the log-rank test was used to
compare the groups for differences in prognoses. Survival durations
were measured between the date when chemotherapy was initiated and
the endpoint. The stepwise Cox proportional hazards model was used
in the multivariate analyses. P<0.05 was considered to indicate
a statistically significant result. Statistical analysis was
performed using SPSS, version 12.0 (SPSS Inc., Chicago, IL,
USA).
Results
Serum prohepcidin levels in MM
patients
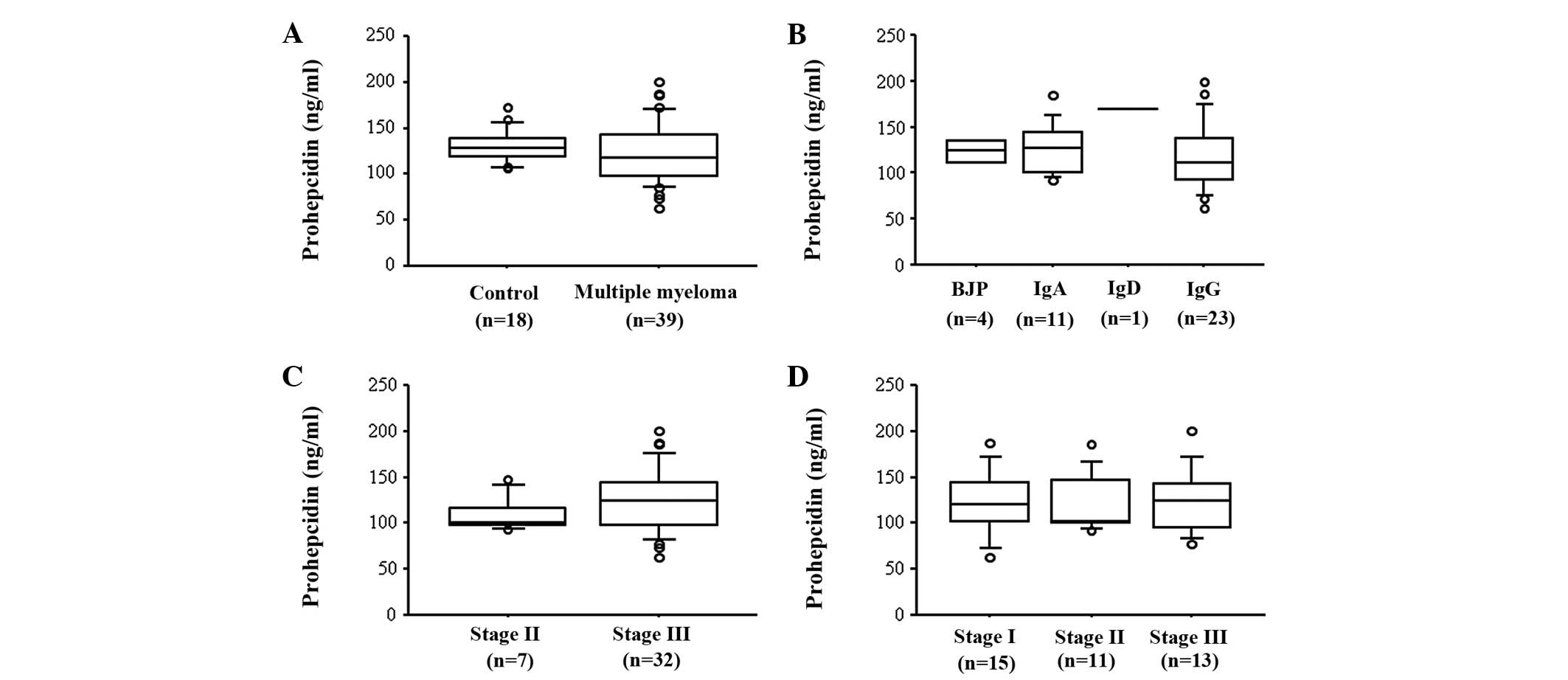
The serum level of prohepcidin did not differ
significantly between patients at the time of diagnosis of MM and
normal controls (121.3±32.4 vs. 130.8±17.8 ng/ml, P= 0.11; Fig. 1A). However, patients with mild or
no renal insufficiency (CCr ≥50 ml/min) had significantly lower
prohepcidin levels (116.1±31.2 ng/ml) when compared to healthy
subjects (P=0.03). In addition, serum prohepcidin levels were not
associated with the immunoglobulin isotype, Durie-Salmon stage or
ISS stage (Fig. 1B, C and D).
