Introduction
Acute appendicitis is the most common etiology of
acute abdomen (1). Appendicectomy
has been the predominant treatment of acute appendicitis for more
than a century since being introduced by McBurney in the 1880’s and
being performed by Grooves in 1883. Since then, the procedure has
been standardized among surgeons (2). In 1886, Fitz published a classic
study of 247 patients with perforated appendicitis, whereby early
appendectomy was advocated (3). As
a classic surgical procedure, open appendicectomy is considered to
be safe and effective surgery for acute appendicitis that avoids
perforation. It is the gold standard treatment of appendicitis due
to low morbidity, short length of hospitalization and rare
postoperative complications. Prompt appendicectomy is traditionally
used for treating acute appendicitis, with the exception of
immediate appendicectomy, which may be technically demanding due to
the distorted anatomy and difficulties in closing the appendiceal
stump as a result of inflamed tissues (4). Exploratory laparotomy often results
in an ileocecal resection or a right-sided hemicolectomy due to
technical problems or a suspicion of malignancy resulting from the
presence of distorted tissues (5).
Nonoperative management has been used for a number
of patients. In 1959, Coldrey reported 471 patients who underwent
treatment with antibiotics alone and in 1977, Anonymous reported
425 patients who were treated with antibiotics and traditional
Chinese medicine (6,7). Previously, nonoperative treatment has
played a minor role in treating acute appendicitis. However, it may
be used to avoid surgical complications, including small bowel
obstruction and negative appendicectomy. Recently, with the
development of imaging diagnosis, including computerized tomography
and ultrasound, nonoperative therapy for the treatment of acute
appendicitis has acquired increasing interest. Investigations into
novel and efficient antibiotics have also provided new
opportunities for nonsurgical treatment of appendicitis (8). Antibiotic therapy, the main
nonoperative therapy, is becoming increasingly important in the
treatment of acute appendicitis (9,10).
Previous studies have shown that perforated appendicitis in
children may be treated with antibiotics (11–13).
Furthermore, retrospective studies in adults with perforated
appendicitis who were treated conservatively indicated that late
recurrences exhibited a mild clinical course (14). However, morbidity and mortality
rates remained unsatisfactory for conservatively treated and
appendectomized patients.
Randomized controlled trials (RCTs) have been
conducted, however, the benefits of appendicectomy versus
antibiotic treatment for appendicitis remain in debate. Specific
studies have suggested that the surgical approach demonstrates a
number of advantages, while other studies have been unable to
conclusively identify a significant difference between the two
treatments (15,16). Therefore, the aim of the present
meta-analysis was to compare antibiotic and appendicectomy
treatment for acute appendicitis in cases where surgeons were not
limited by technical constraints.
Materials and methods
Search strategy
Objectives, search strategy, study selection
criteria, data elements, methods for extraction and methods for
assessing study quality were defined. Four independent reviewers
completed each step in this protocol and resolved disagreements by
