Introduction
Focal nodular hyperplasia (FNH) is a benign
hyperplastic lesion and the number of reports of FNH has been
increasing owing to the widespread use of diagnostic imaging at
routine medical check-ups. The characteristic imaging findings of
FNH are: i) central scar formation, ii) nutrient vessels extending
radially from the center and iii) the presence of Kupffer cells
(1). When using an imaging
modality in the diagnosis of FNH, the key is to identify the
spoke-wheel pattern of nutrient vessels radiating from the center
of the FNH lesion. However, with contrast-enhanced computed
tomography (CT), the detection rate of tumors <3 cm is
reportedly as low as 3%, even though the detection rate of tumors
>3 cm is 65% (2). With
contrast-enhanced ultrasonography (US), the detection rates of
tumors >3 cm, <3 cm and <2 cm are 95, 30 and 16.7%,
respectively (3). The detection of
spoke-wheel patterns in FNH <3 cm is particularly difficult,
resulting in low detection rates. Currently, Sonazoid-enhanced US
is commonly used to obtain detailed hemodynamic information of
hepatic lesions and to make a qualitative diagnosis (4–11);
however, due to the monochromatic representation of the contrast
agent, detailed visual examination of the hemodynamics in small
tumors and tumors with rapid blood flow is often difficult.
In this study, we used arrival time parametric
imaging (At-PI), which enables color display of contrast agent
dynamics in contrast-enhanced US to investigate the detection rate
of spoke-wheel patterns in FNH <3 cm.
Materials and methods
Patient background
Five patients (3 males and 2 females) with FNH <3
cm who had undergone Sonazoid-contrast US at the Toho University
Omori Medical Center in Tokyo, Japan between February 2008 and
March 2009 were enrolled in the study. The mean tumor diameter was
20.2±7.2 mm (Table I). FNH was
diagnosed on the basis of high-density signals in the early phase
and iso-density signals in the equilibrium phase of abdominal CT as
well as histological findings of FNH, including irregular
hyperplastic hepatocytes and fibrotic scarring involving abnormal
blood vessels in post-US biopsy. This study was performed with
approval of the Ethics Committee at Toho University Omori Medical
Center. Written informed patient consent was obtained from the
patient.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Case | Age (years) | Gender
(male/female) | Tumor diameter
(mm) | Echo level
(high/low) | Time needed to
contrast an entire tumor (sec) |
|---|
| 1 | 47 | F | 14 | Low | 1.7 |
| 2 | 59 | M | 17 | Low | 2.5 |
| 3 | 34 | M | 14 | Low | 2.8 |
| 4 | 43 | F | 28 | Low | 2.5 |
| 5 | 56 | M | 28 | Low | 2.0 |
Sonazoid-enhanced US
Ultrasonography was performed using a Toshiba Aplio
XG ultrasound device (SSA-790A; Toshiba Medical Systems, Tochigi,
Japan) with a 3.75 MHz convex array probe (PVT-375 BT) at a
mechanical index of 0.22–0.29. The focus was set at the bottom end
of the tumors and 0.5 ml Sonazoid (perfluorobutane; GE Healthcare,
Oslo, Norway) was injected into the cubital vein. Data generated in
the first 40 sec was saved as raw data on the hard disk. US was
performed by the same operator to maintain imaging consistency.
