Introduction
In previous years, there has been a global increase
in the incidence of tuberculosis (TB), along with the prevalence of
acquired immunodeficiency syndrome, and the emergence of
multidrug-resistant strains. Tuberculous peritonitis (TBP) is
primarily caused by hematogenous spread and rarely results from the
contagious spread of an infected bowel or fallopian tubes (1,2). It
is estimated that TBP represents 4–10% of all extrapulmonary TB
cases (3,4).
Diagnosis of TBP is difficult since the clinical
features are nonspecific and ascitic fluid may contain few tubercle
bacilli that can neither be observed nor cultured. Undiagnosed and
untreated TBP results in a mortality rate of 50–60% (5); however, the disease is usually
curable when treated properly. Patients with liver cirrhosis are at
an increased risk of developing TBP (6,7). TBP
in cirrhotic patients can mimic spontaneous bacterial peritonitis
(SBP) and is frequently not considered in differential diagnosis,
resulting in delayed diagnosis and even mortality (7). Awareness of the clinical features of
TBP in patients with cirrhosis is crucial for improving diagnostic
accuracy and survival. However, the study of TBP characteristics in
patients with cirrhosis, compared with those of SBP, is limited
(8). Therefore, a retrospective,
matched case-control study was performed to compare the clinical
characteristics of TBP and SBP in patients with cirrhosis.
Materials and methods
Patient selection
In this retrospective study, the hospital records of
12 patients with cirrhosis who were diagnosed with TBP in the
Zhejiang Provincial People’s Hospital (Hangzhou, China) between
2008 and 2011 were reviewed. For the purpose of comparison, 25
patients with definite SBP were selected that matched the TBP
patients in age and gender during the same period. The study was
approved by the Human Ethics Committee of Zhejiang Provincial
People’s Hospital. Written informed consent was obtained from the
patient’s family.
Methods
The diagnosis of liver cirrhosis was confirmed by
clinical observations, image analysis or the presence of
esophagogastric varices. The severity of liver cirrhosis was graded
according to the Child-Pugh classification. Patients with human
immunodeficiency virus coinfection or hepatocellular carcinoma were
excluded.
All 12 cirrhotic patients with compatible symptoms,
including fever, abdominal pain and distention, were diagnosed with
TBP if one or more of the following criteria was met: i) Positive
culture of Mycobacterium tuberculosis from ascites; ii)
positive detection of acid-fast bacilli in ascites; iii)
demonstration of caseating granulomata in histological examination
of peritoneal biopsy specimens; iv) positive detection of
Mycobacterium tuberculosis in ascites after polymerase chain
reaction (PCR); and v) response to antituberculous therapy.
All 25 patients with cirrhosis and clinical
manifestations of SBP were diagnosed with definite SBP, defined as
SBP caused by one monobacteria (culture was positive for ascites)
and a polymorphonuclear leukocyte count in the ascitic fluid of
≥250 cells/μl. Patients with suspected secondary peritonitis were
excluded, as discussed by Rimola et al (9).
Patient demographics, clinical manifestations,
presence of extraperitoneal tuberculosis, hematological data,
ascetic fluid analysis and the culture of ascites for bacteria were
recorded. The culture of biopsies or ascitic fluid for
Mycobacterium tuberculosis was not performed.
Statistical analyses
Proportions were compared using the χ2
test or a two-tailed Fisher’s exact test. Continuous variables were
compared using the Student’s t-test or the Mann-Whitney U test.
Statistical analyses were performed using SPSS software, version
12.0 (SPSS, Inc., Chicago, IL, USA). P<0.05 was considered to
indicate a statistically significant difference.
Results
Demographic and clinical
manifestations
Demographic and clinical characteristics of the 37
participants are shown in Table I.
