Introduction
Pulmonary alveolar proteinosis (PAP) is a rare
diffuse pulmonary disease initially described by Rosen et al
in 1958 (1). The clinical features
of PAP include the accumulation of periodic acid-Schiff
(PAS)-positive lipoproteinaceous material, predominantly
phospholipid surfactants and surfactant apoproteins, in the distal
air spaces, resulting in impaired gas transfer.
Patients with PAP may suffer from progressive
dyspnea and cough, which may be accompanied by exacerbated hypoxia.
Its course is variable, ranging from progressive deterioration to
spontaneous improvement (2).
Radiographic analysis of the disease revealed ground-glass
opacities with multiple bilateral, irregular and dense
inhomogeneous lesions, which have a ‘crazy-paving’ pattern on
computed tomography (CT) scans (2). Confirmation of diagnosis of PAP is
achieved through using typical electron-microscopic findings in
sputum, lung washings and lung biopsy specimens, without which the
condition is frequently mistaken for interstitial lung disease,
particularly sarcoidosis.
For the treatment of PAP, various different
therapies have been utilized over the years, for example, postural
drainage, antibiotics and intermittent positive pressure breathing
(3). Major advances were achieved
in the late 90s by Kitamura et al (4) and Tanaka et al (5), who identified the presence of
autoantibodies neutralizing granulocyte-macrophage
colony-stimulating factor (GM-CSF) in the serum and lung tissue of
patients with idiopathic PAP, and since then various specific
treatments have been attempted or proposed (6). However, despite this, the standard
treatment remains whole lung lavage (WLL), which was modified
following the original description by Ramirez et al
(7) in 1963.
In the present study, 11 patients with PAP who were
treated with WLL were followed up, and their clinical
manifestations, treatment outcomes and prognosis were reviewed.
Patients and methods
Patients and study design
The present study was conducted at the Wuxi People’s
Hospital Affiliated to Nanjing Medical University (Wuxi, Jiangsu,
China) for the diagnosis and therapy of PAP in China. Patients
diagnosed with PAP, who had hypoxia or worsening disease, were
recruited between 2003 and 2011 from the Department of Respiratory
Medicine. Patient history, physical examinations and other data
were collected at the time of diagnosis, when possible.
Results from the bronchoalveolar lavage (BAL),
characteristic high resolution-CT (HR-CT) and/or histopathological
observations from biopsies were used as the basis for diagnosis. In
the present study, transbronchial lung biopsy was used to diagnose
3 patients. PAP was also diagnosed using surgical lung biopsy (4
patients) and BAL (3 patients). Additionally, 1 patient was
diagnosed using BAL at the Zhongshan Hospital of Fudan University
(Shanghai, China).
Disease severity score (DSS)
A PAP DSS was assigned to each patient. This score
was based on the presence of symptoms, including dyspnea or cough,
and the grade reduction of PaO2, as previously described
(8,9).
Pulmonary function tests and arterial
blood gas analysis
Measurements were obtained from each patient,
including the maximum vital capacity (VCmax), forced expiratory
volume in 1 second (FEV1), forced vital capacity (FVC) and
diffusing capacity for carbon monoxide (DLCO). Arterial blood gas
was also analyzed. To measure the pulmonary function, the Jaeger
MS-PFT and MS-Diffusion spirometer (Jaeger, Hoechberg, Germany)
were used, and all the processes were handled by the same
technician. The pulmonary function tests were performed when the
patient was admitted to hospital and two weeks after WLL. The
arterial blood gas analysis was conducted by the clinical
laboratory with a GEM Premier 3000 blood gas analyzer (Beckman
Coulter, Miami, FL, USA) prior to and following WLL. The blood was
obtained from the radial artery at room temperature.
WLL
In order to determine whether WLL is required,
universal indicators were used, which include severe dyspnea and/or
hypoxemia and a PaO2 level of <60 mmHg. The risks
associated with WLL include those specifically associated with
general anesthesia, double-lumen endotracheal intubation and
mechanical ventilation necessary for the procedure. Additionally,
there are risks associated with the lavage itself, as well as the
requirement for continued ventilatory support post-procedure and
monitoring in a critical care setting. Electrocardiogram as well as
tests of coagulation, liver and kidney functions were performed
prior to the procedure, which was then performed in the operating
room.
Therapeutic alveolar lavage of either the right or
left lung was performed under general anesthesia and paralysis.
