Introduction
Recurrent pregnancy losses (RPLs) affect 1% of women
and there are a number of factors playing a part. RPL is one of the
least understood pathological processes, in spite of being one of
the most common reproductive problems. The reason for 68% of RPL
cases is idiopathic. In at least 50% of couples with RPL,
evaluation, including parental karyotyping, hysterosalpingography
or hysteroscopy and antiphospholipid antibody testing may be normal
(1).
For the successful progress of pregnancy, an
effective uteroplacental circulation is mandatory and this
circulation is affected by hemostatic disorders. Considering the
fact that hemostatic failures may cause an obstruction of the
placental vascular lacunes, unexpected changes in coagulation
factors during pregnancy may be the reason for RPL. Pregnancy is a
hypercoagulable state characterized by increased levels of
prothrombotic factors and decreased antithrombotic factors.
Apolipoprotein E (Apo E) is a protein that plays a
key role in the metabolism of cholesterol and triglycerides by
binding to receptors in the liver to mediate clearance of
chylomicrons and very-low-density lipoproteins from the bloodstream
(2). The primary site of synthesis
is in the liver; however, other organs and tissues synthesize Apo
E, including the brain, spleen, kidneys, gonads, adrenals and
macrophages. The Apo E gene has three alleles, ε2 (E2), ε3 (E3) and
ε4 (E4), which are on the long (q) arm of chromosome 19 at position
13.2 (3). The Apo E2 allele is
associated with decreased serum low-density lipoprotein (LDL)
cholesterol, whereas the Apo E4 allele is associated with higher
LDL cholesterol. The Apo E4 allele is also thought to be involved
in inflammatory responses, platelet function, apoptosis and
modulation of oxidative stress (4). The role of Apo E has also been
implicated in pregnancy and one study analyzed the effect of Apo E
polymorphisms in pre-eclampsia and RPL (5). Therefore, to investigate whether Apo
E polymorphisms affect the outcome of pregnancy, we conducted a
case-control study. The Apo E allele and genotype distributions of
RPL women were compared with those of healthy parous control
women.
Materials and methods
Patients
A total of 90 women were included in this
case-control study. Of these, 45 women had a history of ≥2
consecutive spontaneous abortions with no previous history of
successful pregnancy and 45 fertile women had at least one live
birth and had no history of spontaneous abortion. Additionally,
they had no previous history of pre-eclampsia, preterm delivery,
ectopic pregnancy or any other pregnancy-related complications, as
well as other non-obstetrical conditions, including chromosomal
abnormalities, Mullerian duct defects, abnormal immunological and
endocrinological tests and thrombophilia. Women with alcohol usage
and smokers were excluded from the study. All the samples were
collected from patients attending the outpatient department of the
Eskişehir Osmangazi University Department of Gynecology and
Obstetrics. All the couples experiencing RPL were evaluated.
Chromosome analyses were performed on all subjects. All women with
RPL were examined by ultrasonography or hysterosalpingography for
detection of anatomical abnormalities of the genital tract. They
also had blood drawn for testing for immunological risk factors,
including antiphospholipid antibodies, antinuclear antibodies,
antithyroid antibodies and lupus anticoagulant, to rule out other
causes of recurrent miscarriage. Blood samples (5 ml) from the
controls and RPL women were collected in ethylenediamine
tetraacetic acid (EDTA)-coated collection vials and DNA was
extracted using Qiagen DNA extraction kits (Qiagen, Hilden,
Germany). This study was approved by the Eskişehir Ethics Committee
No. 1. Written informed consent was obtained from all participants
prior to registering for the study.
Apo E genotyping
Fifty nanograms of genomic DNA was amplified in 25
liters PCR buffer containing 1 unit Taq DNA polymerase. A 228 bp
fragment of the human Apo E gene was amplified with specific
primers. The resulting PCR fragments were analyzed with a probe
(ApoE C112R, detected in channel 530) and with probes labeled with
LightCycler Red 640 (ApoE R158C, detected in channel 640). The Apo
E codon 112 exhibits a Tm of 49.0°C in channel 530 for allele
variant 112C and a Tm of 59.0°C in channel 530 for allele variant
112R. The Apo E codon 158 exhibits a Tm of 63.0°C in channel 640
for allele variant 158R and a Tm of 53.0°C in channel 640 for
allele variant 158C. The use of a color compensation file generated
with the LightMix kit - Color Compensation 530/640 is a
prerequisite to run the duplex reaction. The supplied control DNA
allows for the accurate comparison with unknown samples. aNot
significant. Apo E, apolipoprotein E; RPL, recurrent pregnancy
loss.
