Introduction
Female pattern hair loss (FPHL), characterized by a
diffused reduction in hair thickness, is the most common cause of
hair loss in women and affects >50% of women at the age of 80
(1). Furthermore, an
epidemiological survey in northern China suggested that the
incidence was 6.0% in females, lower than that in Western countries
(2). However, due to the large
population in China, the number of women with FPHL in China is
higher. Although it is a mild dermatological disorder,
psychologists and dermatologists have observed that even clinically
imperceptible hair loss is capable of damaging the quality of life
(QoL) of patients due to the loss of self-image and diminished
self-esteem (3,4). Women with hair loss have reported
experiencing adverse psychosocial reactions, including
irritability, anger, anxiety and depression, due to the significant
sexual and social functions of the appearance of their hair
(5–8).
Treatment options are currently limited and a
substantial length of time is required to reach a satisfactory
outcome. FDA-approved minoxidil topical solution is an effective
and safe treatment for female androgenetic alopecia which acts by
promoting hair follicle cycling and prolonging aging (9,10).
The treatment needs to be continued for at least 12 months prior to
performing an accurate efficacy evaluation (11). However, few studies have examined
the impact of topical minoxidil treatment on the QoL of female
patients. This study was designed to assess the QoL in patients
with FPHL (n=125) and determine the effectiveness of topical
minoxidil treatment in improving the QoL of these patients
(n=31).
Patients and methods
Patients and study design
We recruited 125 FPHL patients to answer visual
analog scale (VAS) (12) and
dermatology life quality index (DLQI) questionnaires (13). Of these, 31 patients were recruited
for the follow-up study in which they were treated with topical 2%
minoxidil solution (1 ml applied twice daily) for 12 months and
then completed the same surveys. The general characteristics of the
patients are described in Table I.
This study was approved by the Nanjing Medical University
Institutional Review Board. Written consent was obtained from all
patients prior to enrollment.
 | Table I.Patient characteristics (n=125). |
Table I.
Patient characteristics (n=125).
| Characteristic | Value |
|---|
| Age (years) | 32.210±10.351 |
| Disease duration
(months) | 31.770±34.446 |
| Ludwig score
(cases) | |
| I | 57 |
| II | 46 |
| III | 22 |
Study assessments
Two indices were used to evaluate the improvement of
patients receiving treatment for 12 months. Each patient was
assessed as one of four grades, namely: ‘significant improvement’,
‘improvement’, ‘no change’ and ‘worsening’ A ‘significant
improvement’ was defined as an increase in the Ludwig score by two,
while ‘improvement’ was defined as an increase in the Ludwig score
by one. A reduction of the score by one or two was considered
‘worsening’. Patients assessed as having a ‘significant
improvement’ or ‘improvement’ were defined as ‘good responders’
while those deemed to have ‘no change’ or to be ‘worsening’ were
defined as ‘poor responders’. The improved value of each QoL index
was compared with the baseline.
DLQI
We modified certain items in the index to ensure it
was appropriate for alopecia patients (Table II). One of the endpoints of the
study was the mean DLQI score for the first-visit patients. The
other major endpoint was the mean improvement in the DLQI score
from the baseline to 12 months later. Each question has four
alternative responses with corresponding scores of 0, 1, 2 and 3,
respectively. The DLQI was calculated by summing the scores of all
questions, with total scores ranging from 0–30, where a lower score
indicates a lower QoL.
| Table II.DLQI and VAS questionnaire. |
Table II.