In the TBP group, three cases demonstrated caseating granulomata
following histological assessment, two cases showed a positive
culture of Mycobacterium tuberculosis, two cases detected
positive for acid-fast bacilli and in the remaining five patients,
diagnosis was based on the positive result of PCR and the response
to antituberculous therapy. Of the 25 patients in the SBP group, 12
cases were infected with Escherichia coli, seven cases were
infected with Klebsiella species, three cases were infected
with Streptococcus species, two cases were infected with
Staphylococcus species and one case was infected with
Aeromonas species. The frequency of Child-Pugh class B was
significantly higher in the TBP group when compared with the SBP
group [8/12 patients (67%) vs. 8/25 patients (32%); P<0.05].
Three cases (25%) in the TBP group exhibited pulmonary TB, but no
case was identified in the SBP group. A statistically significant
increase in the median duration of symptoms prior to presentation
was observed in the TBP group (39.67±30.00 vs. 21.60±21.50 days;
P<0.05). There were no other statistically significant
differences between the groups with regard to age, gender, etiology
of cirrhosis and initial clinical symptoms.
 | Table IDemographic and clinical
characteristics of the study population. |
Table I
Demographic and clinical
characteristics of the study population.
| Characteristics | TBP (n=12) | SBP (n=25) | P-value |
|---|
| Age, years | 58.75±12.66a | 57.84±14.19a | NS |
| Male, n (%) | 8 (67) | 16 (64) | NS |
| Etiology of
cirrhosis, n (%) |
| Hepatitis B
virus | 8 (67) | 17 (68) | NS |
| Hepatitis C
virus | 0 | 1 (4) | NS |
| Alcohol | 3 (25) | 3 (12) | NS |
| Schistosome | 1 (8) | 2 (8) | NS |
| Biliary | 0 | 2 (8) | NS |
| Child-Pugh class, n
(%) | | | <0.05 |
| B | 8 (67) | 8 (32) | |
| C | 4 (33) | 17 (68) | |
| Tuberculosis at other
