Introduction
Acute fulminant myocarditis (AFM) is clinically and
pathologically defined as inflammation of the myocardium, leading
to the sudden onset of heart failure, arrhythmia, fulminant
hemodynamic collapse and sudden mortality (1,2). The
initial severe presentation and favorable long-term prognosis of
AFM is associated with left ventricular function (3). AFM involves serious arrhythmias,
which occasionally have lethal consequences due to cardiac
dysfunction (4).
Intravenous immunoglobulin (IVIG) has been used to
treat inflammatory and autoimmune diseases (5,6).
Immune or autoimmune mechanisms may be involved in the pathogenesis
of myocarditis (7). The
administration of immunoglobulin was reported to be of clinical
value against certain viral infections due to the neutralization of
the virus, the blockade of Fc receptors and the neutralization of a
microbial toxin (5,6,8,9).
Although the immunosuppressive therapy has yielded conflicting
results in patients with acute myocarditis (10), previous studies demonstrated the
effect of the IVIG in acute myocarditis (9,11).
The beneficial effect of IVIG on myocarditis was demonstrated in an
animal study using polyclonal immunoglobulin (11). In the pediatric population, IVIG
was associated with improved recovery of left ventricular function
(9). However, few studies have
specifically focused on IVIG for adult AFM. This retrospective
study was performed to evaluate the effect of IVIG on the cardiac
function and cardiac rhythm of adult patients with AFM.
Methods
Patients and study design
This was an observational retrospective case study
of inpatients who presented with AFM in Guangdong General Hospital
(Guangzhou, China) between January 2001 and December 2010. The
patients were included according to the following criteria: Adult
(age >18 years), acute-onset (duration <3 months) congestive
heart failure and impaired left ventricular function following a
recent viral illness. Patients with coronary artery disease,
long-standing dilated cardiomyopathy, structural heart disease,
systemic autoimmune disease, Kawasaki disease, the presence of
active infection and other specific causes of acute cardiomyopathy
were excluded. Data were collected through patient chart review.
This study was approved by the ethics committee for clinical
investigations of Guangdong General Hospital and informed consent
was obtained from the patient’s family.
Data collection
Clinical data and demographic information were
collected by the review of the medical records of the enrolled
patients. The patients were divided into IVIG therapy and non-IVIG
therapy (control) groups. Blood samples were obtained to analyze
myocardial enzymes, troponin, brain natriuretic peptide, C-reactive
protein and erythrocyte sedimentation rate at baseline.
Echocardiography, electrocardiography and 24-h ambulatory
electrocardiography were performed prior to and following
treatment. Gender, age, cardiac function classification, parameters
of echocardiography, blood test data and incidence of complications
were compared between the two groups.
Echocardiography
Echocardiography data were collected by previously
reported methods (12). Left
ventricular ejection fraction (LVEF), diameter of the left atrium
(LA), left ventricular end-diastolic diameter (LVDD), left
ventricular systolic diameter (LVDS), diameter of the right atrium
(RA) and diameter of the right ventricle (RV) were measured using
echocardiography. The data of left ventricle and left atrium were
measured on parasternal long-axis view, and the data of right
ventricle and right atrium were measured on apical four-chamber
view. The recovery of left ventricular function was assessed in
hospital and post-treatment (four weeks).
IVIG treatment regimens
IVIG (CSL Behring, Marburg, Germany) was
administered at a dose of 400 mg/kg per day for five days. Other
conventional therapies were administered as required, including
high-dose vitamin C, diuretics, digoxin, dopamine, dobutamine,
angiotensin-converting enzyme inhibitor/angiotensin receptor
blocker (ACEI/ARB), vasodilators (sodium nitroprusside,
nitroglycerin) and glucocorticoids. Intra-Aortic Balloon Pumps
(IABPs) were used to treat cardiogenic shock, while temporary
pacemakers were applied to third-degree atrioventricular block
(AVB).