Cardiopulmonary monitoring was performed to ensure that the process
was smooth and that no complications occurred. The patient was
intubated with a double-lumen endobronchial tube and a flexible
bronchoscopy was performed simultaneously to confirm the
appropriate tube placement. The bronchial and tracheal balloons
were inflated to isolate the lungs and intermittent positive
pressure ventilation was initiated with a volume of 400 ml at a
rate of 13 breaths/min. While WLL was performed in one lung, the
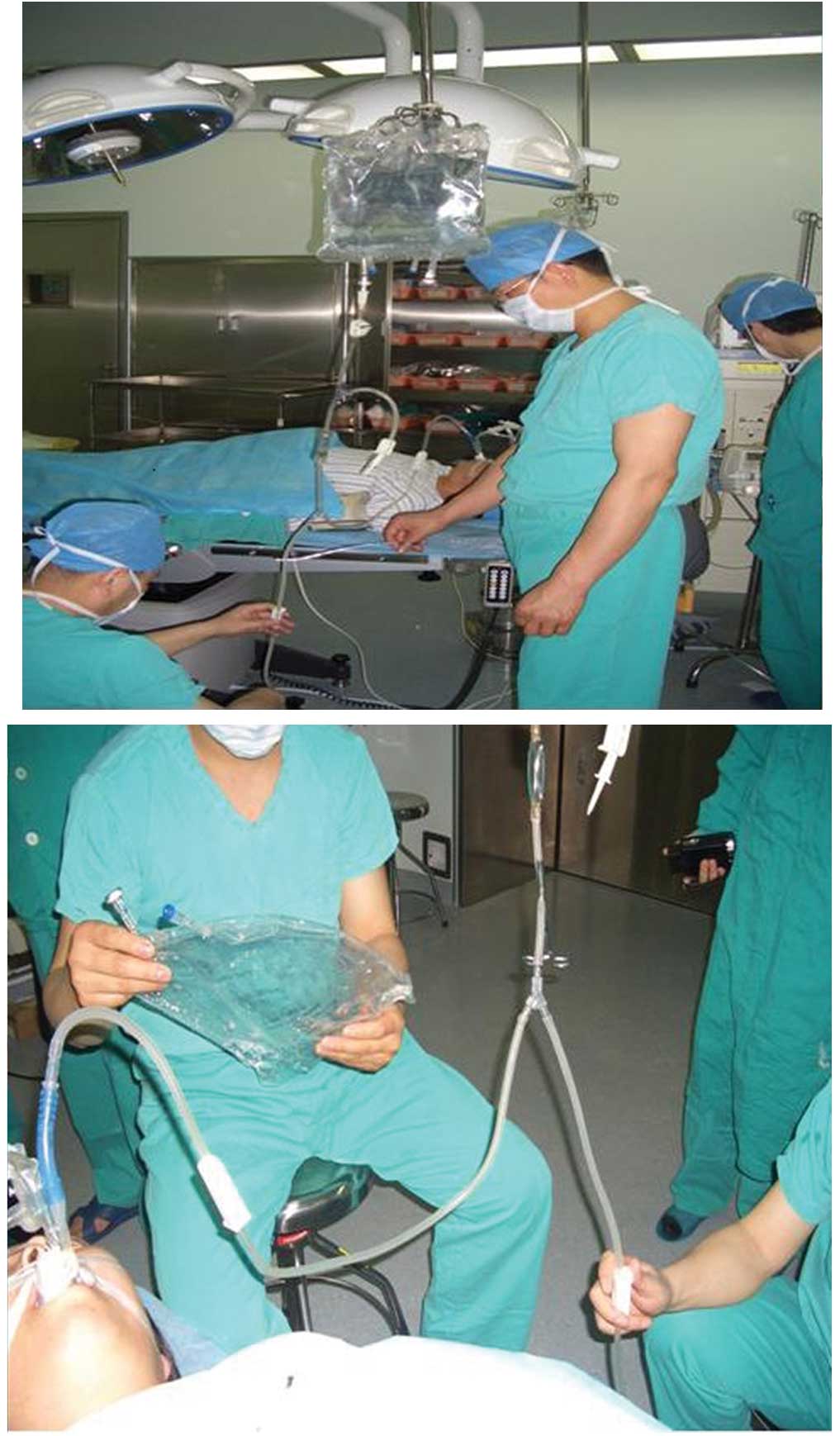
other was ventilated. The WLL procedure is demonstrated in Fig. 1.
The patients were placed on an operating table in
the lateral decubitus position, with the lung being lavaged in the
nondependent position (up) in order to reduce the perfusion of the
treated lung (thus providing an improved ventilation/perfusion
ratio). Sterile 0.9% NaCl warmed to body temperature was used as
lavage fluid. Prior to the lavage procedure, ~200 ml saline was
instilled to fill the lung up to the functional residual capacity.