site, n (%) | 3 (25) | 0 (0) | <0.01 |
| Duration of symptoms
before presentation, days | 39.67±30.00a | 21.60±21.50a | <0.05 |
| Initial symptoms, n
(%) |
| Abdominal
distension | 11 (92) | 23 (92) | NS |
| Fever | 6 (50) | 8 (32) | NS |
| Abdominal pain | 5 (42) | 9 (36) | NS |
| Diarrhea | 3 (25) | 6 (24) | NS |
Laboratory observations
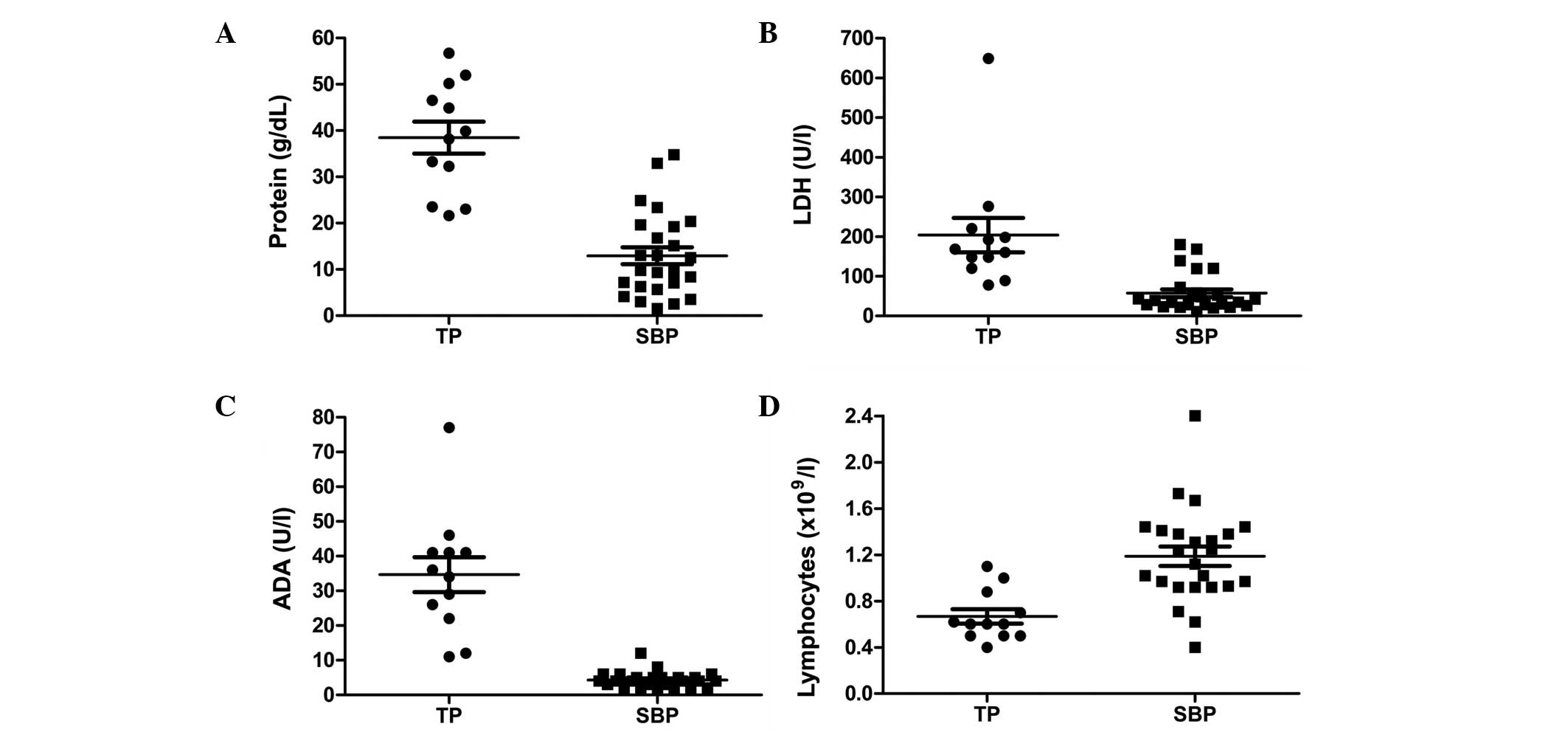
Laboratory observations are summarized in Table II and Fig. 1. The mean peripheral total white
cell count did not differ significantly between the two groups, but
the lymphocyte population was significantly decreased in the TBP
group when compared with the SBP group (0.67±0.22×109/l
vs. 1.19±0.41×109/l; P<0.01). The serum levels of
cancer antigen (CA)-125 in the two groups were elevated, but no
significant difference was observed. The mean serum protein and
albumin concentrations were significantly higher in the TBP group.
In addition, the ascitic total white cell count was increased in
the TBP group when compared with the SBP group, but no significant
difference was observed. However, the proportion of white blood
cells was statistically different with 11 cases (92%) with
lymphocytic predominance in the TBP group and 17 cases (68%) with
neutrophil predominance in the SBP group. Patients in the TBP group
had significantly higher ascitic protein, adenosine deaminase (ADA)
and lactate dehydrogenase (LDH) levels when compared with those in
the SBP group, whereas the distribution of the serum ascites
albumin gradient did not differ between the two groups. The ascitic
protein level was >25 g/l in 9 patients (75%) in the TBP group
(range, 21.62–56.70 g/l) and 2 patients (8%) in the SBP group
(range, 1.50–34.80 g/l). Ascitic ADA activity levels were >27
U/l in 8 patients (67%) in the TBP group (range, 11–77 U/l), but no
patients in the SBP group had levels >27 U/l (range, 2–12 U/l).