discussion.
Literature search
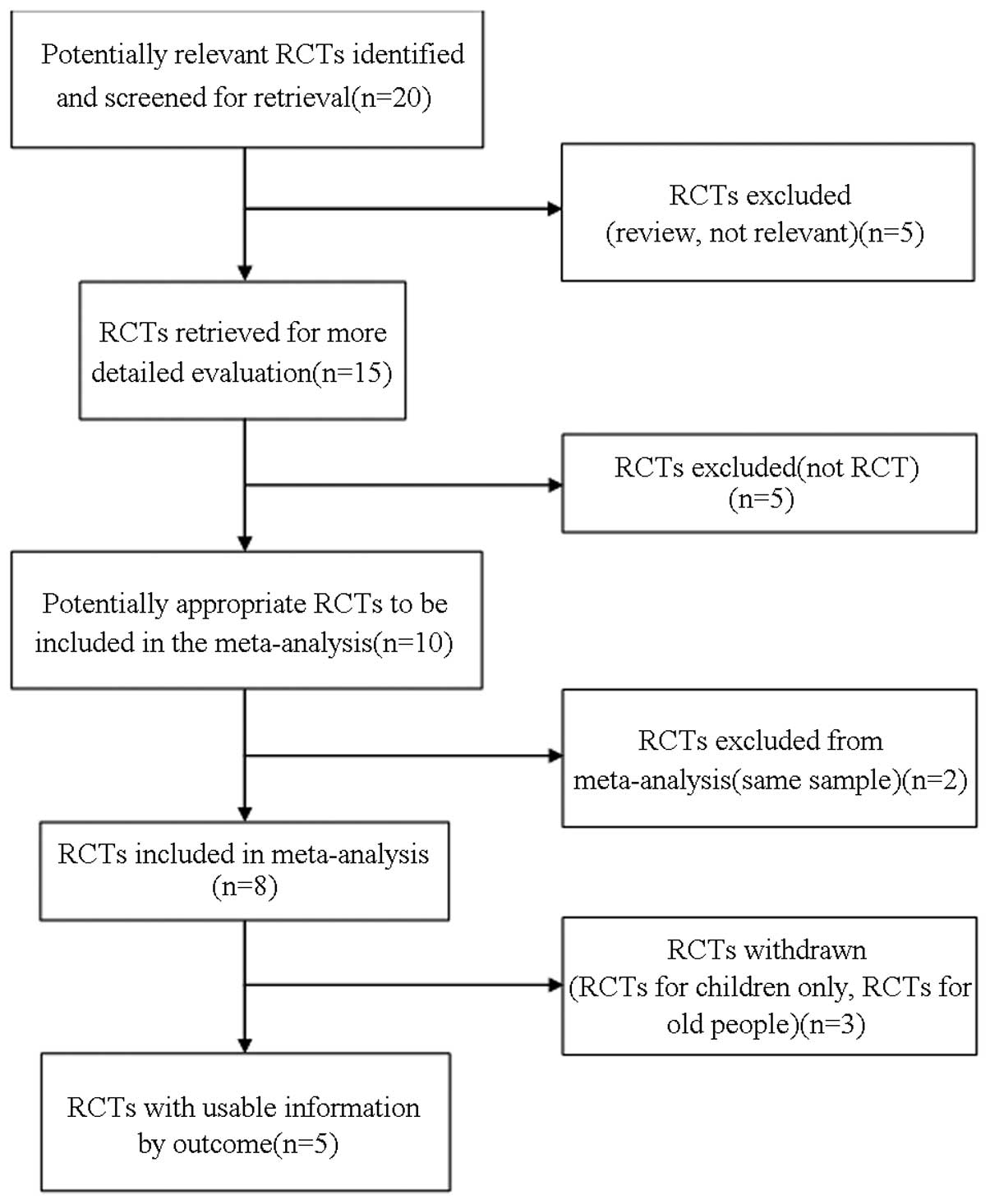
To identify all the relevant studies, a computerized
search (Medline, http://www.ncbi.nlm.nih.gov/pubmed; Embase, http://www.embase.com/info/helpfiles/;
and The Cochrane Library, http://www.thecochranelibrary.com/) was performed
using the terms ‘antibiotic’, ‘appendicectomy’, ‘acute
appendicitis’, ‘versus’ and ‘conservative’ (Fig. 1). In addition, the reference lists
in selected articles were searched manually. There was no language
restriction and the time frame was between June 1996 and September
2012. Relevant RCTs were identified that compared antibiotics with
surgery for the treatment of acute appendicitis in cases where
surgeons were not limited by technical constraints. All patient
groups were well matched in terms of subjects and clinical and
diagnostic variables at inclusion. Appendicectomy was performed
openly or laparoscopically at the surgeon’s discretion. Whenever
possible, surgery was performed by a training registrar with an
experienced surgeon supervising the operation. Patients in the
antibiotic group received intravenous antibiotics for at least 24 h
and those whose clinical status had improved the following day were
discharged to continue with oral antibiotics for ~10 days. In
patients whose clinical conditions showed no improvement,
intravenous treatment was prolonged.
Study selection
Citations selected from the initial search were
subsequently screened for eligibility. Diagnosis of appendicitis,
determined by the attending physician, was made on the following
criteria: History of right lower quadrant pain or periumbilical
pain migrating to the right lower quadrant with nausea or vomiting;
fever of >38°C or leukocytosis of >10,000 cells/ml; right
lower quadrant guarding and tenderness on physical examination; and
in certain cases, ultrasonography, computed tomography and
gynecological examination. Patients were included in the study if
they were aged ≥9 years and were part of a RCT that compared
antibiotic treatment with surgery in acute appendicitis. Patients
were excluded if they were <9 years old, pregnant, had a history
of drug abuse and/or psychiatric disorders and were not involved in
a RCTs.
Data extraction
Data were extracted independently by two reviewers
(Liu Zhihua and Qin Huanlong) and cross-checked to reach a
consensus. The following variables were recorded: Author, journal,
date of publication, geographical region, number of patients, age,
gender, body temperature, white blood cell count on admission,
C-reactive protein, time of hospital stay, complications and time
to work. If necessary, the primary authors were contacted to
retrieve further information.
Statistical analysis
Dichotomous variables were analyzed with odds ratios
(ORs) and a fixed-effects model was used according to
heterogeneity. Continuous variables, when the mean and SD were
presented, were assessed using the weighted mean difference (WMD)
and a random-effects model was used according to heterogeneity if
significant heterogeneity was present. Sensitivity analysis was
applied by removing individual studies from the data set and
analyzing the effects on the overall results to identify sources of
significant heterogeneity (17).
Data analyses were performed using Review Manager version 4.2
software (Nordic Cochrane Centre, Copenhagen, Denmark). P<0.05
was considered to indicate a statistically significant
difference.
