Introduction
Pigmented villonodular synovitis (PVNS) is a rare,
idiopathic, proliferative disorder of the synovium (1) with two different forms: localized
(LPVNS) and diffuse (DPVNS) (2).
LPVNS occurs in small joints, whereas DPVNS typically affects the
entire synovial lining of large joints. PVNS commonly occurs in
patients aged 30–50 years and it has no gender bias (1). It is observed predominantly in the
knee and hip and is less common in the ankle, shoulder and wrist
(3,4). Elbow involvement is extremely rare;
only 24 cases have been reported at this site (2–22).
It is extremely difficult to differentiate PVNS from other soft
tissue tumors on the basis of imaging alone. Therefore, biopsy is
required for definitive diagnosis. We report a rare case of LPVNS
arising from the elbow joint with contracture and discuss the
findings of magnetic resonance imaging (MRI) and thallium (Tl)-201
scintigraphy, which were useful in making the differential
diagnosis retrospectively.
Case report
A 20-year-old, right-handed female reported a mass
on the right elbow; this mass had caused progressive pain over the
last 2 years. Although the patient had not suffered a previous
trauma involving her right elbow joint, the patient recognized pain
and a mass on the flexion side. Physical examination revealed an
elastic and soft tumor measuring 3.0x3.0 cm. It demonstrated no
adhesion to the skin and its margin was well-defined. The active
range of motion of the affected elbow was −15° extension, 80°
flexion, 90° supination and 90° pronation.
A roentgenogram of the right elbow revealed a soft
tissue mass around this joint, with no apparent bone erosion or
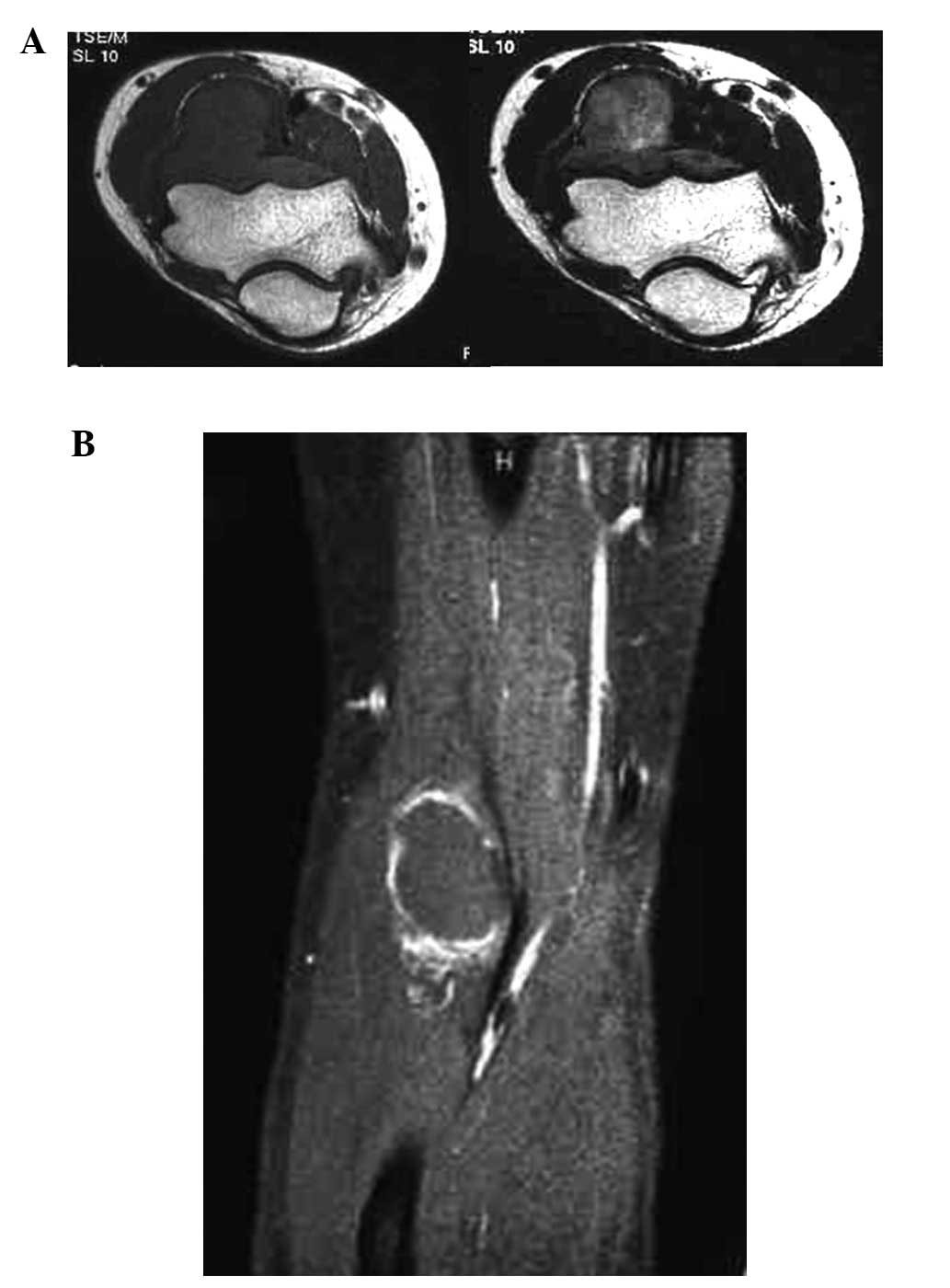
cystic changes (Fig. 1). MRI
revealed that the tumor was located between the brachioradialis and
brachialis. The signal intensity of the tumor was isointense to
muscle tissue on T1-weighted images; however, it was hyper- or
isointense to muscle on T2-weighted images. In images obtained by
gadolinium-enhanced MRI, the margin of the tumor was
well-contrasted (Fig. 2A and B).
