Introduction
Cervical cancer is one of the most common female
malignancies. In certain developing countries, cervical cancer has
the highest incidence; however, in North America and Europe, the
incidence is far lower than the incidences of breast cancer,
endometrial cancer and ovarian cancer. According to the estimates
of the International Cancer Research Center, there are ∼371,200 new
cases of cervical cancer, accounting for ∼9.8% of all tumors and
15% of female cancers annually (1). Of them, 78% of new cases appear in
developing countries, while only ∼4.4% occur in developed
countries. Annually, there are ∼100,000 new cases of cervical
cancer in China, accounting for 1/4 of the global incidence of
cervical carcinoma and ranking first in the prevalence of
gynecological malignancies (2). In
certain developing countries, cervical cancer is the leading cause
of mortality for females. In developed countries, the incidence is
significantly reduced. In certain countries, the mortality rate of
cervical cancer has been reduced by >50% as a result of the
early diagnosis and treatment of cervical precancerous lesions
(3,4). A number of studies have demonstrated
that cervical cancer is associated with human papilloma virus (HPV)
infection, particularly the high-risk HPV genotypes (5–7).
At present, a HPV genotyping assay has been adopted
in developed regions as a main method for screening cervical
lesions. A HPV vaccine is currently the first choice for the
prevention of HPV infection and consequent reduction of the
incidence of cervical cancers. Research on HPV vaccines is mainly
targeted at high-risk HPV genotypes. It is reported that persistent
infection with HPV is the crucial factor for cervical cancer
(8). To investigate the results of
the HPV vaccine and HPV examination-based screening for cervical
cancer prevention, HPV infection in large population requires
examination.
A preliminary epidemiological study has investigated
different genotypes of HPV infection in a number of regions in
China (9). However, in Xinjiang,
where the incidence of cervical cancer is highest, there have been
no region-based population surveys of HPV infection. In the current
study, the analysis of female HPV infection in the Urumqi district
of Xinjiang was examined, including assessment of age and genotype
distribution. This study provides scientific evidence for the HPV
vaccine prevention plan and support for an effective cervical
cancer prevention strategy.
Subjects and methods
Subjects
Females aged 18–69 years in the Urumqi Saybagh
district were recruited. All patients provided informed consent.
The subjects were divided into four groups, including 543 migrant
workers, 525 white-collar workers (government employees, employees
in institutionalized organizations and managers in companies), 487
workers in service industries and 714 community residents with a
total of 2,269. By the stratified cluster random sampling method,
age-stratified sampling was also applied in selected populations,
with every 5 years as the age group. Prior written and informed
consent were obtained from every patient and the study was approved
by the ethics review board of First Affiliated Hospital of Xinjiang
Medical University (Urumqi, China).
Instruments and reagents
A HPV nucleic acid amplification typing detection
reagent kit was purchased from Cape Biochemistry Ltd., Co.
(Guangdong, China). A HybriMax medical nucleic acid molecule rapid
hybridization instrument, an Autocyte Prep system for liquid-based
cytology, CytoRich Preservative fluid and an electronic colposcope
were purchased from Shenzhen Goldway Industrial Inc. (Shenzhen,
China).
HPV detection
All subjects underwent gynecological examination and
cervical secretion was collected. A genome extraction kit from Cape
Biochemistry Ltd., Co. was used for DNA extraction. Polymerase
chain reaction (PCR) amplification using the ABI7300 PCR
amplification instrument (Cape Biochemistry Ltd. Co.) and
hybridization were performed. Results were obtained by visual
observation. A clear blue purple dot was considered positive.
According to the film HPV genotype distribution map, the HPV
subtype was determined. If the two control points were positive and
other points were negative, DNA test results of HPV subtypes in the
reagent kit were considered negative. If at least one HPV genotype
point was positive, it demonstrated single or mixed HPV
infection.
Liquid-based cytology test (LCT)
An AutoCyte liquid-based thin-film machine (TriPath
Imaging Inc., BD Diagnostics, Burlington, NC, USA) was used for
automatic production and dyeing. Results were examined by optical
microscopy and cytological diagnosis was in accordance with The
Bethesda System (TBS, 2001) (10).
Colposcopy and pathological
diagnosis
For all the subjects with abnormal LCT results,
colposcopy and biopsy were performed. For positive high-risk HPV
infection in cervical secretions with atypical squamous cells of
undetermined sign and/or low-grade squamous intraepithelial lesions
in the LCT or worse, colposcopy was performed again. Biopsy was
performed by electronic colposcopy in suspicious lesions for
pathological diagnosis.