Correlation between serum prohepcidin
levels and laboratory parameters
The serum prohepcidin levels were weakly correlated
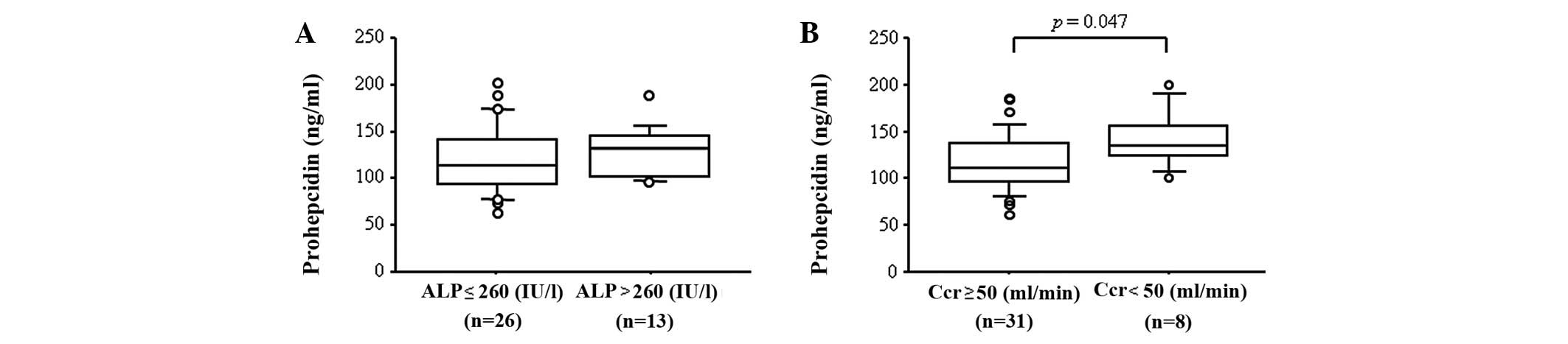
with alkaline phosphatase (ALP; r=0.32, P=0.048; Table II). However, serum prohepcidin
levels in patients in the abnormal ALP (>260 IU/l) group were
similar when compared to patients in the normal ALP (≤260 IU/l)
group (P=0.26, Fig. 2A). By
contrast, although there was no correlation between prohepcidin
levels and parameters of renal function, including blood urea
nitrogen, creatinine, CCr or eGFR (Table II), patients with severe renal
insufficiency (CCr <50 ml/min) had significantly higher
prohepcidin levels when compared to patients with mild or no renal
insufficiency (CCr ≥50 ml/min, P=0.047, Fig. 2B). These results indicate that
serum prohepcidin levels were associated with ALP and renal
function, but that these associations were weak. In addition, there
was no correlation between prohepcidin levels and the percentage of
bone marrow plasma cells, red blood cell count, hemoglobin,
hematocrit, platelet count, serum levels of iron, ferritin,
asparate aminotransferase (AST), alanine aminotransferase (ALT),
LDH, uric acid, C-reactive protein, calcium, albumin and sβ2M
(Table II). No correlation between
levels of prohepcidin and serum cytokines, including IL-1β, IL-6
and TNF-α, was observed (Table
II).
| Table IICorrelation between serum prohepcidin
and laboratory parameters. |
Table II
Correlation between serum prohepcidin
and laboratory parameters.
