Introduction
Chronic kidney disease (CKD) is a risk factor for
end-stage renal disease (ESRD). Early detection and timely
management are essential for the medical care of patients with CKD.
In clinical practice, information derived from kidney biopsies is
commonly considered a ‘gold’ standard that establishes the
histopathological patterns concerning renal injury. However,
biopsies are invasive and may result in various complications,
including gross hematuria, and major complications that may
eventually result in renal failure (1). Thus, certain disorders, including
coagulopathy, are contraindicated for biopsy. Alternatively,
Doppler sonography is a noninvasive method of examination that is
widely used for the evaluation of patients with CKD.
Morphological changes associated with renal
dysfunction, including the size, parenchymal echogenicity and
corticomedullary differentiation of the injured kidneys, may be
shown by sonography. However, these parameters lack specificity in
the assessment of renal failure (2). Furthermore, it has been reported that
the morphological changes detectable by sonography appear much
later than the biochemical indicators, including increased serum
creatinine levels (3).
An increased resistive index (RI) has been reported
to correlate with glomerulosclerosis (GS), tubulointerstitial
damage (TI) and vascular lesions (4). However, the results are not
consistent (5). More notably, a
previous study regarding renal histology has investigated small
populations, and correlation analysis between reduced Doppler
velocity in the interlobar arteries and histopathological changes
in the impaired kidney is lacking (6).
The present study aimed to evaluate the correlations
of a number of Doppler parameters, not only the RI but also the
peak systolic velocity (PSV) and end-diastolic velocity (EDV), with
histopathological changes in order to determine their significances
in clinical decision-making concerning the care of patients with
CKD.
Materials and methods
Patient information
A retrospective study was conducted and the medical
records of 992 consecutive patients with CKD who underwent
treatment between January 2006 and December 2010 at the Departments
of Nephrology at the First Affiliated Hospital of Nanchang
University (Nanchang, China), the General Hospital of Guangzhou
Military Command of PLA (Guangzhou, China) and the First People’s
Hospital of Jiujiang City (Jiujiang, China) were reviewed. The CKD
diagnostic criteria used in this study fulfilled the guidelines
proposed by the Kidney Disease Outcomes Quality Initiative of the
National Kidney Foundation (7),
and the classifications were made as follows: Stage 1, estimated
glomerular filtration rate (eGFR, ml/min/1.73 m2)
>90; stage 2, eGFR = 60–89; stage 3, eGFR = 30–59; stage 4, eGFR
= 15–29; and stage 5, eGFR <15 or dialysis. For each patient,
the age, gender, blood pressure, urinary protein, serum creatinine
levels and eGFR at the renal biopsy were recorded. The study was
conducted in accordance with the Declaration of Helsinki and
approved by the Research Ethics Committee of the First Affiliated
Hospital of Nanchang University, the General Hospital of Guangzhou
Military Command of PLA and the First People’s Hospital of Jiujiang
City. Prior to this study, informed consent was obtained from all
patients.
Doppler ultrasonography
Ultrasound evaluation was performed 24 h prior to
the renal biopsy for all patients. In the maximum long-axis section
images, the largest diameter and width of each kidney were
measured. The patients were scanned in a supine or decubitus
position to achieve an ultrasound beam as close to parallel to the
blood flow direction in the intrarenal artery as possible. An
ultrasound probe covered with transmission gel was gently placed on
the skin over the kidneys. The PSV, EDV and RI were routinely
measured as previously reported (8).
Histological evaluation
The renal biopsy samples were evaluated for the
severity of GS and TI damage based on previous scoring systems
(9). Briefly, the GS score for
each patient was evaluated in periodic acid-Schiff-stained sections
and defined as follows: 0, normal GS; 1, matrix expansion or GS
<25%; 2, GS = 26–50%; 3, GS = 51–75%; and 4, GS >75%. The TI
score was assessed in azan- or periodic acid-methenamine
silver-stained sections and defined as follows: 0, normal; 1, mild
fibrosis around the vasculature; 2, mild fibrosis around the
tubules; 3, moderate fibrosis with tubular casts or tubular damage;
and 4, severe fibrosis with cell infiltration. The average score of
the entire area of the biopsy sample of each patient was calculated
for each histological component.
