Introduction
A port wine stain (PWS) is a congenital vascular
malformation characterized pathologically by ectasia of superficial
dermal capillaries and clinically by persistent macular erythema
(1,2).
According to the color of PWS lesions and the degree
of capillary dilation, pathologically, PWS is divided into 3 types:
i) the pink type, the color of the lesions includes pink, bright
red and dark red and the diameter of the dilated capillary is
approximately 50–80 μm; ii) the purple type, the color of the
lesions is prunosus, including light purple and dark purple and the
diameter of the dilated capillary is approximately 120–150 μm; iii)
the proliferative type, the color of the lesions is prunosus, the
lesion surface is slightly thickened or even nodular and the
diameter of the dilated capillary is greater than 150 μm. The
vascular depth of all three types is approximately 100–1000 μm
(3–5).
Photodynamic therapy (PDT) has become one of the
most effective treatments for PWS at present (6), but there remain certain challenges.
For example, various clinical outcomes are achieved within the same
clinical type after the same doses of PDT, as the size and depth of
the dilated capillaries vary from type to type, even in the same
type of lesion or in different lesions of one patient. Knowledge
concerning the vascular structure of PWSs may aid in the selection
of treatment doses and improve the therapeutic effect of PDT.
Biopsies are invasive and may cause side effects that make
follow-up studies difficult, thus the development of non-invasive
techniques for morphological assessment has important clinical
significance.
Optical coherence tomography (OCT) is a high speed,
high-resolution, non-invasive technique capable of generating
cross-sectional images of tissue microstructure. OCT uses low
coherent laser light to localize backscattering events within a
specimen (similar to ultrasonography) (7). Skin is a naturally high light
scattering non-transparent medium. The detection depth depends on
the wavelength; the maximum penetration depth in skin is
approximately 2 mm when using a l300-nm band. In the last 20 years,
OCT has become a reliable method for living tissue imaging
(8).
OCT has shown potential in the characterization and
diagnosis of a variety of dermatological disorders, including
bullous diseases, malignant melanoma, scabies, psoriasis and basal
cell carcinomas (9–14). OCT also has been used in PWS. For
example, Ziolkowska et al (15) presented one OCT image of a PWS with
ectatic vessels on the cheek. Bazant-Hegemark et al
(16) used an unsupervised,
real-time classification algorithm to classify 96 synthesized test
images and 7 clinical images of PWS. However, few reports have
identified the vascular image features of PWS patients nor have
identified the main features of other similar structures in OCT
images. Thus, strong support for the clinical diagnosis and
treatment of PWS using OCT is lacking.
In a previous study (17) we obtained the structural parameters
of PWSs including epidermal thickness, diameter and depth of
dilated blood vessels by comparing the OCT image of PWS lesions and
contralateral normal skin in 41 patients, but we failed to obtain
the corresponding histopathological sections.
In the present study, an OCT system was first used
to detect rabbit ear skin structures and obtain certain parameters
including vascular diameter, shape and location. Histopathological
images were compared with the OCT images to identify
clinicopathological correlations. Second, the OCT system was used
on PWS patients to detect the size and depth of their vascular
structures so as to provide vascular information for the objective
diagnosis of PWS pathological type, selection of optimal clinical
treatment dosages and prediction of therapeutic effect.
Materials and methods
Experimental instrument
A time domain OCT system (provided by Beijing
Newraysing Laser Tech Co. Ltd., Beijing, China) with an optic
Michelson interferometer with a broadband superluminescent diode
(SLED) light source (center wavelength 1310 nm; maximum output
power, 10 mW; bandwidth, 70 nm) was utilized. This OCT system
records 4 frames per sec with a detection depth of ∼1 mm and an
axial and transverse resolution of 10 and 9 μm, respectively, in
skin tissue. The scanning range is 2.85×2.5 mm (axial x lateral)
and image size is 400×400 pixels (axial x lateral). Signal-noise
ratio is 108 dB.