Tl-201 scintigrams revealed an abnormal accumulation in the area of
the mass in the early and delayed phases (Fig. 3). No other abnormal accumulation
was detected.
On the basis of clinical findings and imaging
characteristics, the tumor was diagnosed as a primary soft tissue
tumor and an incisional biopsy was performed. Microscopic
examination revealed a nodular growth covered by synovial lining
cells. Mitotic figures were observed in parts, as were a large
number of multinucleated giant and inflammatory cells. The stroma
presented fibrosis and hemosiderin deposition was observed in areas
of the surface (Fig. 4).
Histological findings were characteristic of PVNS.
One month later, marginal excision with anterior
capsulectomy was performed since the tumor demonstrated adhesion to
the anterior lesion of the joint capsule. There was no apparent
bone erosion and the capsule was brownish-yellow. The tumor was
dumbbell shaped since a dull groove was created by the tendons of
the brachioradialis and brachialis and its surface was smooth.
Complete excision, including the anterior capsule was performed to
reduce the risk of local recurrence. Following surgical treatment,
the active range of motion of the operated joint was recovered
fully to 0° extension and 140° flexion with physical training. The
pain and mass were fully resolved following treatment and there was
no recurrence 5 years after surgery.
Discussion
The term PVNS was introduced by Jaffe et al
in 1941, based on clinical and pathological experience (23). PVNS is a benign, locally invasive
disease of the synovium and is currently classified as a giant cell
tumor of the tendon sheath or diffuse-type giant cell tumor; the
former description corresponds to LPVNS and the latter to DPVNS
(24). LPVNS is a small, discrete
lesion that usually occurs intra-articularly in the knee. The
etiology of PVNS remains a matter of debate (6,7,11).
Previous studies have not clarified whether the disease is a
locally aggressive neoplasm or a reactive synovitis (4,5). It
is clear, however, that the presence of blood in joints is
essential for the occurrence of PVNS. Proliferation of villi occurs
following hemorrhage in the joint space. A number of these villi
are damaged and crushed by joint motion. Then, hemorrhage recurs
and the synovium demonstrates continuous hyperplasia. The
macroscopic appearance consists of a dark yellow-brown mass and
villous thickening of the synovial membrane (7,19).
A literature review identified only 24 documented
cases of PVNS involving the elbow joint; of these, 15 were case
reports and nine were included in seven large retrospective PVNS
series of all sites: one case from Scott (8), one from Granowitz et
al(2), two from Docken
(5), one from Pandey and Pandey
(15), one from Miller (14), one from Ushijima et
al(11) and two from Schwartz
et al(4) (Table I). In the seven large retrospective
PVNS series, LPVNS comprised 246 and DPVNS comprised 78 of the 421
cases. There were no details of the remaining 97 cases. In past
reports of PVNS involving the elbow joint, five cases of LPVNS
(18,19) and 17 cases of DPVNS were
identified, in which this information was available. Gender was
reported in 16 of 24 cases; there were four males and 12 females.