Statistical analysis
All Doppler parameters were expressed as the mean ±
standard deviation. SPSS software, version 16.0 (SPSS, Inc.,
Chicago, IL, USA) was used for statistical analysis. Student’s
t-test was used to statistically analyze differences in the PSV,
EDV and RI values in the main renal artery and interlobar artery
between two groups. The correlations of the clinical and
histological factors with the ultrasonographic indices were
evaluated by stepwise multivariate regression analysis. P<0.05
was considered to indicate a statistically significant
difference.
Results
Clinical characteristics of the
patients
A total of 992 patients were diagnosed with CKD by
renal biopsy, including 92 patients with IgA nephropathy, 109 with
focal segmental GS, 103 with membranous nephropathy, 98 with
minimal change disease, 149 with diabetic nephrosclerosis, 68 with
crescentic glomerulonephritis, 32 with hypertensive
nephrosclerosis, 134 with lupus nephritis, 114 with interstitial
nephritis, 21 with amyloidosis, 17 with hereditary nephritis, 18
with hematopoietic stem cell transplantation-related nephropathy,
nine with acute postinfectious glomerulonephritis and 28 with
membranoproliferative glomerulonephritis.
The 992 patients underwent a renal biopsy and
sonography. The baseline characteristics are shown in Table I. There were 112 patients with CKD
stage 1, 278 with stage 2, 334 with stage 3, 198 with stage 4 and
70 with stage 5.
 | Table IBaseline characteristics of the
participants (n=992). |
Table I
Baseline characteristics of the
participants (n=992).
| Variable | Value |
|---|
| Demographic |
| Age (years; mean ±
SD) | 63±11 |
| Male/female (n) | 605/387 |
| Body mass index
(kg/m2) | 24.41±3.52 |
| Comorbidities |
| Hypertension [n
(%)] | 641 (64.6) |
| Systolic BP (mmHg;
mean ± SD) | 134.6±33.7 |
| Diastolic BP, (mmHg;
mean ± SD) | 84.7±23.2 |
| Diabetes mellitus [n
(%)] | 293 (29.5) |
| Cardiovascular
disease [n (%)] | 281 (28.3) |
| Laboratory |
| Hemoglobin (g/l;
mean ± SD) | 97.5±23.5 |
| Serum creatinine
(μmol/l; mean ± SD) | 221.4±62.6 |
| eGFR (ml/min/1.73
m2; mean ± SD) | 21.2±5.9 |
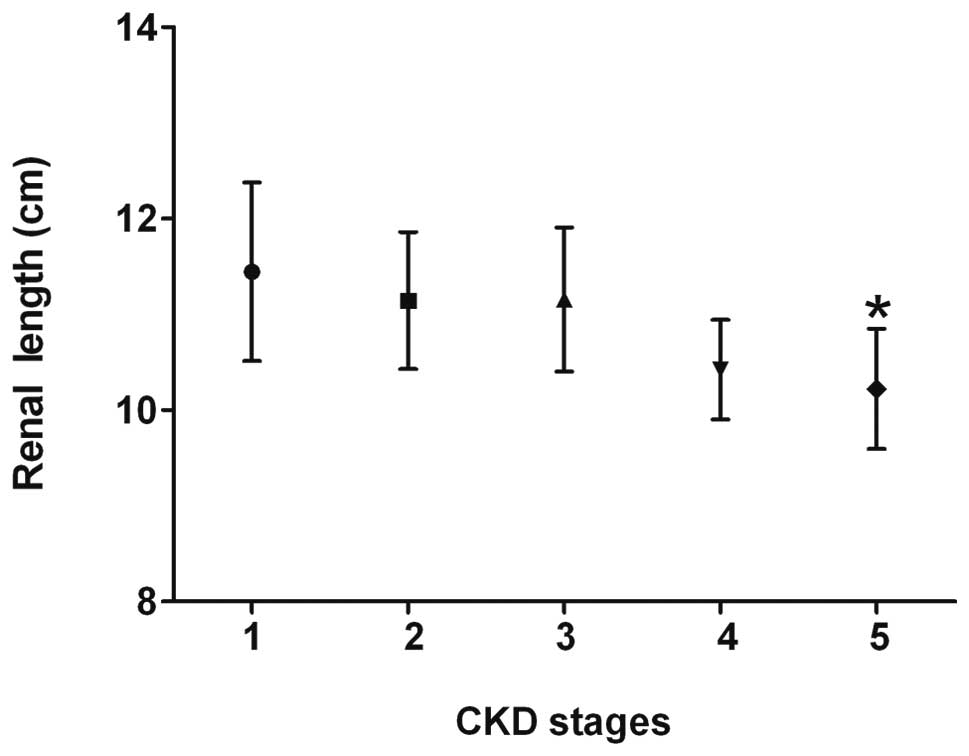