Subsequent to this, aliquots between 500 and 600 ml saline were
instilled to the lung. Saline bags were placed ~60 cm above the
table surface, allowing the fluid to flow into the lungs by
gravity. Following each instillation, the fluid was drained
passively by positioning the operation table, with the addition of
concomitant chest percussion. The recovered fluid was collected via
a 2-way stopcock into 500 ml bottles to allow turbidity to be
assessed. The procedure was repeated until the effluent, which was
initially opaque and milky, became clear (Fig. 2). A total of ~6,000–26,000 ml of
warm saline was poured into the lung. The residual saline solution
was then aspirated as far as possible.
Following pallanesthesia, the patient was extubated
and transferred to the hospital ward. The lavage of the other lung
was performed following an interval of 4–10 days.
Ethical considerations
The present study was approved by the Ethics Review
Committee of Wuxi People’s Hospital and Nanjing Medical University.
Informed consent was obtained from all participants following a
detailed description of the purpose and potential benefits of the
study.
Statistical analysis
All statistical analyses were performed using SPSS
statistical software version 19.0 (SPSS, Inc., Chicago, IL, USA).
The paired t-test was used to compare the differences between
continuous variables prior to and following WLL, whilst the
Wilcoxon T test was employed to compare the categorical variables.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Demographics
The age at diagnosis ranged between 31 and 66 years,
with a mean age of 48.3 years. A male predominance (eight males
versus three females) was observed in the present study. Detailed
demographics of the study population are illustrated in Table I.
 | Table IDemographics and disease features at
diagnosis. |
Table I
Demographics and disease features at
diagnosis.
| Characteristic | Value |
|---|
| Gender, n (%) |
| Male | 8 (72.7) |
| Female | 3 (27.3) |
| Age, years (mean ±
SD) | 48.3±10.8 |
| PAP type, n (%) |
| Primary | 11 (100.0) |
| Secondary | 0 (0.0) |
| Smoking habits, n
(%) |
| Never | 3 (27.3) |
| Previous | 2 (18.2) |
| Current | 6 (54.5) |
| Radiographic PAP
features, n (%) |
| Characteristic | 11 (100.0) |
| Non
characteristic | 0 (0.0) |
| DSS grade, n (%) |
| 1 | 0 (0.0) |
| 2 | 1 (9.1) |
| 3 | 1 (9.1) |
| 4 | 5 (45.5) |
| 5 | 4 (36.4) |
Diagnostic methods
PAP was diagnosed using either surgical lung biopsy
(4 patients) or BAL (3 patients) at the Wuxi People’s Hospital
Affiliated to Nanjing Medical University. One patient was diagnosed
using BAL at the Zhongshan Hospital of Fudan University. The
remaining patients were assessed using HR-CT scans to observe
characteristic ‘crazy-paving’.
Smoking habits
In total, 8 out of 11 patients (72.7%) were current
or ex-smokers (75% current, 25% previous; Table I). All the females had never smoked
before. All active smokers at the time of diagnosis reported a
heavy consumption of >20 cigarettes/day.
Symptoms and DSS
Among the symptoms reported at the time of
diagnosis, the majority of PAP patients complained about dyspnea
(90%), followed by cough (27.3%) and sputum (27.3%). Physical
examination revealed acropachy in one case. The distribution of the
patients according to DSS grades is shown in Table I. The majority of patients had DSS
scores of 4 and 5.
Analysis of disease course and WLL
The follow-up time ranged between two and eight
years. Following WLL, all patients showed an improvement in
respiratory symptoms and the survival rate was 100%. The majority
of patients received WLL once, however, one patient underwent WLL
three times between 2003 and 2009 and another patient underwent WLL
twice within two years. In all patients, no severe adverse effects
occurred during and subsequent to WLL.
The levels of oxygen markedly improved following
therapeutic lavage. The mean PaO2 was 54.8±7.4 mmHg
prior to WLL, which increased to 68.0±8.5 mmHg following WLL. The
PaO2 following WLL showed moderate improvement
(P=0.010), while the D(A-a)O2 also improved following
WLL (P=0.028; Table II).
