Introduction
The incidence of chronic kidney disease (CKD) is
>7% per year, and is increasing annually. According to the
latest data from the International Society of Nephrology (ISN),
>500 million individuals worldwide suffer from various kidney
diseases, and CKD, complicated by cardiovascular and
cerebrovascular diseases, is the cause of mortality for >1
million individuals every year. CKD has become a serious threat to
human health, following cardiovascular and cerebrovascular disease,
cancer and diabetes. Patients with CKD are treated using lifelong
dialysis or renal transplantation, putting a huge economic burden
on families, medical institutions and society. Renal fibrosis is a
pathophysiological process, in which the kidney function is
gradually damaged. Further damage ultimately leads to a loss of
function. The early treatment of renal fibrosis may delay or even
reverse the fibrotic lesions; thus, the early diagnosis of renal
fibrosis is necessary. The diagnosis of mild renal fibrosis is
difficult, and biopsy remains the clear gold diagnostic standard.
Acoustic radiation force impulse imaging (ARFI) is a novel
technology that has been used in the differential diagnosis of
liver fibrosis, and breast and thyroid benign and malignant tumors.
The value of ARFI has been widely recognized, particularly for the
diagnosis of liver fibrosis (1–4).
However, its significance in the diagnosis of renal fibrosis has
yet to be elucidated. The aim of the present study was to
investigate the assessment value of virtual touch quantization
(VTQ) in the pathological typing of renal fibrosis.
Patients and methods
Subjects
In total, 76 patients [43 males and 33 females; age,
11–75 years (40.37±16.13 years)], who were admitted for CKD to the
Department of Nephrology Medicine, The Affiliated Hospital of
Binzhou Medical College (Binzhou, China) between June 2010 and June
2012, were recruited and enrolled in this study. The extent of
renal fibrosis of each patient was verified using ultrasound-guided
renal biopsy pathology. This study was conducted in accordance with
the Declaration of Helsinki and with approval from the Ethics
Committee of Binzhou Medical College (Binzhou, China). Written
informed consent was obtained from all participants.
Methods
Experiments were performed using a Siemens Acuson
S2000™ color Doppler ultrasound system (Siemens Medical Solutions
USA, Inc., Detroit, MI, USA), equipped with ARFI technology
software and a 4C1 probe with frequencies ranging between 2.0 and
5.0 MHz and a function of VTQ determination. The patient was asked
to lie in prone position and was initially examined using
conventional two-dimensional ultrasound, with a longitudinal
section scanning of the right kidney. The sound beam was maintained
as perpendicular as possible to the kidney capsule. Subsequently
the patient was asked to hold their breath, and the VTQ sampling
box was placed in the right renal subcapsular parenchyma as the
image stabilized in the VTQ mode. Each position of each patient was
assessed five times and the average VTQ value was recorded.
Puncture biopsy
Puncture biopsy of the right inferior pole of the
kidney parenchyma was performed using an 18G transfixion pin of a
Bard automatic biopsy device (Bard Peripheral Vascular Inc., Tempe,
AZ, USA) under ultrasonic guidance. A 2.2-cm kidney tissue biopsy
was obtained and subsequently fixed in 10% formalin, prior to being
sent for pathological examination. The patients were divided into
four groups according to the extent of their kidney fibrosis, as
follows: non-fibrosis, mild fibrosis (fibrosis extent, ≤25%),
moderate fibrosis (fibrosis extent, 26–50%) and severe fibrosis
(fibrosis extent, >50%).
Statistical analysis
The SPSS software program version 16.0 (SPPS Inc.,
Chicago, IL, USA) was used for statistical analyses. Results are
presented as the mean ± standard deviation. The differences between
the groups were compared using an independent sample t-test.
P<0.05 was considered to indicate a statistically significant
difference.
Results
The kidney tissue biopsies sent for pathological
examination were classified into four groups according to the
extent of fibrosis, as follows: non-fibrosis (n=14), mild fibrosis
(n=40), moderate fibrosis (n=21) and severe fibrosis (n=1). The
corresponding VTQ values were 1.59±0.14, 2.15±0.38, 2.29±0.53 and
2.24 m/sec, respectively (Table
I). As there was only one patient in the severe fibrosis group,
this group was excluded from statistical analysis. Pairwise
comparisons of the non-fibrosis group with the mild and moderate
fibrosis groups demonstrated that the VTQ values were significantly
increased in the mild and moderate fibrosis groups (P<0.01).