Correlation of renal length with the CKD
stage
The size of the kidneys was significantly reduced in
the patients with stage 5 CKD, compared with that of the patients
with stages 1, 2 or 3 CKD (Fig.
1). However, in the patients with stages 1–3 CKD, no
significant association between the renal length and disease
progression was identified, and the renal length showed a
statistical but weak correlation with the renal function and
histological damage scores (Table
II).
| Table IICorrelation coefficients (r) of the
ultrasonographic parameters with the clinical and histological
parameters (n=992). |
Table II
Correlation coefficients (r) of the
ultrasonographic parameters with the clinical and histological
parameters (n=992).
| Renal parameters | Renal length | RI | PSV | EDV |
|---|
| Serum creatinine
levels | −0.11 | 0.10 | 0.32a | 0.05 |
| eGFR | 0.29a | −0.31a | −0.03 | −0.07 |
| Glomerulosclerosis
score | −0.27a | 0.28a | 0.64a | 0.10 |
| Tubulointerstitial
damage score | −0.19b | 0.43a | 0.55b | 0.09 |
| CKD stage | −0.04 | 0.02 | 0.23a | 0.06 |
Correlation of RI with clinical and
histological parameters
The RI was correlated with the renal function and
histological damage scores and demonstrated the most evident
correlation with the TI scores among the three histological
components (Table II). However,
it was not observed to be associated with the serum creatinine
levels or CKD stage.
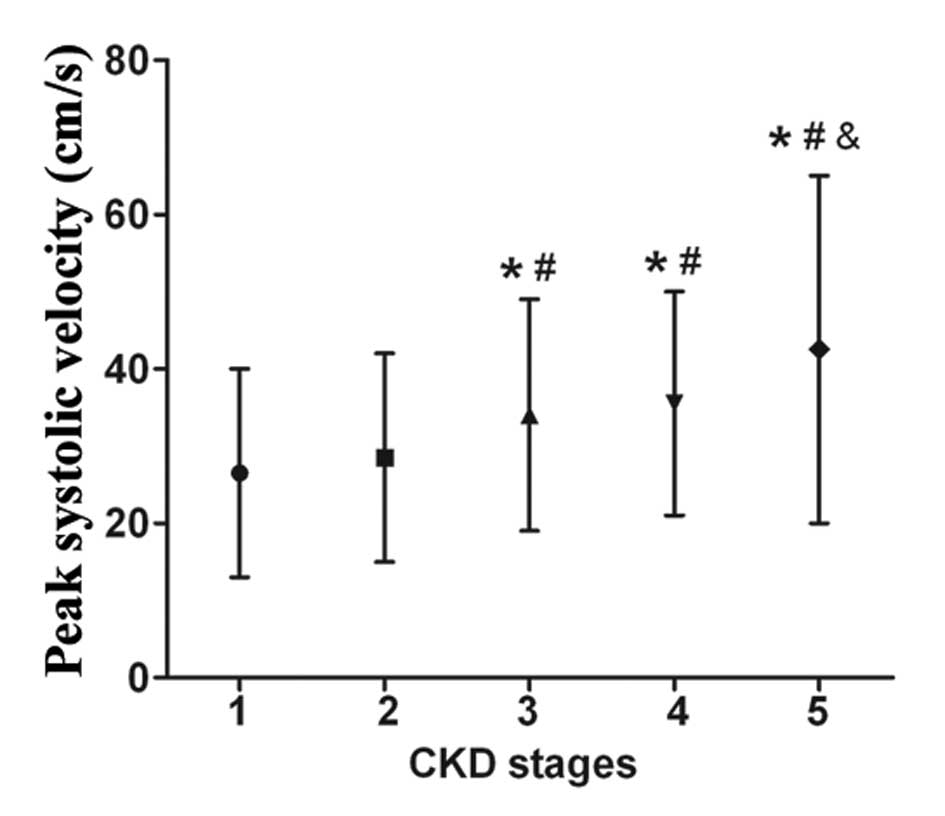
Correlation of PSV and EDV with clinical
and histological indices
No correlation of the EDV with the clinical and
histological indices was identified. By contrast, the PSV increased
as the CKD stage progressed (Fig.
2), and it was correlated with the GS (r=0.64, P<0.01) and
TI (r=0.55, P<0.01) scores, showing the strongest correlation
with the GS score among the three histological components (Table II). Stepwise multivariate
regression analysis showed that the GS (β= −0.29, P<0.01) and TI
(β=0.36, P<0.01) scores were risk factors for increased PSV in
patients with CKD.
Discussion
In the present study, the clinical significances of
various parameters of Doppler ultrasonography, including the RI,