Detection using rabbit ears by OCT
Two New Zealand rabbits were used, weighing ∼0.5–1
kg. The experimental procedure was performed with the rabbits under
deep anesthesia using a 3:2 ratio mixture of xylazine (20 mg/ml)
and ketamine hydrochloride (100 mg/ml; 0.5ml/kg, intramuscular
injection). Repeat injections were administered, as required, to
keep the rabbits under deep anesthesia. Ear skin was coated with
depilatory cream for 3 min, then was gently removed with saline
tampon. A total of 12 test sites were documented with digital
photographs. The skin was pretreated with glycerol to substantially
increase the penetration depth of light through the skin and
enhance differentiation between skin layers by reducing light
scattering in the tissue (18–21).
The hand-held OCT detector was placed directly on the skin with
mild pressure and images were obtained by scanning from the side of
the preparation. Each test site was scanned three times. The
structural parameters, including diameter and depth of dilated
blood vessels in OCT images, were determined by a measuring tool
embedded in the image processing software (physical distance or
depth was obtained by dividing optical depth by the bulk index of
refraction of the tissue). The average of the three measurements
was calculated as the mean. All OCT measurements were performed by
the same investigator. The biopsy specimens were obtained within 5
min after the test, fixed in 10% buffered formalin, processed in
paraffin, sectioned and stained with hematoxylin and eosin.
Histopathological images were compared with the OCT images to
assess the degree of their correspondence.
Detection of PWS by OCT
