Introduction
Henoch-Schönlein purpura (HSP) is a common
vasculitis syndrome with systemic small-vessel vasculitis as the
primary lesions. The main pathology is leukocytoclastic vasculitis
of small dermal vessels and similar vasculitis characteristics are
present in other sites, including the joints, gastrointestinal
tract and kidneys (1). The main
clinical manifestation of HSP is cutaneous purpura and this may be
accompanied by abdominal pain and arthralgia. In addition, renal
injury is also common. However, cases of HSP accompanied by
pulmonary hemorrhage are rare. In China, there have been few
studies on HSP and there have been scattered studies worldwide. In
the clinic, HSP is usually ignored due to lack of evident bleeding.
We have treated only one patient, a female child, with HSPN. The
patient was finally diagnosed with HSP accompanied by pulmonary
hemorrhage using a combination of laboratory examination, analysis
of clinical manifestations and imaging examination. Following
treatment, the disease condition was improved. In the present study
we report on the diagnosis and treatment methods used for this
disease, with a review of the literature. The study was conducted
in accordance with the Declaration of Helsinki and with approval
from the Ethics Committee of the First Affiliated Hospital, Henan
University of Traditional Chinese Medicine (TCM; Zhengzhou, China).
Written informed consent was obtained from the patient’s
family.
Case report
An 11-year-old female patient was hospitalized on
April 3, 2012 due to cutaneous purpura of the lower limbs for half
a month and urine test abnormality for three days. The patient
presented with cutaneous purpura of the lower limbs without
apparent cause (0.5–5 mm maximum diameter, bright red in color,
skin swelling, no fading when compressed, and symmetric
distribution). The patient also presented with knee and ankle joint
pain and abdominal pain, but there were no symptoms of
hematochezia, hematemesis or hemoptysis. Blood examination in The
First Affiliated Hospital, Henan University of Traditional Chinese
Medicine, showed that routine urine was normal. After the
administration of hydrocortisone, cimetidine and amoxicillin for
one week, the purpura disappeared and pain was relieved. The drug
administration was immediately stopped while observations were
conducted. Ten days following drug withdrawal, routine urine
re-examination was conducted and gave the following results: urine
protein (PRO) 3+; occult blood (BLD) 3+; and erythrocyte +++/HP.
The patient was hospitalized on April 3, 2012 with HSPN at the
First Affiliated Hospital, Henan University of Traditional Chinese
Medicine (TCM). On admission, the lower limbs had no erythra or
edema and there was no accompanying discomfort such as fever,
abdominal pain, arthralgia, cough or expiratory dyspnea. Feces was
normal and urine was deep yellow with appropriate volume.
Physical examination revealed the following: the
body temperature was 36.5°C; the pulse was 96 bpm; the breathing
frequency was 24 times/min; the blood pressure was 80/50 mmHg; and
the body weight was 30 kg. The patient’s consciousness and mental
state were normal. There was no erythra anywhere on the body and
the pharyngeal cavity was hyperemic. Double lung auscultation
indicated that the sound of the patient’s breath was clear, and dry
and moist rales were not audible. Heart auscultation did not
present any abnormality and the abdomen was soft and had no
tenderness or rebound pain. The liver and spleen under the rib cage
were palpable, the bowel sounds were normal and bilateral renal
percussion was negative. The spine and joints of the four
extremities did not present any deformity, and the four extremities
did not present erythra or edema. The neurological examination
revealed no abnormality.
