Introduction
A dermoid cyst is a rare benign tumor, which is
principally situated close to the midline of the body. It is a
developmental lesion, histologically composed of ectoderm and
mesoderm; however, it has no endoderm. In approximately 7% of
cases, these cysts affect the head and neck region; they are
frequently encountered in the area of the lateral eyebrow, the
orbit and the nose (>80%), with the remainder located in the
neck, occipital or frontal midline, lip or palate (1). However, little is known about dermoid
cysts in the subcutaneous tissue of the mastoid region. We report a
case of a dermoid cyst in the subcutaneous tissue of the mastoid
region without hearing loss and vertigo, which was misdiagnosed as
an intumescent retroauricular lymph node. The location of this
tumor and its clinical features make this a unique case.
Case report
The patient was a 22-year-old male presenting a lump
that had grown gradually under the skin of the right mastoid for 2
years. The patient denied any hearing loss or vertigo. There was no
pain and no inflammation in the lump. The patient was healthy, with
the exception of the lump. The patient had been assessed at the
community hospital one year earlier and was treated with
antibiotics, which were ineffective. The patient then came to
Xijing Hospital (Xi’an, China) for further evaluation and
treatment.
On examination, the two ears appeared normal. The
patient had normal and symmetrical facial and cervical structures
with no deformities of the pinnae or external auditory canals. The
ear drums were normal and no air-fluid levels or bubbles were
observed behind the drum. Impedance audiometry and audiogram were
also normal. There were no significant findings in the remainder of
the head and neck examination, with the exception of the tumor,
which was initially considered a retroauricular lymph node.
Surgical biopsy was performed with the patient under
local anesthesia. When the skin flap was opened, a pink
encapsulated mass was observed occupying the right mastoid surface.
The mass extended from the subcutaneous tissue to the mastoid
cortical plate without destruction of the mastoid bony wall. The
tumor and mastoid cortical plate were umbilicated in the mastoid
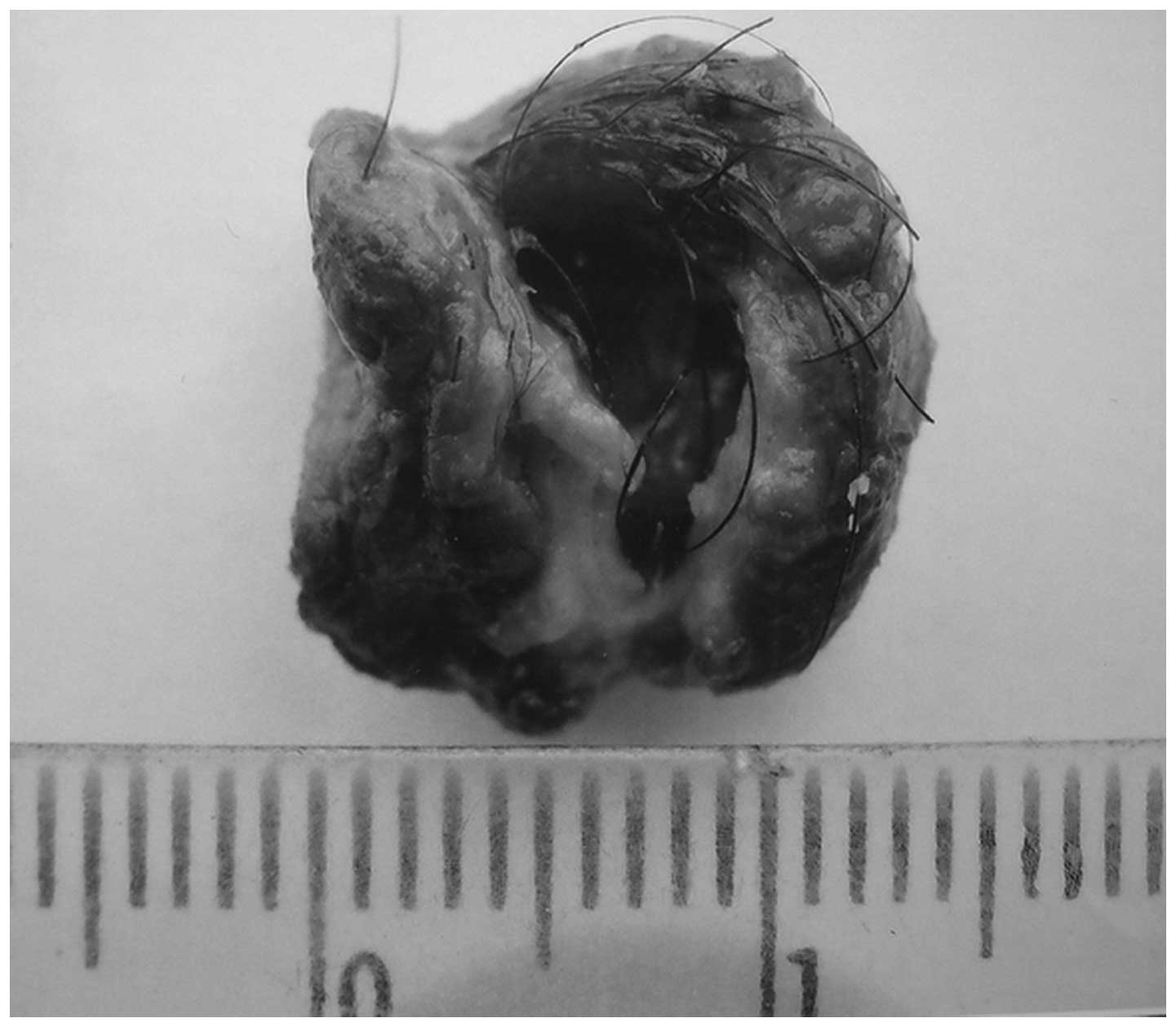
cavity. The mastoid cavity maintained integrity. The surface of the
mass was granulated and a number of hairs were observed in the
tumor when it was slivered. The diameter of the tumor was
approximately 1.3×10−2 m (Fig. 1). Following complete removal of the
tumor, the defect was reinforced with muscle and fascia.