PSV and EDV of the interlobar arteries, in patients with CKD were
investigated. Among the ultrasonographic indices, the RI and PSV
showed correlations with the renal function and histological damage
scores. PSV was also a good marker of the CKD stage, but RI was
not. By contrast, the renal length showed only a weak correlation
with renal function.
Previous studies have shown that kidney length is
often affected by the body size of a patient (10,11),
and multiple conditions, including diabetic nephropathy and amyloid
nephropathy, may also cause kidney enlargement. In agreement, the
results of the present study showed that the parameter of kidney
size was a poor indicator of the CKD stage.
In this study, the RI demonstrated a correlation
with a number of histological parameters, and the most evident was
observed with the TI score. Renal fibrosis, particularly
tubulointerstitial fibrosis, is the common outcome of almost all
cases of progressive or advanced CKD. Renal fibrosis is also a
reliable predictor of prognosis and a major determinant of renal
insufficiency (12). Consistent
with the findings of the present study, a previous study has shown
that renal arterial RI is associated with severe histological
changes and poor renal outcome during CKD (13). Thus, RI may contribute to the
identification of patients at a high risk of ESRD who may benefit
from nephroprotective treatments.
One more important finding of the present study is
that the PSV of the interlobar arteries increased as the CKD stage
progressed and it correlated with renal histological changes,
including the GS and TI scores. The PSV is a semiquantitative
indicator of intrarenal blood flow on spectral Doppler imaging, and
markedly depends on the distension of the small arteries in the
kidney. Thus, the PSV is associated with renal vascular compliance
and vascular resistance (14). The
results of the present study suggest that PSV changes in the
interlobar artery may be closely associated with a certain renal
histopathologic type; however, the detailed mechanisms remain
unknown.
Of note, the study does not suggest that any Doppler
parameter in the intrarenal artery is able to replace renal biopsy.