DLQI and VAS questionnaire.
| No. | Question |
|---|
| 1 | Over the last week,
how have you been affected by alopecia? Have you felt burning,
pain, itching, irritation or oils on your scalp? |
| 2 | Over the last week,
how embarrassed, frustrated or self conscious have you been because
of your alopecia? |
| 3 | Over the last week,
how much has your alopecia interfered with your shopping or other
outdoor activities? |
| 4 | Over the last week,
how much has your alopecia influenced your hair style? Do you need
to wear a hat, wig or special hair type to cover the thinner
area? |
| 5 | Over the last week,
how much has your alopecia affected any social or leisure
activities? |
| 6 | Over the last week,
how much has your alopecia made it difficult for you to do any
sport or hobbies? |
| 7 | Over the last week,
has your alopecia prevented you from working or studying? |
| 8 | Over the last week,
how much has your alopecia created problems with your partner or
any of your close friends or relatives? |
| 9 | Over the last week,
how much has your alopecia caused any sexual difficulties? |
| 10 | Over the last week,
how much of a problem has the treatment for your alopecia been, for
example by making your home messy or taking up time? |
| 11 | Assess your alopecia
condition yourself from score 0–100 (VAS). |
VAS
Subjective assessment (the patient’s perception of
hair loss severity) of the 125 first-visit patients and a
comparison between the assessment results prior to and following
treatment were conducted using a VAS (8,12,14–16)
in which the patient’s evaluation was scored from 0 (completely