| Variable | Correlation
coefficient | P-value |
|---|
| Red blood cell
count | 0.22 | 0.19 |
| Hemoglobin | 0.07 | 0.67 |
| Hematocrit | 0.10 | 0.53 |
| Platelet count | 0.15 | 0.36 |
| Serum iron | −0.31 | 0.06 |
| Ferritin | 0.04 | 0.82 |
| AST | −0.07 | 0.68 |
| ALT | −0.10 | 0.55 |
| ALP | 0.32 | 0.048 |
| Blood urea
nitrogen | 0.24 | 0.15 |
| Creatinine | 0.20 | 0.22 |
| Uric acid | 0.15 | 0.36 |
| CCr | −0.23 | 0.16 |
| eGFR | −0.25 | 0.13 |
| CRP | 0.11 | 0.49 |
| Bone marrow plasma
cells (%) | −0.02 | 0.91 |
| Calcium | −0.07 | 0.67 |
| Albumin | 0.18 | 0.28 |
| Sβ2M | 0.02 | 0.92 |
| IL-6 | 0.15 | 0.37 |
| TNF-α | 0.07 | 0.70 |
| IL-1β | −0.02 | 0.91 |
Relevance of serum prohepcidin levels to
prognosis
The median follow-up among MM patients was 14.9
months (range, 0.9–71.5) and 19 of 39 patient mortalities occurred
due to disease progression. To study the correlation between the
prohepcidin level at diagnosis and the duration of survival, we
divided the 39 MM patients into two groups according to prohepcidin
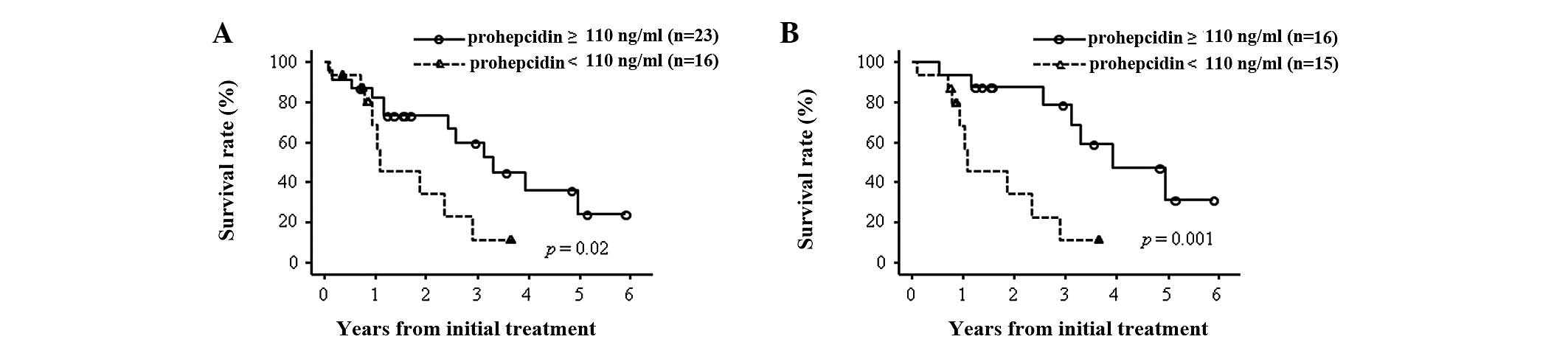
levels and compared the survival rates. We designated patients as
high-prohepcidin when the prohepcidin level was higher than 110
ng/ml, corresponding to one SD below the mean in normal controls,
and low-prohepcidin when it was lower than 110 ng/ml. The overall
survival of the 16 low-prohepcidin patients was significantly
shorter than that of the 23 high-prohepcidin patients (median, 26.9
vs. 51.1 months, P=0.02; Fig.
3A).
We subsequently investigated whether prohepcidin was
an independent prognostic factor in MM. A Cox proportional hazards
model using established prognostic factors (24), along with levels of prohepcidin and
several cytokines, including IL-1β, IL-6 and TNF-α, was generated.
In the univariate analysis, platelet count, and serum levels of
creatinine,serum calcium, sβ2M, performance status and prohepcidin
were significant prognostic factors (Table III). In addition, a multivariate
analysis showed that serum creatinine (HR, 5.32; 95% CI,
1.10–25.64), serum calcium (HR, 3.53; 95% CI, 1.01–12.33),
performance status (HR, 4.15; 95% CI, 1.32–13.09) and serum
prohepcidin (HR, 5.29; 95% CI, 1.65–17.03) were significant
prognostic factors (Table III). We
investigated whether prohepcidin was an independent prognostic
factor for MM among the 31 patients with CCr ≥50 ml/min. The
overall survival of the 15 low-prohepcidin patients with CCr ≥50
ml/min was significantly poorer than that of the 16
high-prohepcidin patients with CCr ≥50 ml/min (median, 26.9 vs.
92.3 months, P=0.001; Fig. 3B).