Statistical analysis
The continuous variables that followed a symmetrical
distribution are presented as the mean ± standard deviation, with
the exception of Fig. 1. The
variables in Fig. 1 are presented
as the mean ± standard error. These continuous variables were
compared using the two independent samples Student’s t-test. Data
that followed an asymmetric distribution are presented as medians
and interquartile ranges, and were compared using the
Kruskal-Wallis nonparametric test. The categorical variables are
presented as frequencies and were analyzed using χ2 and
Fischer exact tests. P<0.05 was considered to indicate a
statistically significant difference. All statistical analyses were
performed with the Statistical Package for Social Sciences version
16.0 (SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristics
A total of 75 patients were initially eligible for
the study; however, 17 patients were excluded due to insufficient
clinical data. Fifty-eight patients were ultimately included. Of
these 58, 32 patients were treated with IVIG (400 mg/kg per day)
for five days, while the remaining patients did not receive IVIG
therapy. The IVIG and non-IVIG groups were similar with regard to
baseline characteristics, including gender, age, cardiac function
classification, parameters of echocardiography, blood test data and
incidence of complications (Table
I). The cardiac functions of the patients were classified as
NYHA classes II to IV. Ten patients (33%) of the IVIG group who had
NYHA class IV heart failure or cardiogenic shock received IABP
support, compared with three patients (16%) in the control group
(P=0.073). There were seven (27%) mortalities in the control group
and two (6%) in the IVIG group (P=0.072).
 | Table IInitial demographic and clinical
characteristics of 58 patients with AFM. |
Table I
Initial demographic and clinical
characteristics of 58 patients with AFM.
| Variable | IVIG group
(n=32) | Control group
(n=26) | P-value |
|---|
| Age (years)a | 30.6±14.1 | 30.0±16.6 | 0.905 |
| Maleb | 15/32 (47) | 13/26 (50) | 0.813 |
| NYHA
classificationb | | | 0.144 |
| Class I | 0/32 (0) | 0/26 (0) | |
| Class II | 8/32 (25) | 6/26 (23) | |
| Class III | 13/32 (41) | 11/26 (42) | |
| Class IV | 11/32 (34) | 9/26 (35) | |
|
Echocardiographya |
| Left ventricular
ejection fraction (%) | 45.3±15.2 | 43.5±19.6 | 0.703 |
| Diameter of left
atrium (mm) | 30.3±5.3 | 31.5±7.3 | 0.711 |
| Diameter of right
atrium (mm) | 43.0±8.7 | 46.1±9.0 | 0.211 |
| Left ventricular
diastolic diameter (mm) | 47.1±7.3 | 50.1±9.3 | 0.197 |
| Left ventricular
systolic diameter (mm) | 35.3±8.9 | 37.9±12.2 | 0.543 |
| Diameter of right
ventricle (mm) | 50.9±7.7 | 50.5±13.7 | 0.898 |
| Laboratory
testsa |
| A-hydroxybutyrate
dehydrogenase (U/l) | 959.2±1167.6 | 641.8±486.8 | 0.585 |
| Lactate
dehydrogenase (U/l) | 1707.7±3021.5 | 923.6±851.9 | 0.632 |
| Creatine kinase
(U/l) | 2228.3±5271.8 | 889.1±825.7 | 0.179 |
| Creatine kinase-MB
(U/l) | 40.4±56.2 | 28.8±23.9 | 0.454 |
| Troponin
(ng/ml) | 10.2±21.8 | 2.2±2.7 | 0.789 |
| Brain natriuretic
peptide (pg/ml) |
12746.8±13620.1 | 4690.6±8780.7 | 0.117 |
| C-reactive protein
(mg/l) | 46.5±51.2 | 34.9±31.7 | 0.480 |
| Erythrocyte
sedimentation rate (mm/h) | 20.0±16.5 | 19.7±18.8 | 0.969 |
|
Complicationsb |
| Pulmonary
edema | 13/32 (41) | 7/26 (27) | 0.428 |
| Cardiogenic
shock | 12/32 (38) | 4/26 (15) | 0.061 |
| Multiple Organ
Dysfunction Syndrome | 8/32 (25) | 2/26 (8) | 0.166 |
| Renal failure | 8/32 (25) | 1/26 (4) | 0.065 |
| Cardiac
arrest | 1/32 (3) | 2/26 (8) | 0.853 |
| Aspen
syndrome | 2/32 (6) | 4/26 (15) | 0.482 |
| Therapiesb |
| Vitamin C | 30/32 (94) | 23/26 (88) | 0.808 |
|
Glucocorticoid | 28/30 (93)c | 18/19 (95)c | 0.088 |
| Intra-aortic
balloon pumps | 10/30 (33)c | 3/19 (16)c | 0.073 |
| Pacemaker | 15/30 (50)c | 8/19 (42)c | 0.212 |
| Mortalityb | 2/32 (6) | 7/26 (27) | 0.072 |
Changes in left ventricular function
The patients of the two groups did not differ
significantly with regard to the echocardiographic data at the
baseline. The effect of IVIG treatment on LVEF (Fig. 1) and LVDD (Fig. 2) was investigated.