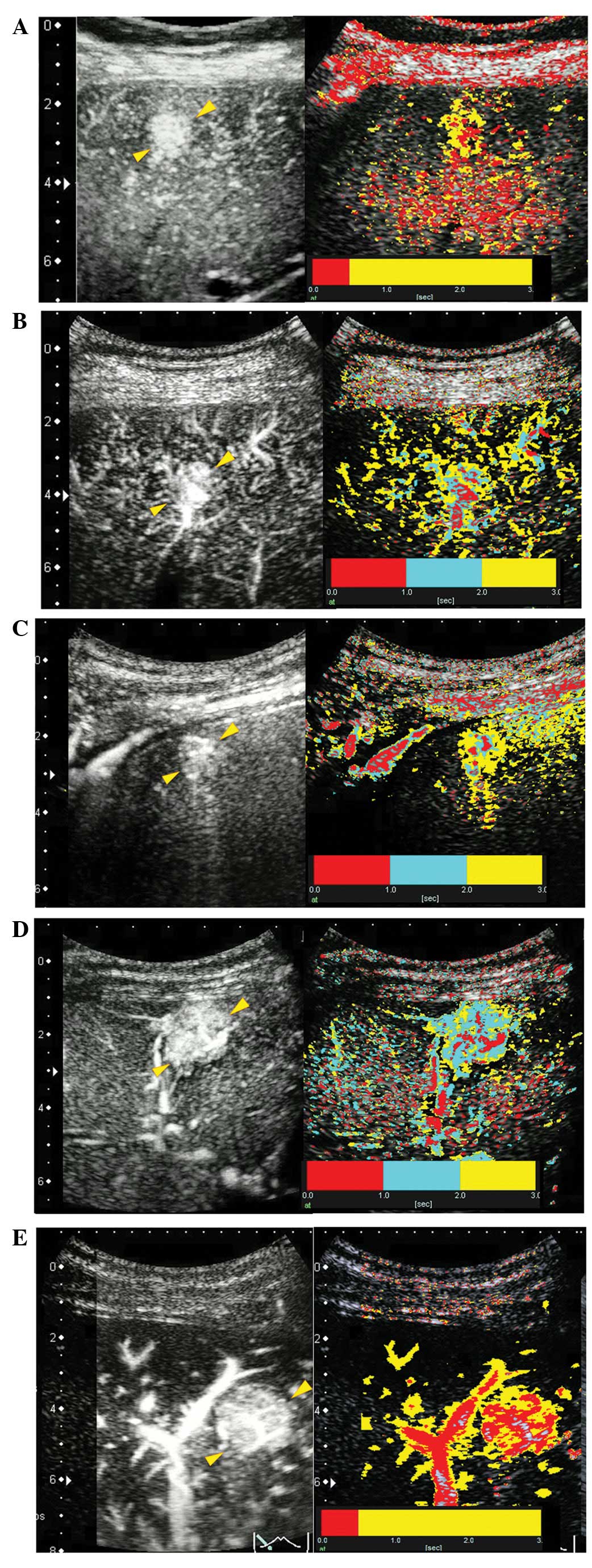
At-PI
Following US, At-PI was performed using the
proprietary image analysis software of the ultrasound system. The
system set the point at which the contrast agent reached the
hepatic tumor as time zero and sequentially calculated the arrival
time at individual pixels representing the tumor. A color map was
created and automatically superimposed on a B-mode image. Then, two
parametric-color scales were used to analyze color patterns and the
time setting for color distribution. Parametric-color scale 1, with
time 0–0.5 sec in red and time >0.5 sec in yellow, was used to
analyze tumors contrasted within 2 sec. Parametric-color scale 2
was used for tumors requiring ≥2 sec for contrast enhancement and
red, cyan and yellow were used to represent the times 0-1, 1-2 and
>2 sec, respectively (Fig.
1).
Micro-flow imaging
Following US, micro-flow imaging (MFI) was also
performed using the proprietary image analysis software of the
ultrasound system. The system started counting time when the
contrast agent reached the tumor and the arrival time of individual
pixels representing the tumor was sequentially calculated. A color
map was created and automatically superimposed on a B-mode
image.
Tumor assessment
At-PI video images were evaluated by three
ultrasonographic specialists with extensive experience (14, 17 and
33 years) in the contrast-enhanced US of liver diseases. The
specialists had no access to the clinical background of the
patients, hemanalysis, imaging findings or final diagnosis.
Detection of a spoke-wheel pattern was considered a positive
imaging finding. Similarly, MFI images were generated to analyze
contrast agent dynamics.
Results
Case 1 (47-year-old female) had a 14-mm tumor with
low echo signals in hepatic segment 8 (S8). Since it took 1.7 sec
to contrast the entire tumor, parametric-color scale 1 was used in
At-PI analysis. Three ultrasonographic specialists identified a
spoke-wheel pattern on the At-PI images, even though no
identification was made in MFI.