Statistical analysis
VFP software was used for database building
(Microsoft Corp, Redmond, WA, USA). SPSS 16.0 software (SPSS, Inc.,
Chicago, IL, USA) was used for statistical analysis. Data are
presented as the mean ± standard error of the mean (SEM). The HPV
infection rates in different age groups with different occupations,
cervical intraepithelial neoplasia (CIN; a premalignant cervical
disease) rate comparison of different levels and cervical lesion
HPV detection rate comparison of different degrees from
pathological results were examined by χ2 test. Single
factor analysis was performed for each factor and analyzed by the
logistic regression model. P<0.05 was considered to indicate a
statistically significant result.
Results
Detected rates of different HPV genotypes
in cervical lesions of females of different ages
In this study, 2,269 females were enrolled with an
average age of 39.65±0.203 years, ranging from 18 to 69 years. The
subjects included 543 migrant workers (individuals going to Urumqi
region to work from the other areas of China) with an average age
of 35.60±0.612 years, 525 white-collar workers (government
employees, employees in institutionalized organizations and
managers in companies) with an average age of 34.90±0.319 years,
487 workers in service industries with an average age of
32.78±0.364 years and 714 community residents with an average age
of 43.60±0.225 years.
As shown in Table
I, there were 460 positive cases of HPV, with a detection rate
of 20.27% in the whole investigated group in this study. A total of
21 HPV genotypes were detected, including 13 high-risk genotypes:
HPV-16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 68; five
low-risk genotypes: HPV-6, 11, 42, 43, 44; and three common
genotypes of Chinese individuals: HPV-53, 56 and CP8304. For the
females with infections of high-risk HPV genotypes, the high-risk
HPV genotypes were mainly HPV-16, 58, 52 and 18, which accounted
for 43.35, 18.35, 8.86 and 7.59%, respectively, of the total
infection. The four genotypes accounted for 78.16% of the high-risk
HPV genotypes.
 | Table I.Distribution of HPV genotypes
infecting females in Urumqi. |
Table I.
Distribution of HPV genotypes
infecting females in Urumqi.
| HPV genotype | Total positive