The study was approved by the PLA Postgraduate
Medical School ethics board. All animal experiments were carried
out in accordance with the guidelines of the Animal Care and Use
Committee of PLA Postgraduate Medical School. A total of 85 cases
of Chinese patients with PWS on the face and neck were recruited
from the outpatients of the Department of Laser Medicine, General
Hospital between May 2010 and October 2011, and informed consent
was obtained. Among the 81 PWS patients, 53 cases with 77 test
sites belonged to the purple type and 28 cases with 44 test sites
belonged to the proliferative type. Patients of the purple type
were aged from 1 to 28 years, with an average age of 6.06±7.61, and
patients of the proliferative type were aged from 15 to 28, average
age 21.23±3.32. There was a statistical difference in age between
the two types (P<0.01). The exclusion criteria were as follows:
history of treatment; history of significant hematological,
cardiac, hepatic, or renal disease; history of skin disease likely
to interfere with the study; pregnant or breast feeding; with scar
constitution; with other hemangioma or syndrome.
Procedure and methods
Test sites were documented with digital photographs.
The test sites including PWS lesions and contralateral or near
normal skin (the latter was used as control) were pretreated with
glycerol, then detected by OCT. The average of the three
measurements was calculated corresponding to the mean. All OCT
measurements were performed by the same investigator.
Statistics
Quantitative variables were expressed as means ± SD.
Data were analyzed with the statistical software SPSS 13.0. A
two-tailed Student’s t-test for independent samples was used to
