Introduction
A schwannoma is a benign encapsulated nerve sheath
tumor arising from Schwann cells. It occurs predominantly in
middle-aged adults with no gender predilection. Patients typically
present with a slowly growing, painless mass in the head, neck and
flexor surfaces of the upper and lower extremities. An
intramuscular schwannoma is rare and its clinical behavior may be
different from that of a schwannoma occurring in other locations
(1,2). We present an unusual case of an
intramuscular schwannoma originating from the musculocutaneous
nerve in an elderly female. To the best of our knowledge, this is
the first description of a musculocutaneous nerve schwannoma within
the coracobrachialis muscle. Written informed consent for
publication was obtained from the patient.
Case report
A 71-year-old female was referred to Fukuoka
University (Fukuoka, Japan) with a 7-month history of a slowly
growing, painless mass in the medial aspect of the right proximal
upper arm. Physical examination revealed an elastic-hard, poorly
mobile, non-tender mass. Neurovascular examinations, including
Tinel’s sign, were normal. Laboratory data were within normal
limits. The patient’s past medical history was unremarkable.
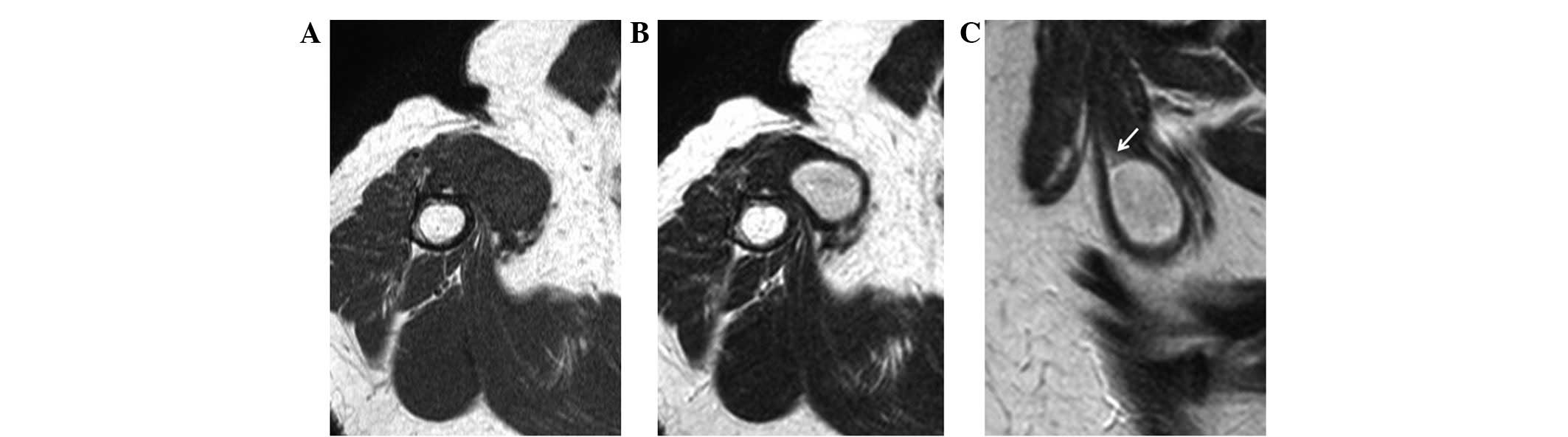
Magnetic resonance imaging (MRI) demonstrated an oval-shaped soft
tissue mass in the right coracobrachialis muscle, measuring
3.0×2.0×2.0 cm. The mass presented homogeneous iso-signal intensity
relative to skeletal muscle on T1-weighted images (Fig. 1A) and high signal intensity on
T2-weighted images (Fig. 1B). A
rim of fat surrounding the mass was also observed (Fig. 1C). Based on these findings, a
preoperative diagnosis of a benign neurogenic tumor, including
intramuscular schwannoma was made.
Surgery was performed under general anesthesia.
First, the tumor and the proximal and distal portions of the
affected nerve were exposed (Fig.
2A). A longitudinal incision was carefully made in the
epineurium far away from the fascicles. The epineurial layers were
gently peeled away until the shiny surface of the tumor was
exposed. The entire tumor mass was shelled out in one piece without
damage to the fascicles. Intraoperative findings were consistent
with the diagnosis of schwannoma. Grossly, the smooth-surfaced
tumor was yellow-whitish (Fig.
2B). Microscopically, the tumor demonstrated a proliferation of
spindle-shaped cells arranged in short bundles or interlacing
fascicles in Antoni A areas (Fig.
2C). Edematous, hypocellular areas known as Antoni B were also
observed (Fig. 2D). Neither
nuclear atypia nor mitotic figures were observed. These features
confirmed the diagnosis of a schwannoma.
There was no immediate neurological deficit
following surgery. At six months of follow-up, the patient had no
evidence of recurrence and no neurological deficit.