cases | Positive ratio of
populationa | Positive ratio of
groupa |
|---|
| High-risk | | | |
| HPV-16 | 137 | 137/2269 (6.03) | 137/316 (43.35) |
| HPV-18 | 24 | 24/2269 (1.05) | 24/316 (7.59) |
| HPV-31 | 21 | 21/2269 (0.93) | 21/316 (6.65) |
| HPV-33 | 13 | 13/2269 (0.57) | 13/316 (4.11) |
| HPV-35 | 0 | 0 | 0 |
| HPV-39 | 10 | 10/2269 (0.44) | 10/316 (3.16) |
| HPV-45 | 5 | 5/2269 (0.22) | 5/316 (1.58) |
| HPV-51 | 5 | 5/2269 (0.22) | 5/316 (1.58) |
| HPV-52 | 28 | 28/2269 (1.23) | 28/316 (8.86) |
| HPV-56 | 5 | 5/2269 (0.22) | 5/316 (1.58) |
| HPV-58 | 58 | 58/2269 (2.56) | 58/316 (18.35) |
| HPV-59 | 0 | 0 | 0 |
| HPV-68 | 10 | 10/2269 (0.44) | 10/316 (3.16) |
| Low-risk | | | |
| HPV-6 | 5 | 5/2269 (0.22) | 5/14 (35.71) |
| HPV-11 | 3 | 3/2269 (0.13) | 3/14 (21.43) |
| HPV-42 | 3 | 3/2269 (0.13) | 3/14 (21.43) |
| HPV-43 | 3 | 3/2269 (0.13) | 3/14 (21.43) |
| HPV-44 | 0 | 0 | 0 |
| Common type for
Chinese | | | |
| HPV-53 | 10 | 10/2269 (0.44) | 10/30 (33.33) |
| HPV-66 | 10 | 10/2269 (0.44) | 10/30 (33.33) |
| HPV-CP8304 | 10 | 10/2269 (0.44) | 10/30 (33.33) |
| Mixed infection | 100 | 100/2269 (4.41) | 100/100 (100.0) |
| Total | 460 | | |
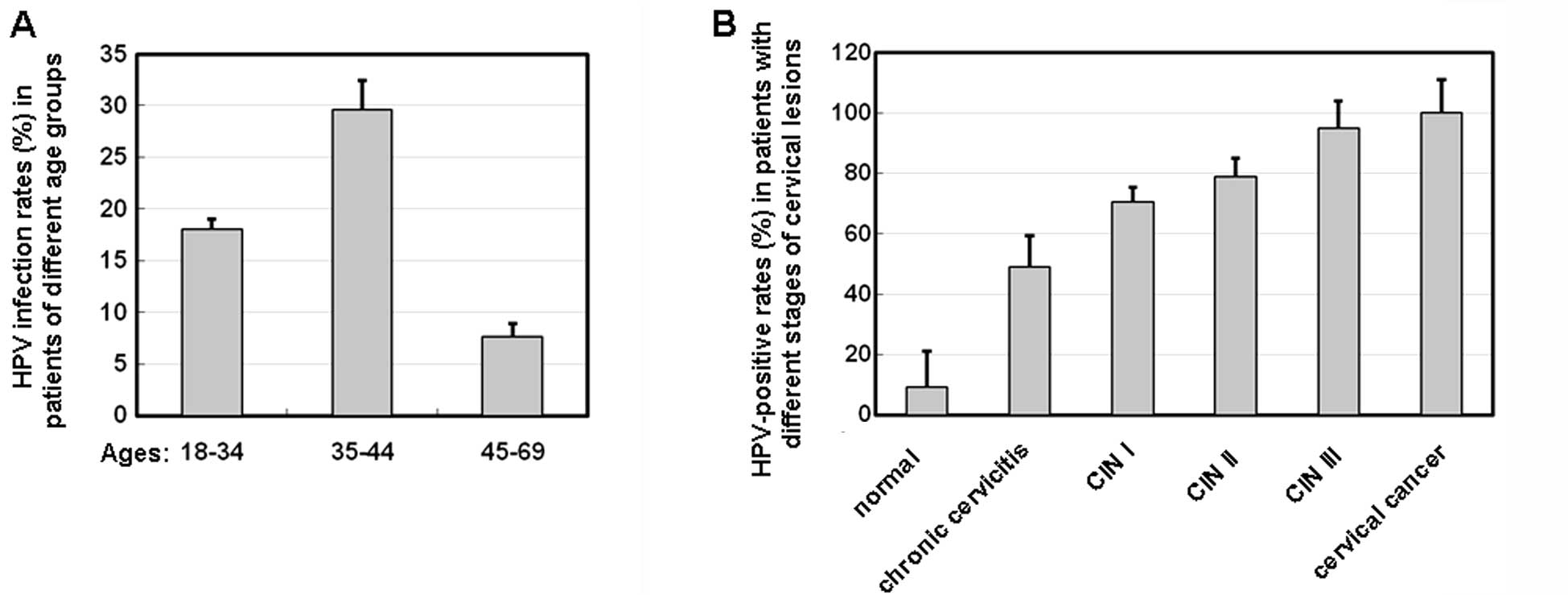
As shown in Fig.
1A, the high-risk HPV-positive rates in the three age groups
(18–34, 35–44 and 45–69 years) were 18.07, 29.64 and 7.64%
(χ2=105.02, P<0.05), respectively. The differences in
the high-risk HPV-positive rates in the three age groups were
significant (χ2=19.43, P<0.05; χ2=22.62,
P<0.01; and χ2=66.17, P<0.01, respectively).
HPV-positive rates are higher among the
groups with deteriorating cervical lesions
To determine whether HPV infection is related to
different degrees of cervical lesions, HPV infection was determined
in the patients with different degrees of cervical lesions. As
shown in Fig. 1B, the HPV-positive
rate in normal groups without symptoms of cervical lesions was ∼9%.
The HPV-positive rates in chronic cervicitis and CIN I patients
were ∼49 and 70%, respectively. The HPV-positive rates in CIN II
and CIN III patients were ∼79 and 95%, respectively. However, the
HPV-positive rate in cervical cancer patients was ∼100%. These
results suggest that HPV infection rates are increased in groups
with deteriorating cervical lesions (χ2=697.72,
P<0.05).