Univariate analysis showed that platelet count, serum calcium, sβ2M
and prohepcidin were significant prognostic factors. A multivariate
analysis also showed that serum prohepcidin (HR, 5.65; 95% CI,
1.60–19.95) was a significant prognostic factor (Table IV).
| Table IIISurvival analysis in all multiple
myeloma patients by Cox proportional hazards model. |
Table III
Survival analysis in all multiple
myeloma patients by Cox proportional hazards model.
| | Univariate
| Multivariate
|
|---|
| n | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age (years) | | | | | | | |
| <65 | 16 | | | | | | |
| ≥65 | 23 | 1.43 | 0.56–3.69 | 0.46 | | | |
| Hemoglobin
(g/dl) | | | | | | | |
| ≥10 | 18 | | | | | | |
| <10 | 21 | 2.32 | 0.90–6.02 | 0.08 | | | |
| Platelet
(/μl) | | | | | | | |
| ≥130,000 | 30 | | | | | | |
| <130,000 | 9 | 4.02 | 1.37–11.82 | 0.01 | | | |
| LDH | | | | | | | |
| normal | 31 | | | | | | |
| abnormal | 8 | 2.43 | 0.64–9.21 | 0.19 | | | |
| ALP (IU/l) | | | | | | | |
| ≤260 | 26 | | | | | | |
| >260 | 13 | 0.84 | 0.30–2.36 | 0.74 | | | |
| Creatinine
(mg/dl) | | | | | | | |
| <2 | 34 | | | | | | |
| ≥2 | 5 | 4.29 | 1.14–16.18 | 0.03 | 5.32 | 1.10–25.64 | 0.02 |
| Calcium
(mg/dl) | | | | | | | |
| <10 | 32 | | | | | | |
| ≥10 | 7 | 3.33 | 1.10–10.10 | 0.03 | 3.53 | 1.01–12.33 | 0.048 |
| Albumin (g/dl) | | | | | | | |
| ≥3.5 | 32 | | | | | | |
| <3.5 | 7 | 1.90 | 0.65–5.49 | 0.24 | | | |
| Bone marrow plasma
cells (%) | | | | | | | |
| <33 | 17 | | | | | | |
| ≥33 | 22 | 2.39 | 0.89–6.41 | 0.08 | | | |
| Sβ2M (mg/l) | | | | | | | |
| <3.5 | 18 | | | | | | |
| ≥3.5 | 21 | 3.27 | 1.19–8.93 | 0.02 | | | |
| Performance
status | | | | | | | |
| 1–3 | 34 | | | | | | |
| 4 | 5 | 5.66 | 1.83–17.50 | <0.001 | 4.15 | 1.32–13.09 | 0.02 |
| Prohepcidin
(ng/ml) | | | | | | | |
| ≥110 | 23 | | | | | | |
| <110 | 16 | 3.18 | 1.18–8.55 | 0.02 | 5.29 | 1.65–17.03 | 0.01 |
| IL-6 (pg/ml) | | | | | | | |
| <4 | 18 | | | | | | |
| ≥4 | 19 | 1.58 | 0.61–4.09 | 0.35 | | | |
| TNF-α (pg/ml) | | | | | | | |
| <15.6 | 25 | | | | | | |
| ≥15.6 | 11 | 0.86 | 0.32–2.31 | 0.77 | | | |
| IL-1β (pg/ml) | | | | | | | |
| <10 | 31 | | | | | | |
| ≥10 | 1 | 7.07 | 0.79–63.29 | 0.08 | | | |
| Table IVSurvival analysis in multilpe myeloma
patients without severe renal insufficiency by Cox proportional
hazards model. |
Table IV
Survival analysis in multilpe myeloma
patients without severe renal insufficiency by Cox proportional
hazards model.