dissatisfied) to 100 (completely satisfied). The VAS is a simple
tool for measuring the satisfaction of the patients regarding the
state of their hair loss and the effect of the treatment.
Statistical analyses
The Kruskal-Wallis Test was used to analyze the
correlation between clinical characteristics (age, duration and
severity) and the QoL of the patients. Pearson correlation
coefficients determined whether the opinion of the patient
regarding their hair loss correlated with the DLQI (the correlation
between the indices). The indices prior to and following the
treatment were compared using the Student’s paired t-test.
Comparison of the improved value of each QoL index of the good
responders and poor responders from the baseline was performed
using the Student’s unpaired t-test. The data are presented as the
means ± SD.
Results
Correlation between clinical
characteristics and the QoL of first-visit patients
All patients were classified using the Ludwig
criteria. Analysis of the correlation between clinical
characteristics (age, duration and severity) and VAS and DLQI
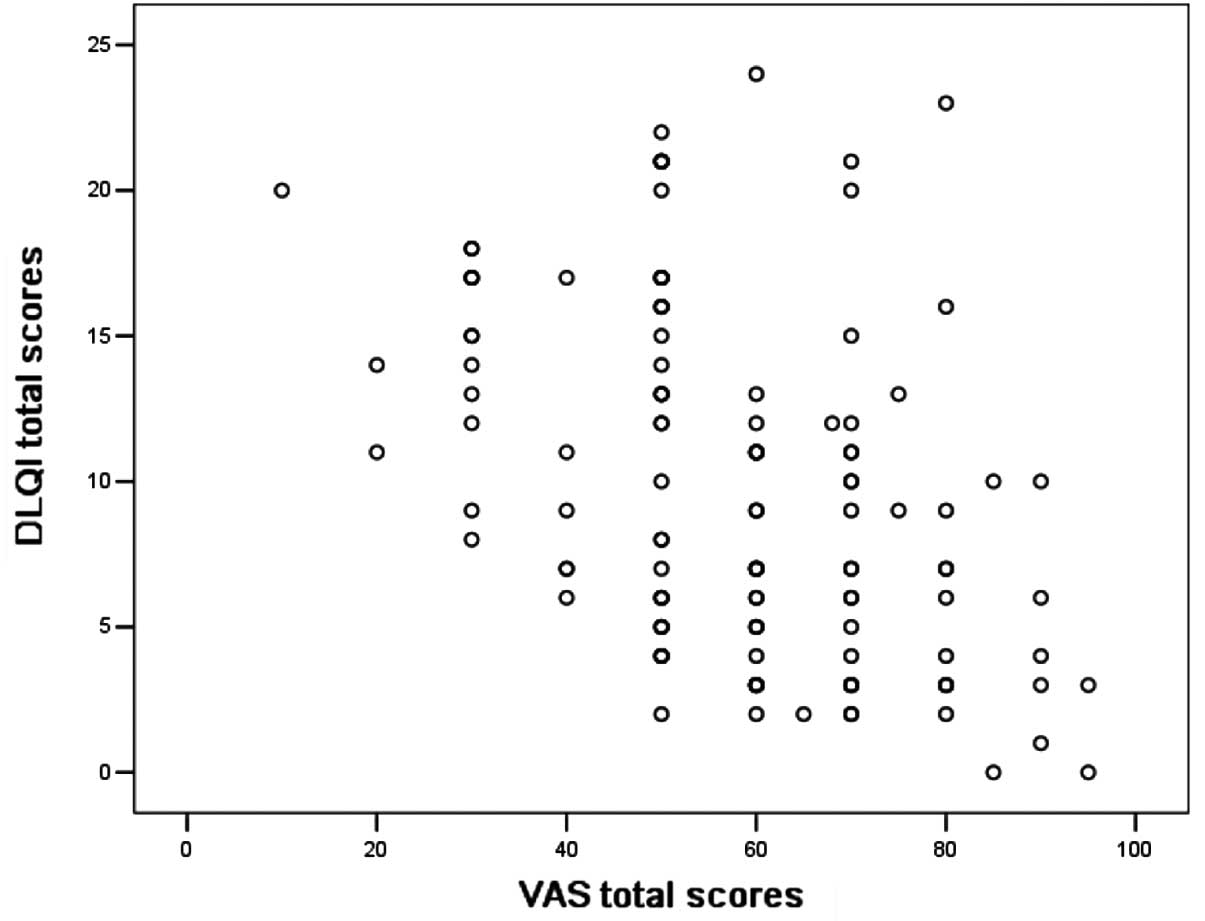
values was performed on the 125 first-visit patients. The scores
for the VAS and DLQI indices were 57.78±18.06 and 9.62±5.92,
respectively. There was no correlation between age, duration and
the two indices. However, the group with the greatest severity also
had the highest DLQI total score (P<0.05, Kruskal-Wallis Test)
and the lowest score on the VAS scale (P<0.05, Kruskal-Wallis
Test; Table III). The DLQI and VAS
scales correlated markedly with a statistically significant