The ascitic LDH level was >90 U/l in 10 patients (83%) in the
TBP group (range, 78–649 U/l) and 5 patients (20%) in the SBP group
(range, 11–180 U/l).
| Table IILaboratory observations of patients
with TBP and SBP. |
Table II
Laboratory observations of patients
with TBP and SBP.
| Parameters | TBP (n=12) | SBP (n=25) | P-value |
|---|
| Hematological
observations upon admission |
| White cell count,
109/l | 4.83±1.45a | 7.58±5.78a | NS |
| Lymphocyte,
109/l | 0.67±0.22a | 1.19±0.41a | <0.01 |
| Protein, g/l | 71.19±7.28a | 63.90±8.92a | <0.05 |
| Albumin, g/l | 31.62±5.08a | 27.48±4.16a | <0.05 |
| CA-125, U/ml | 594±504a | 439±340a | NS |
| Ascitic fluid
observations upon admission |
| White cell count,
μl | 1840±1503a | 1390±1912a | NS |
| Lymphocyte
predominant, n (%) | 11 (92) | 1 (4) | <0.01 |
| Neutrophil
predominant, n (%) | 0 | 17 (68) | <0.01 |
| Monocyte
predominant, n (%) | 0 | 4 (16) | NS |
| Equivocal, n
(%) | 1 (8) | 3 (12) | NS |
| Protein, g/dl | 38.50±11.96a | 12.94±9.16a | 0 |
| >25 g/l, n
(%) | 9 (75) | 2 (8) | 0 |
| SAAG |
| ≥11 g/l | 10 (83) | 22 (88) | NS |
| ADA, U/l | 34.67±17.54a | 4.32±2.25a | 0 |
| ≥30 U/l, n
(%) | 8 (67) | 0 | 0 |
| LDH, U/l |
203.83±150.55a | 57.44±48.06a | 0 |
| ≥90 U/l | 10 (83) | 5 (20) | 0 |
Discussion
The therapeutic techniques to treat TBP and SBP
differ largely. TBP requires conservative quadruple
antituberculosis treatment, while SBP requires empirical
antimicrobial therapy. However, the diagnostic complications of TBP
presents a technical hindrance for effective therapy for these
patients.
TBP in patients with cirrhosis presents with
nonspecific signs and symptoms, including abdominal distension,
fever, abdominal pain and diarrhea, and hence mimics those of SBP.
In the present study, it was identified that the clinical symptoms
are similar between TBP and SBP in patients with cirrhosis. The
onset of TBP is often insidious, even in patients with cirrhosis
(7,8). Consistent with a previous study, the
median duration of symptoms prior to presentation was >1 month
for cirrhotic patients with TBP (8). All patients were examined for signs
of TB at additional sites and three cases (25%) in the TBP group
were diagnosed with pulmonary TB, but no cases were identified in
the SBP group. Therefore, examination for TB at additional sites is
important for diagnosing TBP.
Numerous studies have demonstrated that SBP occurs
mainly in cirrhotic patients with Child-Pugh class C (10,11),
with only one study demonstrating that TBP occurs primarily in
cirrhotic patients with Child-Pugh class B (8). The present study revealed similar
results with 17 cases (68%) of Child-Pugh class C in the SBP group
and 8 cases (67%) of Child-Pugh class B in the TBP group. The
present results also indicate that compared with SBP, TBP may
develop relatively early in the course of cirrhosis. In addition,
the higher protein and albumin concentrations in the serum of
cirrhotic patients with TBP may elucidate why the Child-Pugh class
is mainly type B in the TBP group.
Notably, there was a significant decrease in the
number of lymphocytes in the peripheral blood of cirrhotic patients
with TBP. CD4+ T-lymphopenia is considered to be a reaction of
mycobacterial infection and not a manifestation of underlying
secondary immunodeficiency (12).
Chau et al (13)
hypothesized that sequestration of lymphocytes in the peritoneum
may result in lymphopenia in the peripheral blood during a later
phase of TBP. Therefore, lymphopenia in the peripheral blood may
function as a marker for TBP.
Previous studies have shown that an elevation of
serum CA-125 levels may be used as a novel marker for the diagnosis
and follow-up of patients with TBP (14,15).
In the present study, the serum levels of CA-125 in the two groups
were found to be elevated, however, no significant difference was
observed. These results were not comparable with earlier
observations since there have been no previous studies on the
advantages of determining serum CA-125 levels for the diagnosis of
TBP and SBP.