Assessment of study quality
Included trials were reviewed and appraised for
methodological quality using the Jadad composite scale (17). High-quality trials scored >2 out
of a maximum possible score of 5 (18).
Results
Description of studies
Of the 983 patients in the five RCTs (19–23),
391 patients were allocated to the antibiotic group, while 592
patients comprised the appendicectomy group. The therapeutic
effects of each treatment were evaluated. Patient characteristics
and evaluation index are shown in Tables I and II, respectively.
 | Table IPatient characteristics comparing
antibiotic treatment with appendicectomy in acute appendicitis. |
Table I
Patient characteristics comparing
antibiotic treatment with appendicectomy in acute appendicitis.
| Antibiotic
treatment/Appendicectomy |
|---|
|
|
|---|
| Characteristics | Gibeily GJ (14) | Hansson J (15) | Styrud J (16) | Turhan AN (17) | Eriksson S (18) |
|---|
| Patients, n | 17/15 | 119/250 | 128/124 | 107/183 | 20/20 |
| Age, years | 38.3 | 37/34 | NR | NR | 27.8/35.0 |
| Males, n | 40.95/8 | 62/138 | 128/124 | 65/125 | 14/13 |
| Females, n | 12/7 | 57/112 | 0/0 | 42/58 | 6/7 |
| Body temperature,
°C | NR | 37.5/37.5 | 37.5/37.4 | NR | 37.2/37.1 |
| WBC,
k/mm3 | 12.1/14.3 | 12.2/13.5 | 12.5/12.4 | NR | 13.8/13.9 |
| C-reactive protein,
mg/l | NR | 56/54 | 55/54 | NR | 41/40 |
| Table IIEvaluation index comparing antibiotic