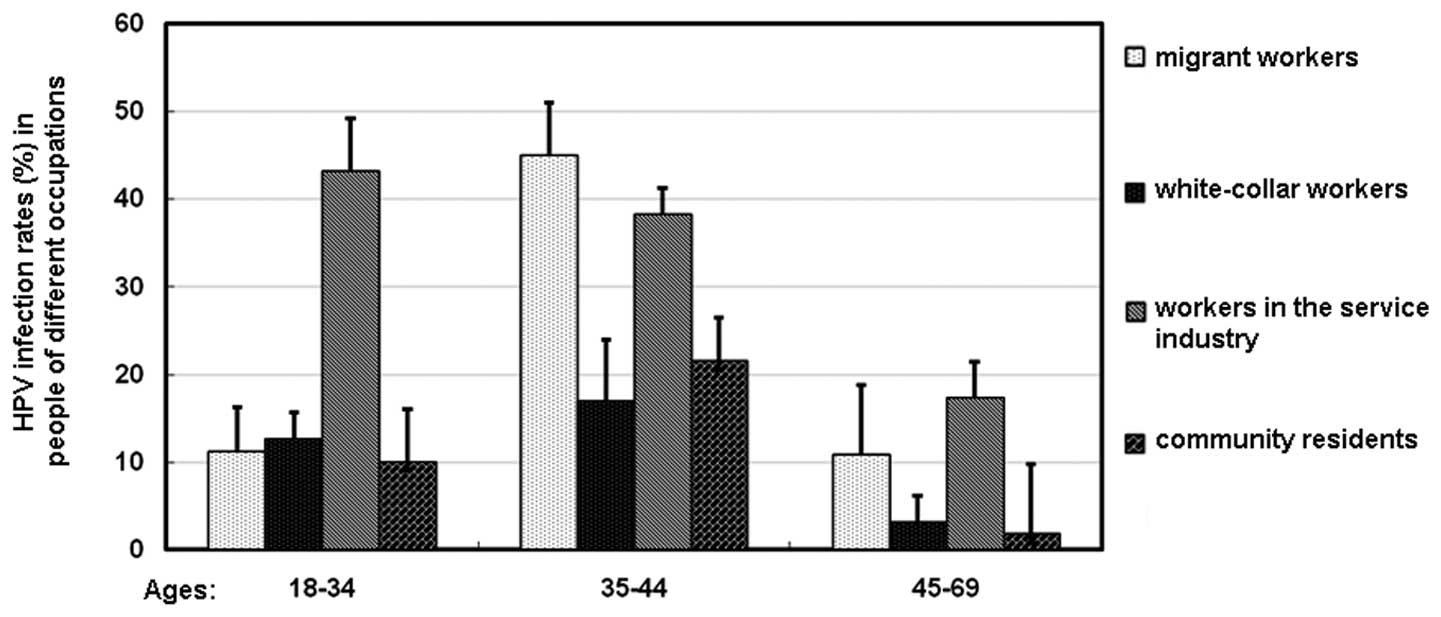
Comparison of the HPV infection rates
among different occupation groups
The HPV infection rates in patients with different
occupations were also investigated. As shown in Fig. 2, the 35–44-year-old migrant worker
group had the highest HPV infection rates among all the groups in
the three different age ranges. The HPV infection rate of females
in service industries was significantly higher compared with those
of the white-collar workers, community residents and migrant worker
groups (χ2=74.46, P<0.05; χ2=84.93,
P<0.05; and χ2=13.41, P<0.05, respectively) at all
three age ranges. These results suggest that the 35–44-year-old
migrant worker group and the service industry workers may have a
higher risk of HPV infection.
Analyses of the high-risk HPV
infections
To investigate the factors related to the HPV
infections, single analysis was performed to study the related
factors by comparing data between the HPV-positive and HPV-negative
groups. As shown in Table II,
several factors, including the number of marriages, education
level, smoking history, number of abortions, condom use, number of
sexual partners and number of sexual partners within the last 5
years, as well as occupation were significantly different between
the two groups (P<0.05; Table
II). This analysis indicates that the number of marriages,
education level, smoking history, number of abortions, use of
condoms, number of sexual partners, number of sexual partners in
the past five years and occupation were associated with HPV
infection rates (P<0.05).
| Table II.Single factor analysis of the risk
factors of HPV infection. |
Table II.