| | Univariate
| Multivariate
|
|---|
| n | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age (years) | | | | | | | |
| <65 | 14 | | | | | | |
| ≥65 | 17 | 1.76 | 0.60–5.16 | 0.31 | | | |
| Hemoglobin
(g/dl) | | | | | | | |
| ≥10 | 18 | | | | | | |
| <10 | 13 | 2.01 | 0.72–5.60 | 0.18 | | | |
| Platelet count
(/μl) | | | | | | | |
| ≥130,000 | 26 | | | | | | |
| <130,000 | 5 | 5.33 | 1.38–20.55 | 0.02 | | | |
| LDH | | | | | | | |
| normal | 27 | | | | | | |
| abnormal | 4 | 4.23 | 0.83–21.53 | 0.08 | | | |
| ALP (IU/l) | | | | | | | |
| ≤260 | 21 | | | | | | |
| >260 | 10 | 0.97 | 0.30–3.09 | 0.95 | | | |
| Calcium
(mg/dl) | | | | | | | |
| <10 | 28 | | | | | | |
| ≥10 | 3 | 6.61 | 1.19–36.81 | 0.03 | 3.63 | 0.65–20.26 | 0.14 |
| Albumin (g/dl) | | | | | | | |
| ≥3.5 | 27 | | | | | | |
| <3.5 | 4 | 1.87 | 0.50–6.94 | 0.35 | | | |
| Bone marrow plasma
cells (%) | | | | | | | |
| <33 | 15 | | | | | | |
| ≥33 | 16 | 2.29 | 0.76–6.86 | 0.14 | | | |
| Sβ2M (mg/l) | | | | | | | |
| <3.5 | 18 | | | | | | |
| ≥3.5 | 13 | 2.98 | 1.02–8.74 | 0.046 | | | |
| Performance
status | | | | | | | |
| 1–3 | 29 | | | | | | |
| 4 | 2 | 4.49 | 0.93–21.72 | 0.06 | | | |
| Prohepcidin
(ng/ml) | | | | | | | |
| ≥110 | 16 | | | | | | |
| <110 | 15 | 6.24 | 1.82–21.35 | 0.004 | 5.65 | 1.60–19.95 | 0.01 |
| IL-6 (pg/ml) | | | | | | | |
| <4 | 15 | | | | | | |
| ≥4 | 14 | 1.29 | 0.44–3.76 | 0.64 | | | |
| TNF-α (pg/ml) | | | | | | | |
| <15.6 | 18 | | | | | | |
| ≥15.6 | 10 | 0.78 | 0.26–2.30 | 0.65 | | | |
| IL-1β (pg/ml) | | | | | | | |
| <10 | 23 | | | | | | |
| ≥10 | 1 | 10.99 | 1.00–121.24 | 0.05 | | | |
Discussion
Hepcidin regulates intestinal iron absorption and
the release of iron from hepatic stores and from macrophages
involved in the recycling of iron from hemoglobin (5). Hepcidin may also play a role in the
anemia of patients with MM (19).
However, the clinical significance of prohepcidin, the pro-hormone
form of hepcidin, has not been elucidated in patients with MM. In
this study, serum prohepcidin levels in MM patients were neither
correlated with serum iron nor ferritin levels, but appeared to be
associated with ALP levels and renal insufficiency (Table II and Fig. 2B). In contrast, low serum
prohepcidin levels were independently associated with a poorer
prognosis as compared to high serum prohepcidin levels in MM
patients regardless of renal insufficiency. Although the sample
size was insufficient, our study is the first to elucidate the
clinical significance of serum prohepcidin levels in patients with
MM.
Serum prohepcidin levels are not correlated with
iron absorption in healthy individuals (25,26).
Young et al reported that there was no significant
correlation between serum hepcidin and serum prohepcidin levels in
healthy women and that prohepcidin was not correlated with iron
status (27). In addition, IL-6
was markedly increased within 3 h after injection of
lipopolysaccharide (LPS), which is considered to be an upstream
activator of inflammation in healthy individuals, and urinary
hepcidin peaked within 6 h, followed by a significant decrease in
serum iron (14). However, there
were no significant changes in serum prohepcidin levels within a
22-h time frame in that study of healthy individuals (14). In MM patients with anemia, urinary,
or serum hepcidin was positively correlated with serum ferritin and
negatively with hemoglobin (19,28,29).
By contrast, serum prohepcidin was not correlated with serum iron
and ferritin in our subjects. These findings suggest that, similar
to in healthy individuals, serum prohepcidin levels are not
associated with serum hepcidin levels in MM patients, although
urinary or serum hepcidin levels were not determined in the present
study.