treatment with appendicectomy in acute appendicitis. |
Table II
Evaluation index comparing antibiotic
treatment with appendicectomy in acute appendicitis.
| Antibiotic
treatment/Appendicectomy |
|---|
|
|
|---|
| Index | Gibeily GJ
(14) | Hansson J (15) | Styrud J (16) | Turhan AN (17) | Eriksson S
(18) |
|---|
| Patients, n | 17/15 | 119/250 | 128/124 | 107/183 | 20/20 |
| Hospital stay,
daysa |
8.6±1.7/7.8±0.9 | 2+0.1/3+0.2 |
3.0±1.4/2.6±1.2 |
3.14±0.1/2.4±0.14 |
3.1±0.1/3.4±1.9 |
| Complications,
n | 4/5 | 36/80 | 15/17 | NR | 0/1 |
| Time to work,
daysa |
16.8±3.5/42±9.1 | NR |
8.0±80/10.1±7.6 | NR | NR |
Methodological quality
The mean Jadad score of the included studies was 3
out of a maximum possible score of 5 (Table III). The main study limitation
was associated with the limited sample numbers in three of the
studies. However, the sample size of the meta-analysis included 983
patients. Therefore, the limitation may not have an important
effect.
| Table IIIJadad scores. |
Table III
Jadad scores.
| Antibiotic
treatment/Appendicectomy |
|---|
|
|
|---|
| Methodological
qualities | Gibeily GJ
(14) | Hansson J (15) | Styrud J (16) | Turhan AN (17) | Eriksson S
(18) |
|---|
| Was the study
described as randomized? | 1 | 1 | 1 | 1 | 1 |
| Was the method used
to generate the sequence of randomization described and
appropriate? | 0 | 1 | 0 | 0 | 1 |
| Was the study
