Introduction
Gastric carcinoma is one of the most common types of
cancer affecting the digestive system. Over one-third of all
gastric carcinoma cases worldwide occur in China (1,2),
where the incidence and mortality rates of gastric carcinoma are on
the increase. The 5-year survival rate of patients with gastric
cancer is currently less than 20%, since most patients are
diagnosed at a later stage with advanced disease, when metastasis
has occurred, and are therefore often unsuitable for curative
surgery. Metastasis is the main cause of treatment failure in
patients with gastric carcinoma. Considering the difficulty of
treating disseminated disease, which is often apparent at
diagnosis, as well as the poor prognosis of patients with gastric
carcinoma, molecular diagnostic and prognostic markers for this
aggressive form of cancer should be established.
Phosphatase and tensin homolog (PTEN) is a tumor
suppressor, also known as mutated in multiple advanced cancer 1 or
tumor growth factor-β-regulated and epithelial cell-enriched
phosphatase 1. Its gene is located on chromosome 10q 23.3 (3–5) and
encodes a 403-residue protein with lipid and protein phosphatase
activity (6). PTEN, functioning as
a lipid phosphatase, dephosphorylates
phosphatidylinositol-(3,4,5)-triphosphate (PIP3) (6), a lipid product of class I
phosphoinositide 3-kinases. In turn, PIP3 activates important
kinases such as phosphoinositide-dependent kinase 1 and the
serine-threonine protein kinase AKT (7). Therefore, PTEN affects processes such
as cell cycle progression, apoptosis, migration, metabolism,
transcription and translation by negatively regulating the AKT
pathway and decreasing phosphorylation of AKT substrates (8). PTEN, functioning as a protein
phosphatase, is able to dephosphorylate focal adhesion kinase,
which inhibits cell invasion and metastasis. PTEN also inhibits the
mitogen-activated protein kinase signaling pathway, thus
restricting cell differentiation (9,10).
The loss or downregulation of PTEN appears to be a
common event in many types of tumors. The PTEN gene was previously
reported to be transcriptionally silenced by promoter methylation
in a number of gastric cancer cases (11). However, the role of the loss or
reduced expression of PTEN in gastric carcinoma progression and
prognosis remains unclear, especially when including paired
adjacent non-neoplastic tissue as a control. Since changes of gene
expression in a tumor may be due to individual variation rather
than tumor-specific activity, paired adjacent non-neoplastic tissue
samples were obtained to investigate for possible variations in
PTEN expression among patients.
The aim of this study was to evaluate the clinical
significance of the expression of PTEN protein in patients with
gastric carcinoma, and to investigate the correlation of PTEN
expression with the clinicopathological parameters and the
prognosis of these patients.
Materials and methods
Tissue microarray
The gastric cancer (GC) tissue microar-rays (TMAs)
used in the present study were purchased from Shanghai Outdo
Biotech Co., Ltd. (Shanghai, China). Human research ethics was
approved by the Ethics Committee of the Third Xiangya Hospital,
Central South University (Hunan, China). All patients provided
written informed consent to participate in this study. In total,
159 tumor tissues and 151 paired adjacent non-neoplastic tissues
were obtained. None of the 159 patients had received radiotherapy
or chemotherapy prior to surgery. Clinicopathological data
including gender, age at diagnosis, histological grade, American
Joint Committee on Cancer (AJCC) tumor stage, depth of invasion,
lymph node metastasis, distant metastasis and clinical follow-up
information were obtained from all patients.
Gastric carcinoma samples were histologically
reviewed by one pathologist. Tumors were graded according to the
Thoenes grading system and were histologically classified according
to the World Health Organization Classification System. Depth of
invasion and lymph node metastasis were staged according to the
Union for International Cancer Control (UICC) criteria. Patients
with lymph node metastasis stage >N0 or with distant metastasis
(i.e., M1) were considered to have metastatic disease. Overall
survival time was estimated as the time from diagnosis to the date
of death or last contact.
Immunohistochemistry
Immunostaining of the TMA slides was performed on a
TechMate 500 (Dako A/S, Copenhagen, Denmark) automatic staining
instrument according to the manufacturer’s instructions. The TMA
slides were incubated with PTEN monoclonal antibody (dilution,
1:50; #9559, clone 138G6, Cell Signaling Technology, Inc., Beverly,
MA, USA) overnight at 4°C. The TMA slides were then incubated for
30 min with a labeled polymer horseradish peroxidase detection kit
(EnVision+; Dako, Carpinteria, CA, USA). A positive control,
derived from tissue with previously confirmed PTEN expression, was
used in all TMAs. Slides in which the PTEN antibody replaced by
control IgG (#3900, Cell Signaling Technology) served as negative
controls. Signal detection was performed using a Dako signaling
amplification system.
Evaluation of tissue staining
PTEN expression was evaluated according to the
staining intensity and the percentage of cells expressing PTEN.
PTEN staining was evaluated by one pathologist and two observers
simultaneously, and a consensus was reached for each score. Tissues
with <5% of PTEN-positive cells were labeled 0. Staining
intensity was scored from 0 to 3 (0, negative; 1, weak; 2, moderate
and 3, strong). The level of PTEN staining was evaluated by
calculating the immunoreactive score (IRS) (12) from the staining intensity (I) and
the percentage (P) of PTEN-positive cells: IRS=IxP. IRS=0 was
considered as negative and IRS>0 as positive expression.
Total PTEN expression was calculated as cytoplasmic
PTEN expression + nuclear PTEN expression. Cases with total IRS of
gastric carcinoma tissues/total IRS of paired adjacent
non-neoplastic tissues ≤0.5 were considered to have a
down-regulated PTEN expression.
Statistical analysis
Analyses were performed using GraphPad Prism
software version 5 (GraphPad Software, Inc., San Diego, CA, USA)
for Windows and MedCalc software (MedCalc, Mariakerke, Belgium).