Case 2 (59-year-old male) had a 17-mm tumor with low
echo signals in S8. Since 2.5 sec was required to contrast the
tumor, parametric-color scale 2 was used in At-PI. Three
specialists observed a spoke-wheel pattern in At-PI but not in
MFI.
Case 3 (34-year-old male) had a 14-mm tumor with low
echo signals in S8. Since 2.8 sec was required for tumor
enhancement, parametric-color scale 2 was used in At-PI. A positive
diagnosis of FNH was made using MFI and At-PI.
Case 4 (43-year-old female) had a 28-mm tumor with
low echo signals in S5. As 2.5 sec was required for tumor
enhancement, parametric-color scale 2 was used in the analysis. A
positive diagnosis was made using the two imaging modalities.
Case 5 (56-year-old male) had a 28-mm tumor with low
echo signals in S3. Since it took 2.0 sec to contrast the tumor,
parametric-color scale 1 was used in At-PI analysis. A spoke-wheel
pattern was identified using MFI and At-PI. Fig. 2 shows the At-PI and MFI images from
all cases.
Discussion
First reported by Edmondson (12) in 1956, FNH is characterized by its
high prevalence in females aged 20–50 years (76.2–88%) (13–16)
and often exists as a solitary lesion (76.2%) (15,16).
Although the pathogenesis of FNH is currently unknown, Wanless
et al suggested that FNH is caused by hyperplasia of liver
parenchyma in response to angiodysplasia since a number of FNH
cases have involved vascular and neuroendocrine abnormalities
(17,18). An association with birth control
pills and thyroid hormones has also been proposed; however,
according to certain studies, these agents promote the growth of
FNH, but do not cause FNH (19–22).
Typical imaging findings of FNH are: i) central scar
formation, ii) nutrient vessels radiating from the center and iii)
the presence of Kupffer cells (1).
With various forms of diagnostic imaging of FNH, it is essential to
identify the spoke-wheel pattern of nutrient vessels radiating from
the center of the lesion. Although 95% of FNH >3 cm are detected
successfully, the detection of FNH <3 cm is often difficult with
a rate of 30% for FNH <3 cm and 16.7% for <2 cm by
contrast-enhanced US (3). Since
the malignant potential of FNH has been considered negative in
previous clonal studies (23–25),
patients with a definitive pre-operative diagnosis of FNH are
counter-indicated for surgical resection and are generally placed
under observation. This also means that a pre-operative needle
biopsy is essential in the diagnosis of FNH; however, a definitive
diagnosis of FNH <20 mm is often difficult to make (26). Furthermore, the use of needle
biopsy in the diagnosis of FNH has been controversial (2,12,27).
For this reason, FNH patients are generally followed-up if a
diagnosis of FNH is made following comprehensive imaging
analysis.
Since its introduction, the ultrasound contrast
agent Sonazoid has been used to thoroughly investigate the
angioarchitectonic patterns of hepatic lesions whose hemodynamics
were previously difficult to understand in detail (4–11).
In addition, the MFI function (Toshiba Medical Systems), which was
developed to analyze the angioarchitectonic patterns of hepatic
lesions, has been reported to be useful (28,29).
However, the drawback of MFI is the difficulty associated with the
evaluation of angioarchitecture and contrast agent dynamics due to
rapid monochromatic enhancement of small lesions or lesions with a
short contrast time. By contrast, At-PI has the advantage of
displaying temporal changes in contrast-enhanced imaging findings
with arbitrary colors, thus having better potential for detecting
the spoke-wheel patterns of FNH <3 cm. As anticipated, At-PI
enabled us to identify spoke-wheel patterns visually. By contrast,
it was difficult with MFI to identify spoke-wheel patterns in 2 of
5 cases, even though MFI, which traces contrast agent dynamics in
detail, proved extremely useful in the evaluation of hemodynamics
in relatively larger FNH or in FNH that contrasted slowly. In 1 of
the 2 failed cases, it took 1.7 sec to contrast the 14-mm lesion
and the lesion in another case was 17 mm and took 2.5 sec for
contrast enhancement. These tumors were small and contrasted
quickly. Even in these situations, the At-PI system enabled the
detection of nutrient vessels radiating from the center of tumors
due to the arbitrary contrast time settings. To clearly distinguish
colors, a longer interval was set to analyze tumors that contrasted
slowly, while a shorter interval was set for those that contrasted
rapidly and this led to split-second visualization of blood vessels
forming a spoke-wheel pattern.