The predominance of lymphocytes in ascites is a
characteristic of TBP (16). In
the present study, 11 cases (92%) were identified to have
lymphocytic predominance in the TBP group, while 17 cases (68%) had
neutrophil predominance in the SBP group. Therefore, we
hypothesized that the aforementioned ascitic fluid features may be
a good indicator for diagnosis. In addition, patients in the TBP
group were observed to have significantly higher ascitic fluid
total protein levels when compared with the SBP group. Several
studies have demonstrated that patients with an ascitic protein
level of >25 g/l have a high sensitivity for TBP (6,8). In
the present study, the ascitic protein level was >25 g/l in 9
patients (75%) in the TBP group, but only in 2 patients (8%) in the
SBP group. The protein concentration in the ascites of cirrhotic
patients with SBP was ~13 g/l (17). Therefore, a higher protein
concentration in the ascites may be considered as a useful marker
for the diagnosis of TBP.
ADA has been investigated as a rapid diagnostic tool
for TBP (18), however, the role
of ADA in the setting of cirrhosis is controversial (19,20).
Hillebrand et al (19)
identified that ADA activity showed imperfect specificity and low
sensitivity in cirrhotic patients with TBP. These observations were
countered by Liao et al (20), who reported that ADA activity
showed a high specificity and sensitivity in those patients using a
cut-off value of >27 U/l. In the present study, the mean ascitic
ADA activity level in 12 patients with cirrhosis and TBP was 35.58
U/l and 8 of these patients had ADA activity level >27 U/l. The
maximum ascitic ADA activity level in the 25 patients with SBP was
12 U/l with a mean of 4.32 U/l. Therefore, we hypothesize that the
examination of ADA activity is a critical test for diagnosing
TBP.
Ascitic LDH levels increased due to the release of
LDH from neutrophils (16).
Elevation of ascitic LDH may be associated with numerous diseases,
including TBP (6,7) and SBP (21). A previous study has demonstrated
that an ascitic LDH level of >90 U/l is a useful parameter with
high sensitivity and low specificity for the screening of TBP,
irrespective of the presence of liver cirrhosis (6). In the present study, the mean ascitic
LDH level in the TBP group was 204 U/l and 10 of these patients
showed an LDH level of >90 U/l. The maximum ascetic LDH level in
the SBP group was 180 U/l with a mean of 57 U/l. Therefore, in a
clinical setting, this parameter may be useful in discriminating
against TBP.
It is important to be aware of the possibility of
TBP in cirrhotic patients with ascites, including patients with
known portal hypertension or SBP. In conclusion, clinical features
and elevated serum CA-125 levels may not be specific in
differentiating from SBP. However, TBP should be considered with
the following criteria: Cirrhotic patients with Child Pugh class B;
TB identified at additional sites; lymphopenia in the peripheral
blood; an ascitic protein concentration of >25 g/l; a
predominance of lymphocytes in ascites; ascitic ADA activity levels
of >27 U/l; and ascitic LDH levels of >90 U/l.
Acknowledgements
The study was supported by a grant from the Zhejiang
Provincial Natural Science Foundation of China (no. LY12H03014) and
the Zhejiang Province Health Bureau (no.2012KYA016).
References
|
1
|
Mehta JB, Dutt A, Harvill L and Mathews
KM: Epidemiology of extrapulmonary tuberculosis. A comparative
analysis with pre-AIDS era. Chest. 99:1134–1138. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tang LC, Cho HK and Wong Taam VC: Atypical
presentation of female genital tract tuberculosis. Eur J Obstet
Gynecol Reprod Biol. 17:355–363. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Demir K, Okten A, Kaymakoglu S, et al:
Tuberculous peritonitis - reports of 26 cases, detailing diagnostic
and therapeutic problems. Eur J Gastroenterol Hepatol. 13:581–585.
2001.PubMed/NCBI
|
|
4
|
Sochocky S: Tuberculous peritonitis. A
review of 100 cases. Am Rev Respir Dis. 95:398–401. 1967.PubMed/NCBI
|
|
5
|
Chow KM, Chow VC, Hung LC, Wong SM and
Szeto CC: Tuberculous peritonitis-associated mortality is high
among patients waiting for the results of mycobacterial cultures of
ascitic fluid samples. Clin Infect Dis. 35:409–413. 2002.