The Student’s t-test was used to compare PTEN expression between
tumor and adjacent non-neoplastic tissue. The correlations between
PTEN expression and clinicopathological characteristics were
analyzed using contingency tables and Pearson’s χ2 test,
except for parameters with small sample sizes, for which Fisher’s
exact test was used. Survival time was analyzed according to the
PTEN expression level by the Kaplan-Meier method and compared using
the log-rank test. Cox regression model was used for multivariate
analyses. The clinical sensitivity and specificity of PTEN
expression were determined using receiver operator characteristic
(ROC) curves, and area under the curve (AUC) was calculated. In all
analyses, P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient clinicopathological
characteristics
The clinicopathological characteristics of the 159
de novo gastric carcinoma patients are recorded in Table I. There were 112 males with a
median age of 63 years (range, 45–84), and 47 females with a median
age of 67 years (range, 34–83). Histological grade was used to
assess differentiation stage; 2, 40 and 117 patients had grade I,
II and III tumors, respectively. AJCC tumor stage was used to stage
the primary gastric carcinomas; 13, 49, 86 and 11 patients were
classified as having stage I, II, III and IV tumors, respectively.
Depth of invasion was assessed using UICC criteria, and 11, 14, 104
and 30 patients were classified as stage T1, T2, T3 and T4,
respectively. Lymph node metastasis was assessed using UICC
criteria and 36, 26, 49 and 48 patients were classified as N0, N1,
N2 and N3, respectively. Regarding distant metastasis, 148 patients
were classified as M0, and 11 as M1. The mean duration of follow-up
was 33.7 months (median, 38 months; range, 0–61 months).
 | Table IClinicopathological characteristics of
159 gastric cancer patients according to PTEN expression
profile. |
Table I
Clinicopathological characteristics of