Single factor analysis of the risk
factors of HPV infection.
| Variables | HPV-positive
cases | HPV-negative
cases | OR value | 95% CI |
|---|
| Number of
marriages | | | | |
| 0 | 70 | 133 | 1 | |
| 1 | 471 | 1405 | 0.632a | 0.408–1.001 |
| ≥2 | 93 | 97 | 1.786a | 1.022–3.369 |
| Education level | | | | |
| Junior high school
or below | 464 | 863 | 1 | |
| High school or
above | 169 | 773 | 0.369a | 0.304–0.601 |
| Married | | | | |
| Yes | 551 | 1445 | 1 | |
| No | 82 | 191 | 0.854 | 0.534–1.313 |
| History of cervical
disease | | | | |
| Yes | 384 | 982 | 1 | |
| No | 250 | 653 | 1.019 | 0.765–1.343 |
| Tuberculosis | | | | |
| Yes | 4 | 8 | 1 | |
| No | 630 | 1627 | 1.289 | 0.231–7.083 |
| History of STDs | | | | |
| Yes | 25 | 55 | 1 | |
| No | 609 | 1580 | 1.187 | 0.587–2.402 |
| History of
smoking | | | | |
| No | 303 | 904 | 1 | |
| Yes | 331 | 731 | 1.349a | 1.039–1.771 |
| Age of first
menstruation | | | | |
| ≤11 years | 106 | 297 | 1 | |
| 12–15 years | 432 | 1078 | 1.133 | 0.791–1.622 |
| ≥16 years | 95 | 261 | 1.041 | 0.641–1.649 |
| Menopause | | | | |
| Yes | 93 | 233 | 1 | |
| No | 541 | 1402 | 1.032 | 0.712–1.523 |
| Abortion | | | | |
| Yes | 74 | 231 | 1 | |
| No | 560 | 1404 | 0.811 | 0.532–1.201 |
| Number of
abortions | | | | |
| 1 | 184 | 598 | 1 | |
| 2 | 237 | 545 | 1.415a | 1.024–1.961 |
| ≥3 | 212 | 493 | 1.406a | 1.001–1.972 |
| Condom use | | | | |
| Yes | 216 | 666 | 1 | |
| No | 418 | 969 | 1.334a | 1.005–1.761 |
| Number of sexual
partners | | | | |
| 1 | 500 | 1430 | 1 | |
| 2 | 91 | 140 | 1.855a | 1.231–2.807 |
| ≥3 | 42 | 66 | 1.901a | 1.603–3.422 |
| Number of sexual
partners in the past 5 years | | | | |
| 1 | 479 | 1366 | 1 | |
| 2 | 87 | 157 | 1.577a | 1.042–2.376 |
| ≥3 | 67 | 113 | 1.749a | 1.103–2.789 |
| Sexual intercourse
outside marriage | | | | |
| Yes | 50 | 140 | 1 | |
| No | 583 | 1496 | 0.933 | 0.569–1.523 |
| Age at first sexual
intercourse | | | | |
| ≤18 years | 129 | 295 | 1 | |
| 19–22 years | 224 | 668 | 0.761 | 0.524–1.121 |
| ≥23 years | 280 | 673 | 0.931 | 0.637–1.336 |
| Occupation | | | | |
| Community
residents | 91 | 623 | 1 | |
| White-collar
workers | 64 | 461 | 1.902 | 0.831–1.743 |
| Migrant
workers | 134 | 409 | 3.288a | 2.241–4.851 |
| Workers in
service industry | 171 | 316 | 3.995a | 2.473–5.247 |
To further confirm the results, logistic regression
model analysis was performed on variables with statistical
significance in univariate analysis (α in=0.05, α out=0.10; in, the
inclusion criteria; out, the exclusion criteria). The data in
Table III shows that education
level, number of sexual partners, condom use and occupation were
incorporated into the model. The results suggest that education
level and condom use were two protective factors of HPV infection,
while the number of sexual partners and occupation were risk
factors for HPV infection.
| Table III.Multiple factor analysis of the risk
factors of HPV infection. |
Table III.