Furthermore, while it is necessary to analyze the
video to fully understand contrast agent dynamics in MFI, At-PI
enables the diagnosis of FNH by means of a single, static,
color-mapped B-mode image that shows the direction and timing of
contrast enhancement in the tumor. Therefore, it is easy to explain
the findings of contrast agent dynamics, making the system highly
useful in a clinical setting. We consider that At-PI is an
effective tool for investigating the detailed hemodynamics of small
hepatic tumors and tumors with rapid blood flow. At-PI using
Sonazoid-enhanced US was useful for identifying spoke-wheel
patterns of FNH <3 cm.
Abbreviations:
|
FNH
|
focal nodular hyperplasia;
|
|
At-PI
|
arrival time parametric imaging;
|
|
MFI
|
micro-flow imaging;
|
|
US
|
ultrasonography;
|
|
CT
|
computed tomography
|
References
|
1.
|
Ueda K, Matsui O, Kawamori Y, et al:
Differentiation of hyper-vascular hepatic pseudolesions from
hepatocellular carcinoma: value of single-level dynamic CT during
hepatic arteriography. J Comput Assist Tomogr. 22:703–708. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Brancatelli G, Federle MP, Grazioli L,
Blachar A, Peterson MS and Thaete L: Focal nodular hyperplasia: CT
findings with emphasis on multiphasic helical CT in 78 patients.
Radiology. 219:61–68. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Ungermann L, Eliás P, Zizka J, Ryska P and
Klzo L: Focal nodular hyperplasia: spoke-wheel arterial pattern and
other signs on dynamic contrast-enhanced ultrasonography. Eur J
Radiol. 63:290–294. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Takahashi M, Maruyama H, Ishibashi H,
Yoshikawa M and Yokosuka O: Contrast-enhanced ultrasound with
perflubutane microbubble agent: evaluation of differentiation of
hepatocellular carcinoma. AJR Am J Roentgenol. 196:W123–W131. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Hiraoka A, Hirooka M, Koizumi Y, et al:
Modified technique for determining therapeutic response to
radiofrequency ablation therapy for hepatocellular carcinoma using
US-volume system. Oncol Rep. 23:493–497. 2010.
|
|
6.
|
Luo W, Numata K, Kondo M, et al:
Sonazoid-enhanced ultrasonography for evaluation of the enhancement
patterns of focal liver tumors in the late phase by intermittent
imaging with a high mechanical index. J Ultrasound Med. 28:439–448.
2009.PubMed/NCBI
|
|
7.
|
Shiozawa K, Watanabe M, Kikuchi Y, et al:
Evaluation of sorafenib for hepatocellular carcinoma by
contrast-enhanced ultrasonography: a pilot study. World J
Gastroenterol. 18:5753–5758. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Kudo M: New sonographic techniques for the
diagnosis and treatment of hepatocellular carcinoma. Hepatol Res.
37(Suppl 2): S193–S199. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Wakui N, Takayama R, Kamiyama N, et al:
Diagnosis of hepatic hemangioma by parametric imaging using
sonazoid-enhanced US. Hepatogastroenterology. 58:1431–1435. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Wakui N, Sumino Y and Kamiyama N: A case
of high-flow hepatic hemangioma: analysis by parametoric imaging
using sonazoid-enhanced ultrasonography. J Med Ultrasonics.
37:87–90. 2010. View Article : Google Scholar
|
|
11.
|
Wakui N, Takayama R, Matsukiyo Y, et al: A
case of poorly differentiated hepatocellular carcinoma with
intriguing ultrasonography findings. Oncol Lett. 4:393–397.