negative correlation in all first-visit patients (P<0.000,
r=−0.441, Pearson correlation; Fig.
1).
| Table III.Correlation between single variables
and QoL. |
Table III.
Correlation between single variables
and QoL.
| Variable | DLQI | VAS |
|---|
| Age (years) | | |
| <30 | 10.300±5.873 | 55.870±19.462 |
| 30–50 | 9.590±5.996 | 56.480±18.722 |
| >50 | 9.250±4.979 | 56.250±10.607 |
| P-value | 0.797 | 0.946 |
| Disease duration
(months) | | |
| <12 | 10.520±5.999 | 59.130±16.832 |
| 12–24 | 9.480±6.583 | 55.000±17.705 |
| >24 | 9.860±5.842 | 56.390±18.652 |
| P-value | 0.672 | 0.764 |
| Severity (Ludwig
score) | | |
| I | 7.950±5.280 | 64.790±17.050 |
| II | 9.820±6.130 | 56.050±15.300 |
| III | 12.530±5.830 | 49.000±15.610 |
| P-value | <0.050 | <0.001 |
Comparison of DLQI and VAS scores prior
to and following the administration of topical minoxidil
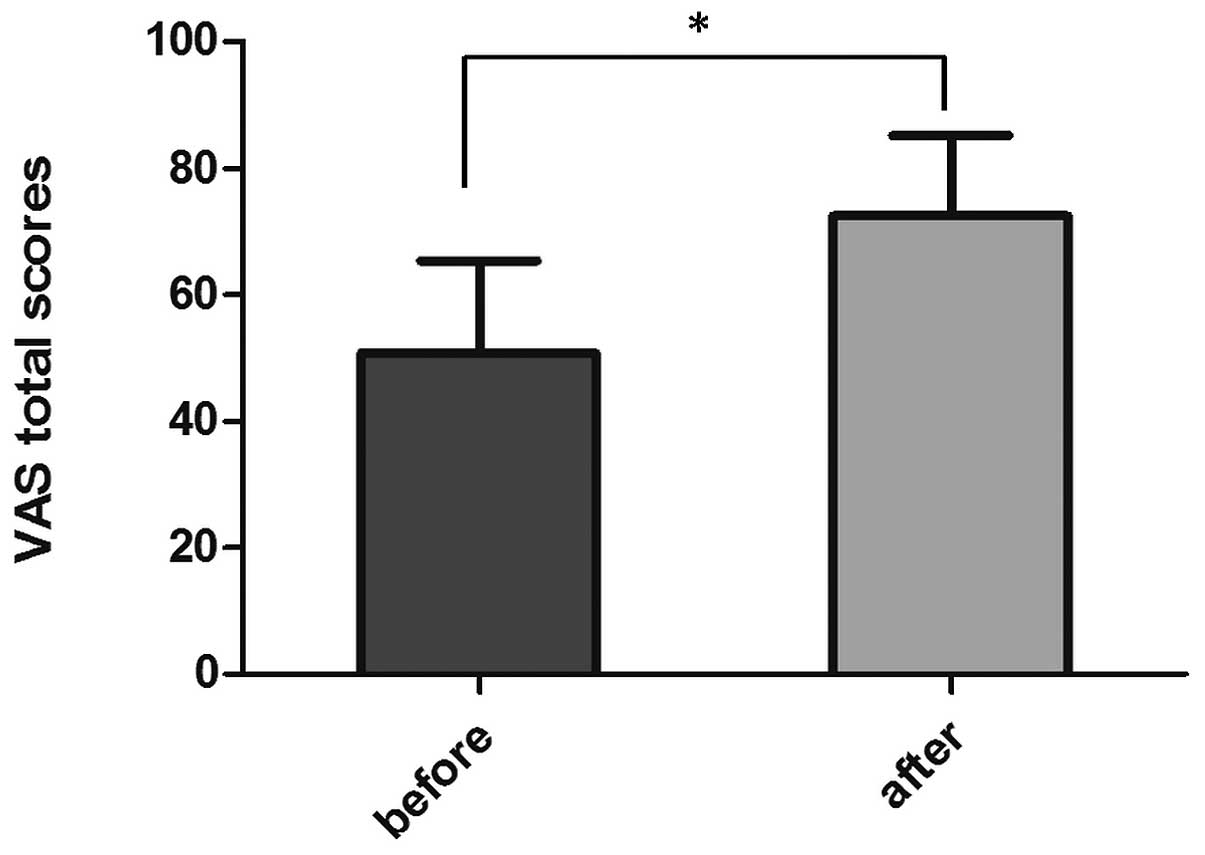
We analyzed the responses to the VAS and DLQI
questionnaires from 31 patients prior to and following treatment.
The scores for the VAS indices prior to and following the
administration of minoxidil were 50.81±14.61 and 72.52±12.79
(P<0.000, n=31, Student’s paired t-test), respectively (Fig. 2). The total scores for the DLQI
indices were 8.94±5.65 and 4.45±3.36, prior to and following
treatment, respectively. The difference between DLQI scores was
statistically significant (P<0.01, n=31; Student’s paired
t-test). With regard to specific life events, there were
significant differences in the scores for ‘symptoms and feelings’
(P<0.01, lane 1), ‘daily activities’ (P<0.01, lane 2) and
‘leisure’ (P<0.05, lane 3; Fig.
3).