159 gastric cancer patients according to PTEN expression
profile.
| Characteristics | Total no. | Cytoplasmic PTEN
negative, n=98 (62%) | P value | Nuclear PTEN
negative, n=119 (75%) | P value | Total PTEN negative,
n=77 (48%) | P value | Downregulated PTEN
expression, n=113 (71%) | P value |
|---|
| Gender | | | | | | | | | |
| M | 112 | 70 (63%) | 0.725 | 84 (75%) | 1 | 54 (48%) | 1 | 82 (78%) | 0.025 |
| F | 47 | 28 (60%) | | 35 (74%) | | 23 (49%) | | 25 (58%) | |
| Age (years) | | | | | | | | | |
| Median | 65 | 65 | | 67 | | 65 | | 65 | |
| Range | 34–84 | 41–83 | | 41–84 | | 41–83 | | 41–84 | |
| Histological
grade | | | | | | | | | |
| I | 2 | 0 (0%) | 0.016 | 2 (100%) | 0.287 | 0 (0%) | 0.244 | 1 (50%) | 0.717 |
| II | 40 | 19 (48%) | | 33 (83%) | | 17 (43%) | | 28 (70%) | |
| III | 117 | 79 (68%) | | 84 (72%) | | 60 (51%) | | 80 (73%) | |
| AJCC stage | | | | | | | | | |
| I | 13 | 5 (38%) | 0.271 | 6 (46%) | 0.051 | 1 (8%) | 0.012 | 4 (33%) | 0.018 |
| II | 49 | 33 (67%) | | 39 (80%) | 0.013a | 29 (59%) | 0.002a | 36 (77%) | 0.004a |
| III | 86 | 54 (63%) | | 64 (74%) | | 42 (49%) | | 60 (74%) | |
| IV | 11 | 6 (55%) | | 10 (91%) | | 5 (45%) | | 9 (82%) | |
| Depth of
invasion | | | | | | | | | |
| T1 | 11 | 7 (64%) | 0.897 | 7 (64%) | 0.828 | 4 (36%) | 0.851 | 6 (60%) | 0.578 |
| T2 | 14 | 8 (57%) | | 11 (79%) | | 7 (50%) | | 10 (71%) | |
| T3 | 104 | 66 (63%) | | 78 (75%) | | 52 (50%) | | 71 (71%) | |
| T4 | 30 | 17 (57%) | | 23 (77%) | | 14 (47%) | | 22 (81%) | |
| Lymph node
metastasis | | | | | | | | | |
| N0 | 36 | 20 (56%) | 0.836 | 27 (75%) | 0.632 | 17 (47%) | 0.841 | 22 (65%) | 0.213 |
| N1 | 26 | 16 (62%) | | 17 (65%) | | 11 (42%) | | 17 (68%) | |
| N2 | 49 | 32 (65%) | | 37 (76%) | | 26 (53%) | | 40 (83%) | |
| N3 | 48 | 30 (63%) | | 38 (79%) | | 23 (48%) | | 30 (68%) | |
| Distant
metastasis | | | | | | | | | |
| M0 | 148 | 92 (62%) | 0.75 | 109 (74%) | 0.29 | 72 (49%) | 1 | 100 (71%) | 0.728 |