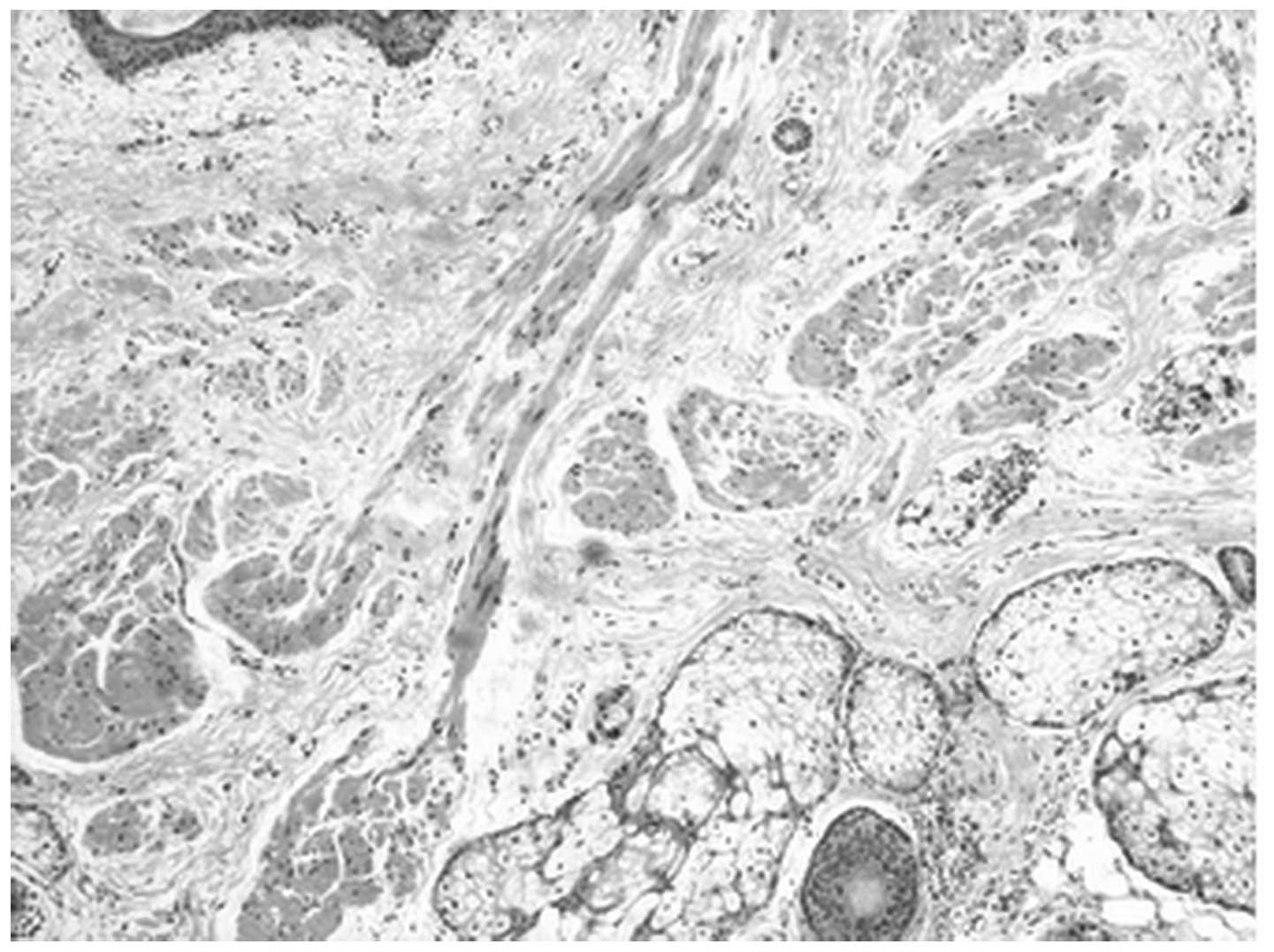
Pathological analysis confirmed the diagnosis that
the tumor was a dermoid cyst (Fig.