analyze the measurement data. P<0.05 was considered to indicate
a statistically significant result.
Results
Appearance of the vascular structure
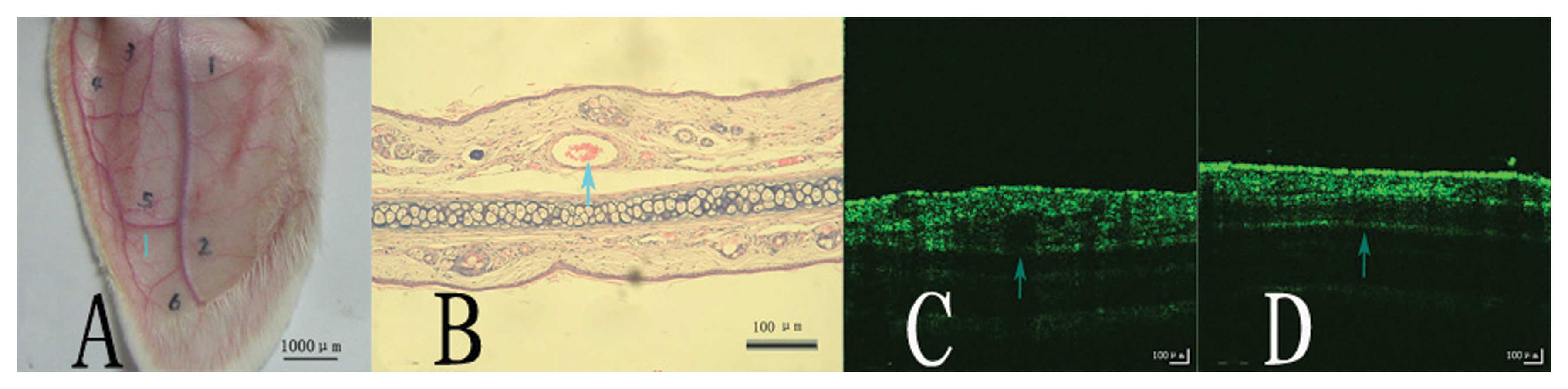
The dermal blood vessels were distinguished clearly
from normal tissue by the OCT system (Fig. 1C and D, a dark round or horizontal
band area is visible, corresponding to a vascular structure), and
the size and depth of the vascular structures were measured
precisely. The diameter and depth of blood vessels were
238.75±79.90 and 148.92±45.73 μm, respectively, as measured by OCT
images, 179.58±78.441 and 186.75±43.88 μm, respectively as measured
by corresponding histopathological sections. There was no
statistical difference in vascular diameter and depth (P>0.05)
between the results measured by OCT images and by histopathological
sections. A good correlation of vascular structures was found
between the images of the histopathological sections of the rabbit
ears (Fig. 1B, a blood-filled
vessel lined with flattened endothelial cells) and the OCT images
(Fig. 1C and D).
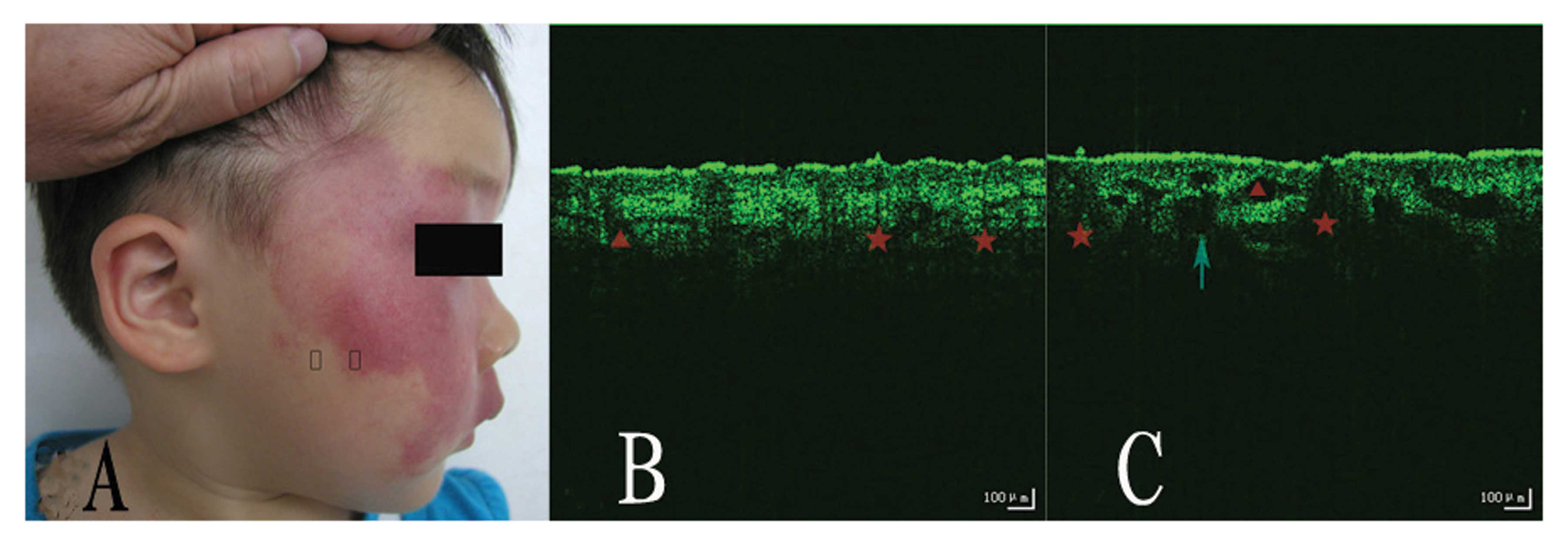
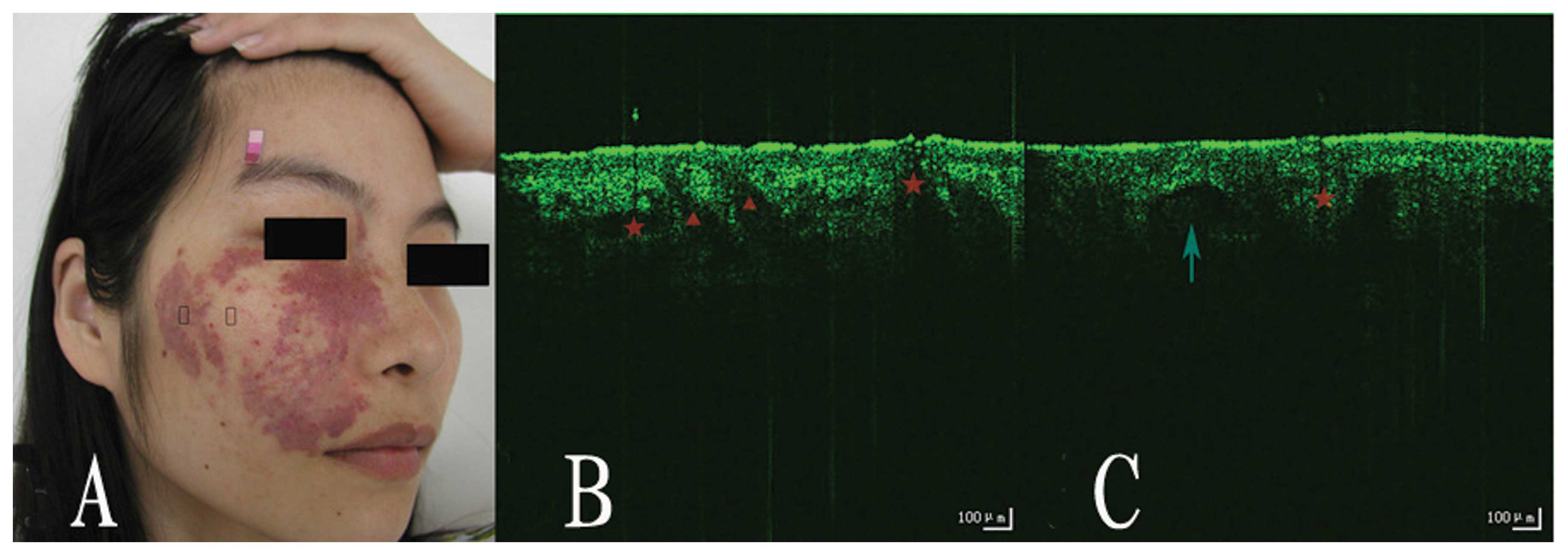
Appearance of the skin structure
The epidermal layer, dermal layer and skin
appendages, including hair follicles and sebaceous glands, were
clearly visible from the OCT images (Fig. 2 and 3B
and C). We also could distinguish PWS lesions from normal skin.
Compared to normal skin, we observed that the stratum corneum
(horny layer) was discontinuous, the dermo-epidermal border was
frequently blurred, and the number of sebaceous glands and dilation
of blood vessels were increased in the OCT images of PWS lesions.