At the baseline, the LVEF of the two groups was
similar (IVIG versus control group: 45.3±15.2 versus 43.5±19.6%;
P=0.703). Four weeks subsequent to treatment, the mean LVEF in the
IVIG group was 62.2±10.2%, compared with 48.3±20.4% in the control
group. At four weeks post-treatment, the LVEF of the two groups had
improved significantly compared with the baseline values
(PIVIG<0.001, Pcontrol=0.027). The
patients treated with IVIG had a higher LVEF than those without
IVIG at four weeks (P=0.011).
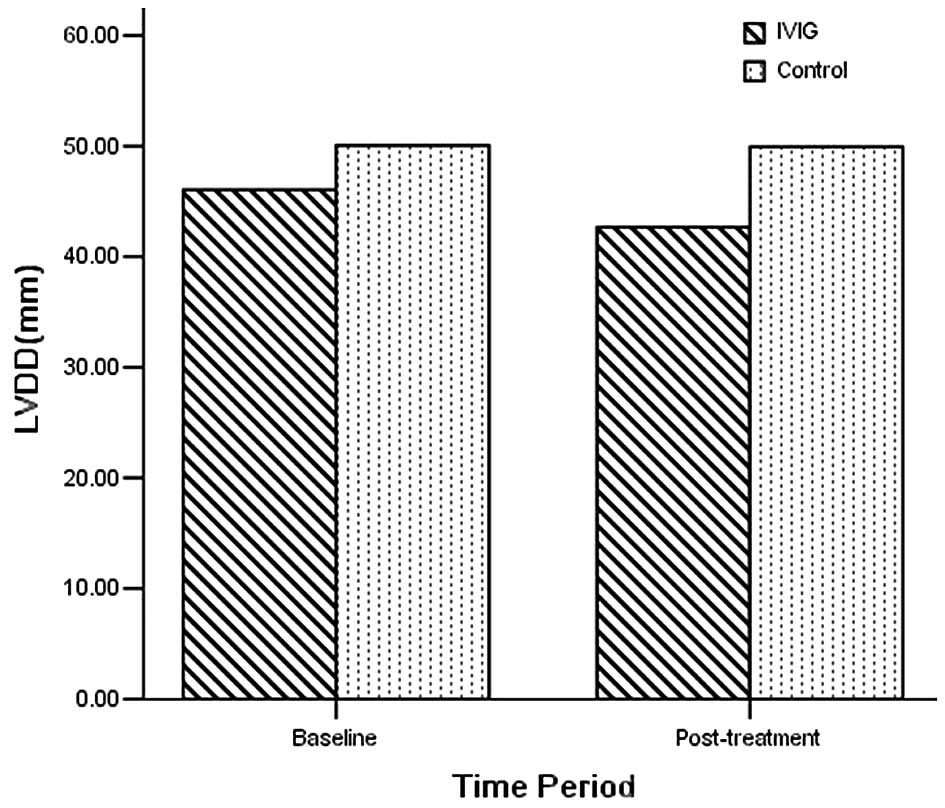
Four weeks subsequent to treatment, the LVDD of the
IVIG group (44.2±5.8 mm) was reduced compared with that of the
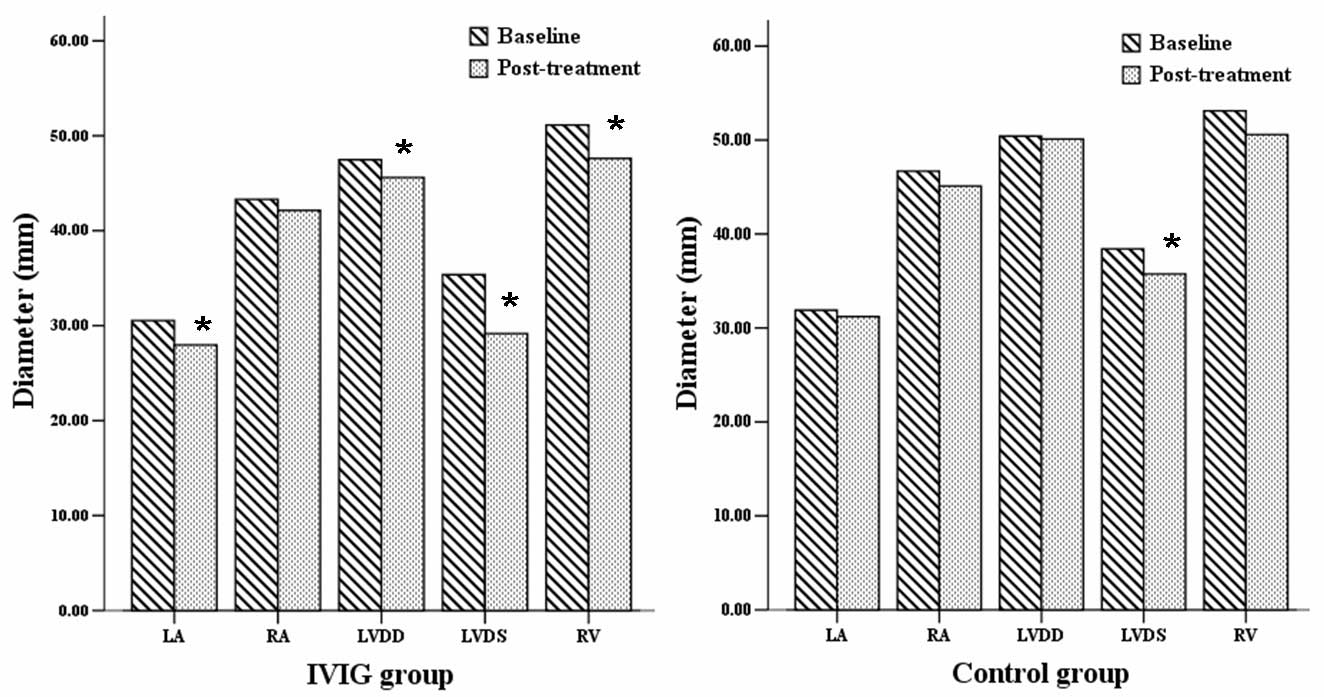
control group (49.6±10.3 mm; P=0.048; Fig. 2). Furthermore, the LA, LVDD, LVDS
and RV of the IVIG group showed recovery at four weeks
(PLA<0.001, PLVDD=0.006,
PLVDS<0.001, PRV=0.007), with the
exception of RA (P=0.232). However, only the LVDS of the control
group had improved at four weeks (PLVDS=0.012; Fig. 3).
Arrhythmia and changes in
echocardiography results
The patients exhibited several types of arrhythmia,
including bradycardia, AVB, atrial arrhythmia, ventricular
arrhythmia and bundle branch block. The changes in the ST segment
and T wave were also observed. Ventricular tachycardia/ventricular
fibrillation (VT/VF) occurred in 8 of the 32 (25.0%) patients in
the IVIG group and 3 of the 26 (11.5%) patients in the control
group at baseline. Seventeen of the 32 (53.1%) patients in the IVIG
group exhibited AVB at baseline compared with 8 of the 26 (30.8%)
patients in the control group. Following treatment, the episodes of
VT/VF and AVB were reduced in the IVIG group
(PVT/VF=0.025, PAVB=0.003); however, there
were no significant differences in the control group following
treatment (PVT/VF=0.564, PAVB=0.083).