Hepcidin is specifically synthesized in the liver as
an 84 amino acid prepropeptide and processed to its mature form in
hepatocytes (30). It was reported
that posttranslational processing of hepcidin in hepatocytes is
mediated by the prohormone convertase furin, and the inhibition of
furin activity prevents the conversion of prohepcidin to hepcidin,
but does not inhibit its release from the cell (6). Serum prohepcidin levels in patients
with chronic hepatitis C were positively correlated with serum
ferritin (21) and IL-6 (20) levels. These results may indicate a
positive correlation between serum prohepcidin and serum hepcidin
levels in patients with chronic hepatitis C. By contrast, there was
a negative correlation between serum prohepcidin and serum hepcidin
levels in patients with inflammatory bowel disease (IBD) by
univariate analysis (31). These
conflicting results may indicate that the role of prohepcidin may
differ in various diseases, including chronic hepatitis C, IBD and
MM. The serum levels of prohepcidin and hepcidin, the expression of
converting enzyme and iron status in each disease, including MM,
should be further analyzed.
In the present study, serum prohepcidin levels were
weakly associated with renal function as assessed by CCr, with
significantly higher prohepcidin levels observed in patients with
severe renal insufficiency (CCr <50 ml/min) when compared to
patients with mild or no renal insufficiency (P= 0.047; Fig. 2B). Kulaksiz et al reported
that in chronic renal insufficiency prohepcidin levels were
significantly increased when compared with those in healthy
controls, suggesting that the kidney may be involved in the
metabolism or elimination of prohepcidin (13). Taes et al also reported that
increased serum prohepcidin concentrations were observed with
declining kidney function (32).
These results suggest that renal function is one influencing factor
on serum prohepcidin levels in the patients with MM in the present
study, although this effect may be small in our study
population.
The overall survival of the low-prohepcidin group
was poorer than that of the high-prohepcidin group (Fig. 3A, Table III). Renal insufficiency is a known
prognostic factor in MM (24) and
the overall survival of the group with severe renal insufficiency
(creatinine ≥2 mg/dl) in our study was also poorer (Table III). Prohepcidin levels may be
inversely correlated with renal function (Table II) and the prohepcidin levels in
the group of MM patients with severe renal insufficiency were
significantly higher than those in the groups with mild or no renal
insufficiency (Fig. 2B). In
addition, seven out of eight patients with severe renal
insufficiency (CCr <50 ml/min) were included in the
high-prohepcidin group. When patients with severe renal
insufficiency were excluded, the difference in overall survival
between the high-prohepcidin group and low-prohepcidin group became
more pronounced (Fig. 3B,
P=0.001). Thus, although renal function should be considered in
order to analyze the association between prohepcidin levels and
overall survival, our results indicate that the poor prognosis of
the low-prohepcidin patients group does not depend on renal
insufficiency. The mechanism leading to a poor prognosis in
patients with normal renal function and lower prohepcidin levels
should be further examined.
In the present study, levels of prohepcidin and ALP,
a known prognostic factor in MM (33), were correlated (Table II). This result is not consistent
with lower prohepcidin levels being a poor prognostic factor in MM.
In addition, we could not demonstrate any correlation between serum
levels of prohepcidin and IL-6, TNF-α or IL-1β. Serum IL-6 is
elevated in MM (18) and hepcidin
mRNA was reportedly upregulated by IL-6 (16,17).
The hepatic IL-6/STAT3 signal has a role in anemia of inflammation
in vivo (34). IL-6 levels
have also been reported as a prognostic factor in MM (18). However, levels of prohepcidin were
not associated with IL-6, and IL-6 was not associated with
prognosis in the present study. We suggest that expression of
prohepcidin may not be regulated by these cytokines in MM and it is
possible that serum levels of prohepcidin are more useful to
prognosis than those of inflammatory cytokines or ALP in MM.
In conclusion, iron homeostasis may not affect serum
prohepcidin levels in MM patients, but serum prohepcidin levels
were weakly correlated with renal function and ALP. In addition,
low serum prohepcidin may be an indicator for poor prognosis in MM
patients regardless of their degree of renal function.
Acknowledgements
We thank Ms. Ayaka Hamabe for the
technical assistance.
References
|
1
|
Vanderkerken K, Asosingh K, Croucher P and
Van Camp B: Multiple myeloma biology: lessons from the 5TMM models.