The present study sought to investigate the correlations between
Doppler indices and certain renal histopathological parameters,
including TI and GS. RI and PSV in the interlobar artery may
potentially be used as indicators for detecting renal dysfunction.
Further studies concerning Doppler parameters that have potential
implications for the noninvasive evaluation of kidney damage are
warranted.
Acknowledgements
This study was supported by the grants from the
National Natural Science Foundation of China (no. 81270895 and
81360137) and the Science and Technology Planning Project of
Guangdong Province (no. 2011B061300020 and 2011B061200034).
References
|
1
|
Gao J, Ng A, Shih G, Goldstein M, Kapur S,
Wang J and Min RJ: Intrarenal color duplex ultrasonography: a
window to vascular complications of renal transplants. J Ultrasound
Med. 26:1403–1418. 2007.PubMed/NCBI
|
|
2
|
Park SB, Kim JK and Cho KS: Complications
of renal transplantation: ultrasonographic evaluation. J Ultrasound
Med. 26:615–633. 2007.PubMed/NCBI
|
|
3
|
Langer JE and Jones LP: Sonographic
evaluation of the renal transplant. Ultrasound Clin. 2:73–88. 2007.
View Article : Google Scholar
|
|
4
|
Sugiura T, Nakamori A, Wada A and Fukuhara
Y: Evaluation of tubulointerstitial injury by Doppler
ultrasonography in glomerular diseases. Clin Nephrol. 61:119–126.
2004. View
Article : Google Scholar : PubMed/NCBI
|
|
5
|
Parolini C, Noce A, Staffolani E,
Giarrizzo GF, Costanzi S and Splendiani G: Renal resistive index
and long-term outcome in chronic nephropathies. Radiology.
252:888–896. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hanamura K, Tojo A, Kinugasa S, Asaba K
and Fujita T: The resistive index is a marker of renal function,
pathology, prognosis, and responsiveness to steroid therapy in
chronic kidney disease patients. Int J Nephrol. 2012:1395652012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
National Kidney Foundation. K/DOQI
clinical practice guidelines for chronic kidney disease:
evaluation, classification, and stratification. Am J Kidney Dis.
39(Suppl 1): S1–S266. 2002.PubMed/NCBI
|
|
8
|
Gao J, Chevalier J, Auh YH, Rubin JM, Wang
H, Sun LN, Seshan S and Min R: Correlation between Doppler
parameters and renal cortical fibrosis in lupus nephritis: a
preliminary observation. Ultrasound Med Biol. 39:275–282. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Asaba K, Tojo A, Onozato ML, Kinugasa S,
Miyazaki H, Miyashita K, Uehara Y, Hirata Y, Kimura K, Goto A,
Omata M and Fujita T: Long-term renal prognosis of IgA nephropathy
with therapeutic trend shifts. Intern Med. 48:883–890. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Miletić D, Fuckar Z, Sustić A, Mozetic V,
Stimac D and Zauhar G: Sonographic measurement of absolute and
relative renal length in adults. J Clin Ultrasound. 26:185–189.
1998.PubMed/NCBI
|
|
11
|
Sustić A, Mavrić Z, Fuckar Z, Miletić D,
Mozetic V and Mlinarić B: Kidney length in postoperative acute
renal failure. J Clin Ultrasound. 26:251–255. 1998.PubMed/NCBI
|
|
12
|
Liu Y: Cellular and molecular mechanisms
of renal fibrosis. Nat Rev Nephrol. 7:684–696. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bigé N, Lévy PP, Callard P, Faintuch JM,
Chigot V, Jousselin V, Ronco P and Boffa JJ: Renal arterial
resistive index is associated with severe histological changes and
poor renal outcome during chronic kidney disease. BMC Nephrol.
13:1392012.PubMed/NCBI
|
|
14
|
Krumme B: Renal Doppler sonography -
update in clinical nephrology. Nephron Clin Pract. 103:c24–c28.
2006. View Article : Google Scholar : PubMed/NCBI
|