| M1 | 11 | 6 (55%) | | 10 (91%) | | 5 (45%) | | 9 (82%) | |
Gastric carcinomas showed significant
loss of cytoplasmic but not nuclear PTEN expression relative to
non-neoplastic tissues
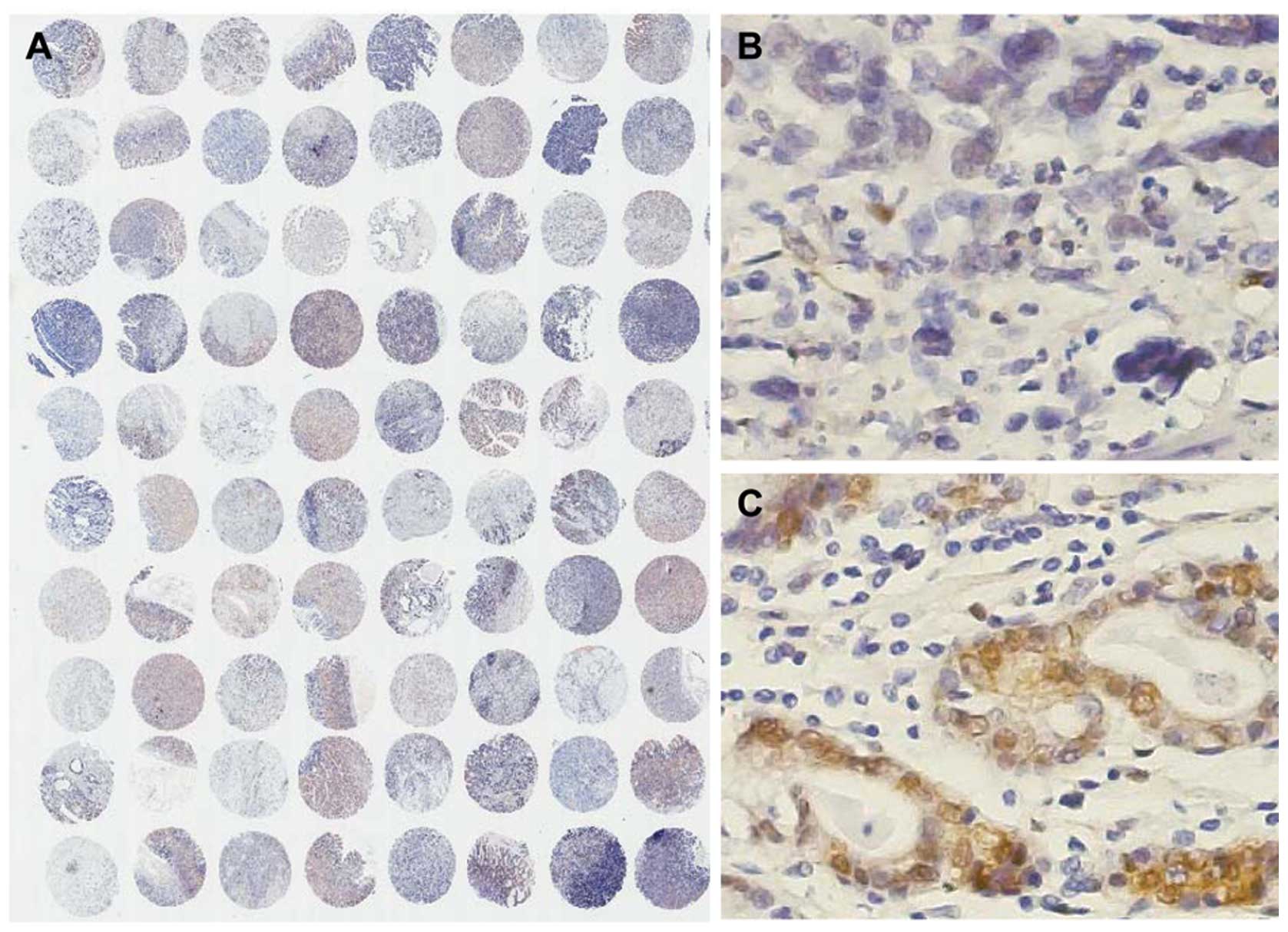
The expression levels of PTEN in gastric carcinoma
and adjacent non-neoplastic tissue were determined by immuno
histochemistry using a PTEN-specific antibody (Fig. 1A). The immunostaining pattern of
PTEN was characterized by cytoplasmic and nuclear staining of the
carcinoma and adjacent non-neoplastic tissues. Representative
images of PTEN-negative and -positive expression are shown in
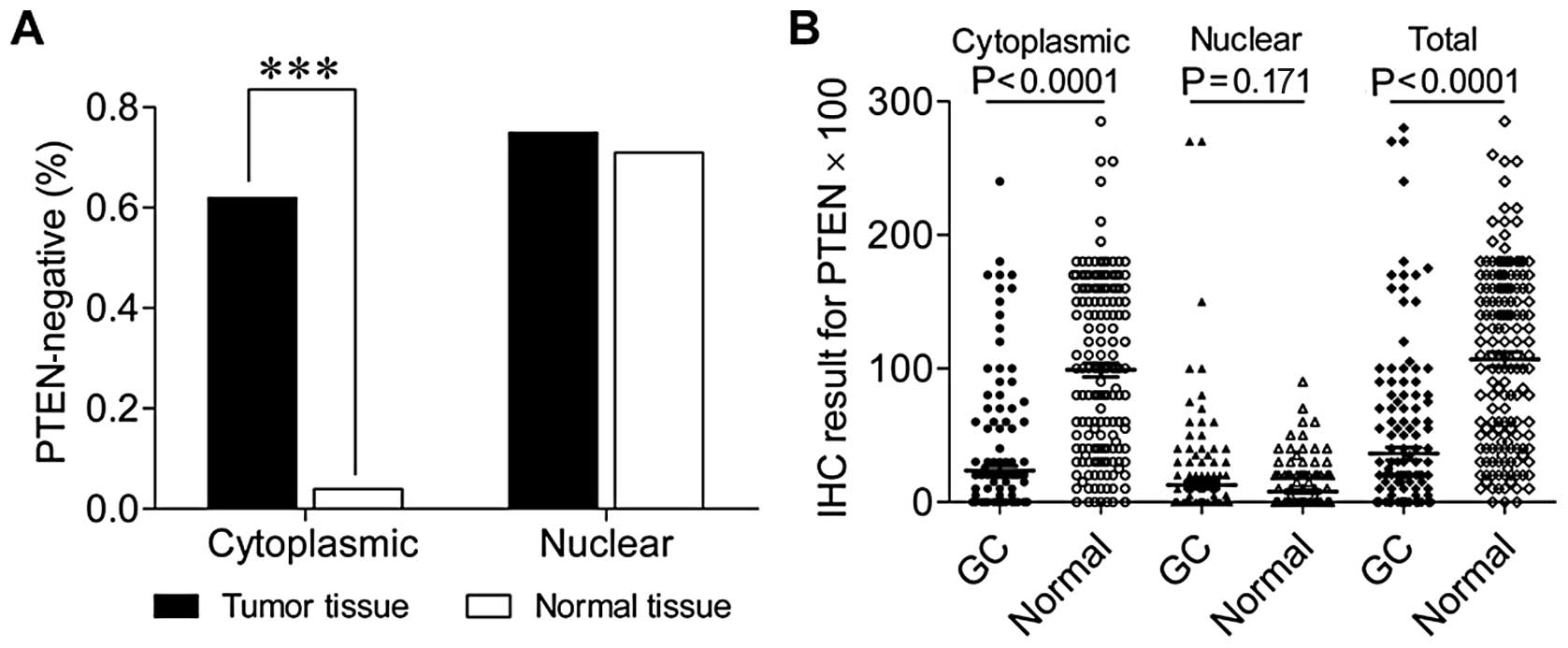
Fig. 1B and C, respectively. The
percentage of gastric carcinoma tissue samples lacking cytoplasmic
PTEN expression (62%, 98/159) was significantly higher compared
with that of adjacent non-neoplastic tissue (5%, 7/151) (Fig. 2). By contrast, the percentages of
gastric carcinoma tissue and adjacent non-neoplastic tissue samples
lacking nuclear PTEN expression were high, but similar (75%,
119/159 vs. 70%, 105/151, respectively) (Fig. 2A). Quantification of
immunohistochemistry, confirmed that cytoplasmic and total PTEN
expression levels were significantly lower in gastric carcinoma
tissues compared to adjacent non-neoplastic tissues (both,
P<0.0001) (Fig. 2B), no
difference was detected in nuclear expression (P=0.171). These data
indicate that, relative to adjacent non-neoplastic tissue, the loss
of PTEN expression in gastric carcinoma is mainly due to the
downregulation or loss of cytoplasmic rather than nuclear
expression.
Correlations between loss of
cytoplasmic/nuclear PTEN expression and clinicopathological
characteristics
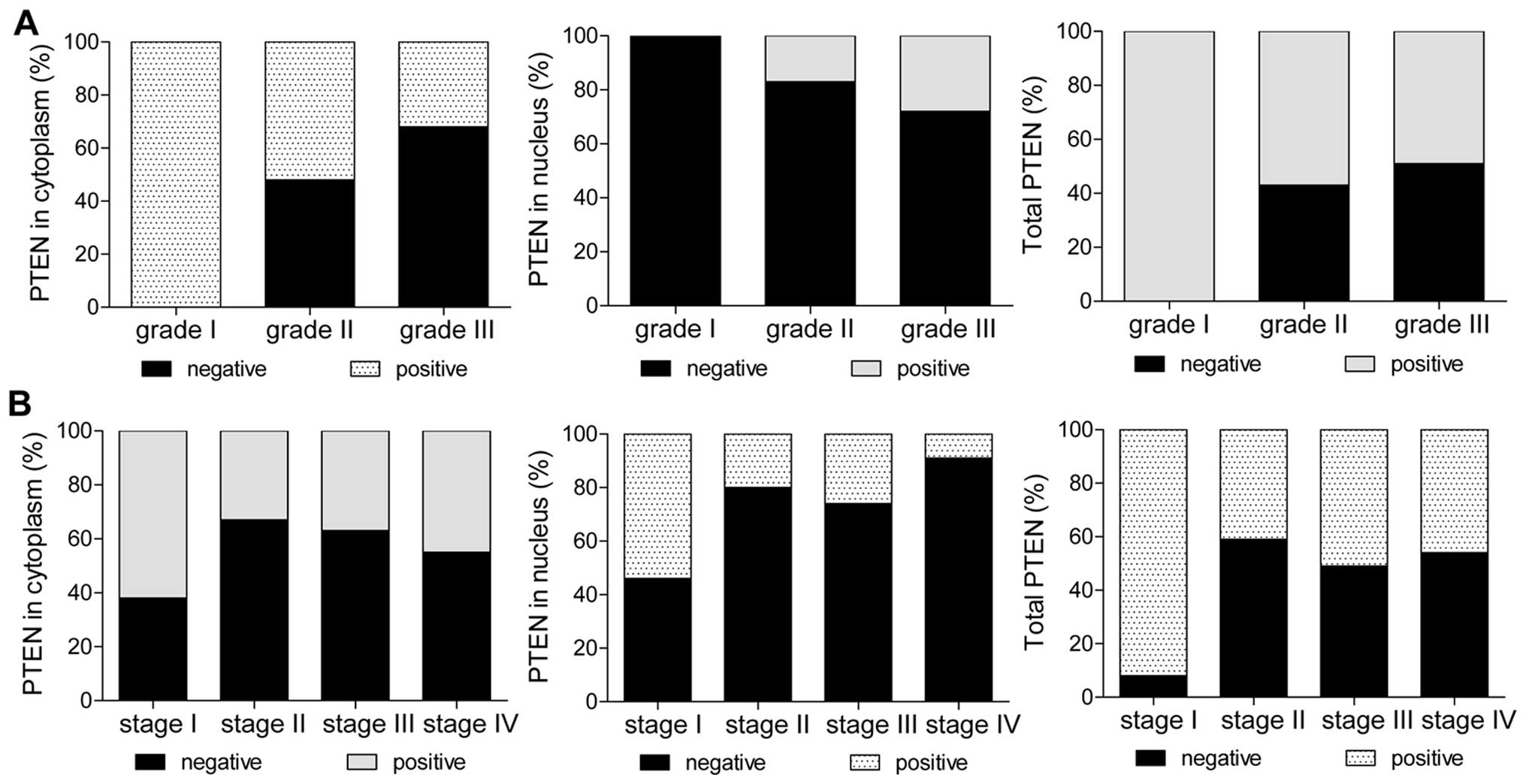
Among 159 patients with gastric carcinoma, the
histological grade was significantly correlated with the loss of
cytoplasmic PTEN expression (P=0.016) (Fig. 3A and Table I), but not with the loss of nuclear
or total PTEN expression (Fig.