Although the episodes of bradycardia, atrial arrhythmia, bundle
branch block and the change in the ST-T tended to decrease
post-treatment, the difference did not achieve statistical
significance in this small sample (Table II).
| Table IIIncidence of arrhythmia and the
change in ST-T in the IVIG and control groups pre- and
post-treatment. |
Table II
Incidence of arrhythmia and the
change in ST-T in the IVIG and control groups pre- and
post-treatment.
| IVIG group
(n=32) | Control group
(n=26) |
|---|
|
|
|
|---|
| Time-point | Bradycardia | AVB | VT/VF | Atrial
arrhythmia | Ventricular
arrhythmia | BBB | ST-T change | Bradycardia | AVB | VT/VF | Atrial
arrhythmia | Ventricular
arrhythmia | BBB | ST-T change |
|---|
| Baseline n (%) | 17 (53.1) | 17 (53.1) | 8 (25.0) | 6 (18.8) | 10 (31.3) | 17 (53.1) | 25 (78.1) | 11 (42.3) | 8 (30.8) | 3 (11.5) | 2 (7.7) | 6 (23.1) | 6 (23.1) | 15 (57.7) |
| Post-treatment n
(%) | 4 (12.5) | 3a (9.4) | 1a (3.1) | 1 (3.1) | 2 (6.3) | 6 (18.8) | 12 (37.5) | 3 (11.5) | 4 (15.4) | 3 (11.5) | 0 (0.0) | 3 (11.5) | 4 (15.4) | 7 (26.9) |
Discussion
Despite the therapeutic efficacy suggested by
previous studies (9,11), IVIG therapy for AFM has been rarely
reported. In this study, IVIG therapy improved the LVEF and reduced
the LVDD compared with the control group. Furthermore, compared
with the baseline values, the LA, LVDD, LVDS, RV and the episodes
of VT/VF and AVB were improved at the post-treatment time-point in
the IVIG group.
The damage to the myocardium in AFM may be mediated
by predominantly immunological mechanisms rather than by the direct
effect of viral infection and replication (13,14).
Previous studies have indicated the therapeutic effects of the IVIG
in acute myocarditis (11,15). Weller et al(11) observed that mouse polyclonal
immunoglobulin minimized myocardial damage in Balb/c male mice
infected intraperitoneally with coxsackievirus B3 when administered
24 or 48 h subsequent to infection (11). In another murine model of viral
myocarditis, IVIG administration reduced the extent of myocardial
necrosis or interstitial fibrosis and improved ventricular
remodeling (15). In addition,
certain clinical trials have indicated that IVIG may be beneficial
in acute myocarditis. Drucker et al(9) suggested that the use of high-dose
IVIG for the treatment of acute myocarditis was associated with the
improved recovery of left ventricular function and with a improved
survival rate during the first year following presentation
(9). In patients with new-onset
dilated cardiomyopathy treated with high-dose IVIG, LVEF improved
by 17 EF units (16). IVIG induced
a significant increase in LVEF from 26±2 to 31±3% in 40 patients
with symptomatic chronic congestive heart failure (CHF) and LVEF of
<40% (17). A favorable
clinical response was also observed in 10 case studies (18–27)
and two case series (28,29). However, according to a recent
systematic review (30), certain
studies (31,32) showed no benefit of IVIG. A
randomized controlled trial (RCT) suggested that IVIG did not
augment the improvement in LVEF for 62 patients with recent-onset
dilated cardiomyopathy. This RCT showed no benefit with respect to
cardiac function, functional outcome or event-free survival
(33).
Certain studies have suggested the mechanism
underlying the effect of high-dose IVIG in acute myocarditis
(17,34–36).
IVIG induced a marked rise in plasma levels of the
anti-inflammatory mediators interleukin (IL)-10, IL-1 receptor
antagonist and soluble tumor necrosis factor receptors.
Furthermore, levels of N-terminal pro-atrial natriuretic peptide
continued to decrease toward the end of the study during IVIG
therapy (17). IVIG decreased
cardiac inflammation and downregulated proinflammatory cytokines
that have direct negative inotropic effects (34–36).