Immunol Rev. 194:196–206. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Palumbo A and Anderson K: Multiple
myeloma. N Engl J Med. 364:1046–1060. 2011. View Article : Google Scholar
|
|
3
|
Kyle RA, Gertz MA, Witzig TE, Lust JA,
Lacy MQ, Dispenzieri A, Fonseca R, Rajkumar SV, Offord JR, Larson
DR, et al: Review of 1027 patients with newly diagnosed multiple
myeloma. Mayo Clin Proc. 78:21–33. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Krause A, Neitz S, Mägert HJ, Schulz A,
Forssmann WG, Schulz-Knappe P and Adermann K: LEAP-1, a novel
highly disulfide-bonded human peptide, exhibits antimicrobial
activity. FEBS Lett. 480:147–150. 2000.
|
|
5
|
Nemeth E and Ganz T: Regulation of iron
metabolism by hepcidin. Annu Rev Nutr. 26:323–342. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Valore EV and Ganz T: Posttranslational
processing of hepcidin in human hepatocytes is mediated by the
prohormone convertase furin. Blood Cells Mol Dis. 40:132–138. 2008.
View Article : Google Scholar
|
|
7
|
Nemeth E, Tuttle MS, Powelson J, Vaughn
MB, Donovan A, Ward DM, Ganz T and Kaplan J: Hepcidin regulates
cellular iron efflux by binding to ferroportin and inducing its
internalization. Science. 306:2090–2093. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tomosugi N, Kawabata H, Wakatabe R,
Higuchi M, Yamaya H, Umehara H and Ishikawa I: Detection of serum
hepcidin in renal failure and inflammation by using ProteinChip
System. Blood. 108:1381–1387. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kemna E, Tjalsma H, Laarakkers C, Nemeth
E, Willems H and Swinkels D: Novel urine hepcidin assay by mass
spectrometry. Blood. 106:3268–3270. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ganz T, Olbina G, Girelli D, Nemeth E and
Westerman M: Immunoassay for human serum hepcidin. Blood.
112:4292–4297. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ashby DR, Gale DP, Busbridge M, Murphy KG,
Duncan ND, Cairns TD, Taube DH, Bloom SR, Tam FW, Chapman RS, et
al: Plasma hepcidin levels are elevated but responsive to
erythropoietin therapy in renal disease. Kidney Int. 75:976–981.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schwarz P, Strnad P, von Figura G,
Janetzko A, Krayenbühl P, Adler G and Kulaksiz H: A novel
monoclonal antibody immunoassay for the detection of human serum
hepcidin. J Gastroenterol. 46:648–656. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kulaksiz H, Gehrke SG, Janetzko A, Rost D,
Bruckner T, Kallinowski B and Stremmel W: Pro-hepcidin: expression
and cell specific localisation in the liver and its regulation in
hereditary haemochromatosis, chronic renal insufficiency, and renal
anaemia. Gut. 53:735–743. 2004. View Article : Google Scholar
|
|
14
|
Kemna E, Pickkers P, Nemeth E, van der
Hoeven H and Swinkels D: Time-course analysis of hepcidin, serum
iron, and plasma cytokine levels in humans injected with LPS.
Blood. 106:1864–1866. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nemeth E, Valore EV, Territo M, Schiller
G, Lichtenstein A and Ganz T: Hepcidin, a putative mediator of
anemia of inflammation, is a type II acute-phase protein. Blood.
101:2461–2463. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Nemeth E, Rivera S, Gabayan V, Keller C,
Taudorf S, Pedersen BK and Ganz T: IL-6 mediates hypoferremia of
inflammation by inducing the synthesis of the iron regulatory
hormone hepcidin. J Clin Invest. 113:1271–1276. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee P, Peng H, Gelbart T, Wang L and
Beutler E: Regulation of hepcidin transcription by interleukin-1
and interleukin-6. Proc Natl Acad Sci USA. 102:1906–1910. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pelliniemi TT, Irjala K, Mattila K, Pulkki
K, Rajamäki A, Tienhaara A, Laakso M and Lahtinen R: Immunoreactive
interleukin-6 and acute phase proteins as prognostic factors in
multiple myeloma. Finnish Leukemia Group Blood. 85:765–771.
1995.PubMed/NCBI
|
|
19
|
Sharma S, Nemeth E, Chen YH, Goodnough J,
Huston A, Roodman GD, Ganz T and Lichtenstein A: Involvement of
hepcidin in the anemia of multiple myeloma. Clin Cancer Res.
14:3262–3267. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lee SH, Jeong SH, Park YS, Hwang JH, Kim
JW, Kim N and Lee DH: Serum prohepcidin levels in chronic hepatitis
C, alcoholic liver disease, and nonalcoholic fatty liver disease.