described as double-blind? | 0 | 1 | 0 | 0 | 1 |
| Was the method of
double-blinding described and appropriate? | 0 | 1 | 0 | 0 | 1 |
| Was there a
description of withdrawals and dropouts? | 1 | 1 | 1 | 1 | 1 |
| Total | 2 | 5 | 2 | 2 | 5 |
Outcome of comparison
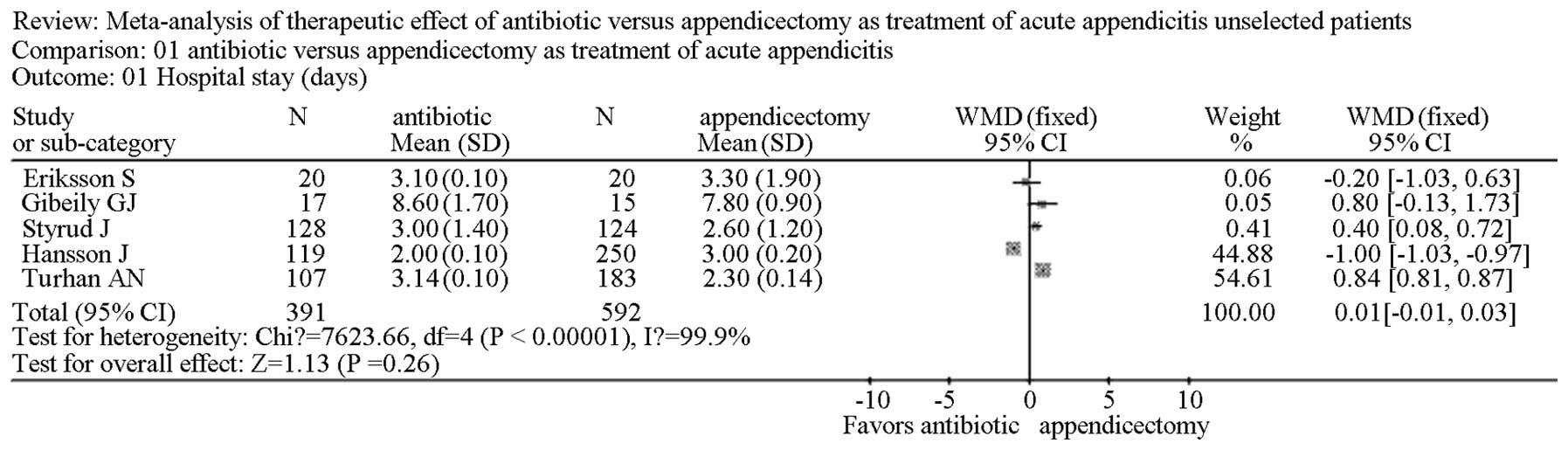
Meta-analysis revealed that the time of hospital
stay (days) in the five studies (19–23)
was not significantly different in the antibiotic group when
compared with the appendicectomy group. In addition, there was no
evidence of significant heterogeneity [WMD, 0.01; 95% confidence
interval (CI), −0.01–0.03; P=0.26; Fig. 2].
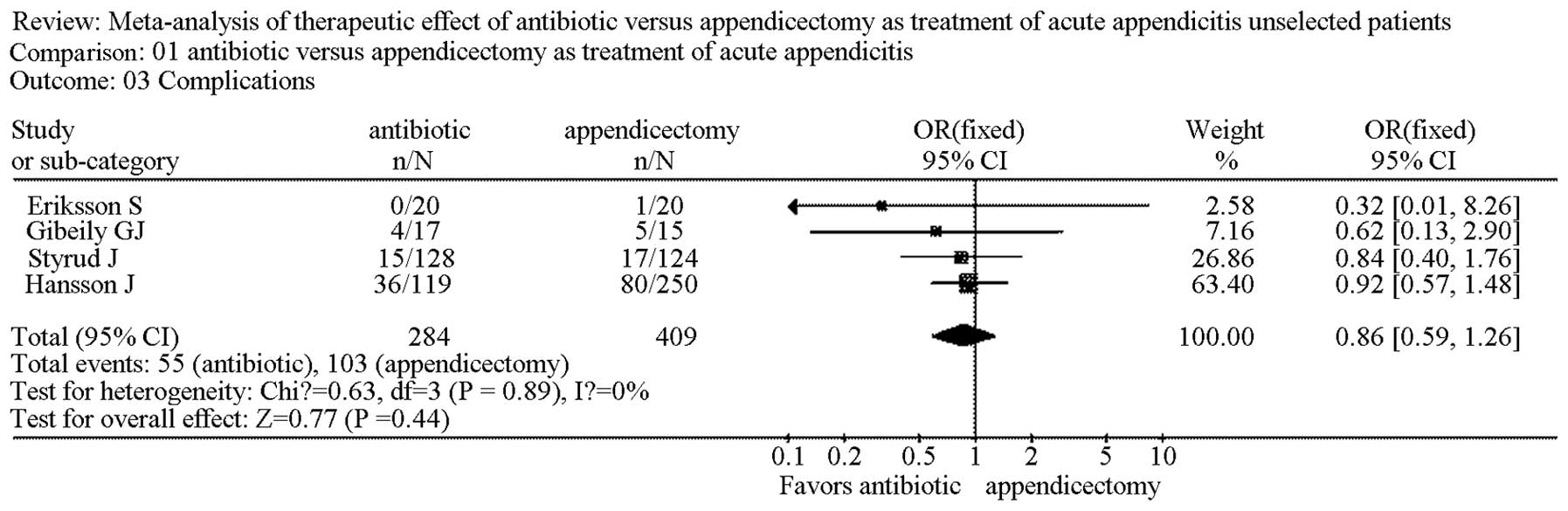
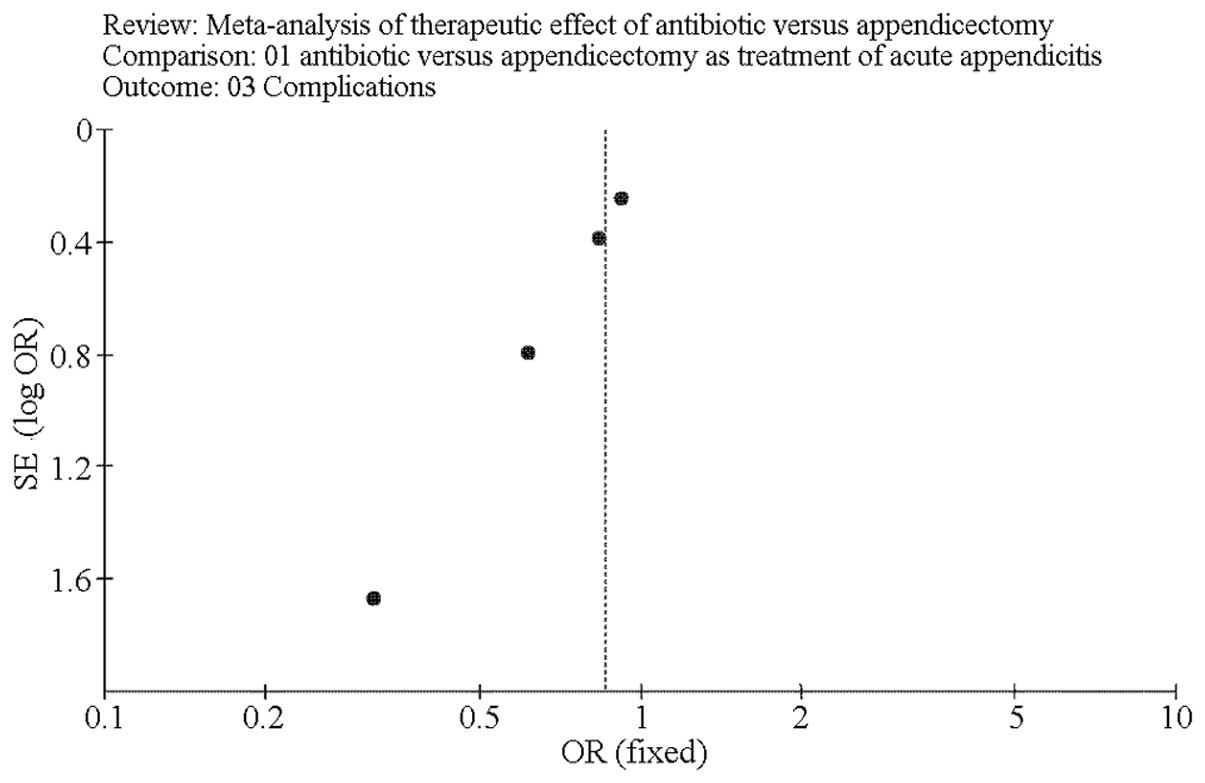
Complications
Four studies reported complications of the two
treatments (19–21,23).
Meta-analysis revealed that the complications observed were not
significantly different between the antibiotic and the
appendicectomy groups (OR, 0.86; 95% CI, 0.59–1.26; P=0.50). In
addition, there was no significant heterogeneity (Fig. 3).
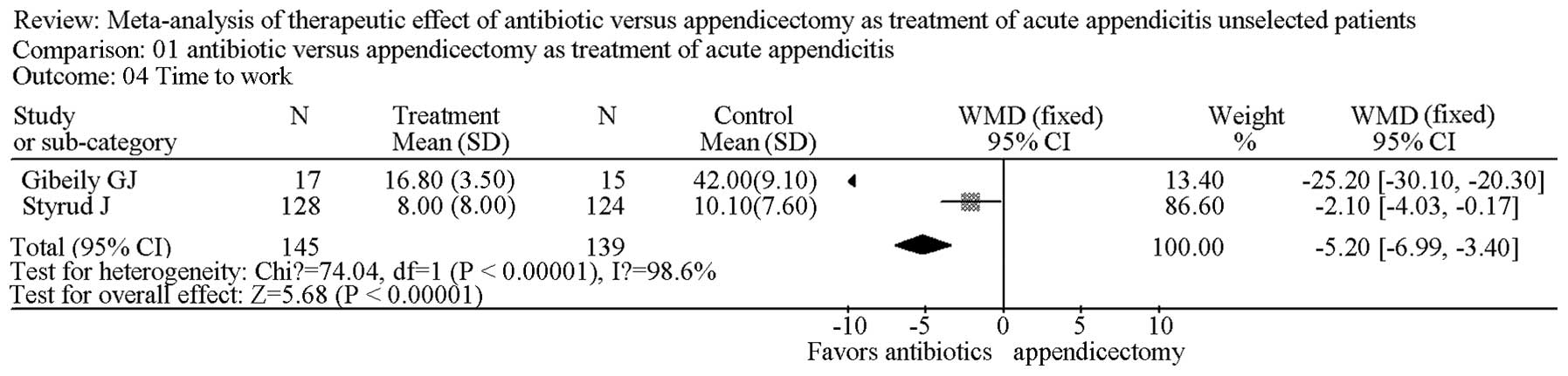
Time (days) to work
Two studies reported the time (days) to work
(19,25). The results demonstrated that time
to work was significantly longer in the appendicectomy group when
compared with the antibiotic group (WMD, −5.20; 95% CI,
−6.99--3.40; P<0.00001). There was no significant heterogeneity
(Fig. 4).