3A). AJCC tumor stage was significantly correlated with the
loss of nuclear PTEN expression (P=0.013, AJCC tumor stage I vs.
stages II–IV) and with the loss of total PTEN expression (P=0.012)
(Fig. 3B and Table I). When comparing AJCC tumor stage,
the percentage of stage II–IV carcinomas with loss of total PTEN
expression was significantly greater compared with that of stage I
carcinomas (P=0.002) (Fig. 3B and
Table I). These results suggest
that the loss of total PTEN expression is an effective marker which
may be used in the differentiation of AJCC stage I from stage II–IV
tumors. No statistically significant correlations between the loss
of cytoplasmic, nuclear or total PTEN expression with other
clinicopathological characteristics, including gender, age, depth
of invasion, lymph node metastasis and distant metastasis were
observed (Table I).
Correlation between the downregulation of
PTEN expression and clinicopathological characteristics
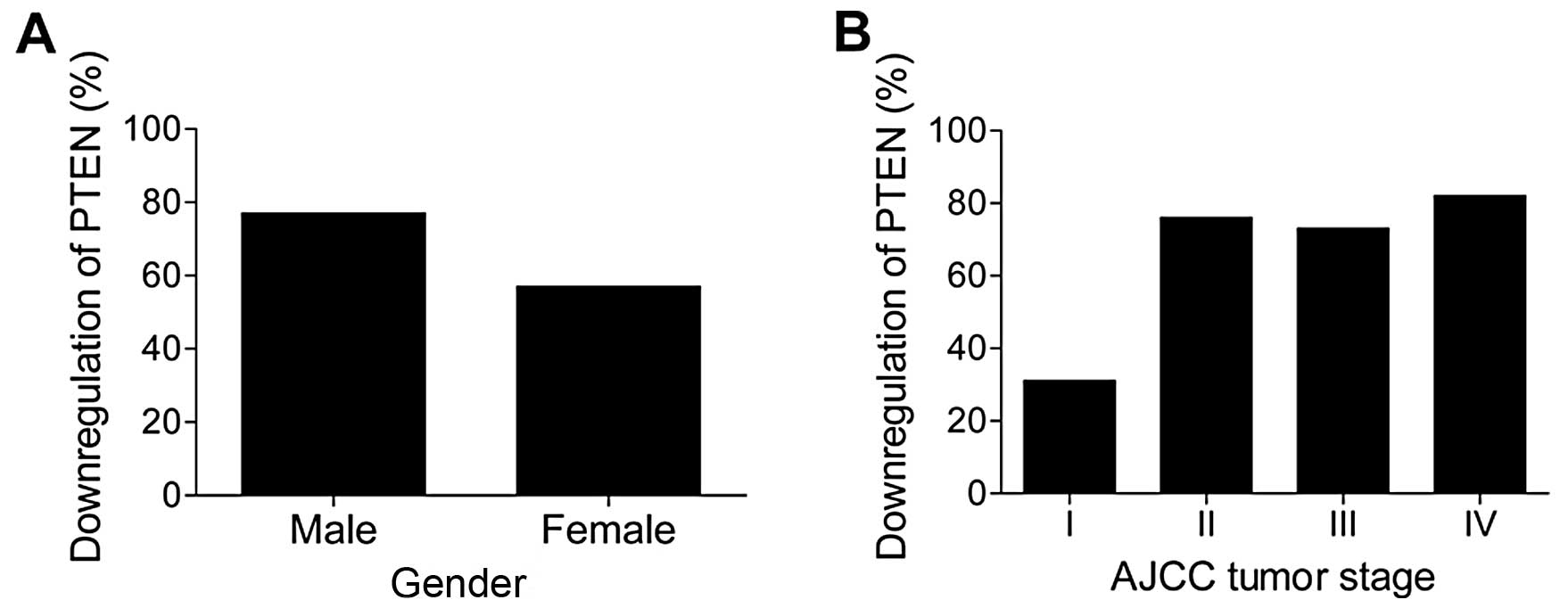
Possible correlations were investigated between the
downregulation of total PTEN expression (i.e., total IRS of gastric
carcinoma tissues/total IRS of paired adjacent non-neoplastic
tissues ≤0.5) with the clinicopathological characteristics of
gastric carcinoma patients. Downregulation of PTEN expression was
significantly correlated with gender (P=0.025) (Fig. 4A and Table I) and AJCC tumor stage (P= 0.018)
(Fig. 4B and Table I). When AJCC stage I carcinomas
were compared with stage II–IV carcinomas, the association between
the downregulation of PTEN expression and AJCC tumor stage became
more significant (P=0.004) (Fig.
4B and Table I), suggesting
that the downregulation of PTEN has the potential to be used in the
differentiation of AJCC stage I from stage II–IV tumors. By
contrast, no correlation between the downregulation of total PTEN
expression with other clinicopathological characteristics was
observed (Table I).