A routine blood test revealed the following: a white
blood cell (WBC) count of 5.1×109 cells/l; a hemoglobin
(HGB) level of 110 g/l; a red blood cell (RBC) count of
4.1×1012 cells/l; and a platelet (PLT) count of
260×109/l (2012. 04. 04). The results of a routine urine
test were as follows: PRO 3+, BLD 3+ and RBC 3+/HP. The fecal
occult blood test was negative, the urine protein level at 24 h was
2.56 g/2000 ml urine and the urinary N-acetyl-β-D-glucosaminidase
(NAG) enzyme level was 33.3 U/gCr. The coagulation functions were
as follows: the prothrombin time was 10.5 sec, the international
normalized ratio (INR, prothrombin time ratio) was 0.98, the
fibrinogen level was 4.05 g/l, the activated partial prothrombin
time was 36.1 sec (normal value, 24–36 sec) and the D-dimer level
was 0.22 mg/l. The T-cell subset counts were: CD3+,
416/μl; CD4+, 137/μl; CD8+, 208/μl;
and CD4+/CD8+, 0.65/μl. Liver and
kidney function tests revealed the following: TP, 66.3 g/l; A, 38.7
g/l; alanine aminotransferase (ALT), 13.0 U/l; aspartate
aminotransferase (AST), 24 U/l; blood urea nitrogen (BUN), 4.49
mmol/l; creatinine (Cr), 61.9 μmol/l; and normal electrolyte
levels. Humoral immunity, complement, C-reactive protein (CRP) and
erythrocyte sedimentation rate (ESR) results were also normal;
anti-nuclear antibody (ANA), extractable nuclear antibody (ENA),
five indicators (HBsAg, HBsAb, HBeAg, HBeAb, HBcAb) of hepatitis B,
three indicators (anti-HCV, anti-HIV, anti-TP) of infectious
diseases and Mycobacterium tuberculosis antibody were
negative. Double renal parenchyma presented mild diffuse changes,
and the liver, gallbladder, spleen and pancreas showed no
significant abnormality. Routine chest radiography indicated an
irregular high-density shadow in the medium upper field of the
right lung. Therefore, pulmonary hemorrhage was considered.
Diagnosis and treatment process
Following admission, the patient’s disease history
was examined. The patient had not recently presented with
respiratory tract infections, including fever, cough, hemoptysis,
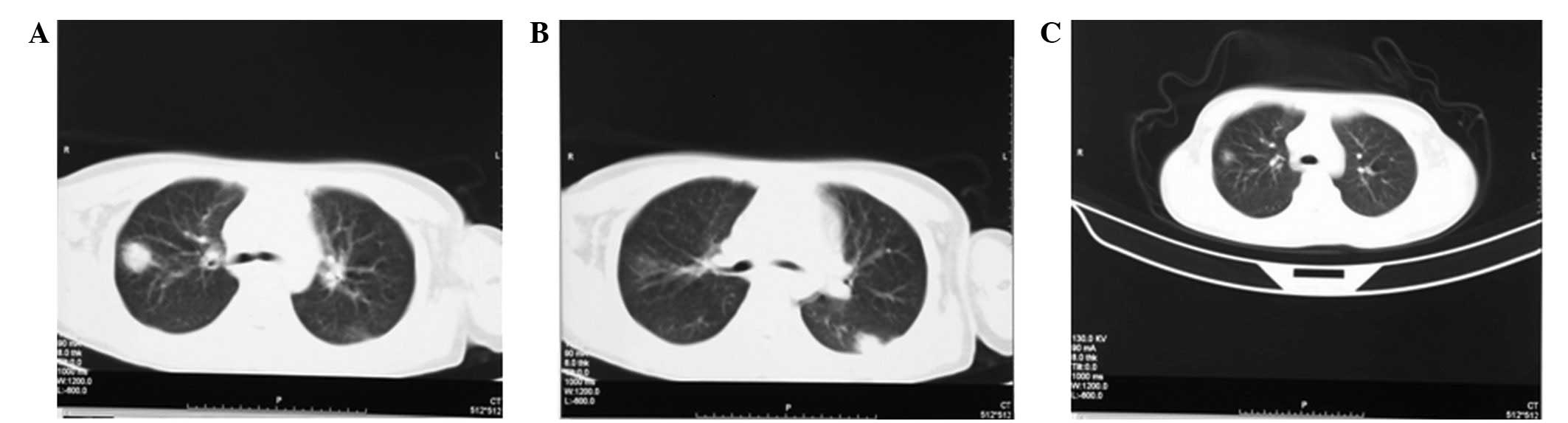
pectoralgia, or hemorrhage. To further investigate the nature of
the pulmonary high density shadow, a double lung CT examination was
conducted. The result indicated that the inferior lobe of the left
lung (Fig. 1B) and the superior
lobe dorsal segment of the right lung presented high-density
shadows (Fig. 1A), and the
property was unclear, but the possibility of pulmonary hemorrhage
was considered. Further examination results indicated that three
serological tests of tuberculosis and the PPD test all were normal,
and a T-spot assay indicated that interferon levels instituted by
both antigen A and antigen B were zero, therefore, tuberculosis was
not considered. Due to disease history, clinical manifestations,
routine blood, blood sedimentation and CRP results, spherical
pneumonia infection was also not considered. As the lesion nature
remained undetermined, a lung aspiration biopsy was recommended,
but the family refused. In addition, five indicators (PT, INR,
APTT, TT, FIB) of coagulation were almost normal, and the 24-hour
urine protein reached the criterion of massive proteinuria.