IVIG decreases the incidence of VT/VF and AVB in AFM
in the present study. The combination of arrhythmias, including
VT/VF and AVB, and heart failure presents a serious challenge in
the management of AFM (1–4). The arrhythmias were resolved during
the convalescent and remote phases among the surviving patients,
and no atrial or ventricular arrhythmias were induced by the
programmed stimulation (4).
In conclusion, this study suggested that IVIG for
the treatment of AFM may be associated with improved recovery of
left ventricular function and a reduction in the episodes of
fulminant arrhythmias.
References
|
1
|
Magnani JW and Dec GW: Myocarditis:
current trends in diagnosis and treatment. Circulation.
113:876–890. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Feldman AM and McNamara D: Myocarditis. N
Engl J Med. 343:1388–1398. 2000. View Article : Google Scholar
|
|
3
|
Amabile N, Fraisse A, Bouvenot J, et al:
Outcome of acute fulminant myocarditis in children. Heart.
92:1269–1273. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ichikawa R, Sumitomo N, Komori A, et al:
The follow-up evaluation of electrocardiogram and arrhythmias in
children with fulminant myocarditis. Circ J. 75:932–938. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wolf HM and Eibl MM: Immunomodulatory
effect of immunoglobulins. Clin Exp Rheumatol. 14(Suppl 15):
S17–S25. 1996.
|
|
6
|
Rosen FS: Putative mechanisms of the
effect of intravenous gamma-globulin. Clin Immunol Immunopathol.
67:S41–S43. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kawai C: From myocarditis to
cardiomyopathy: mechanisms of inflammation and cell death: learning
from the past for the future. Circulation. 99:1091–1100. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yu Z and Lennon VA: Mechanism of
intravenous immune globulin therapy in antibody-mediated autoimmune
diseases. N Engl J Med. 340:227–228. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Drucker NA, Colan SD, Lewis AB, et al:
Gamma-globulin treatment of acute myocarditis in the pediatric
population. Circulation. 89:252–257. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mason JW, O’Connell JB, Herskowitz A, et
al: A clinical trial of immunosuppressive therapy for myocarditis.
The Myocarditis Treatment Trial Investigators. N Engl J Med.
333:269–275. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Weller AH, Hall M and Huber SA: Polyclonal
immunoglobulin therapy protects against cardiac damage in
experimental coxsackievirus-induced myocarditis. Eur Heart J.
13:115–119. 1992.
|
|
12
|
Newburger JW, Sanders SP, Burns JC, et al:
Left ventricular contractility and function in Kawasaki syndrome.
Effect of intravenous gamma-globulin. Circulation. 79:1237–1246.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
O’Connell JB, Robinson JA, Henkin RE and
Gunnar RM: Immunosuppressive therapy in patients with congestive
cardiomyopathy and myocardial uptake of gallium-67. Circulation.
64:780–786. 1981.PubMed/NCBI
|
|
14
|
Anderson JL, Fowles RE, Unverferth DV, et
al: Immunosuppressive therapy of myocardial inflammatory disease.
Initial experience and future trials to define indications for
therapy. Eur Heart J. 8(Suppl): 263–266. 1987. View Article : Google Scholar
|
|
15
|
Kishimoto C, Takamatsu N, Kawamata H, et
al: Immunoglobulin treatment ameliorates murine myocarditis
associated with reduction of neurohumoral activity and improvement
of extracellular matrix change. J Am Coll Cardiol. 36:1979–1984.
2000. View Article : Google Scholar
|
|
16
|
McNamara DM, Rosenblum WD, et al:
Intravenous immune globulin in the therapy of myocarditis and acute
cardiomyopathy. Circulation. 95:2476–2478. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gullestad L, Aass H, Fjeld JG, et al:
Immunomodulating therapy with intravenous immunoglobulin in
patients with chronic heart failure. Circulation. 103:220–225.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Takeda Y, Yasuda S, Miyazaki S, et al:
High-dose immunoglobulin G therapy for fulminant myocarditis. Jap
Circ J. 62:871–872. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nigro G, Bastianon V, Colloridi V, et al:
Human parvovirus B19 infection in infancy associated with acute and
chronic lymphocytic myocarditis and high cytokine levels: report of
3 cases and review. Clin Infect Dis. 31:65–69. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tsai YG, Ou TY, Wang CC, et al:
Intravenous gamma-globulin therapy in myocarditis complicated with
complete heart block: report of one case. Acta Paediatr Taiwan.