Statistical analysis
The frequencies of gene mutations were compared
between women experiencing RPL and the controls using a 2×2
contingency table with Fisher’s exact test (GraphPad InStat, San
Diego, CA, USA). A two-tailed P-value <0.05 was considered to
indicate a statistically significant difference.
Results
Our study included 45 women with RPL and 45 women
for the control group. The mean age of the RPL group was 33±0.78
years and the number of previous miscarriages ranged from 2 to 5.
The mean age of the control group was 33.5±0.7 years and there was
no significant difference between the groups (P>0.05). The mean
number of weeks before pregnancy loss in the patient group was
8.3±0.32 weeks (range, 5–18). The mean birth time for the control
group was 39.3±0.1 (range, 37–41) weeks.
The frequency of the Apo E genotypes for patients
and controls are shown in Table I.
In the RPL group, 66 chromosomes (73.3%) were positive for Apo E3,
16 (17.7%) were positive for Apo E4 and 8 (9%) were positive for
Apo E2. In the control group, 60 chromosomes (66.6%) were positive
for Apo E3, 18 (20%) were positive for Apo E4 and 12 (13.4%) were
positive for Apo E2.
 | Table IDistribution of Apo E alleles among
RPL patients and controls. |
Table I
Distribution of Apo E alleles among
RPL patients and controls.
| Apo E allele | RPL, n (%) | Control, n (%) | P-value |
|---|
| 2 | 8 (9) | 12 (13.4) | 0.342a |
| 3 | 66 (73.3) | 60 (66.6) | 0.328a |
| 4 | 16 (17.7) | 18 (20) | 0.703a |
Apo E3 was the most frequent allele and Apo E2 was
the rarest allele in the two groups. There was no significant
difference in Apo E alleles in the two groups. Apo E2 was observed
less in the patient group than in the control group; however, this
was not statistically significant. There was no significant
difference in Apo E genotype between the RPL and control groups.
The most frequent genotype was Apo E3/E3 for the two groups.
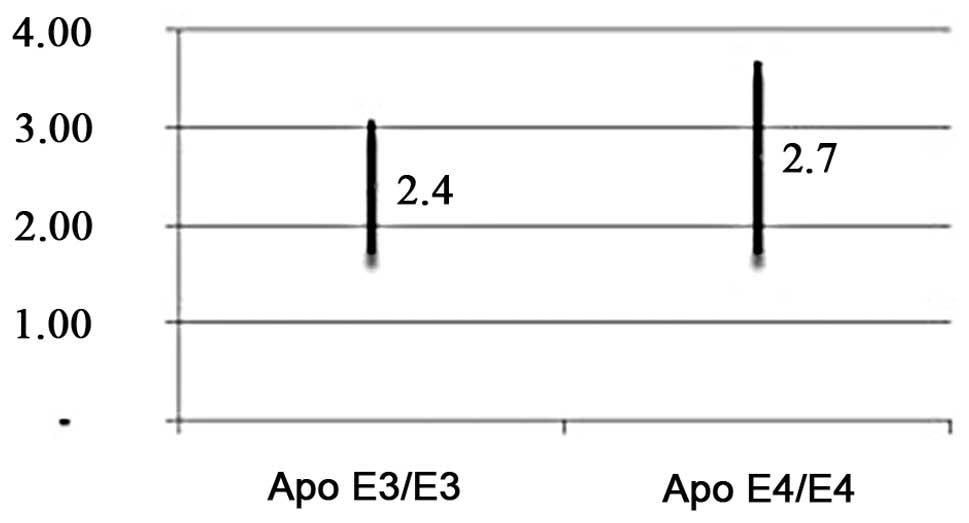
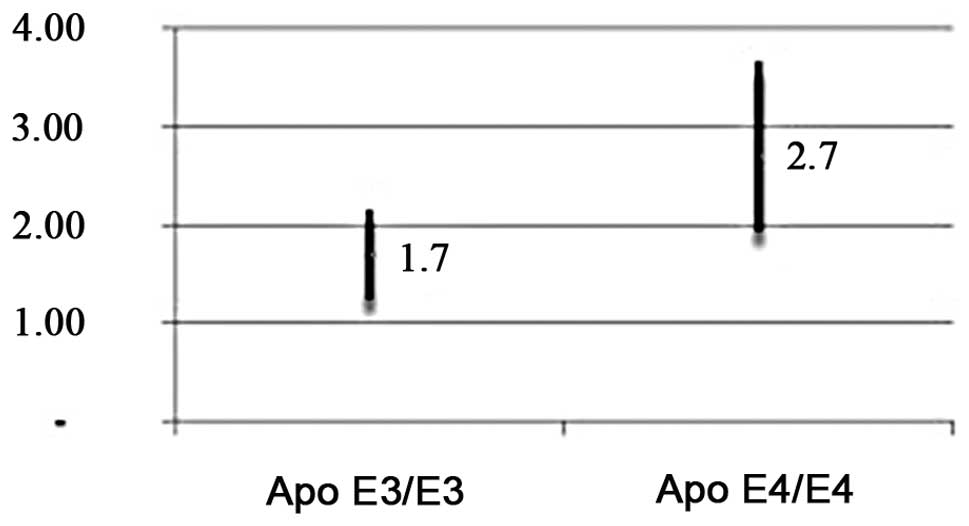
In the RPL group, the mean spontaneous abortion rate
was 2.4±0.65 for the Apo E3/E3 genotype and 2.7±0.95 for the Apo
E4/E4 genotype (P>0.05; Fig.