However, there was no significant difference between the mild and
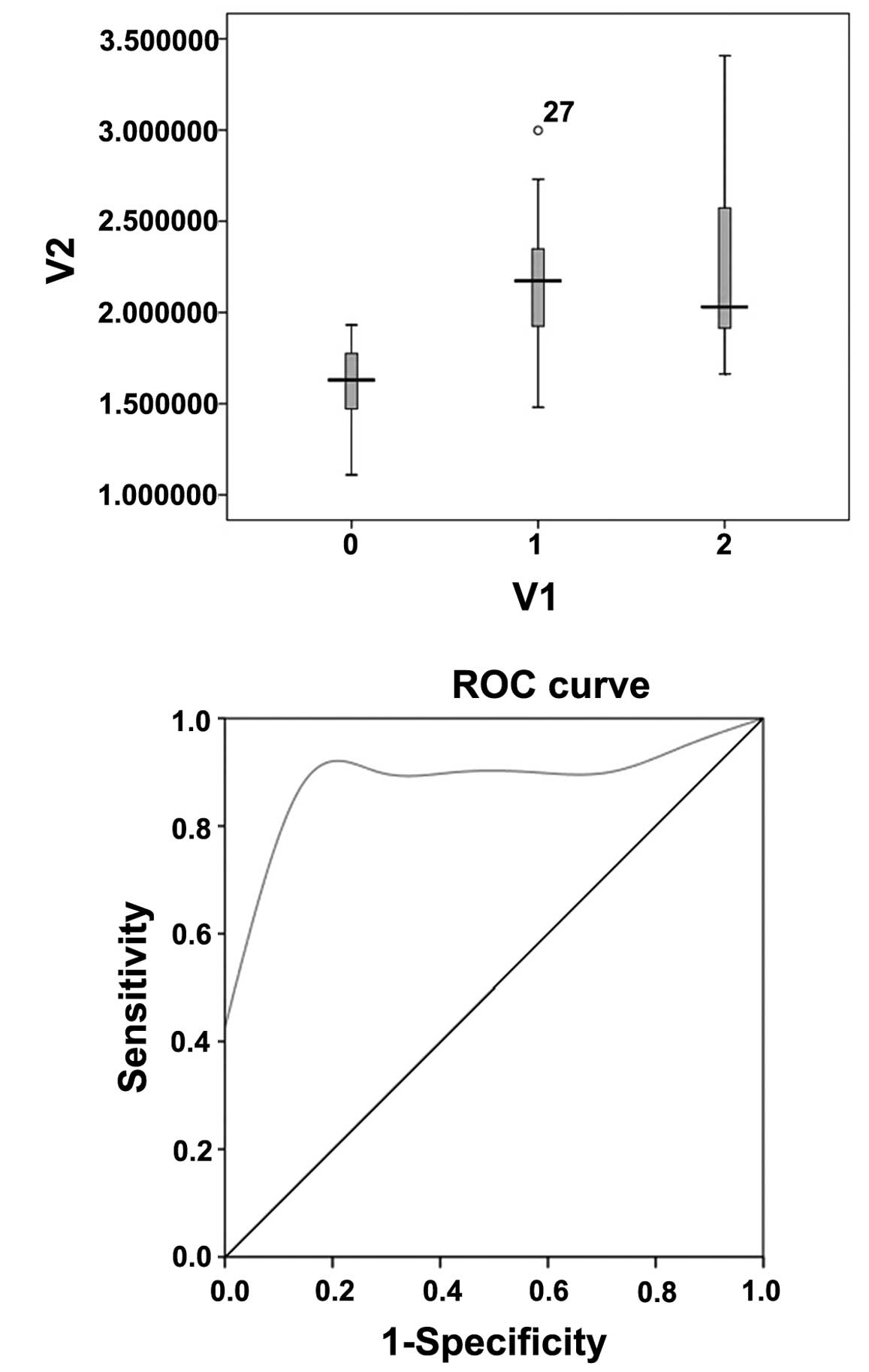
moderate fibrosis groups (P>0.05). The distribution of the VTQ
values of renal parenchyma in the non-fibrosis, mild fibrosis and
moderate fibrosis groups are shown in Fig. 1A. Furthermore, a receiver operating
characteristic (ROC) curve was created using the VTQ values of the
non-fibrosis and mild fibrosis groups. It was demonstrated that an
elevated VTQ value has a certain discriminant value in the
diagnosis of renal fibrosis (P<0.01, Fig. 1B). A measured VTQ value of renal
parenchyma >1.67 m/sec was deemed to be a diagnostic indicator
for renal fibrosis. The diagnostic sensitivity and specificity of
the VTQ value were 86.3 and 83.3%, respectively.
 | Table ICase numbers and VTQ values of the
four groups. |
Table I
Case numbers and VTQ values of the
four groups.