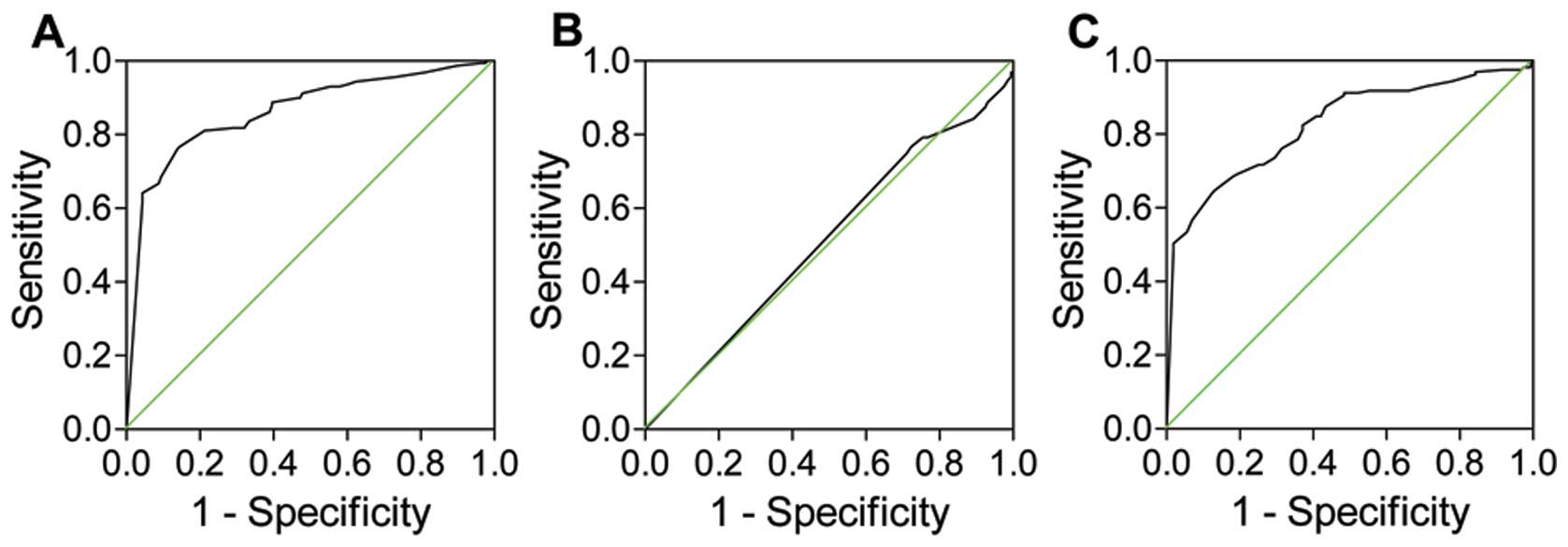
Clinical sensitivity and specificity of
PTEN expression
The clinical sensitivity and specificity of PTEN
expression were examined using ROC curve analysis and the AUC was
calculated as an indicator of overall discrimination. The AUCs for
cytoplasmic, nuclear and total PTEN expression in gastric carcinoma
were 0.865 (P<0.0001), 0.516 (P=0.617) and 0.829 (P<0.0001),
respectively (Fig. 5 and Table II). When using the optimal cut-off
point determined by MedCalc software, the diagnostic accuracies of
cytoplasmic, nuclear and total PTEN expression were 85.9, 53.3 and
85.7%, respectively. Thus, a low PTEN cytoplasmic or total
expression showed significant clinical sensitivity and specificity
in gastric carcinoma, and was able to differentiate between
carcinoma tissue and adjacent non-neoplastic tissue.
| Table IIReceiver operating characteristic
curve analysis of PTEN expression. |
Table II
Receiver operating characteristic
curve analysis of PTEN expression.
| | | Optimal cut-off
point
| | | | | |
|---|
| PTEN expression
pattern | AUC (95% CI) | P-value | Sensitivity
(%) | Specificity
(%) | +PV (%) | −PV (%) | +LR | +LR | Diagnostic accuracy
(%) |
|---|
| Cytoplasmic | 0.865
(0.822–0.901) | <0.0001 | 76.1 | 87.4 | 85.9 | 77.4 | 6.05 | 0.27 | 85.9 |
| Nuclear | 0.516
(0.459–0.573) | 0.617 | 76.7 | 29.1 | 53.3 | 54.3 | 1.08 | 0.80 | 53.3 |
| Total | 0.829
(0.783–0.870) | <0.0001 | 64.2 | 88.7 | 85.7 | 70.2 | 5.7 | 0.40 | 85.7 |
Correlation between loss of PTEN
expression and survival
In order to evaluate the prognostic relevance of
PTEN expression in patients with gastric cancer after surgery, the
Cox regression model was used to investigate the effects of PTEN
expression on overall and 3-year survival. As shown in Tables III and IV, cytoplasmic, nuclear and total PTEN
expression was not associated with median survival time or overall
survival. These data indicate that PTEN expression is not
associated with overall or 3-year survival of patients with gastric
carcinoma after surgery.
| Table IIICorrelation of PTEN expression with
overall survival. |
Table III
Correlation of PTEN expression with
overall survival.
| PTEN expression
profile | HR (95% CI) | P-value | Median survival
time (months) | Survival rate
(%) |
|---|
| Cytoplasmic | | | | |
| Negative | 0.856
(0.556–1.319) | 0.481 | 43 | 43 |
| Positive | | | 28 | 41 |
| Nuclear | | | | |
| Negative | 1.126
(0.704–1.804) | 0.62 | 37 | 42 |
| Positive | | | 43 | 43 |
| Total | | | | |
| Negative | 0.948
(0.626–1.435) | 0.736 | 43 | 43 |
| Positive | | | 35 | 41 |
| Total PTEN
expression relative to adjacent non-neoplastic tissue | | | | |
|
Downregulated | 0.755
(0.474–1.202) | 0.236 | 43 | 45 |
| Not
downregulated | | | 28 | 35 |
| Table IVCorrelation of PTEN expression with
3-year survival. |
Table IV
Correlation of PTEN expression with
3-year survival.