2012.PubMed/NCBI
|
|
12.
|
Edmondson HA: Differential diagnosis of
tumors and tumor-like lesions of liver in infancy and childhood.
AMA J Dis Child. 91:168–186. 1956.PubMed/NCBI
|
|
13.
|
Molina EG: Benign solid lesions of the
liver. Schiff's Disease of the Liver. Schiff ER, Sorrell MR and
Maddrey WC: 2. 9th edition. Lippincott Williams & Wilkins;
Philadelphia, PA: pp. 1352–1375. 2003
|
|
14.
|
Kerlin P, Davis GL, McGill DB, Weiland LH,
Adson MA and Sheedy PF II: Hepatic adenoma and focal nodular
hyperplasia: clinical, pathologic and radiologic features.
Gastroenterology. 84:994–1002. 1983.PubMed/NCBI
|
|
15.
|
Nguyen BN, Fléjou JF, Terris B, Belghiti J
and Degott C: Focal nodular hyperplasia of the liver: a
comprehensive pathologic study of 305 lesions and recognition of
new histologic forms. Am J Surg Pathol. 23:1441–1454. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Shen YH, Fan J, Wu ZQ, et al: Focal
nodular hyperplasia of the liver in 86 patients. Hepatobiliary
Pancreat Dis Int. 6:52–57. 2007.PubMed/NCBI
|
|
17.
|
Wanless IR, Mawdsley C and Adams R: On the
pathogenesis of focal nodular hyperplasia of the liver. Hepatology.
5:1194–1200. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Wanless IR, Albrecht S, Bilbao J, et al:
Multiple focal nodular hyperplasia of the liver associated with
vascular malformations of various organs and neoplasia of the
brain: a new syndrome. Mod Pathol. 5:456–462. 1989.PubMed/NCBI
|
|
19.
|
Baum JK, Bookstein JJ, Holtz F and Klein
EW: Possible association between benign hepatomas and oral
contraceptives. Lancet. 2:926–929. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Ishak KG: Hepatic neoplasms associated
with contraceptive and anabolic steroids. Carcinogenic Hormones:
Recent Results in Cancer Reseach. Lingeman CH: Springer-Verlag; New
York, NY: pp. 73–128. 1979, View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Kaji K, Kaneko S, Matsushita E, Kobayashi
K, Matsui O and Nakanuma Y: A case of progressive multiple focal
nodular hyperplasia with alteration of imaging studies. Am J
Gastroenterol. 93:2568–2572. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Nakamuta M, Ohashi M, Fukutomi T, et al:
Oral contraceptive-dependent growth of focal nodular hyperplasia. J
Gastroenterol Hepatol. 9:521–523. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Zhang SH, Cong WM and Wu MC: Focal nodular
hyperplasia with concomitant hepatocellular carcinoma. J Clin
Pathol. 57:556–559. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Chen TC, Chou TB, Ng KF, Hsieh LL and Chou
YH: Hepatocellular carcinoma associated with focal nodular
hyperplasia. Virchows Arch. 438:408–411. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Paradis V, Laurent A, Flejou JF, Vidaud M
and Bedossa P: Evidence for the polyclonal nature of focal nodular
hyperplasia of the liver by X-chromosome inactivation. Hepatology.
26:891–895. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Hisakura K, Yoshimi F, Asato Y, et al: Two
resected cases of hepatic focal nodular hyperplasia. Liver Cancer.
10:28–33. 2004.(In Japanese).
|
|
27.
|
Charny CK, Jarnagin WR, Schwartz LH, et
al: Management of 155 patients with benign liver tumors. Br J Surg.
88:808–813. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Yang H, Liu GJ, Lu MD, Xu HX and Xie XY:
Evaluation of the vascular architecture of hepatocellular carcinoma
by micro-flow imaging: pathologic correlation. J Ultrasound Med.
26:461–467. 2007.PubMed/NCBI
|
|
29.
|
Sugimoto K, Moriyasu F, Kamiyama N, et al:
Analysis of morphological vascular changes of hepatocellular
carcinoma by microflow imaging using contrast-enhanced sonography.
Hepatol Res. 38:790–799. 2008. View Article : Google Scholar
|