Reported ages ranged from 6 to 61 years, with a mean age of 33.9
years in the 18 cases for which this information was available
(2–22).
 | Table ILiterature review of pigmented
villonodular synovitis (PVNS) arising from the elbow joint. |
Table I
Literature review of pigmented
villonodular synovitis (PVNS) arising from the elbow joint.
| Sources | Knee | Hip | Ankle | Wrist | Elbow | Others | Total | Remarks |
|---|
| Scott (1968) | 2 | 2 | | | 1 | | 5 | |
| Granowitz et
al(1976) | 20 | 2 | 4 | 6 | 1 | 62 | 95 | |
| Docken (1979) | | | | | 2 | | 89 | Incomplete data |
| Pandey and Pandey
(1981) | | | | | 1 | | 47 | Incomplete data |
| Miller (1982) | 18 | 8 | 3 | 1 | 1 | 3 | 34 | |
| Ushijima et
al(1986) | 25 | 5 | 13 | 2 | 1 | 6 | 52 | |
| Schwartz et
al(1989) | 75 | 20 | | | 2 | 2 | 99 | |
| Total | 140 | 37 | 20 | 9 | 9 | 73 | 421 | |
PVNS shows the same radiodensity as that of soft
tissue. The disease causes contour erosion of the underlying bone
or round lytic areas with well-demarcated borders, which are
observed particularly at points of capsular insertion (17). MRI strongly supports the diagnosis
of PVNS through the demonstration of areas of low- or iso-signal
intensity on T1-and T2-weighted images, indicative of signal
attenuation by the abnormal iron content in the hemosiderin within
a thickened synovium (19,25). A number of studies have reported
the MRI features of PVNS in the elbow joint (7,9,13,16,20).
On T1-weighted images, the lesion demonstrates isointensity to
muscle with small areas of low signal intensity, while T2-weighted
images demonstrate mildly increased signal intensity in the lesion.
Foci of low signal intensity are also demonstrated in similar
regions on T2-weighted images. Furthermore, the lesion is enhanced
heterogeneously by the administration of gadolinium-diethylene
triamine pentaacetic acid (DTPA) contrast agent (9). These findings are different from
those in malignant tumors, which show a mass of low- or iso-signal
intensity on T1-weighted images and high signal intensity on
T2-weighted images. Another classic feature observed within the
synovium of other joints with PVNS is the presence of a fatty
signal due to the accumulation of lipid-laden macrophages (7,17).
However, this finding was not observed in our study.
It has been reported that PVNS demonstrates high
isotope accumulation (26),
although little has been reported about the scintigraphic findings
of the disease (27). While a low
retention rate of Tl-201 on delayed imaging is observed in benign
tumors (28), Tl-201 uptake is
observed on early and delayed images in almost all cases of PVNS
(26,29); this simulates the findings of
malignant disease (29). Given the
above findings, the presence of activity on Tl-201 scintigraphy
alone does not aid in the differentiation of PVNS from malignant
diseases. However, this finding is useful in the differentiation of
PVNS from other benign diseases. In addition, a diffuse nodular
juxta-articular pattern of Tl-201 activity is strongly suggestive
of PVNS.
In conclusion, we identified an extremely rare case
of PVNS arising from the elbow joint. When interpreting Tl-201
images for the assessment of bone and soft tissue lesions, it is
important to recognize PVNS as a condition that simulates malignant
tumors. Furthermore, PVNS should be considered in the differential
diagnosis when increased Tl-201 activity is closely related to the
joint. MRI also aids in the differentiation by demonstrating
features of hemosiderin degradation products. These findings are
likely to be extremely helpful in the differential diagnosis of
bone and soft tissue tumors.
References
|
1.
|
Goldman AB and DiCarlo EF: Pigmented
villonodular synovitis. Diagnosis and differential diagnosis.
Radiol Clin North Am. 26:1327–1347. 1988.PubMed/NCBI
|
|
2.
|
Granowitz SP, D’Antonio J and Mankin HL:
The pathogenesis and long-term end results of pigmented
villonodular synovitis. Clin Orthop Relat Res. 335–351.
1976.PubMed/NCBI
|
|
3.
|
Pignatti G, Mignani G, Bacchini P,
Calderoni P and Campanacci M: Case report 590: Diffuse pigmented
villonodular synovitis with a cartilaginous component. Skeletal
Radiol. 19:65–67. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Schwartz HS, Unni KK and Pritchard DJ:
Pigmented villonodular synovitis. A retrospective review of
affected large joints. Clin Orthop Relat Res. 243–255.
1989.PubMed/NCBI
|
|
5.
|
Docken WP: Pigmented villonodular
synovitis: a review with illustrative case reports. Semin Arthritis
Rheum. 9:1–22. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Breimer CW and Freiberger RH: Bone lesions
associated with villonodular synovitis. Am J Roentgenol Radium Ther
Nucl Med. 79:618–629. 1958.PubMed/NCBI
|
|
7.
|
DiCaprio MR, Damron TA, Stadnick M and
Fuller C: Pigmented villonodular synovitis of the elbow: a case
report and literature review. J Hand Surg Am. 24:386–391. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Scott PM: Bone lesions in pigmented
villonodular synovitis. J Bone Joint Surg Br. 50:306–311.