Multiple factor analysis of the risk
factors of HPV infection.
| Factor | B | SE | Wald | df | P-value | Exp(B) | 95% CI for Exp(B)
|
|---|
| Lower | Upper |
|---|
| Education
level | −0.871 | 0.152 | 32.233 | 1 | 0.000 | 0.423 | 0.301 | 0.559 |
| Number of sexual
partners | 0.326 | 0.133 | 5.923 | 1 | 0.012 | 1.379 | 1.062 | 1.791 |
| Condom use | −0.372 | 0.146 | 6.238 | 1 | 0.009 | 0.681 | 0.509 | 0.919 |
| Occupation | 0.453 | 0.061 | 51.949 | 1 | 0.000 | 1.581 | 1.389 | 1.778 |
Discussion
In this study, a stratified cross-sectional survey
was performed to conduct genotyping detection of 21 types of HPV in
a large sample. The distribution of HPV-DNA subtypes varies in
different districts and ethnic groups. de Sanjosé et al
(11) conducted a meta-analysis of
HPV infection in six regions of the world in 157,879 females
without cervical lesions (by cytological diagnosis). The HPV
infection rate was ∼10.4%.
The prevalence of HPV infection varies
significantly. The HPV infection rates are as follows: 22.1% in
Africa, 20.4% in the central United States and Mexico, 11.3% in
North America, 8.1% in Europe and 8.0% in Asia (11). Bell et al (12) determined the mean HPV infection
rate of 287 American Indian females (by PCR assay) to be 21.25%. Of
these, 67.2% was high-risk HPV infection and 41% was multiple
infection, and the common HPV infection subtypes were HPV-59, 39
and 73. In China, Li and Dai (13)
conducted a study to determine the HPV infection rate in three
regions of Shanxi, Shenyang and Shenzhen. The authors identified
that the HPV infection rate was 16.1% and HPV-16 is the most common
virus type, followed by HPV-58, 52 and 18 (13). In the present study, we identified
that the HPV infection rate in Urumqi, Xinjiang is 20.27%, higher
than that of Europe and the results of the study by Li and Dai, and
similar to that of American Indian females, which may be explained
by the fact that Xinjiang is an area with a high incidence of
cervical cancer. We demonstrated that the common subtypes in
Urumqi, Xinjiang are HPV-16, 58, 52 and 18, which is similar to the
results of the study by Li and Dai (8). The existing vaccines are only
effective for subtypes 16 and 18; however, 58 and 52 are also
highly prevalent. Therefore, a customized HPV vaccine is required
for the prevention and treatment of cervical lesions in Chinese
females.
In a number of developed countries, including Spain
and South Korea, the HPV infection peak usually occurs in young
individuals under the age of 25 years and it declines sharply as
age increases. In certain areas of South America, the HPV infection
rate of 35–54-year-olds is lower than that of younger individuals
(<25 years) and elderly individuals (>55 years). In countries
with a high incidence of cervical cancer, including India and
Nigeria, the HPV infection rate of individuals aged 35–54 years is
higher than that in younger individuals (<25 years) and elderly
individuals (>55 years) (14).
In the present study, we identified that that the infection rate of
individuals aged 35–44 years is significantly higher than that in
younger individuals (18–34 years) and elderly individuals (>45
years). The infection rate of HPV in the younger individuals was
significantly higher than that in the elderly group. Our results
are similar to data in India and Nigeria, but different from data
in developed countries including Spain and South Korea. The high
infection rate in the 35 to 44 age group was possibly due to the
reason that females in that age group are sexually active.
HPV infection rates were increased with aggravated
cervical lesions. The HPV infection rate in cervical cancer was
100%, demonstrating again the correlation between cervical cancer
and HPV infection. HPV infection rates in different age groups with
different professions were also examined. The HPV infection rate of
workers in service industries was significantly higher than the
infection rates of white-collar workers, community residents and
migrant workers. Among workers in service industries, the HPV
infection rate of females aged 18–34 years was higher than that of
those aged 35–44 and 45–69 years. This indicates that female
workers in service industries aged 18–34 years are the most
sexually active. A lack of health protection is a possible reason
for the high HPV infection rate.
In this study, we identified that the number of
marriages, education level, smoking history, number of abortions,
condom use, number of sexual partners, number of sexual partners in
the past five years and occupation are risk factors for HPV
infection. A large number of epidemiological studies have shown
that a premature sex life, multiple sexual partners, unprotected
sexual intercourse and abortion increase the risk of cervical
cancer (15–17). One study reported that as the
smoking time increases, the risk of cervical cancer increases
(18). In the current study,
smoking was also observed to be a risk factor for HPV infection.
The use of condoms avoids cross-infection, thus reducing the
prevalence of HPV.
In conclusion, the infection rate of HPV is high in
Urumqi, Xinjiang, with HPV-16, 58, 52 and 18 as the common
genotypes. Since females aged 35–44 years have the highest rate of
infection, screening of cervical lesions and health habit guidance
should be performed.