View Article : Google Scholar
|
|
6
|
Shakil AO, Korula J, Kanel GC, Murray NG
and Reynolds TB: Diagnostic features of tuberculous peritonitis in
the absence and presence of chronic liver disease: a case control
study. Am J Med. 100:179–185. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Aguado JM, Pons F, Casafont F, San Miguel
G and Valle R: Tuberculous peritonitis: a study comparing cirrhotic
and noncirrhotic patients. J Clin Gastroenterol. 12:550–554. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kim NJ, Choo EJ, Kwak YG, et al:
Tuberculous peritonitis in cirrhotic patients: comparison of
spontaneous bacterial peritonitis caused by Escherichia coli
with tuberculous peritonitis. Scand J Infect Dis. 41:852–856. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rimola A, García-Tsao G, Navasa M, et al:
Diagnosis, treatment and prophylaxis of spontaneous bacterial
peritonitis: a consensus document. International Ascites Club. J
Hepatol. 32:142–153. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Choi JP, Lee SO, Kwon HH, et al: Clinical
significance of spontaneous Aeromonas bacterial peritonitis
in cirrhotic patients: a matched case-control study. Clin Infect
Dis. 47:66–72. 2008.PubMed/NCBI
|
|
11
|
Choi EJ, Lee HJ, Kim KO, et al:
Association between acid suppressive therapy and spontaneous
bacterial peritonitis in cirrhotic patients with ascites. Scand J
Gastroenterol. 46:616–620. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Beck JS, Potts RC, Kardjito T and Grange
JM: T4 lymphopenia in patients with active pulmonary tuberculosis.
Clin Exp Immunol. 60:49–54. 1985.
|
|
13
|
Chau TN, Leung VK, Wong S, et al:
Diagnostic challenges of tuberculosis peritonitis in patients with
and without end-stage renal failure. Clin Infect Dis. 45:e141–e146.
2007. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mas MR, Cömert B, Sağlamkaya U, et al:
CA-125; a new marker for diagnosis and follow-up of patients with
tuberculous peritonitis. Dig Liver Dis. 32:595–597. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Choi CH, Kim CJ, Lee YY, et al: Peritoneal
tuberculosis: a retrospective review of 20 cases and comparison
with primary peritoneal carcinoma. Int J Gynecol Cancer.
20:798–803. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sanai FM and Bzeizi KI: Systematic review:
tuberculous peritonitis - presenting features, diagnostic
strategies and treatment. Aliment Pharmacol Ther. 22:685–700. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Shaw E, Castellote J, Santín M, et al:
Clinical features and outcome of spontaneous bacterial peritonitis
in HIV-infected cirrhotic patients: a case-control study. Eur J
Clin Microbiol Infect Dis. 25:291–298. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Riquelme A, Calvo M, Salech F, et al:
Value of adenosine deaminase (ADA) in ascitic fluid for the
diagnosis of tuberculous peritonitis: a meta-analysis. J Clin
Gastroenterol. 40:705–710. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hillebrand DJ, Runyon BA, Yasmineh WG and
Rynders GP: Ascitic fluid adenosine deaminase insensitivity in
detecting tuberculous peritonitis in the United States. Hepatology.
24:1408–1412. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Liao YJ, Wu CY, Lee SW, Lee CL, Yang SS,
Chang CS and Lee TY: Adenosine deaminase activity in tuberculous
peritonitis among patients with underlying liver cirrhosis. World J
Gastroenterol. 18:5260–5265. 2012.PubMed/NCBI
|
|
21
|
Sevinc A, Sari R and Fadillioglu E: The
utility of lactate dehydrogenase isoenzyme pattern in the
diagnostic evaluation of malignant and nonmalignant ascites. J Natl
Med Assoc. 97:79–84. 2005.PubMed/NCBI
|