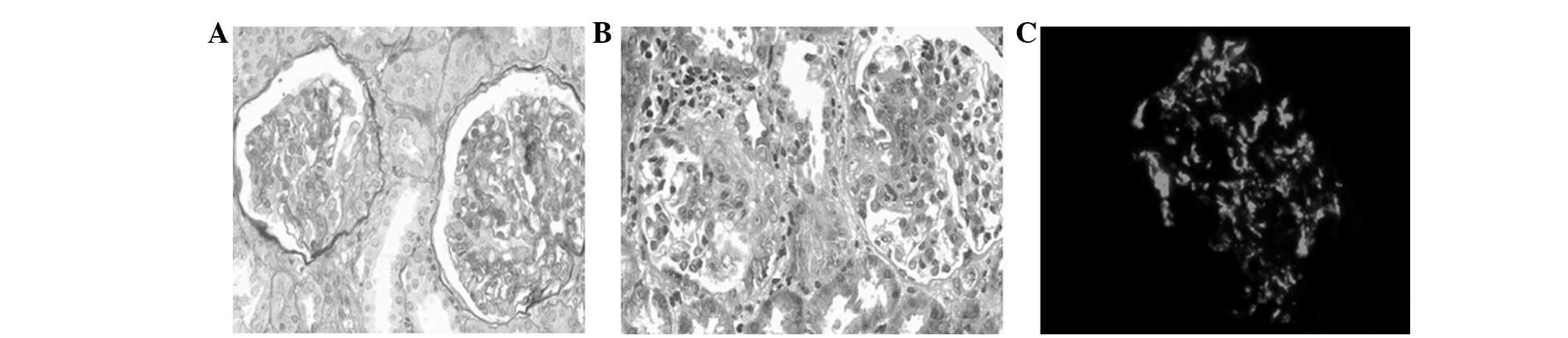
Therefore, renal biopsy puncture was conducted. Renal pathological
observation under a light microscope showed 12 glomeruli. Among
them, there were two cellular crescents, and one glomerular segment
that presented mesenteric and endothelial cell proliferation and
lobulation. In addition, three glomerular segments presented mild
mesenteric proliferation and focal segmental hypertrophy of
podocytes, and two glomerular segments presented endothelial cell
swelling. The basement membrane showed no significant abnormality,
and the stroma presented a small amount of mononuclear cell
infiltration (Fig. 2A and B).
Immunofluorescence showed that the IgA (+++), C3 (+) mesentery and
capillary vessels had small block- and particle-like deposits
(Fig. 2C). Tests for IgG, IgM,
HBsAg, HBeAg and HBcAg were negative, and the expression levels of
type IV collagens α3 and α5 were normal. Therefore the patient was
diagnosed with HSPN (IIIα) or pulmonary hemorrhage. The following
treatment schemes were prepared: i) orally administered prednisone
tablets, 2 mg/kg.day, three times daily; ii) tripterygium glycoside
tablets, 2 mg/kg.day, three times daily; iii) Benazepril tablets,
10 mg/day; iv) due to the consideration of pulmonary hemorrhage,
anticoagulant therapies, including heparin and Zantin were not
used; v) traditional Chinese medicine was used for ‘clearing heat’
and ‘detoxifying and cooling blood’ and hemostasis. After 10 days
of treatment, CT re-examination showed that the original pulmonary
hemorrhage was altered; it was markedly absorbed and reduced
(Fig. 1C). A routine urine test
gave the following results: PRO 2+, BLD 3+, RBC 3+/HP and 24-hour
urine protein, 0.99 g/day. The patient was recovering and so was
discharged. The treatments were continued outside the hospital, and
the doses of prednisone and tripterygium glycosides were gradually
reduced. On August 19, 2012, the patient was visited and examined.