Pulmonary function tests were performed two weeks subsequent to WLL
for nine patients. All but one patient had a slight improvement in
DLCO (P=0.000; Table III). VCmax
improved in four cases and worsened in five cases. No significant
difference in the mean VCmax (% predicted) prior to and following
WLL was identified. The mean FVC (% predicted) and FEV1 (%
predicted) decreased following WLL, and no significant differences
were detected in FVC (% predicted) and FEV1 (% predicted) prior to
and following WLL (P=0.072; Table
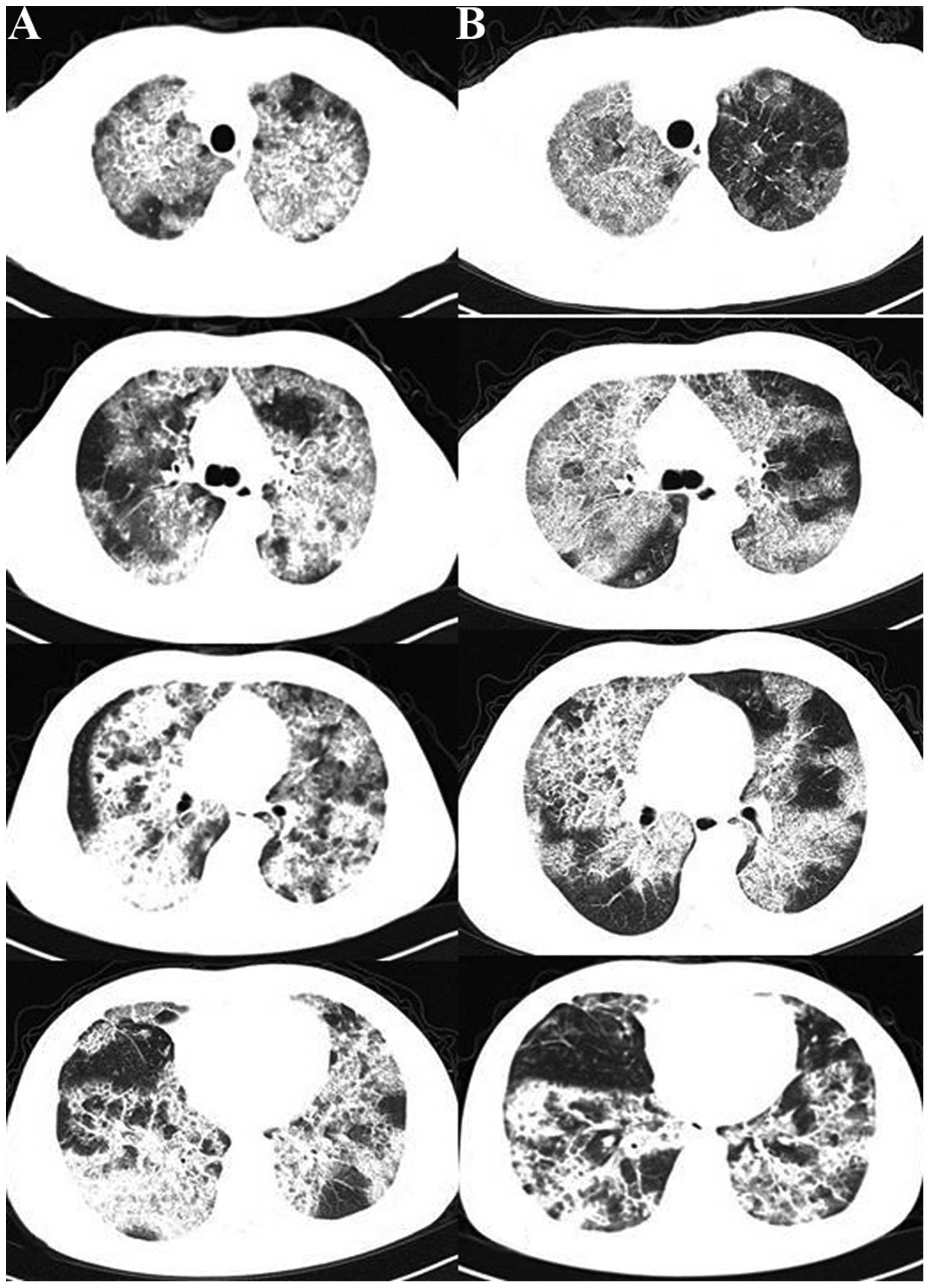
III). Chest radiographs revealed that all but one patient
showed a significant improvement following WLL. A representative CT
scan image is shown in Fig. 3.
| Table IIPre- and post-lavage arterial blood
gas analysis (mmHg). |
Table II
Pre- and post-lavage arterial blood
gas analysis (mmHg).