Discussion
The musculocutaneous nerve arises from the lateral
cord of the brachial plexus. It penetrates the coracobrachialis
muscle at the level of the tendon of the latissimus dorsi
muscle and passes obliquely between the biceps brachii muscle and
the brachialis muscle to continue into the forearm as the lateral
antebrachial cutaneous nerve (3,4). Its
initial branches are motor in function and the remaining fibers are
sensory in function at the cubital fossa. Although few cases of
schwannoma originating from the musculocutaneous nerve have been
documented (2,5), there is, to the best of our
knowledge, no literature describing a musculocutaneous nerve
schwannoma within the coracobrachialis muscle.
The histological hallmark of a schwannoma is the
pattern of alternating Antoni A and B areas, as demonstrated in the
present case. The relative amounts of these two components vary and
may blend imperceptibly or change abruptly. Antoni A tissue is
highly cellular and demonstrates nuclear palisading and associated
Verocay bodies. Antoni B tissue is less cellular and lacks
distinctive architectural features. A number of schwannomas have
thick-walled vessels with fibrinoid and hyaline changes in the
vessel walls. When examined by immunohistochemistry, schwannomas
typically show diffuse, strong expression of S-100 protein and
abundant pericellular collagen type IV (6). Unlike neurofibroma, neurofilament
protein staining is usually limited to entrapped axons at the
periphery of the tumor.
Intramuscular schwannomas are rare (5); they originate from a small nerve
branch within the muscle. The clinical features are different from
those of schwannomas occurring in other locations (1,2). In
intramuscular schwannomas, neurological symptoms or signs,
including pain, Tinel’s sign, sensory disturbance or motor
weakness, are few. It may therefore be difficult to identify the
neurogenic origin based on physical examination. Using MRI, the
majority of lesions demonstrate iso- or low signal intensity on
T1-weighted images and high signal intensity on T2-weighted images,
as shown in the present case. Post-contrast images show marked
central enhancement (1). In the
present case, the origin of the tumor was not a small motor branch
but a trunk of the musculocutaneous nerve. Despite its rare
occurrence, it is important to be aware of the possible existence
of a major nerve trunk schwannoma in the coracobrachialis
muscle.
Enucleation is a standard surgical procedure for
schwannomas. However, certain schwannomas are not easily enucleated
and enucleation may result in iatrogenic nerve injury, even with
atraumatic procedures. Donner et al (7) recommended extracapsular enucleation
with good results; however, the procedure is likely to damage the
fascicles in the capsular layer during dissection. Previously,
intracapsular enucleation has been performed to minimize the risk
of nerve injury (8–10). Date et al (9) reported that neurological deficit
following enucleation is significantly lower using the
intracapsular compared with the extracapsular technique. The
authors mentioned that en bloc resection should not be performed
since the main purpose of schwannoma surgery is the relief of
symptoms. In the present case, gentle dissection along the plane of
the tumor capsule from the epineurial layers allowed the tumor to
be shelled out in one piece without disturbing the fascicles.
In summary, we have reported the first case of an
intramuscular schwannoma originating from the musculocutaneous
nerve. Although rare, schwannomas should be included in the
differential diagnosis of a well-defined, oval-shaped soft tissue
mass arising within the coracobrachialis muscle.
Acknowledgements
This study was supported in part by
the Ogata Foundation and the Foundation for the Promotion of
Medical Science.
References
|
1.
|
Kwon BC, Baek GH, Chung MS, Lee SH, Kim HS
and Oh JH: Intramuscular neurilemoma. J Bone Joint Surg Br.
85:723–725. 2003.
|
|
2.
|
Shimose S, Sugita T, Kubo T, Matsuo T,
Nobuto H, Tanaka K, Arihiro K and Ochi M: Major-nerve schwannomas
versus intramuscular schwannomas. Acta Radiol. 48:672–677. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Osborne AW, Birch RM, Munshi P and Bonney
G: The musculo-cutaneous nerve. J Bone Joint Surg Br. 82:1140–1142.
2000. View Article : Google Scholar
|
|
4.
|
Tagliafico AS, Michaud J, Marchetti A,
Garello I, Padua L and Martinoli C: US imaging of the
musculocutaneous nerve. Skeletal Radiol. 40:609–616. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Knight DM, Birch R and Pringle J: Benign
solitary schwannomas: a review of 234 cases. J Bone Joint Surg Br.
89:382–387. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Rodriguez FJ, Folpe AL, Giannini C and
Perry A: Pathology of peripheral nerve sheath tumors: diagnostic
overview and update on selected diagnostic problems. Acta
Neuropathol. 123:295–319. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Donner TR, Voorhies RM and Kline DG:
Neural sheath tumors of major nerves. J Neurosurg. 81:362–373.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Park MJ, Seo KN and Kang HJ: Neurological
deficit after surgical enucleation of schwannomas of the upper
limb. J Bone Joint Surg Br. 91:1482–1486. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Date R, Muramatsu K, Ihara K and Taguchi
T: Advantages of intra-capsular micro-enucleation of schwannoma
arising from extremities. Acta Neurochir (Wien). 154:173–178. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Kim SM, Seo SW, Lee JY and Sung KS:
Surgical outcome of Schwannomas arising from major peripheral
nerves in the lower limb. Int Orthop. 36:1721–1725. 2012.
View Article : Google Scholar : PubMed/NCBI
|