Acknowledgements
This study was supported by the
National Natural Science Foundation of China (grant no. 81101555)
and the Project of the Opening Laboratory of Infection and Immunity
(grant no. GRMY-2011-05), operated by Institute Pasteur of
Shanghai, Chinese Academy of Sciences and the First Affiliated
Hospital, Xinjiang Medical University.
References
|
1.
|
Louie KS, de Sanjose S, Diaz M, et al:
Early age at first sexual intercourse and early pregnancy are risk
factors for cervical cancer in developing countries. Br J Cancer.
100:1191–1197. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Lang J: Problems in connection with
diagnosis and treatment of cervical lesions. Zhonghua Fu Chan Ke Za
Zhi. 36:261–263. 2001.(In Chinese).
|
|
3.
|
Weinstein LC, Buchanan EM, Hillson C, et
al: Screening and prevention: cervical cancer. Prim Care.
36:559–574. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Cuzick J, Arbyn M, Sankaranarayanan R, et
al: Overview of human papillomavirus-based and other novel options
for cervical cancer screening in developed and developing
countries. Vaccine. 26(Suppl 10): K29–K41. 2008. View Article : Google Scholar
|
|
5.
|
Cruickshank ME: The role of human
papillomavirus in risk management. Rev Gynaecol Practice.
3:292–233. 2003. View Article : Google Scholar
|
|
6.
|
Walboomers JM, Jacobs MV, Manos MM, et al:
Human papillomavirus is a necessary cause of invasive cervical
cancer worldwide. J Pathol. 189:12–19. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Pilch H, Günzel S, Schäffer U, et al: The
presence of HPV DNA in cervical cancer: correlation with
clinico-pathologic parameters and prognostic significance: 10 years
experience at the Department of Obstetrics and Gynecology of the
Mainz University. Int J Gynecol Cancer. 11:39–48. 2001.
|
|
8.
|
Stevens MP, Garland SM, Tan JH, et al: HPV
genotype prevalence in women with abnormal pap smears in Melbourne,
Australia. J Med Virol. 81:1283–1291. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Wu K, Fu Y and Jiang H: Molecular
epidemiology analysis of cervical HPV in women of childbearing age
in Guangzhou, China. Guangdong Med. 25:386–391. 2004.(In
Chinese).
|
|
10.
|
Prandi S, Beccati D, De Aloysio G, et al:
Applicability of the Bethesda System 2001 to a public health
setting. Cancer. 108:271–276. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
de Sanjosé S, Diaz M, Castellsagué X, et
al: Worldwide prevalence and genotype distribution of cervical
human papillomavirus DNA in women with normal cytology: a
meta-analysis. Lancet Infect Dis. 7:453–459. 2007.PubMed/NCBI
|
|
12.
|
Bell MC, Schmidt-Grimminger D, Patrick S,
Ryschon T, Linz L and Chauhan SC: High prevalence of human
papillomavirus infection in American Indian women of the Northern
Plains. Gynecol Oncol. 2:236–241. 2007.(In Chinese).
|
|
13.
|
Li N and Dai M: Human papillomavirus
infection in China: a multi-centric cross-sectional study. Chinese
Journal of Disease Control and Prevention. 12:411–415. 2008.
|
|
14.
|
Franceschi S, Herrero R, Clifford GM, et
al: Variations in the age-specific curves of human papillomavirus
prevalence in women worldwide. Int J Cancer. 119:2677–2684. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Zeng ZP, Chen F, Liu B, et al: Studies of
risk factors of cervical cancers in Yangcheng County, Shanxi
Province, China. Tumor Prevention Research. 31:178–181. 2004.
|
|
16.
|
Zhao FH, Ma JF, Qiao YL, et al:
Association between high-risk human papillomavirus DNA load and
cervical intraepithelial lesion. Zhonghua Liu Xing Bing Xue Za Zhi.
25:921–924. 2004.(In Chinese).
|
|
17.
|
Zhao FH, Forman MR, Belinson J, et al:
Risk factors for HPV infection and cervical cancer among unscreened
women in a high-risk rural area of China. Int J Cancer.
118:442–448. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Deacon JM, Evans CD, Yule R, et al: Sexual
behaviour and smoking as determinants of cervical HPV infection and
of CIN3 among those infected: a case-control study nested within
the Manchester cohort. Br J Cancer. 83:1565–1572. 2000. View Article : Google Scholar
|