| PTEN expression
profile | HR (95% CI) | P-value | Median survival
time (months) | Survival rate
(%) |
|---|
| Cytoplasmic | | | | |
| Negative | 0.697
(0.432–1.124) | 0.149 | 36 | 57 |
| Positive | | | 28 | 46 |
| Nuclear | | | | |
| Negative | 1.206
(0.716–2.031) | 0.378 | 36 | 52 |
| Positive | | | 36 | 55 |
| Total | | | | |
| Negative | 0.827
(0.522–1.310) | 0.520 | 36 | 57 |
| Positive | | | 35 | 49 |
| Total PTEN
expression relative to adjacent non-neoplastic tissue | | | | |
|
Downregulated | 0.800
(0.480–1.335) | 0.421 | 36 | 55 |
| Not
downregulated | | | 28 | 48 |
Discussion
In the present study, we used TMAs of tumor and
paired adjacent non-neoplastic tissues to evaluate the clinical
significance of PTEN in patients with gastric carcinoma. We showed
that PTEN expression was frequently lost in the cytoplasm in
gastric carcinoma compared with adjacent non-neoplastic tissue. The
loss of cytoplasmic PTEN expression was significantly correlated
with histological grade, and the loss of nuclear or total PTEN
expression was significantly correlated with AJCC tumor stage. The
level of PTEN expression was also downregulated in gastric
carcinoma compared with paired adjacent non-neoplastic tissue.
Downregulation of total PTEN expression was significantly
associated with gender and AJCC tumor stage, and the frequency of
PTEN downregulation was positively correlated with AJCC tumor
stage. Thus, a low PTEN expression may be a marker for gastric
carcinoma. These findings also indicate a novel molecular basis for
the critical role of PTEN loss in the development and progression
of gastric carcinoma.
The tumor suppressor PTEN is encoded by a gene that
shows the greatest selection for loss in the human genome (13). Studies have shown that the PTEN
gene is frequently mutated or lost in many types of human primary
carcinomas (14). In addition,
PTEN expression is often dysregulated in carcinoma, even in the
absence of genetic loss or mutation (15). In mice, PTEN deletion or mutation
significantly contribute to tumorigenesis, and conditional knockout
of PTEN leads to neoplasia in multiple tissues (16,17).
Functional PTEN expression has been shown to inhibit the growth and
invasive properties of cancer cells, and thus improve survival
outcomes in various types of tumors (18–22).
These studies have demonstrated the pivotal roles of PTEN in cancer
initiation and progression. Similarly, we found that 62% of the
gastric carcinomas demonstrated loss of cytoplasmic PTEN compared
with 5% of adjacent non-neoplastic tissues, by using TMA and immuno
histochemistry. Moreover, 72% of the gastric carcinomas showed
downregulation of total PTEN expression relative to the adjacent
non-neoplastic tissues. The lower cytoplasmic and total PTEN
expression levels in gastric carcinoma compared to adjacent
non-neoplastic tissues observed in this study were consistent with
the findings reported by Zheng et al(23). Furthermore, the reduced cytoplasmic
or total PTEN expression levels had significant clinical
implications for gastric carcinoma based on ROC curves. These data
indicate that downregulation or loss of PTEN may be an etiological
factor in the development and progression of gastric carcinoma.
In mice, tumor burden and levels of phosphorylated
AKT increase significantly when the expression level of PTEN
decreases by 25%, particularly in the mammary gland (24). These findings suggest that even
small reductions in PTEN catalytic activity are likely to have a
significant clinical impact. In the gastric carcinoma patients
included in this study, the rate of loss of cytoplasmic PTEN
expression was positively correlated with histological grade. The
loss or downregulation of total PTEN expression was also correlated
with AJCC tumor stage. Thus, the loss of nuclear or total PTEN
expression, and downregulation of total PTEN expression can be used
in the differentiation of AJCC stage I from stage II–IV gastric
carcinomas. These data also suggest that PTEN expression is
significantly associated with the progression of gastric
carcinoma.
A number of studies have shown that a decreased PTEN
expression is also correlated with the progressive outcome of solid
cancers, including ovarian, prostate and cervical cancer (25,26).
Regarding its association with survival, Deng et al(27) reported that PTEN expression was not
correlated with survival time, whereas Bai et al(28) showed that patients with nuclear
PTEN expression had higher survival rates compared with those
without nuclear PTEN expression. In this study, we found no
significant correlation of PTEN expression, including cytoplasmic,
nuclear and total expression, with overall or 3-year survival,
results which are consistent with the findings of Deng et
al(27). Although the
differences in associations observed between our study and the
results reported by Bai et al(28) may be due to methodological
differences or the number of patients examined, it is likely that
PTEN expression in gastric carcinoma may not serve as a prognostic
marker, but as a marker for differentiating tumor stage and
progression. Additional studies are required to further explore the
role of PTEN expression (or lack thereof) in the prognosis of
gastric cancer, and take into account postsurgical treatments that
potentially affect survival independently of PTEN expression, such
as adjuvant therapy.
In conclusion, results showed that the cytoplasmic
PTEN expression was frequently lost in gastric carcinoma compared
with adjacent non-neoplastic tissue. Furthermore, the total PTEN
expression was downregulated in gastric carcinoma relative to
non-neoplastic tissue in the patients included in this study. Loss
and downregulation of PTEN expression were associated with several
clinicopathological characteristics, notably AJCC stage. These
findings suggest that the loss or downregulation of PTEN expression
is involved in tumorigenesis and the progression of primary gastric
carcinoma. Our findings also indicate that PTEN is a promising new
molecular target for designing novel preventive and therapeutic
strategies to control gastric carcinoma.