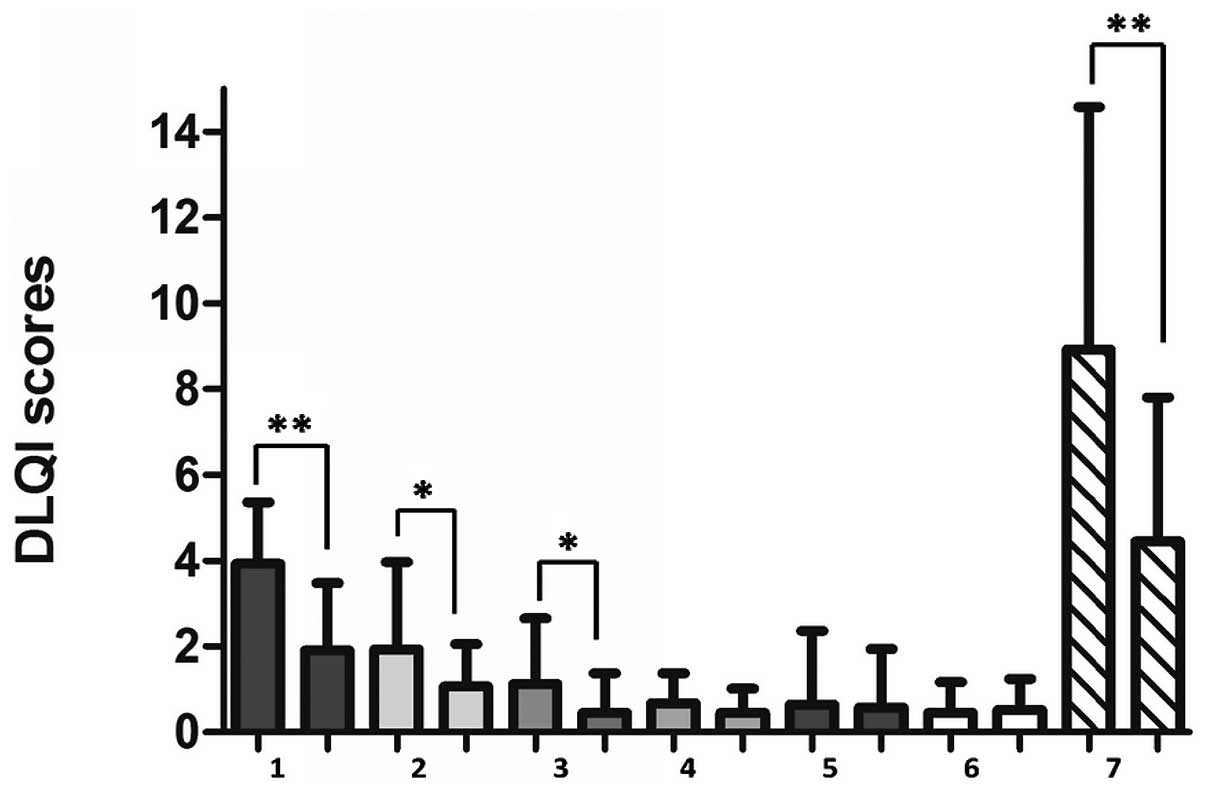 | Figure 3.Comparison of dermatology life quality
index (DLQI) scores prior to and following the administration of
topical minoxidil: 1, symptoms and feelings; 2, daily activities;
3, leisure; 4, work and school; 5, personal relationships; 6,
treatment and 7, total score. *P<0.05,
**P<0.01, n=31, Student’s paired t-test. Data
presented are the means ± SD. |
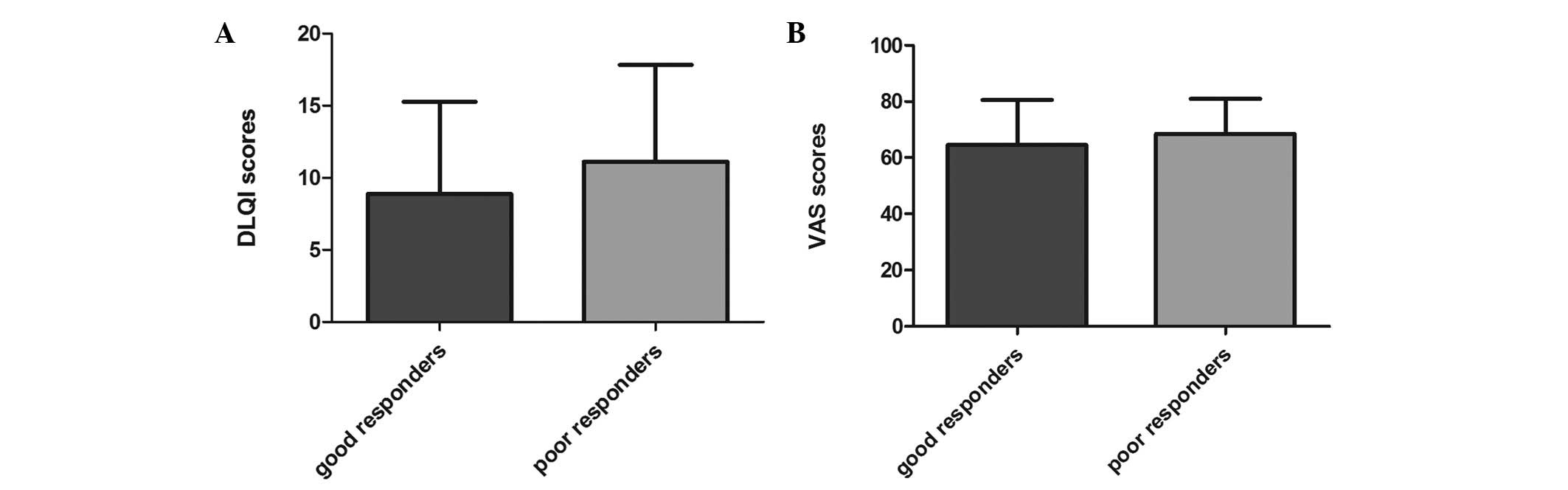
Comparison between good and poor
responders
The results of the evaluation performed by
clinicians were: ‘significant improvement’ in four cases;
‘improvement’ in 19 cases; ‘no change’ in five cases and
‘worsening’ in three cases. In total, 23 cases were assessed as
good responders and eight as poor responders. The improved values
for VAS from the baseline were 64.57±15.95 in the good responders
and 68.5±12.46 in the poor responders. The improved values for the
DLQI total scores from the baseline were 8.87±6.41 in the good
responders and 11.13±6.71 in the poor responders (Fig. 4). No significant differences were
observed between the scores of the good responders and poor
responders assessed by Student’s unpaired t-test.
Discussion
Multiple clinical trials have confirmed that topical
minoxidil ameliorates hair loss in FPHL patients. Our study
demonstrated that such treatment also improves the QoL of patients.
Yamazaki et al (12)
verified that DLQI and VAS are two highly reliable and sensitive
indices for assessing the improvement of QoL in male patients with
androgenic alopecia following oral finasteride treatment. We used
their study as a reference when conducting an assessment of the QoL
in female Chinese patients.
To explore the QoL of FPHL patients, we investigated
125 first-visit patients with a total DLQI score of 9.62±5.92,
which was close to 10 [>10 indicates a very severe impact
(17)]. This value is higher than
that in a previous study (12),
which reported a value of 5.74±6.14 in male patients; however, the
value is similar to the score for decubitus, while exceeding the
scores for atopic dermatitis and psoriasis (18). Collective evidence has suggested
that FPHL impairs the QoL of female patients to the same extent as
certain lifelong skin disorders such as psoriasis. Studies by Cash
et al (5) and van der Donk
et al (19) reported that
those seeking treatment for FPHL experienced social anxiety
disorder more severely, which is consistent with our observation
that FPHL has a greater impact on the QoL and psychology in female
patients than in male patients. Women are more likely to suffer
from mental illness as they pay more attention to their self-image
in society (12).