We obtained the structural parameters of patients with PWS. The
dilated vascular depth and diameter measured by OCT images were
226.89±61.14 and 125.63±19.09 (the purple type), 195.59±59.45 and
193.93 ±32.43 (the proliferative type). There was no statistical
difference in the depth of vessels between the two types
(P>0.05), while there was a statistical difference in the
diameter of the vessels between them (P<0.01) (Table I).
 | Table IVascular depth and diameter of vessels
from patients with purple- and proliferative-type PWS measured by
OCT images. |
Table I
Vascular depth and diameter of vessels
from patients with purple- and proliferative-type PWS measured by
OCT images.
| Group | Depth of dilated
blood vessels (mean ± SD in μm) | Diameter of dilated
blood vessels (mean ± SD in μm) |
|---|
| Purple type | 226.89±61.14 | 125.63±19.09 |
| Proliferative
type | 195.59±59.45 | 193.93±32.43a |
Discussion
The average diameter of dilated capillaries in
patients with PWS is usually greater then 50 μm, in contrast to a
vessel diameter of 10 μm in normal skin (17–21).
This OCT system has an axial resolution of l0 μm, thus we could not
visualize the normal skin capillaries while it was possible to
identify the dilated capillaries in the papillary layer of the
PWSs. Vessels in PWS lesions may be located anywhere from
approximately 150–750 μm below the skin surface, thus this OCT
system with an in-depth penetration of 1 mm, was able to basically
achieve the requirements of this study.
In the present study the test sites were pretreated
with glycerol. OCT images distinguished between epidermal and
dermal layers, and dilated capillaries and skin appendages
including hair follicles and eccrine ducts were identified in the
surrounding tissues.
The vascular structures commonly appeared as
signal-poor round or oval areas sharply demarcated in the papillary
structures of the dermis. Since the absorption coefficient
(μa) in the epidermis, dermis and blood is 23, 2.4 and
266 l/mol. cm, respectively (22),
beneath the large diameter vessels, an ‘optical shadow’ is evident
relative to the surrounding tissues due to the absorption of light
by hemoglobin (23–25) .
Similar to the vascular structures, eccrine ducts
are also signal-poor round or oval areas sharply demarcated in the
papillary layer. The most marked difference is that the grayscale
value under eccrine ducts is higher than that of the adjacent
tissues at the same depth (26).
This demonstrates that eccrine ducts do not scatter or absorb
light. As a result, signal intensity is relatively undiminished
after passing through these structures.
By comparison with the OCT images of normal skin, we
observed that the stratum corneum (horny layer) succession was
intermittent and the dermo-epidermal border was frequently blurred
in PWS lesions; the reason for which remains unclear. The number of
sebaceous glands and dilated blood vessels were increased,
consequently the lesion surface of patients with PWSs is oily in
clinical examination. OCT images demonstrated a clear correlation
to clinical performance.
The mean vascular depth of vessels in the PWSs
measured by OCT images in our study was 226.89±61.14 μm in the
purple type and 195.59±59.45 μm in the proliferative type,
respectively. There was no statistical difference between them.
However, Barsky et al (5)
and Zhou et al (27)
obtained a mean vessel depth of 0.46±0.1 and 0.45±0.2 mm,
respectively, through assessment of pathological sections (5). The difference may be due to the
limitation of OCT penetration, since the blood vessels in deep
sites cannot be measured and calculated, or due to dehydration of
pathological sections. Therefore, the mean vessel depth measured by
pathological sections is deeper than that by OCT images. The mean
vascular diameter of the PWSs in our study was 125.63±19.09 μm in
the purple type and 193.93±32.43 μm in the proliferative type,
respectively. There was statistical difference between them. The
mean blood vessel diameter was greater than that of other studies
[the mean blood vessel diameter of a typical biopsy and confocal
microscopy study was 87.72±3.21 μm (4)]. The result of our previous study
(17) was 94.61±20.09 μm. The
explanation for this might be collapse of blood vessels ex
vivo and dehydration of pathological sections, so that the mean
blood vessel diameter measured on pathological sections was smaller
than that on OCT images in vivo. Moreover, in the previous
studies, the clinical types of PWSs were not classified; the
vessels assessed also included those of the pink type with a
smaller blood vessel diameter.