The urine protein quantification at 24 h was 0.068 g; routine urine
results were: PRO -, BLD 1+ and RBC 5–8/HP; and no recurrent
purpura was visible.
Discussion
HSP is a common clinical allergic disease in
pediatric patients, and its main lesion is systemic small-vessel
vasculitis. As numerous systemic small vessels are involved,
multiple-system manifestations, including cutaneous purpura, joint
swelling and pain, gastrointestinal symptoms and nephritis are
visible. Among them, nephritis is the most important diagnostic
indicator of HSP and it is the most common cause of mortality in
patients with HSP. In addition, HSP has certain rare severe
complications, including gastrointestinal bleeding,
intussusception, intestinal perforation, intracranial hemorrhage
and pulmonary hemorrhage. There are numerous reports of HSP
accompanied by lung injury, but there are fewer reports of HSP
accompanied by pulmonary hemorrhage. The literature reports that
HSP accompanied by pulmonary hemorrhage is usually more severe in
the clinic and easily causes mortalities. We definitively diagnosed
an 11-year old female patient with anaphylactoid purpura nephritis
accompanied by pulmonary hemorrhage. Further examination revealed a
typical cutaneous purpura disease history, arthralgia, proteinuria
and hematuria. A renal biopsy showed mesangial cell proliferation
and crescent formation when viewed using light microscopy, and
immunofluorescence indicated IgA deposition. X-ray signs of
pulmonary hemorrhage were also present. However, as for clinical
manifestations, there were no obvious cough, anhelation or
expiratory dyspnea symptoms. Following the administration of oral
prednisone tablets, tripterygium glycoside tablets, traditional
Chinese medicine and general antiinflammatory treatment, the
disease condition was relieved. The severity of the clinical
manifestations in the present study is markedly different from that
in the cases reported in the literature.
Lung injury is potentially present in all patients
with HSP. The etiology of HSP is leukocytoclastic angiitis in the
small vessels of the dermis. Therefore, HSP has numerous clinical
symptoms, including pulmonary hemorrhage. The pulmonary hemorrhage
is likely due to an allergic diffuse vasculitis, and may
additionally be caused by an allergic reaction or immune function
disorder. IgA immune complex deposition, fragmentation and the
adhesion of a large number of white blood cells are the main causes
of pulmonary hemorrhage, and they promote an increase in the
permeability of the pulmonary capillary network to cause changes in
pulmonary respiratory symptoms and chest X-rays. Kathuria and
Cheifec (2) reported that
microscopy showed HSP pulmonary alveolar hemorrhage, indicating
leucocytolastic vasculitis with IgA deposition. However, in one
69-year-old patient reported by Usui et al(1), where the cause of mortality was HSP
pulmonary hemorrhage, the lung tissue autopsy presented edema,
extravasation of red blood cells and neutrophil infiltration of the
alveolar wall, but there was no clear hemoleukocytic vasculitis
manifestation, which was likely a result of steroid pulse therapy
changing the pathology. These data indicate that the main
pathogenic cause of the pulmonary hemorrhage in HSP is vasculitis
and the hemorrhaging has little correlation with the coagulation
function of patients. In the present study, the coagulation
function indicators indicated a hypercoagulable state [prothrombin
time, 10.5 sec; INR, 0.98; fibrinogen level, 4.05 g/l and D-dimer,
0.22 mg/l]. Due to the objections of family members, a pulmonary
biopsy was not conducted. However, renal biopsy showed a large
number of IgA deposits, confirming the previous analysis.