| Groups | Case number | VTQ value |
|---|
| Non-fibrosis | 14 | 1.59±0.14 |
| Mild fibrosis | 40 | 2.15±0.38a |
| Moderate
fibrosis | 21 | 2.29±0.53a |
| Severe fibrosis | 1 | 2.24 |
Discussion
The common pathway for the development of CKD, such
as primary and secondary glomerular diseases, tubular, interstitial
and vascular diseases, and renal transplant chronic rejection
disease, to terminal nephropathy is kidney fibrosis. The main
pathological change is the absence of normal renal units,
which are replaced by a large quantity of fibroblasts and
myofibroblasts. The generation and accumulation of extracellular
matrix, including collagen fibers and fibronectin, causes
glomerulosclerosis and tubulointerstitial fibrosis and ultimately
leads to the loss of kidney function (5,6). The
pathological change in renal fibrosis is a gradual evolutive
process from light to severe. It may be inhibited or delayed by
early medication, but in severe instances it is irreversible.
Therefore, the early diagnosis of renal fibrosis is likely to be
beneficial for the treatment of the disease (7). At present, the clinical diagnosis of
renal fibrosis is dependent on renal biopsy. However, a needle
biopsy is an invasive diagnostic method with a degree of risk
involved. Thus, a new, non-invasive and repeatable diagnostic
method is required.
Flexibility is an important physical property of
biological tissues. The flexibility is not only different among
various tissue types, but also in the pathological states of the
same tissue. As a result of this, ultrasound elasticity imaging
techniques have emerged. Ophir et al(8) first proposed the concept of
elastography in 1991. Following 20 years of research and
development, ultrasound elasticity imaging technology has been
widely used in the differential diagnosis of benign and malignant
superficial organs, such as the breast and thyroid (9–12).
It has also been used in the diagnosis of liver fibrosis and
cirrhosis (1–4) and in the study of various
pathological types of advanced gastric cancer (13). Based on ultrasound elastography,
ARFI is an established imaging technology, which includes virtual
touch tissue imaging (VTI) and VTQ. VTQ is an ultrasound imaging
technology for the quantitative assessment of tissue elasticity. It
only produces target displacement in the region of interest, but no
overall displacement, which makes up the qualitative deficiency of
the past ultrasound elasticity imaging technology. VTQ is an
absolute quantitative indicator that is capable of supporting
tissue image contrast between patients. The ARFI technique has been
shown to be capable of measuring the quantitative flexibility of
abdominal organs, including the liver, kidney and stomach (13–16).
A recent investigation demonstrated the application of ARFI for the
study of pancreatic cystic lesions (17).
VTQ technology for the diagnosis of renal fibrosis
has been rarely reported and remains controversial, due to the
current lack of a unified quantitative standard. Stock et
al(18) hypothesized that
renal parenchymal was likely to harden as a result of fibrosis and
that the elasticity was likely to decrease when lesions occurred in
the kidney. In addition, it was hypothesized that the VTQ value or
the Young’s modulus of the renal cortex were likely to have a
corresponding change that was potentially meaningful for the early
diagnosis of renal fibrosis. However, Syversveen et
al(19,20) reported that VTQ was not able to
significantly distinguish mild fibrosis from non-fibrosis in a
transplanted kidney. Furthermore, there are great differences in
the VTQ values of different examiners.
In this study, 76 patients with fibrosis, in whom
the extent of the fibrosis had been confirmed using renal puncture
biopsy, were analyzed using VTQ. It was observed that the VTQ
values of patients with mild renal fibrosis were significantly
higher than those of the non-fibrosis group (P<0.01). However,
the VTQ values of patients with mild renal fibrosis showed no
significant difference from the patients with moderate renal
fibrosis. The severe fibrosis group was excluded as there was only
one patient classified as having severe fibrosis, which was
insufficient for a statistical analysis. According to the maximum
area under the ROC curve, a VTQ value of >1.67 m/sec was
determined as a diagnostic indicator of mild fibrosis of the renal
cortex with a sensitivity of 86.3% and a specificity of 83.3%. The
VTQ technique provides a novel reference for the clinical diagnosis
of renal fibrosis. This is consistent with our assumption and
results of the study of Stock et al(18). However, there are certain
limitations in this study, the VTQ technique is not capable of
accurately differentiating between light and moderate renal
fibrisis. This may be due to the fact that there are large numbers
of cross-data between light and moderate renal fibrosis.