1968.PubMed/NCBI
|
|
9.
|
Sekiya H, Ozawa H, Sugimoto N, Kariya Y
and Hoshino Y: Pigmented villonodular synovitis of the elbow in a
6-year-old girl: a case report. J Orthop Surg (Hong Kong).
15:106–108. 2007.PubMed/NCBI
|
|
10.
|
Torisu T, Iwabuchi R and Kamo Y: Pigmented
villonodular synovitis of the elbow with bony invasion. Clin Orthop
Relat Res. 94:275–280. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Ushijima M, Hashimoto H, Tsuneyoshi M and
Enjoji M: Pigmented villonodular synovitis. A clinicopathologic
study of 52 cases. Acta Pathol Jpn. 36:317–326. 1986.PubMed/NCBI
|
|
12.
|
Weissman BN: Arthrography in arthritis.
Radiol Clin North Am. 19:379–392. 1981.PubMed/NCBI
|
|
13.
|
Wyatt MC, Rolton N and Veale GA: Pigmented
villonodular synovitis of the elbow with a fenestrated fossa: a
case report. J Orthop Surg (Hong Kong). 17:127–129. 2009.PubMed/NCBI
|
|
14.
|
Miller WE: Villonodular synovitis:
pigmented and nonpigmented variations. South Med J. 75:1084–1086.
10921982. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Pandey S and Pandey AK: Pigmented
villonodular synovitis with bone involvement. Arch Orthop Trauma
Surg. 98:217–223. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Pimpalnerkar A, Barton E and Sibly TF:
Pigmented villonodular synovitis of the elbow. J Shoulder Elbow
Surg. 7:71–75. 1998. View Article : Google Scholar
|
|
17.
|
Lindenbaum BL and Hunt T: An unusual
presentation of pigmented villonodular synovitis. Clin Orthop Relat
Res. 122:263–267. 1977.PubMed/NCBI
|
|
18.
|
Ekman EF, Cory JW and Poehling GG:
Pigmented villonodular synovitis and synovial chondromatosis
arthroscopically diagnosed and treated in the same elbow.
Arthroscopy. 13:114–116. 1997. View Article : Google Scholar
|
|
19.
|
Geiger EV, Reize P, Wehrmann M and Wülker
N: Radial and ulnar neuropathy due to pigmented villonodular
synovitis of the elbow. J Shoulder Elbow Surg. 15:e8–e10. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Jerome JT and Sankaran B: Pigmented
villonodular synovitis of the elbow. Indian J Pediatr. 76:414–416.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Deo RP, Mehta AR and Pathak R: Invasive
pigmented villonodular synovitis of the elbow joint. A case report
and review of the literature. Indian J Cancer. 20:78–81.
1983.PubMed/NCBI
|
|
22.
|
Aydingöz U, Leblebicioglu G, Gedikoglu G
and Atay OA: Pigmented villonodular synovitis of the elbow in a
6-year-old girl. J Shoulder Elbow Surg. 11:274–277. 2002.
|
|
23.
|
Jaffe HL, Lichtenstein L and J SC:
Pigmented villonodular synovitis, bursitis and tenosynovitis. Arch
Pathol. 31:731–765. 1941.
|
|
24.
|
Somerhausen NS and Dal Cin P: Giant cell
tumour of tendon sheath. Pathology and Genetics of Tumours of Soft
Tissue and Bone. Fletcher CDM, Unni KK and Mertens F: IARC Press;
Lyon: pp. 110–111. 2002
|
|
25.
|
Llauger J, Palmer J, Rosón N, Cremades R
and Bagué S: Pigmented villonodular synovitis and giant cell tumors
of the tendon sheath: radiologic and pathologic features. AJR Am J
Roentgenol. 172:1087–1091. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Kawakami N, Kunisada T, Sato S, et al:
Thallium-201 scintigraphy is an effective diagnostic modality to
distinguish malignant from benign soft-tissue tumors. Clin Nucl
Med. 36:982–986. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Bravo SM, Winalski CS and Weissman BN:
Pigmented villonodular synovitis. Radiol Clin North Am. 34:311–326.
1996.
|
|
28.
|
Hicks RJ: Functional imaging techniques
for evaluation of sarcomas. Cancer imaging. 5:58–65. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Mackie GC: Pigmented villonodular
synovitis and giant cell tumor of the tendon sheath: scintigraphic
findings in 10 cases. Clin Nucl Med. 28:881–885. 2003. View Article : Google Scholar : PubMed/NCBI
|