Sensitivity analysis
Removing individual studies from the data set did
not substantially change the OR and WMD values or the level of
significance for the three most important clinical outcomes (time
of hospital stay, time to work and complications).
Testing for publication bias
A funnel plot of the outcome of complications
following treatment with antibiotics and appendicectomy in the
included studies demonstrated symmetry, indicating there was no
serious publication bias (Fig.
5).
Discussion
Acute appendicitis is the most common
intra-abdominal condition requiring emergency surgery (24,25).
Appendicectomy has been regarded as the gold standard for acute
appendicitis for more than a century. However, conservative
treatment has been increasingly studied in selected patients during
recent years. In addition, the increasing diagnostic accuracy of
acute appendicitis has contributed to the use of antibiotic therapy
(26–28).
The present meta-analysis evaluated the therapeutic
effects of antibiotics and appendicectomy for the treatment of
acute appendicitis. The meta-analysis results indicated that there
was no significant difference between the antibiotic and
appendicectomy groups with regard to the time of hospital stay and
complications. However, time to work was significantly longer in
the appendicectomy group when compared with the antibiotic
group.
The time of hospital stay was not significantly
different between the antibiotic and appendicectomy groups.
Conservative therapy has delayed effects on appendicitis compared
with that of appendicectomy (29).
Therefore, patients must wait for the alleviation of symptoms in
hospital. However, following parenteral administration of
antibiotics for only 24 h, patients with appendicitis were
discharged with oral antibiotics and had a follow-up examination 1
week after discharge, shortening the time of hospital stay
(30). Therefore, the present
study found that there was no significant differences between the
two groups in terms of hospital stay.
There was no significant difference between the
antibiotic and appendicectomy groups in terms of complications.
However, major complications, including small bowel obstruction,
wound rupture and postoperative cardiac problems, were mainly
observed in the appendicectomy group, while minor complications,
including diarrhea and fungal infection, existed primarily in the
antibiotic group (31,32). Therefore, antibiotic therapy is
advantageous compared with appendicectomy for the treatment of
acute appendicitis (33).
Time to work may be the main advantage of antibiotic
treatment for acute appendicitis. Results revealed that time to
work was significantly longer in the appendicectomy group when
compared with the antibiotic group. This may be due to the longer
recovery time required following surgery before patients were able
to work (34).
There are additional advantages of antibiotic
treatment versus surgery, one of which may be the overall medical
cost (35). In addition,
antibiotic treatment may avoid surgical complications, including
small bowel obstruction and negative appendicectomy (36). Additionally, the rate of mortality
is low compared with appendicectomy (37). Antibiotic treatment is also
recommended in patients with a high surgical risk, particularly
elderly patients with poor heart and lung function or severely
obese patients, which may be a contraindication for surgery
(21,38).
However, disadvantages of antibiotic treatment also
exist. Allergy to the therapeutic agents may withhold the
application of antibiotic treatment (39). However, this problem may be avoided
relatively easily if surgeons pay increased attention to the
possibility of allergies and prescribe antibiotics suitable for
different patients (40).
Due to the large number of patients, antibiotic
abuse may also be a problem, which may enhance multiple drug
resistance in bacterial strains against various antibiotics
(41). However, it can be resolved
by using antibiotics according to the results of bacterial culture,
appropriately. Furthermore, comprehensive medical history and
physical examination are necessary and the definite diagnosis may
also be confirmed by imaging examination (42).
It is ineffective to analyze trials that differ in
terms of underlying conditions and intervention in a meta-analysis
(43). Conditions and
interventions were similar in the present meta-analysis in order to
increase clinical homogeneity between the trials. However, one
study discriminated the patient groups as intention-to-treat and
per protocol (20) and clinical
variables were not mentioned. In addition, one study classified the
complications as major or minor (20).
The number of patients is relatively small in
numerous RCTs. In the present meta-analysis, a relatively large
number of patients were included to enhance the reliability of the
results. As previously mentioned, of the 983 patients in the five
RCTs, 391 were allocated to the antibiotic group, while 592
comprised the appendicectomy group and the therapeutic effects of
the two treatments were evaluated.
In the present study, randomization, allocation
concealment and blinding assessment of outcomes were rarely
performed, as only two studies were reported as double-blinded
tests, due to ethical concern or practical difficulty (20,23).
However, this may be superior to a number of other studies, which
had rare allocation concealment and blinding assessment (17). Theoretically, the absence of
allocation concealment and double-blinding may have resulted in
overvaluing the effects of antibiotic treatment on specific
measures of postoperative recovery and other associated indexes
(44). However, Bruix et al
reported that individual quality measures, including blinding and
allocation concealment, are not reliably associated with the
strength of treatment effects in meta-analyses of RCTs (45).