1). In the control group, the mean pregnancy rate was 1.7±0.43
for the Apo E3/E3 genotype and 2.8±0.83 for the Apo E4/E4 genotype.
(P>0.05; Fig. 2).
Discussion
In this study, we examined Apo E gene polymorphisms
and their association with RPL. According to our results, there is
no significant correlation between RPL and Apo E gene
polymorphisms. The Apo E4 allele has been shown to be associated
with an elevated risk of recurrent miscarriage in a previous study
(6). Furthermore, Ergin et
al(7) reported an increased
prevalence of Apo E3/3 and E4/4 genotypes among Turkish women
experiencing RPL. Conversely, a study conducted on 150 RPL patients
and 160 controls reported that there was no association between Apo
E polymorphisms and RPL (8). They
concluded that the clinical management of RPL patients should not
be affected by the presence or absence of Apo E polymorphisms.
Apo E genotype distribution differs among
populations. Eichner et al(3) reviewed the frequencies of E2, E3 and
E4 alleles in different populations and reported that these range
from 0.02–0.13 for E2, 0.06–0.85 for E3 and 0.11–0.31 for E4. In
our study, Apo E3 (73.3–66.6%) was the most frequent Apo E allele
in the two groups. There were no significant differences in the
frequency of Apo E alleles. The Apo E2 (9–13.4%) allele was the
rarest gene in the two groups.
Apo E is a glycosylated protein characterized by its
wide tissue distribution and multiple functions. Apo E
polymorphisms have been extensively studied in a variety of
diseases, including multiple sclerosis (9) and Alzheimer’s disease (10). Significantly higher plasma LDL
concentrations have been observed in individuals with the Apo E4
allele. Elevated plasma lipid levels contribute to the pathogenesis
of thrombus formation by accumulating in the intima of blood
vessels whose endothelial cells have been activated by inflammatory
cytokines (11). Apo E has also
been shown to play an important role in the inflammatory response.
Animals expressing the E4 allele have significantly greater
systemic elevations of the pro-inflammatory cytokines, tumor
necrosis factor (TNF)-α and interleukin (IL)-6 (12). As pregnancy is a hypercoagulable
state, it is not surprising that the additive effect of an Apo E4
genotype superimposed on this hypercoagulable state increases the
risk of clotting. Pregnant women have an increased risk of
thromboembolism compared with non-pregnant women, with an
underlying rate of venous thrombosis of ∼1/1,000 pregnancies
(13).
The role of thrombophilia in the causation of RPL
has been proven. Inherited thrombophilia is considered to be a
multifactorial condition in which susceptibility is conferred by a
number of genetic polymorphisms (14). This may explain why women who carry
the thrombophilic mutation in one of the susceptibility genes do
not develop the thrombotic complications. The impact of
polymorphisms of the Apo E allele on reproductive outcome is being
pursued and has yielded conflicting conclusions.
Corbo et al(15) identified that the lowest
reproductive efficiency occurs with the presence of the E2 allele,
intermediate with the E4 allele and highest with the E3 allele.
Zetterberg et al(16)
compared the frequency of Apo E alleles in spontaneous abortuses
and the adult population and reported that the E4 allele may have
embryo protective effects. In one of the studies, altered
expression of the Apo E3 isoform has been implicated in women
having pre-eclampsia during pregnancy, whereas another study
observed no association between Apo E polymorphisms and a
pre-eclampsia state (5,17). In another study, a mild to moderate
association was observed in Apo E gene mutation in women with RPL
compared to controls (18).