Although we are able to make a diagnosis according
to HSP disease history, pulmonary typical manifestations and
imaging symptoms, it remains difficult to make a differential
diagnosis of HSP accompanied by pulmonary hemorrhage in the clinic
since other vasculitis diseases, including systemic lupus
erythematosus (SLE), Wegener’s granulomatosis and pulmonary
hemorrhage-nephritis syndrome also have similar pulmonary
hemorrhage manifestations. In addition, bacterial pneumonia,
pneumonedema, pulmonary embolism and pulmonary tuberculosis also
induce similar conditions, and are likely to be accompanied by HSP.
Therefore, it is important to conduct immunological examinations,
including antineutrophil cytoplasmic antibody (ANCN), ANA and ENA
analyses. As lung biopsy has a certain risk for patients with this
type of condition, it is necessary to identify important diagnostic
information using methods including bronchoscopy, right cardiac
catheterization and pulmonary arteriography. Certain authors
suggest IgA deposition in the renal glomerulus to be the only
reliable identification criterion for differentiating HSP
accompanied by pulmonary hemorrhage from other vasculitis syndromes
(3). Renal biopsy of the case
reported in this study showed a large number of IgA deposits and
the patient was finally diagnosed with anaphylactoid purpura
nephritis accompanied by pulmonary hemorrhage. However, the authors
consider that this indicator should be adopted more as a useful
indicator, and that the use of multiple indicators is more
appropriate for conducting a comprehensive judgment of the clinical
diagnosis. In addition, it is necessary to identify clinical
microscopic diagnosic indicators for HSP accompanied by pulmonary
hemorrhage.
In a previous study, HSP accompanied by pulmonary
hemorrhage has been divided into severe and mild types (4). Mild HSP accompanied by pulmonary
hemorrhage presents mild pulmonary injury and/or renal injury,
mostly with a single attack and favorable prognosis, and part of
patients may naturally heal. However, severe cases rapidly present
respiratory failure and renal inadequacy. Therefore, the mortality
rate is high. In 15 cases of HSP accompanied by pulmonary
hemorrhage reported in other studies, the patients all presented
with severe multiple-organ injuries. Among them, six patients
succumbed to pulmonary hemorrhage (5). In the present study, although the
skin and joints manifested severe injuries, renal injury reached
the pathological IIIα level and pulmonary imaging revealed a large
shadow, the clinical respiratory manifestations were mild and no
severe emergency events, such as bleeding or respiratory failure,
occurred. It has been reported that HSP accompanied by pulmonary
hemorrhage mainly occurs in young individuals and adults, and the
mortality rate of adult patients with HSP accompanied by pulmonary
hemorrhage is higher (5,6). In a study of 18 patients with HSP
accompanied by pulmonary hemorrhage whose data were reported, three
of 11 cases younger than 18 years old succumbed, and four of five
cases older than 40 years old also succumbed (3), which indicated that the prognosis of
the adolescent patients was better than that of the adult patients.
In the present study, the patient was 11 years old and it was
unclear whether her young age was the reason for milder clinical
symptoms and a better prognosis. The existence of a correlation
between age and prognosis and the cause for the correlation will be
confirmed by further studies.