In conclusion, the present meta-analysis indicated
that acute appendicitis may be treated successfully with
antibiotics. In addition, the therapeutic effects of antibiotics
and appendicectomy were comparable for the treatment of acute
appendicitis. Therefore, we recommend that more individuals are
considered for antibiotic therapy instead of surgery.
Acknowledgements
This study was supported by a grant from the
National Natural Science Foundation of China (no. 81070293).
References
|
1
|
Humes DJ and Simpson J: Acute
appendicitis. BMJ. 333:530–534. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Howie JG: Acute appendicitis: acute
appendicitis or acute appendicectomy? BMJ. 333:6532006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fitz RH: Perforating inflammation of the
vermiform appendix: with special reference to its early diagnosis
and treatment. Am J Med Sci. 92:321–346. 1886.
|
|
4
|
Andersson RE and Petzold MG: Nonsurgical
treatment of appendiceal abscess or phlegmon: a systematic review
and meta-analysis. Ann Surg. 246:741–748. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Choudhary RK and Hassn AM: Managing acute
appendicitis. Neuroimmune appendicitis may be distinct pathological
entity. BMJ. 326:492003.PubMed/NCBI
|
|
6
|
Coldrey E: Five years of conservative
treatment of acute appendicitis. J Int Coll Surg. 32:255–261.
1959.
|
|
7
|
No authors listed. Combined traditional
Chinese and Western medicine in acute appendicitis. Chin Med J
(Engl). 3:266–269. 1977.
|
|
8
|
Varadhan KK, Humes DJ, Neal KR and Lobo
DN: Antibiotic therapy versus appendectomy for acute appendicitis:
a meta-analysis. World J Surg. 34:199–209. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Vons C: Can acute appendicitis be treated
by antibiotics and in what conditions? J Chir (Paris). 146:17–21.
2009.(In French).
|
|
10
|
Liu K, Ahanchi S, Pisaneschi M, Lin I and
Walter R: Can acute appendicitis be treated by antibiotics alone?
Am Surg. 73:1161–1165. 2007.PubMed/NCBI
|
|
11
|
Levin T, Whyte C, Borzykowski R, Han B,
Blitman N and Harris B: Nonoperative management of perforated
appendicitis in children: can CT predict outcome? Pediatr Radiol.
37:251–255. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Aprahamian CJ, Barnhart DC, Bledsoe SE,
Vaid Y and Harmon CM: Failure in the nonoperative management of
pediatric ruptured appendicitis: predictors and consequences. J
Pediatr Surg. 42:934–938. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Abeş M, Petik B and Kazil S: Nonoperative
treatment of acute appendicitis in children. J Pediatr Surg.
42:1439–1442. 2007.
|
|
14
|
Dixon MR, Haukoos JS, Park IU, et al: An
assessment of the severity of recurrent appendicitis. Am J Surg.
186:718–722. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wilson DG, Bond AK, Ladwa N, Sajid MS,
Baig MK and Sains P: Intra-abdominal collections following
laparoscopic versus open appendicectomy: an experience of 516
consecutive cases at a district general hospital. Surg Endosc.
27:2351–2356. 2013. View Article : Google Scholar
|
|
16
|
Varadhan KK, Neal KR and Lobo DN: Safety
and efficacy of antibiotics compared with appendicectomy for
treatment of uncomplicated acute appendicitis: meta-analysis of
randomised controlled trials. BMJ. 344:e21562012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yang Z, Zheng Q and Wang Z: Meta-analysis
of the need for nasogastric or nasojejunal decompression after
gastrectomy for gastric cancer. Br J Surg. 95:809–816. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Moher D, Pham B, Jones A, et al: Does
quality of reports of randomised trials affect estimates of
intervention efficacy reported in meta-analyses? Lancet.
352:609–613. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gibeily GJ, Ross MN, Manning DB, Wherry DC
and Kao TC: Late-presenting appendicitis: a laparoscopic approach
to a complicated problem. Surg Endosc. 17:725–729. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hansson J, Körner U, Khorram-Manesh A,
Solberg A and Lundholm K: Randomized clinical trial of antibiotic
therapy versus appendicectomy as primary treatment of acute
appendicitis in unselected patients. Br J Surg. 96:473–481. 2009.
View Article : Google Scholar
|
|
21
|
Styrud J, Eriksson S, Nilsson I, et al:
Appendectomy versus antibiotic treatment in acute appendicitis. A
prospective multicenter randomized controlled trial. World J Surg.
30:1033–1037. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Turhan AN, Kapan S, Kütükçü E, Yiğitbaş H,
Hatipoğlu S and Aygün E: Comparison of operative and non operative
management of acute appendicitis. Ulus Travma Acil Cerrahi Derg.