Korean J Hepatol. 16:288–294. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jaroszewicz J, Rogalska M, Flisiak I and
Flisiak R: Successful antiviral therapy is associated with a
decrease of serum prohepcidin in chronic hepatitis C. World J
Gastroenterol. 16:1747–1752. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shinzato T, Abe K, Furusu A, Harada T,
Shinzato K, Miyazaki M and Kohno S: Serum pro-hepcidin level and
iron homeostasis in Japanese dialysis patients with erythropoietin
(EPO)-resistant anemia. Med Sci Monit. 14:CR431–CR437.
2008.PubMed/NCBI
|
|
23
|
Durie BG and Salmon SE: A clinical staging
system for multiple myeloma. Correlation of measured myeloma cell
mass with presenting clinical features, response to treatment, and
survival. Cancer. 36:842–854. 1975. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Greipp PR, San Miguel J, Durie BG, Crowley
JJ, Barlogie B, Bladé J, Boccadoro M, Child JA, Avet-Loiseau H,
Kyle RA, et al: International staging system for multiple myeloma.
J Clin Oncol. 23:3412–3420. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Roe MA, Spinks C, Heath AL, Harvey LJ,
Foxall R, Wimperis J, Wolf C and Fairweather-Tait SJ: Serum
prohepcidin concentration: no association with iron absorption in
healthy men; and no relationship with iron status in men carrying
HFE mutations, hereditary haemochromatosis patients undergoing
phlebotomy treatment, or pregnant women. Br J Nutr. 97:544–549.
2007. View Article : Google Scholar
|
|
26
|
Hadley KB, Johnson LK and Hunt JR: Iron
absorption by healthy women is not associated with either serum or
urinary prohepcidin. Am J Clin Nutr. 84:150–155. 2006.PubMed/NCBI
|
|
27
|
Young MF, Glahn RP, Ariza-Nieto M, Inglis
J, Olbina G, Westerman M and O’Brien KO: Serum hepcidin is
significantly associated with iron absorption from food and
supplemental sources in healthy young women. Am J Clin Nutr.
89:533–538. 2009.PubMed/NCBI
|
|
28
|
Katodritou E, Ganz T, Terpos E, Verrou E,
Olbina G, Gastari V, Hadjiaggelidou C, Varthaliti M, Georgiadou S,
Westerman M and Zervas K: Sequential evaluation of serum hepcidin
in anemic myeloma patients: study of correlations with myeloma
treatment, disease variables, and anemia response. Am J Hematol.
84:524–526. 2009. View Article : Google Scholar
|
|
29
|
Maes K, Nemeth E, Roodman GD, Huston A,
Esteve F, Freytes C, Callander N, Katodritou E, Tussing-Humphreys
L, Rivera S, et al: In anemia of multiple myeloma, hepcidin is
induced by increased bone morphogenetic protein 2. Blood.
116:3635–3644. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Pigeon C, Ilyin G, Courselaud B, Leroyer
P, Turlin B, Brissot P and Loréal O: A new mouse liver-specific
gene, encoding a protein homologous to human antimicrobial peptide
hepcidin, is overexpressed during iron overload. J Biol Chem.
276:7811–7819. 2001. View Article : Google Scholar
|
|
31
|
Oustamanolakis P, Koutroubakis IE,
Messaritakis I, Malliaraki N, Sfiridaki A and Kouroumalis EA: Serum
hepcidin and prohepcidin concentrations in inflammatory bowel
disease. Eur J Gastroenterol Hepatol. 23:262–268. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Taes YE, Wuyts B, Boelaert JR, De Vriese
AS and Delanghe JR: Prohepcidin accumulates in renal insufficiency.
Clin Chem Lab Med. 42:387–389. 2004.PubMed/NCBI
|
|
33
|
Cherng NC, Asal NR, Kuebler JP, Lee ET and
Solanki D: Prognostic factors in multiple myeloma. Cancer.
67:3150–3156. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sakamori R, Takehara T, Tatsumi T,
Shigekawa M, Hikita H, Hiramatsu N, Kanto T and Hayashi N: STAT3
signaling within hepatocytes is required for anemia of inflammation
in vivo. J Gastroenterol. 45:244–248. 2010. View Article : Google Scholar : PubMed/NCBI
|