For the treatment of HSP accompanied by pulmonary
hemorrhage, the majority of previous reports (1,5,8,9)
suggest that the active use of steroids (oral prednisone tablets or
methylprednisolone granules), immunosuppressants (cyclophosphamide,
azathioprine and cyclosporine A) are able to markedly reduce the
mortality rate. For 11 child patient cases reported in the
literature, two out of six cases treated with methylprednisolone
granules succumbed, three cases completely recovered and one case
presented continuous proteinuria. The three cases treated with oral
prednisone tablets and cyclophosphamide granules all presented
continuous proteinuria and/or hematuria. One case treated with oral
prednisone tablets combined with azathioprine completely recovered
(3) and one case treated only with
oral prednisone tablets succumbed. The above results indicate that
the clinical efficacy of simple oral prednisone tablets is not
ideal, and the effects of their combination with slow-action
cyclophosphamide is also not ideal. In the present case, although
acute inflammatory reactions, including abdominal pain and
arthralgia, were more severe and renal injury reached medium
severity at the beginning of onset, no cough, expiratory dyspnea,
anemia and critical situations of failure of other organs were
observed. Therefore, methylprednisolone granules were not used, and
intravenous drip of cefatriaxone, oral prednisone and tripterygium
glycoside tablets combined with Chinese herbal medicines were used
for disintoxicating, promoting blood circulation and eliminating
blood stasis. The efficacy of the combined treatments was good. In
the treatment process of this disease case, in addition to
prednisone, we also administered a mild immunosuppressant,
tripterygium glycoside tablets was also used for treatment of this
disease case. Tripterygium wilfordii is a traditional
Chinese medicine. In 1997, it was first reported that its active
components, tripterygium glycosides, had unique anti-inflammatory
and immunosuppressive properties (10). Due to their high immunosuppressive
efficacy and low incidence of side-effects, tripterygium glycosides
are widely used for the treatment of autoimmune diseases and HSPN
at present.
Cases of HSP accompanied by pulmonary hemorrhage are
rare and HSP is typically ignored in the clinic due to a lack of
evident bleeding. However, severe cases are acute and critical, and
the mortality rate is high. Therefore, in clinical treatment of
HSP, attention should be paid to pulmonary symptoms, in addition to
common symptoms on skin, joint, urine and abdomen. Once unexplained
expiratory dyspnea and hemoptysis appear in clinic, the possibility
of accompanying pulmonary hemorrhage should be considered. When
considering the treatment scheme of this disease, it is difficult
to draw a definite conclusion as to whether the applied treatment
scheme is suitable for other patients due to the lack of clinical
cases. Therefore, further studies are required.
References
|
1.
|
Usui K, Ochiai T, Muto R, et al: Diffuse
pulmonary hemorrhage as a fatal complication of Schönlein-Henoch
purpura. J Dermatol. 34:705–708. 2007.
|
|
2.
|
Kathuria S and Cheifec G: Fatal pulmonary
Henoch-Schönlein syndrome. Chest. 82:654–656. 1982.
|
|
3.
|
Vats KR, Vats A, Kim Y, Dassenko D and
Sinaiko AR: Henoch-Schönlein purpura and pulmonary hemorrhage: a
report and literature review. Pediatr Nephrol. 13:530–534.
1999.
|
|
4.
|
Luo KL and Shao Z: 7 cases of
anaphylactoid purpura accompanied with pulmonary hemorrhage.
Journal of Applied Clinical Pediatrics. 19:1842004.(In
Chinese).
|
|
5.
|
Carter ER, Guevara JP and Moffitt DR:
Pulmonary hemorrhage in an adolescent with Henoch-Schönlein
purpura. West J Med. 164:171–173. 1996.
|
|
6.
|
Wright WK, Krous HF, Griswold WR, et al:
Pulmonary vasculitis with hemorrhage in anaphylactoid purpura.
Pediatr Pulmonol. 17:269–271. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Weiss VF and Naidu S: Fatal pulmonary
hemorrhage in Henoch-Schönlein purpura. Cutis. 23:687–688.
1979.
|
|
8.
|
Al-Harb NN: Henoch-Schönlein nephritis
complicated with pulmonary hemorrhage but treated successfully.
Pediatr Nephrol. 17:762–764. 2002.
|
|
9.
|
Matsubayashi R, Matsubayashi T, Fujita N,
Yokota T, Ohro Y and Enoki H: Pulmonary hemorrhage associated with
Henoch-Schönlein purpura in a child. Clin Rheumatol. 27:803–805.
2008.
|
|
10.
|
Li LS and Liu ZH: The application
prospects of tripterygium wilfordii in patients with kidney
disease. Chinese Journal of Nephrology Dialysis &
Transplantation. 6:203–204. 1997.(In Chinese).
|