In addition, we observed a number of gaps in the
dermis, which appeared as regular and relatively small linear
structures of poor signal quality (breadth was usually below 50
μm), and may represent lymphatic vessels or small blood vessels
(15). In the papillary dermis,
the outside diameters of blood vessels are generally 17±22 μm,
whereas lymphatic vessels may reach up to 60 μm in diameter
(28). Taking into account that
these structures are present in both PWS lesions and normal skin,
the authors agree that they are lymphatic vessels or small blood
vessels. We also observed a number of gaps in the dermis, which
appeared as irregular and relatively large linear structures of low
lucidity (breadth was usually over 50 μm). In previous studies
these structures have been ascribed to lymphatic vessels or blood
vessels or areas of less dense collagen tissue (28–30).
Considering that these structures are mainly present in PWS lesions
and there is no report concerning abnormal lymphatic vessels or
areas of less dense collagen tissue structures in PWS lesions, the
authors presume they are blood vessels. However, if they are blood
vessels, then the OCT signal below should be attenuated due to the
strong absorption of hemoglobin. The absence of such a signal
attenuation might be due to the fact that the diameter of the blood
vessels is not large enough to absorb sufficient photons so does
not produce an ‘optical shadow’.
The present study indicates that OCT clearly
distinguishes dermal blood vessels in normal tissue, and
distinguishes PWS lesions from normal skin. In addition, OCT
accurately measures vascular diameter and depth of PWSs, which aids
the objective diagnosis of PWS pathological types, the selection of
optimal clinical treatment dosages and the prediction of treatment
effects. Due to the superiority of this real-time, in vivo,
discomfort-free system, OCT may be widely applied in the clinic. In
subsequent research, the authors will expand the number of cases,
and further observe the OCT images of PWSs following PDT
treatment.
References
|
1
|
Mulliken JB: Capillary (port-wine) and
other telangiectatic stains. Vascular Birthmarks: Hemangiomas and
Malformations. Mulliken JB and Young AE: WB Saunders; Philadelphia:
pp. 170–195. 1988
|
|
2
|
Neumann R, Leonhartsberger H, Knobler R
and Hönigsmann H: Immunohistochemistry of port-wine stains and
normal skin with endothelium-specific antibodies PAL-E,
anti-ICAM-1, anti-ELAM-1, and anti-factor VIIIrAg. Arch Dermatol.
130:879–883. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kelly KM, Choi B, McFarlane S, Motosue A,
Jung B, Khan MH, et al: Description and analysis of treatments for
port-wine stain birthmarks. Arch Facial Plast Surg. 7:287–294.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chang CJ, Yu JS and Nelson JS: Confocal
microscopy study of neurovascular distribution in facial port wine
stains (capillary malformation). J Formos Med Assoc. 107:559–566.
2008. View Article : Google Scholar
|
|
5
|
Barsky SH, Rosen S, Geer DE and Noe JM:
The nature and evolution of port wine stains: a computer-assisted
study. J Invest Dermatol. 74:154–157. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang Y, Gu Y, Liao X, Chen R and Ding H:
Fluorescence monitoring of a photosensitizer and prediction of the
therapeutic effect of photodynamic therapy for port wine stains.
Exp Biol Med (Maywood). 235:175–180. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Huang D, Swanson EA, Lin CP, Schuman JS,
Stinson WG, Chang W, et al: Optical coherence tomography. Science.
254:1178–1181. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pierce MC, Strasswimmer J, Park BH, Cense
B and de Boer JF: Advances in optical coherence tomography imaging
for dermatology. J Invest Dermatol. 123:458–463. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gladkova ND, Petrova GA, Nikulin NK,
Radenska-Lopovok SG, Snopova LB, Chumakov YP, et al: In vivo
optical coherence tomography imaging of human skin: norm and
pathology. Skin Res Technol. 6:6–16. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
De Giorgi V, Stante M, Massi D, Mavilia L,
Cappugi P and Carli P: Possible histopathologic correlates of
dermoscopic features in pigmented melanocytic lesions identified by
means of optical coherence tomography. Exp Dermatol. 14:56–59.
2005.
|
|
11
|
Welzel J: Optical coherence tomography in
dermatology: a review. Skin Res Technol. 7:1–9. 2001. View Article : Google Scholar
|
|
12
|
Welzel J, Bruhns M and Wolff HH: Optical
coherence tomography in contact dermatitis and psoriasis. Arch
Dermatol Res. 295:50–55. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Olmedo JM, Warschaw KE, Schmitt JM and
Swanson DL: Optical coherence tomography for the characterization
of basal cell carcinoma in vivo: a pilot study. J Am Acad Dermatol.