2). Two years after surgery there was no evidence of any
recurrent tumor in the region of the right mastoid. All studies
were performed under the consent of the patient and with approval
from the Human Studies Committee of the Xijing Hospital of the
Fourth Military Medical University.
Discussion
Dermoid cysts are tumors composed of two germ
layers, ectoderm and mesoderm. They are epithelial-lined cavities
with skin appendages, including hair, hair follicles and sebaceous
glands. This distinguishes them from cholesteatomas, which are
composed only of ectodermal elements, and teratomas, which are
composed of ectodermal, mesodermal and endodermal elements.
Dermoid cysts may occur anywhere in the body. They
primarily occur in the gonads; however, they also occur at
extragonadal sites along the midline of the body. The head and neck
region is a rare location for such tumors in children and adults.
Therefore, the pathological evaluation and clinical management of
these tumors is extremely difficult. Toynbee reported the first
case of a dermoid cyst of the mastoid in 1866, when hairs were
identified in the mastoid cavity surrounded by epidermis (2). Howie discovered a dermoid cyst in the
middle ear of a 29-year-old female who presented symptoms of
hearing loss and vertigo (3).
Steel reviewed reports on dermoid cysts in the mastoid from 1866 to
1976 and identified four cases in the literature that referred to
non-hair-bearing cysts in the mastoid. Steel also reported a
67-year-old male who had been treated for intermittently-active
chronic otitis media 4 years, which was the result of a dermoid
cyst in the middle ear (4). Fried
and Vernick published a report on a patient aged 22 months who had
a dermoid cyst of the middle ear and mastoid (5). Minatogawa et al reported on a
6-year-old female patient with a dermoid cyst in the middle ear and
low-tone unilateral conductive hearing loss (6). Farris et al reported on an
8-month-old female who was the youngest patient with a congenital
dermoid cyst of the middle ear with a moderate conductive hearing
loss of the ear in 1998. It was suggested that congenital inclusion
may be the cause of the majority of dermoid cysts in the head and
neck (7). Scolozzi et al
reported a case of a 1-year-old female who was initially seen with
a cutaneous fistula of the frontotemporal region, which revealed an
intracranial dermoid cyst (8). Due
to the small number of patients reported, little generalization has
been made about the presentation of dermoids of the mastoid and
middle ear. No gender preponderance has been noted.
The patient in our study was unique in several
respects and there are no previous reports of similar cases. The
patient had no symptoms, with the exception of the
histologically-confirmed dermoid cyst in the subcutaneous tissue of
the mastoid region. Patients previously reported often had a
dermoid cyst in the mastoid and middle ear and usually suffered
from hearing loss and vertigo. However, in this case, the dermoid
cyst extended from the subcutaneous tissue to the right mastoid,
the mastoid cavity was undamaged and hearing loss and vertigo did
not appear. Therefore, prior to pathological analysis, it was
easily confused with an intumescent lymph node.
As with the majority of cysts, local recurrence at
the primary site is common unless the entire wall of the cyst is
removed. Therefore, complete excision of the cyst during surgery
must be ensured.
Although uncommon, dermoid cysts must be considered
in the differential diagnosis of lumps in the mastoid region.
However, their pre-operative differentiation from a retroauricular
lymph node is not easy. Complete resection of the tumor is required
and pathological analysis is important for the diagnosis.
Acknowledgements
The authors thank Wei Yan for help in
section-staining and evaluating the specimen. This study was
supported by the National Natural Science Foundation of People’s
Republic of China (No. 30772261).
References
|
1.
|
Batsakis JG: Teratomas of the head and
neck. Tumours of the Head and Neck. 2nd edition. Lippincott
Williams and Wilkins; Baltimore, MD: pp. 226–232. 1979
|
|
2.
|
Toynbee J: Hairs in the mastoid cells.
Transactions of the Pathological Society of London. 17:2741866.
|
|
3.
|
Howie TO: A case of dermoid or
developmental cyst of the middle-ear cavity. J Laryngol Otol.
76:62–66. 1962. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Steel A: Secretory otitis media due to a
hair-bearing dermoid of the mastoid cavity. J Laryngol Otol.
90:979–989. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Fried MP and Vernick DM: Dermoid cyst of
the middle ear and mastoid. Otolaryngol Head Neck Surg. 92:594–596.
1984.PubMed/NCBI
|
|
6.
|
Minatogawa T, Node MN, Fukuda I and Kumoi
T: Dermoid cyst in the middle ear. J Laryngol Otol. 107:335–338.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Farris PE, Meyerhoff WL and Vuitch F:
Congenital dermoid cyst of the middle ear. Skull Base Surg.
8:77–80. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Scolozzi P, Lombardi T and Jaques B:
Congenital intracranial frontotemporal dermoid cyst presenting as a
cutaneous fistula. Head Neck. 27:429–432. 2005. View Article : Google Scholar : PubMed/NCBI
|