To identify the correlations between the clinical
characteristics of the patient and the severity of hair loss, we
classified all patients using the Ludwig criteria and observed that
there was a significant correlation between the clinical severity
and the VAS and DLQI indices while there were no correlations
between the other factors such as age and disease duration. The
more severe the clinical rating of hair loss, the greater the
impact on the DLQI and VAS scores. To a certain extent, these
results revealed that the clinical severity of hair loss may affect
the QoL of a patient. However a previous study (20) revealed that younger male patients
with a longer duration of hair loss had a reduced QoL, which
contradicts our results. This may be due to gender differences in
psychological needs and clinical features. Moreover, our finding
demonstrated that DLQI negatively correlated with VAS, implying
that the subjective rating for the severity of hair loss markedly
synchronized with the QoL in female patients. This suggests that
dermatologists should consider the subjective satisfaction and
objective rating in their estimation of clinical severity.
To further understand the impact of topical
minoxidil on the QoL of female patients, we compared the scores of
the VAS and DLQI indices prior to and following treatment. The VAS
scores were 50.81±14.61 and 72.52±12.79 prior to and following
treatment, respectively, while the total scores for the DLQI
indices were 8.94±5.65 and 4.45±3.36, respectively. A significant
difference in the evaluations demonstrated that topical minoxidil
may improve the QoL of female patients, particularly in areas of
their lives such as ‘symptoms and feelings’, ‘daily activities’ and
‘leisure’. In a previous study (21), women developed certain coping
mechanisms following the acceptance of hair loss, such as avoiding
negative emotions from their surroundings by reducing their outdoor
activities or by wearing hats or wigs to prevent discomfort.
Therefore it is unsurprising that effective clinical treatments are
able to improve the scores of corresponding items in the
questionnaire. No statistical difference in the scores for
‘treatment’ item of the questionnaire implied that the use of
topical minoxidil did not disturb the life of the patient, as it
was easy to use and did not clutter the patient’s home, which
should be mentioned in clinical use.
We classified the 31 patients into two groups
according to their response to the treatment. There were no
statistically significant differences between the DLQI and VAS
scores of the good responders and poor responders, revealing that
subjective satisfaction and QoL do not always correspond with
objective evaluation in female patients following treatment. This
is consistent with the results from the aforementioned study of
male patients (12). Subjective
satisfaction is considered to be determined by various
psychological factors and a potential variable is the motivation
for treatment. For instance, patients with an intrinsic reason (for
example, improvement of self-image) may experience greater
satisfaction than others with external requirements (wanting to
please others or to increase job opportunities) (22). The initial expectation of the
treatment is another factor, due to the fact that certain patients
may have expectations that go beyond medical limitations and are
therefore likely to lead to disappointment. Moreover, the length of
the treatment prior to any apparent improvement (increased terminal
hair count) may not necessarily result in cosmetic changes that
satisfy certain patients (23).
Overall, dermatologists should be alert to the
following potentially significant factors: sufficient time should
be spent on consultation and at the first visit, patients should
take a few minutes to complete a simple questionnaire regarding
their motivation and expectations of the treatment in order to
promote communication between the doctor and patient. Clinicians
should answer any questions the patient may have to ease their
concerns regarding hair loss and to correct any impractical
expectations, particularly regarding the improvement of hair
quantity and time taken for hair growth. DLQI and VAS are simple
and reliable surveys for understanding the patient’s feelings and
satisfaction prior to and following treatment. However, due to the
‘placebo effect’, certain patients may be satisfied with the
treatment even if they are poor responders, implying that
dermatologists should take the psychological requirement of the
patient into account throughout the therapeutic process.
In conclusion, evidence has suggested that patients
with hair loss experience a significantly impaired QoL, however,
few studies have focused on women with FPHL. Our findings observe
that a reduced QoL is a substantial part of the disease in patients
with FPHL and topical minoxidil solution may improve the QoL. The
current study presents instructive and meaningful information to
dermatologists and hair experts with regard to the benefits of
integrating the psychological factors of a patient into their
clinical treatment. However, further studies concerning the impact
of FPHL treatment on self-esteem, self-image and QoL are required
in the future.