We conducted this study on a group of 45 RPL
patients and their genotype frequencies were compared with those of
45 control samples. We observed no correlation between RPL and Apo
E polymorphisms. Further studies should use an appropriate sample
size. The confusion regarding the role of Apo E in RPL may be
addressed through multicenter studies where samples of different
ethnicities, using the same selection criteria for the RPL group
and controls, are used.
In conclusion, our findings show that further
studies on Apo E gene polymorphisms in RPL are not required. With
growing awareness of the correlation between genetic factors
influencing hemostasis and pregnancy-related disorders,
documentation of thrombotic causes are important due to the
potential of performing randomized controlled clinical trials to
determine the effect of thromboprophylaxis in such cases.
Acknowledgements
The grant for this project was kindly
provided by the Eskişehir Osmangazi University, Scientific Research
Projects Commitee, Eskişehir, Turkey.
References
|
1.
|
Ford HB and Schust DJ: Recurrent pregnancy
loss: etiology, diagnosis, and therapy. Rev Obstet Gynecol.
2:76–83. 2009.PubMed/NCBI
|
|
2.
|
Mahley RW: Apolipoprotein E: cholesterol
transport protein with expanding role in cell biology. Science.
240:622–630. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Eichner JE, Dunn ST, Perveen G, Thompson
DM, Stewart KE and Stroehla BC: Apolipoprotein E polymorphism and
cardiovascular disease: a HuGE review. Am J Epidemiol. 155:487–495.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Bennet AM, Di Angelantonio E, Ye Z,
Wensley F, et al: Association of apolipoprotein E genotypes with
lipid levels and coronary risk. JAMA. 298:1300–1311. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Atkinson KR, Blumenstein M, Black MA, et
al: An altered pattern of circulating apolipoprotein E3 isoforms is
implicated in preeclampsia. J Lipid Res. 501:71–80. 2009.PubMed/NCBI
|
|
6.
|
Goodman C, Goodman CS, Hur J, Jeyendran RS
and Coulam C: The association of Apoprotein E polymorphisms with
recurrent pregnancy loss. Am J Reprod Immunol. 61:34–38. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Ergin E, Jeyendran RS, Ozornek H, Ozay A,
Pillai MD and Coulam C: Is apolipoprotein E codon 112 polymorphism
associated with recurrent pregnancy loss? Fertil Steril.
92:1152009. View Article : Google Scholar
|
|
8.
|
Bianca S, Barrano B, Cutuli N, et al: No
association between apolipoprotein E polymorphisms and recurrent
pregnancy loss. Fertil Steril. 93:2762010. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Shi J, Zhao CB, Vollmer TL, Tyry TM and
Kuniyoshi SM: APOE epsilon 4 allele is associated with cognitive
impairment patients with multiple sclerosis. Neurology. 70:185–190.
2008. View Article : Google Scholar
|
|
10.
|
Huang Y, Weisgraber KH, Mucke L and Mahley
RW: Apolipo-protein E: diversity of cellular origins, structural
and biophysical properties, and effects in Alzheimer’s disease. J
Mol Neurosci. 23:189–204. 2004.PubMed/NCBI
|
|
11.
|
Libby P: Current concepts of the
pathogenesis of the acute coronary syndromes. Circulation.
104:365–372. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Lynch JR, Tang W, Wang H, et al: APOE
genotype and an ApoE-mimetic peptide modify the systemic and
central nervous system inflammatory response. J Biol Chem.
278:48529–48533. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Greer IA: The challenge of thrombophilia
in maternal-fetal medicine. N Engl J Med. 342:424–425. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Coulam CB, Jeyendran RS, Fishel LA and
Roussev R: Multiple thrombophilic gene mutations rather than
specific gene mutations are risk factors for recurrent miscarriage.
Am J Reprod Immunol. 55:360–368. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Corbo RM, Scacchi R and Cresta M:
Differential reproductive efficiency associated with common
apolipoprotein e alleles in postreproductive-aged subjects. Fertil
Steril. 81:104–107. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Zetterberg H, Palmér M, Ricksten A, et al:
Influence of the apolipoprotein E epsilon4 allele on human
embryonic development. Neurosci Lett. 324:189–192. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Makkonen N, Heinonen S, Hiltunen M,
Helisalmi S, Mannermaa A and Kirkinen P: Apolipoprotein E alleles
in women with pre-eclampsia. J Clin Pathol. 54:652–654. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Yenicesu GI, Cetin M, Ozdemir O, et al: A
prospective case-control study analyzes 12 thrombophilic gene
mutations in Turkish couples with recurrent pregnancy loss. Am J
Reprod Immunol. 63:126–36. 2010. View Article : Google Scholar : PubMed/NCBI
|