15:459–462. 2009.PubMed/NCBI
|
|
23
|
Eriksson S and Granström L: Randomized
controlled trial of appendicectomy versus antibiotic therapy for
acute appendicitis. Br J Surg. 82:166–169. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gutt CN, Müller-Stich BP and Reiter MA:
Success and complication parameters for laparoscopic surgery: a
benchmark for natural orifice transluminal endoscopic surgery.
Endoscopy. 41:36–41. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Boni L, Dionigi G, Rovera F and Di
Giuseppe M: Laparoscopic left liver sectoriectomy of Caroli’s
disease limited to segment II and III. J Vis Exp.
24:11182009.PubMed/NCBI
|
|
26
|
Binnebösel M, Otto J, Stumpf M, et al:
Acute appendicitis. Modern diagnostics - surgical ultrasound.
Chirurg. 80:579–587. 2009.(In German).
|
|
27
|
Cavuşoğlu YH, Erdoğan D, Karaman A, Aslan
MK, Karaman I and Tütün OC: Do not rush into operating and just
observe actively if you are not sure about the diagnosis of
appendicitis. Pediatr Surg Int. 25:277–282. 2009.PubMed/NCBI
|
|
28
|
Tzanakis NE, Efstathiou SP, Danulidis K,
et al: A new approach to accurate diagnosis of acute appendicitis.
World J Surg. 29:1151–1156. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Christiansen SE, Jakobsen BW, Lund B and
Lind M: Isolated repair of the medial patellofemoral ligament in
primary dislocation of the patella: a prospective randomized study.
Arthroscopy. 24:881–887. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Malik AA and Bari SU: Conservative
management of acute appendicitis. J Gastrointest Surg. 13:966–970.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lemieux P, Rheaume P, Levesque I, Bujold E
and Brochu G: Laparoscopic appendectomy in pregnant patients: a
review of 45 cases. Surg Endosc. 23:1701–1705. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kamiński J, Zielińska-Leś I and Kozielski
J: Invasive pulmonary aspergillosis as a complication of prolonged
antibiotic therapy. Pol Merkur Lekarski. 18:700–702. 2005.(In
Polish).
|
|
33
|
Matthaiou DK, Peppas G and Falagas ME:
Meta-analysis on surgical infections. Infect Dis Clin North Am.
23:405–430. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wei HB, Huang JL, Zheng ZH, et al:
Laparoscopic versus open appendectomy: a prospective randomized
comparison. Surg Endosc. 24:266–269. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Edelsberg J, Berger A, Schell S, Mallick
R, Kuznik A and Oster G: Economic consequences of failure of
initial antibiotic therapy in hospitalized adults with complicated
intra-abdominal infections. Surg Infect (Larchmt). 9:335–347. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Partelli S, Beg S, Brown J, Vyas S and
Kocher HM: Alteration in emergency theatre prioritisation does not
alter outcome for acute appendicitis: comparative cohort study.
World J Emerg Surg. 4:222009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wong SL, Anthony EY and Shetty AK:
Pyomyositis due to Streptococcus pneumoniae. Am J Emerg Med.
27:6332009.
|
|
38
|
Barbour A, Schmidt S, Rout WR, Ben-David
K, Burkhardt O and Derendorf H: Soft tissue penetration of
cefuroxime determined by clinical microdialysis in morbidly obese
patients undergoing abdominal surgery. Int J Antimicrob Agents.
34:231–235. 2009. View Article : Google Scholar
|
|
39
|
Carson HJ and Cook BA: Mast cell tryptase
in a case of anaphylaxis due to repeat antibiotic exposure. Leg Med
(Tokyo). 11:234–236. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
La Shell MS and Tankersley MS: Antibiotics
for the allergist: part 2. Ann Allergy Asthma Immunol. 102:1–7.
2009.PubMed/NCBI
|
|
41
|
Hellmark B, Unemo M,
Nilsdotter-Augustinsson A and Söderquist B: Antibiotic
susceptibility among Staphylococcus epidermidis isolated
from prosthetic joint infections with special focus on rifampicin
and variability of the rpoB gene. Clin Microbiol Infect.
15:238–244. 2009.
|
|
42
|
Metzger R, Bonatti H and Sawyer R: Future
trends in the treatment of serious Gram-positive infections. Drugs
Today (Barc). 45:33–45. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Hogle NJ, Chang L, Strong VE, et al:
Validation of laparoscopic surgical skills training outside the
operating room: a long road. Surg Endosc. 23:1476–1482. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Suenaga M, Sugiura H, Kokuba Y, Uehara S
and Kurumiya T: Repeated hepatic resection for recurrent
hepatocellular carcinoma in eighteen cases. Surgery. 115:452–457.
1994.PubMed/NCBI
|
|
45
|
Bruix J, Sherman M, Llovet JM, et al:
Clinical management of hepatocellular carcinoma. Conclusions of the
Barcelona-2000 EASL conference European Association for the Study
of the Liver. J Hepatol. 35:421–430. 2001. View Article : Google Scholar : PubMed/NCBI
|