References
|
1.
|
Gan DC and Sinclair RD: Prevalence of male
and female pattern hair loss in Maryborough. J Investig Dermatol
Symp Proc. 10:184–189. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Wang TL, Zhou C, Shen YW, et al:
Prevalence of androgenetic alopecia in China: a community-based
study in six cities. Br J Dermatol. 162:843–847. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Schmidt S, Fischer TW, Chren MM, Strauss
BM and Elsner P: Strategies of coping and quality of life in women
with alopecia. Br J Dermatol. 144:1038–1043. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Williamson D, Gonzalez M and Finlay AY:
The effect of hair loss on quality of life. J Eur Acad Dermatol
Venereol. 15:137–139. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Cash TF, Price VH and Savin RC:
Psychological effects of andro-genetic alopecia on women:
comparisons with balding men and with female control subjects. J Am
Acad Dermatol. 29:568–575. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Hunt N and McHale S: The psychological
impact of alopecia. BMJ. 331:951–953. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Van Neste DJ and Rushton DH: Hair problems
in women. Clin Dermatol. 15:113–125. 1997.
|
|
8.
|
Camacho FM and García-Hernández M:
Psychological features of androgenetic alopecia. J Eur Acad
Dermatol Venereol. 16:476–480. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Messenger AG and Rundegren J: Minoxidil:
mechanisms of action on hair growth. Br J Dermatol. 150:186–194.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Olsen EA, Weiner MS, Amara IA and DeLong
ER: Five-year follow-up of men with androgenetic alopecia treated
with topical minoxidil. J Am Acad Dermatol. 22:643–646.
1990.PubMed/NCBI
|
|
11.
|
Dinh QQ and Sinclair R: Female pattern
hair loss: current treatment concepts. Clin Interv Aging.
2:189–199. 2007.PubMed/NCBI
|
|
12.
|
Yamazaki M, Miyakura T, Uchiyama M, et al:
Oral finasteride improved the quality of life of androgenetic
alopecia patients. J Dermatol. 38:773–777. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Finlay AY and Khan GK: Dermatology life
quality index (DLQI)--a simple practical measure for routine
clinical use. Clin Exp Dermatol. 19:210–216. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Johnson EW: Visual analog scale (VAS). Am
J Phys Med Rehabil. 80:7172001. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Adamchic I, Langguth B, Hauptmann C and
Tass PA: Psychometric evaluation of visual analog scale for the
assessment of chronic tinnitus. Am J Audiol. 21:215–225. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Kondoh A, Ohta Y, Yamamoto K, et al:
Feasibility of modified DLQI-based questionnaires for evaluation of
clinical efficacy of herbal medicine in chronic skin diseases.
Tokai J Exp Clin Med. 30:97–102. 2005.PubMed/NCBI
|
|
17.
|
Katugampola RP, Hongbo Y and Finlay AY:
Clinical management decisions are related to the impact of
psoriasis on patient-rated quality of life. Br J Dermatol.
152:1256–1262. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Hahn HB, Melfi CA, Chuang TY, et al: Use
of the dermatology life quality index (DLQI) in a midwestern US
urban clinic. J Am Acad Dermatol. 45:44–48. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
van der Donk J, Passchier J, Knegt-Junk C,
et al: Psychological characteristics of women with androgenetic
alopecia: a controlled study. Br J Dermatol. 125:248–252.
1991.PubMed/NCBI
|
|
20.
|
Han SH, Byun JW, Lee WS, et al: Quality of
life assessment in male patients with androgenetic alopecia: result
of a prospective, multicenter study. Ann Dermatol. 24:311–318.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Cash TF: The psychology of hair loss and
its implications for patient care. Clin Dermatol. 19:161–166. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Resnik HL: Psychiatric observations on
patients who seek and undergo hair transplantation. J Dermatol Surg
Oncol. 6:1023–1025. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
O’Loughlin S: Topical minoxidil for male
pattern baldness. Ir Med J. 84:3–4. 1991.
|