42:311–313. 2001.PubMed/NCBI
|
|
21
|
Shioji K, Matsuura Y, Iwase T, et al:
Successful immunoglobulin treatment for fulminant myocarditis and
serial analysis of serum thiredoxin: a case report. Circ J.
66:977–980. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tedeschi A, Airaghi L, Giannini S, et al:
High-dose intravenous immunoglobulin in the treatment of acute
myocarditis. A case report and review of the literature. J Intern
Med. 251:169–173. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Stouffer GA, Sheahan RG, Lenihan DJ, et
al: The current status of immune modulating therapy for
myocarditis: a case of acute parvovirus myocarditis treated with
intravenous immunoglobulin. Am J Med Sci. 326:369–374. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kim HS, Sohn S, Park JY and Seo JW:
Fulminant myocarditis successfully treated with high-dose
immunoglobulin. Int J Cardiol. 96:485–486. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Braun JP, Schneider M, Dohmen P and
Döpfmer U: Successful treatment of dilative cardiomyopathy in a
12-year-old girl using the calcium sensitizer levosimendan after
weaning from mechanical biventricular assist support. J
Cardiothorac Vasc Anest. 18:772–774. 2004.
|
|
26
|
Abe S, Okura Y, Hoyano M, et al: Plasma
concentrations of cytokines and neurohumoral factors in a case of
fulminant myocarditis successfully treated with intravenous
immunoglobulin and percutaneous cardiopulmonary support. Circ J.
68:1223–1226. 2004. View Article : Google Scholar
|
|
27
|
English RF, Janosly JE, Ettedgui JA and
Webber SA: Outcomes for children with acute myocarditis. Cardiol
Young. 14:488–493. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Karaaslan S, Oran B, Caliskan U, et al:
Hemolysis after administration of high-dose immunoglobulin in a
patient with myocarditis. Turk J Haematol. 20:237–240. 2003.
|
|
29
|
Khan MA, Das B, Lohe A and Sharma J:
Neonatal myocarditis presenting as an apparent life threatening
event. Clin Pediatr (Phila). 42:649–652. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Robinson JL, Hartling L, Crumley E, et al:
A systematic review of intravenous gamma globulin for therapy of
acute myocarditis. BMC Cardiovascular Disorders. 5:122005.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kishimoto C, Shioji K, Kinoshita M, et al:
Treatment of acute inflammatory cardiomyopathy with intravenous
immunoglobulin ameliorates left ventricular function associated
with suppression of inflammatory cytokines and decreased oxidative
stress. Intern J Cardiol. 91:173–178. 2003. View Article : Google Scholar
|
|
32
|
Wang CY, Li Lu F, Wu MH, et al: Fatal
coxsackievirus A16 infection. Pediatr Infect Dis J. 23:275–276.
2004. View Article : Google Scholar
|
|
33
|
McNamara DM, Holubkov R, Starling RC, et
al: Controlled trial of intravenous immune globulin in recent-onset
dilated cardiomyopathy. Circulation. 103:2254–2259. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Finkel MS, Oddis CV, Jacob TD, et al:
Negative inotropic effects of cytokines on the heart mediated by
nitric oxide. Science. 257:387–389. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Leung DY, Burns JC, Newburger JW and Geha
RS: Reversal of lymphocyte activation in vivo in Kawasaki syndrome
by intravenous gammaglobulin. J Clin Invest. 79:468–472. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hosenpud JD, Campbell SM and Mendelson DJ:
Interleukin-1-induced myocardial depression in an isolate beating
heart preparation. J Heart Transplant. 8:460–464. 1989.PubMed/NCBI
|