Furthermore, the classification in the present study was not
entirely based on the differences between light and moderate renal
fibrosis. The VTQ value measured in the non-fibrosis nephropathy
group demonstrated a certain degree of overlap with that of the
mild fibrosis group and the moderate fibrosis group. As the sample
sizes in this study were small, particularly for the severe renal
fibrosis group, further studies with a larger sample size and more
data are required in order to confirm the findings of this
study.
References
|
1
|
Rifai K, Cornberg J, Mederacke I, et al:
Clinical feasibility of liver elastography by acoustic radiation
force impulse imaging (ARFI). Dig Liver Dis. 43:491–497. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fierbinteanu-Braticevici C, Andronescu D,
Usvat R, et al: Acoustic radiation force imaging sonoelastography
for noninvasive staging of liver fibrosis. World J Gastroenterol.
15:5525–5532. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Toshima T, Shirabe K, Takeish K, et al:
New method for assessing liver fibrosis based on acoustic radiation
force impulse: a special reference to the difference between right
and left liver. J Gastroenterol. 46:705–711. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Takahashi H, Ono N, Eguchi Y, et al:
Evaluation of acoustic radiation force impulse elastography for
fibrosis staging of chronic liver disease: a pilot study. Liver
Int. 30:538–545. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Iwano M and Neilson EG: Mechanisms of
tubulointerstitial fibrosis. Curr Opin Nephrol Hypertens.
13:279–284. 2004. View Article : Google Scholar
|
|
6
|
Liu Y: Epithelial to mesenchymal
transition in renal fibrogenesis: pathologic significance,
molecular mechanism, and therapeutic intervention. J Am Soc
Nephrol. 15:1–12. 2004. View Article : Google Scholar
|
|
7
|
Eddy AA: Molecular basis of renal
fibrosis. Pediatr Nephrol. 15:290–301. 2000. View Article : Google Scholar
|
|
8
|
Ophir J, Céspedes EI, Ponnekenti H, Yazdi
Y and Li X: Elastography: a quantitative method for imaging the
elasticity of biological tissues. Ultrason Imaging. 13:111–134.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Scacchi M, Andrioli M, Carzaniga C, et al:
Elastosonographic evaluation of thyroid nodules in acromegaly. Eur
J Endocrinol. 161:607–613. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Friendich-Rust M, Romenski O, Meyer G, et
al: Acoustic radiation force impulse-imaging for the evaluation of
the thyroid gland: a limited patient feasibility study.
Ultrasonics. 52:69–74. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tozaki M, Isobe S and Fukuma E:
Preliminary study of ultrasonographic tissue quantification of the
breast using the acoustic radiation force impulse (ARFI)
technology. Eur J Radiol. 80:182–187. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Meng W, Zhang G, Wu C, Wu G, Song Y and Lu
Z: Preliminary results of acoustic radiation force impulse (ARFI)
utrasound imaging of breast lesions. Ultrasound Med Biol.
37:1436–1443. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Palmeri ML, Frinkley KD, Zhai L, et al:
Acoustic radiation force impulse (ARFI) imaging of the
gastrointestinal tract. Ultrason Imaging. 27:75–88. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhai L, Madden J, Foo WC, et al: Acoustic
radiation force impulse imaging of human prostates ex vivo.
Ultrasound Med Biol. 36:576–588. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Boursier J, Isselin G, Fouchard-Hubert I,
et al: Acoustic radiation force impulse: a new ultrasonographic
technology for the widespread noninvasive diagnosis of liver
fibrosis. Eur J Gastroenterol Hepatol. 22:1074–1084. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yoneda M, Suzuki K, Kato S, et al:
Nonalcoholic fatty liver disease: US-based acoustic radiation force
impulse elastography. Radiology. 256:640–647. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
D’Onofrio M, Gallotti A, Salvia R, et al:
Acoustic radiation force impulse (ARFI) ultrasound imaging of
pancreatic cystic lesions. Eur J Radiol. 80:241–244.
2011.PubMed/NCBI
|
|
18
|
Stock KF, Klein BS, Vo Cong MT, et al:
ARFI-based tissue elasticity quantification in comparison to
histology for the diagnosis of renal transplant fibrosis. Clin
Hemorheol Microcirc. 46:139–148. 2010.PubMed/NCBI
|
|
19
|
Syversveen T, Brabrand K, Midtvedt K, et
al: Assessment of renal allograft fibrosis by acoustic radiation
force impulse quantification - a pilot study. Transpl Int.
24:100–105. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Syversveen T, Midtvedt K, Berstad AE,
Brabrand K, Strøm EH and Abildgaard A: Tissue elasticity estimated
by acoustic radiation force impulse quantification depends on the
applied transducer force: an experimental study in kidney
transplant patients. Eur Radiol. 22:2130–2137. 2012. View Article : Google Scholar
|