55:408–412. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gambichler T, Orlikov A, Vasa R, Moussa G,
Hoffmann K, Stücker M, et al: In vivo optical coherence tomography
of basal cell carcinoma. J Dermatol Sci. 45:167–173. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ziolkowska M, Philipp CM, Liebscher J and
Berlinen HP: OCT of healthy skin, actinic skin and NMSC lesions.
Medical Laser Application. 24:256–264. 2009. View Article : Google Scholar
|
|
16
|
Bazant-Hegemark F, Meglinski I, Kandamany
N, Monk B and Stone N: Optical coherence tomography: a potential
tool for unsupervised prediction of treatment response for
port-wine stains. Photodiagnosis Photodyn Ther. 5:191–197. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhao S, Gu Y, Xue P, Guo J, Shen T, Wang
T, et al: Imaging port wine stains by fiber optical coherence
tomography. J Biomed Opt. 15:0360202010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
He Y and Wang RK: Dynamic optical clearing
effect of tissue impregnated with hyperosmotic agents and studied
with optical coherence tomography. J Biomed Opt. 9:200–206. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang RK and Elder JB: High resolution
optical tomographic imaging of soft biological tissues. Laser Phys.
12:611–616. 2002.
|
|
20
|
Vargas G, Chan EK, Barton JK, Rylander HG
III and Welch AJ: Use of an agent to reduce scattering in skin.
Lasers Surg Med. 24:133–141. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Vargas G, Chan KF, Thomsen SL and Welch
AJ: Use of osmotically active agents to alter optical properties of
tissue: effects on the detected fluorescence signal measured
through skin. Lasers Surg Med. 29:213–220. 2001. View Article : Google Scholar
|
|
22
|
Lucassen GW, Verkruysse W, Keijzer M and
van Gemert MJ: Light distributions in a port wine stain model
containing multiple cylindrical and curved blood vessels. Lasers
Surg Med. 18:345–357. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Barton J, Welch A and Izatt J:
Investigating pulsed dye laser-blood vessel interaction with color
Doppler optical coherence tomography. Opt Express. 3:251–256. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wong RC, Yazdanfar S, Izatt JA, Kulkarni
MD, Barton JK, Welch AJ, et al: Visualization of subsurface blood
vessels by color Doppler optical coherence tomography in rats:
before and after hemostatic therapy. Gastrointest Endosc. 55:88–95.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Barton JK, Rollins A, Yazdanfar S, Pfefer
TJ, Westphal V and Izatt JA: Photothermal coagulation of blood
vessels: a comparison of high-speed optical coherence tomography
and numerical modelling. Phys Med Biol. 46:1665–1678. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ridgway JM, Armstrong WB, Guo S, Mahmood
U, Su J, Jackson RP, et al: In vivo optical coherence tomography of
the human oral cavity and oropharynx. Arch Otolaryngol Head Neck
Surg. 132:1074–1081. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhou G, Zhang Z and Li J: Computed
assessment of pathological images on 52 case’ biopsies of port wine
stain. Oral and maxillofacial surgery. 9:112–115. 1999.
|
|
28
|
Mogensen M, Morsy HA, Thrane L and Jemec
GB: Morphology and epidermal thickness of normal skin imaged by
optical coherence tomography. Dermatology. 217:14–20. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Salvini C, Massi D, Cappetti A, Stante M,
Cappugi P, Fabbri P and Carli P: Application of optical coherence
tomography in non-invasive characterization of skin vascular
lesions. Skin Res Technol. 14:89–92. 2008.PubMed/NCBI
|
|
30
|
Gambichler T, Moussa G, Sand M, Sand D,
Altmeyer P and Hoffmann K: Applications of optical coherence
tomography in dermatology. J Dermatol Sci. 40:85–94. 2005.
View Article : Google Scholar : PubMed/NCBI
|