Acknowledgements
This study was partly supported by the
Ministry of Science and Technology of China Grants (2011DFA30480)
and the Ministry of Education (China) (IRT1168).
References
|
1
|
Roder DM: The epidemiology of gastric
cancer. Gastric Cancer. 5:5–11. 2002. View Article : Google Scholar
|
|
2
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar
|
|
3
|
Li J, Yen C, Liaw D, et al: PTEN, a
putative protein tyrosine phosphatase gene mutated in human brain,
breast, and prostate cancer. Science. 275:1943–1947. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Li DM and Sun H: TEP1, encoded by a
candidate tumor suppressor locus, is a novel protein tyrosine
phosphatase regulated by transforming growth factor beta. Cancer
Res. 57:2124–2129. 1997.PubMed/NCBI
|
|
5
|
Steck PA, Pershouse MA, Jasser SA, et al:
Identification of a candidate tumour suppressor gene, MMAC1, at
chromosome 10q23.3 that is mutated in multiple advanced cancers.
Nat Genet. 15:356–362. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Maehama T and Dixon JE: The tumor
suppressor, PTEN/ MMAC1, dephosphorylates the lipid second
messenger, phosphatidylinositol 3,4,5-trisphosphate. J Biol Chem.
273:13375–13378. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Goberdhan DC and Wilson C: PTEN: tumour
suppressor, multifunctional growth regulator and more. Hum Mol
Genet. 12:R239–R248. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Stambolic V, Suzuki A, de la Pompa JL, et
al: Negative regulation of PKB/Akt-dependent cell survival by the
tumor suppressor PTEN. Cell. 95:29–39. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Besson A, Robbins SM and Yong VW:
PTEN/MMAC1/TEP1 in signal transduction and tumorigenesis. Eur J
Biochem. 263:605–611. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Waite KA and Eng C: Protean PTEN: form and
function. Am J Hum Genet. 70:829–844. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kang YH, Lee HS and Kim WH: Promoter
methylation and silencing of PTEN in gastric carcinoma. Lab Invest.
82:285–291. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Remmele W and Stegner HE: Recommendation
for uniform definition of an immunoreactive score (IRS) for
immunohistochemical estrogen receptor detection (ER-ICA) in breast
cancer tissue. Pathologe. 8:138–140. 1987.(In German).
|
|
13
|
Bignell GR, Greenman CD, Davies H, et al:
Signatures of mutation and selection in the cancer genome. Nature.
463:893–898. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Salmena L, Carracedo A and Pandolfi PP:
Tenets of PTEN tumor suppression. Cell. 133:403–414. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Carracedo A, Alimonti A and Pandolfi PP:
PTEN level in tumor suppression: how much is too little? Cancer
Res. 71:629–633. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hollander MC, Blumenthal GM and Dennis PA:
PTEN loss in the continuum of common cancers, rare syndromes and
mouse models. Nat Rev Cancer. 11:289–301. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Backman SA, Ghazarian D, So K, et al:
Early onset of neoplasia in the prostate and skin of mice with
tissue-specific deletion of Pten. Proc Natl Acad Sci USA.
101:1725–1730. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lee JI, Soria JC, Hassan KA, et al: Loss
of PTEN expression as a prognostic marker for tongue cancer. Arch
Otolaryngol Head Neck Surg. 127:1441–1445. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tachibana M, Shibakita M, Ohno S, et al:
Expression and prognostic significance of PTEN product protein in
patients with esophageal squamous cell carcinoma. Cancer.
94:1955–1960. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
McMenamin ME, Soung P, Perera S, Kaplan I,
Loda M and Sellers WR: Loss of PTEN expression in paraffin-embedded
primary prostate cancer correlates with high Gleason score and
advanced stage. Cancer Res. 59:4291–4296. 1999.PubMed/NCBI
|
|
21
|
Depowski PL, Rosenthal SI and Ross JS:
Loss of expression of the PTEN gene protein product is associated
with poor outcome in breast cancer. Mod Pathol. 14:672–676. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sano T, Lin H, Chen X, et al: Differential
expression of MMAC/ PTEN in glioblastoma multiforme: relationship
to locali zation and prognosis. Cancer Res. 59:1820–1824.
1999.PubMed/NCBI
|
|
23
|
Zheng H, Takahashi H, Murai Y, et al: Low
expression of FHIT and PTEN correlates with malignancy of gastric
carcinomas: tissue-array findings. Appl Immunohistochem Mol
Morphol. 15:432–440. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Leslie NR and Foti M: Non-genomic loss of
PTEN function in cancer: not in my genes. Trends Pharmacol Sci.
32:131–140. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Harima Y, Sawada S, Nagata K, Sougawa M,
Ostapenko V and Ohnishi T: Mutation of the PTEN gene in advanced
cervical cancer correlated with tumor progression and poor outcome
after radiotherapy. Int J Oncol. 18:493–497. 2001.PubMed/NCBI
|
|
26
|
Yoshimoto M, Cunha IW, Coudry RA, et al:
FISH analysis of 107 prostate cancers shows that PTEN genomic
deletion is associated with poor clinical outcome. Br J Cancer.
97:678–685. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Deng H, Wu RL, Zhou HY, Huang X, Chen Y
and Liu LJ: Significance of Survivin and PTEN expression in full
lymph node-examined gastric cancer. World J Gastroenterol.
12:1013–1017. 2006.PubMed/NCBI
|
|
28
|
Bai Z, Ye Y, Chen D, et al: Homeoprotein
Cdx2 and nuclear PTEN expression profiles are related to gastric
cancer prognosis. APMIS. 115:1383–1390. 2007. View Article : Google Scholar : PubMed/NCBI
|