| Patient number | PaO2
(mmHg) | D(A-a) O2
(mmHg) |
|---|
|
|
|---|
| Pre-lavage | Post-lavage | Pre-lavage | Post-lavage |
|---|
| 1 |
| Lavage 1 | 54.8 | 78.0 | 53.1 | 12.3 |
| Lavage 2 | 63.2 | 60.2 | 31.8 | 39.2 |
| Lavage 3 | 53.0 | 60.0 (9 l/min) | 66.0 | 312.0 |
| 2 | 55.3 | 83.1 | 57.8 | 24.2 |
| 3 | 52.0 | - | 29.0 | - |
| 4 | 34.0 (2 l/min) | 47.0 | 133.0 | 71.0 |
| 5 |
| Lavage 1 | 56.0 (2 l/min) | - | 120.0 | - |
| Lavage 2 | 49.0 | 69.0 | 62.0 | 42.0 |
| 6 | 58.1 | 63.0 | 21.8 | 15.7 |
| 7 | 49.5 | 57.0 | 28.9 | 17.4 |
| 8 | 57.0 | 72.4 | 34.0 | 21.6 |
| 9 | 52.0 | 56.0 (2 l/min) | 52.0 | 124.0 |
| 10 | 41.0 | 67.0 | 30.0 | 16.8 |
| 11 | 65.0 | 62.7 | 45.0 | 48.5 |
| Table IIIPulmonary function tests pre- and
post-lavage |
Table III
Pulmonary function tests pre- and
post-lavage
| FEV1 (% Pred) | FVC (% Pred) | VCmax (% Pred) | DLCO (% Pred) |
|---|
|
|
|
|
|
|---|
| Patient | Pre-lavage | Post-lavage | Pre-lavage | Post-lavage | Pre-lavage | Post-lavage | Pre-lavage | Post-lavage |
|---|
| 1 |
| Lavage 1 | 86.4 | 88.2 | 82.1 | 83.1 | 78.8 | 80.2 | 49.4 | 60.6 |
| Lavage 2 | 93.5 | 93.2 | 79.3 | 78.6 | 76.1 | 76.2 | - | 57.8 |
| Lavage 3 | 85.6 | 86.4 | 78.2 | 80.5 | 76.0 | 77.9 | - | 61.4 |
| 2 | 98.6 | 97.6 | 90.0 | 89.7 | 86.9 | 83.7 | 49.5 | 54.2 |
| 3 | 104.6 | 91.7 | 74.1 | 75.2 | 99.4 | 87.9 | 64.2 | 67.9 |
| 4 | - | - | - | - | - | - | - | - |
| 5 |
| Lavage 1 | - | 57.4 | - | 54.8 | - | 60.7 | - | 34.2 |
| Lavage 2 | 69.0 | 70.2 | 61.3 | 60.7 | 62.0 | 61.9 | 30.8 | 32.4 |
| 6 | 101.0 | - | 96.2 | - | 109.5 | - | 69.6 | - |
| 7 | 46.0 | 43.8 | 40.3 | 43.8 | 38.6 | 40.3 | 23.8 | 27.4 |
| 8 | 88.1 | 76.6 | 73.7 | 69.2 | 72.1 | 67.3 | 55.5 | 59.1 |
| 9 | 106.3 | 94.6 | 92.6 | 87.5 | 22.9 | 31.7 | 62.4 | 59.5 |
| 10 | 69.8 | 67.3 | 68.6 | 66.4 | 69.3 | 57.4 | 46.6 | 56.3 |
| 11 | 68.0 | 68.4 | 69.9 | 70.2 | 67.0 | 67.2 | 29.5 | 32.4 |
Discussion
In the present study, the characteristics of a total
of 11 patients with PAP were described. The median age at diagnosis
in the present study was 48 years, which is higher than the mean
age observed in cohorts analyzed by Seymour et al (10), Xu et al (11), Bonella et al (12) and Campo et al (13), but lower than the cohort
investigated by Inoue et al (9). The male to female ratio was 2:7,
which was similar to the ratio observed by Seymour et al
(10). Furthermore, the present
study revealed that the majority of patients with PAP were smokers
(current or former), however, a significant portion of patients
with PAP had never smoked in other cohorts, ranging between 21 and
43% (9,12).
PAP is a rare diffuse pulmonary disease
characterized by the accumulation of PAS-positive lipoproteinaceous
material, predominantly phospholipid surfactants and surfactant
apoproteins, in the distal air spaces, resulting in impaired gas
transfer. PAP is frequently mistaken for interstitial lung disease.
The presence of macroscopic milky fluid and/or the presence of
amorphous, eosinophilic, PAS positive material, the presence of
lipid laden macrophages on BAL analysis as well as the appearance
of a ‘crazy paving pattern’ in the high resolution CT scan images
of the thorax, are all used as diagnostic tools. In the present
study, the diagnosis of PAP was confirmed by either surgical lung
biopsy (4 patients) or BAL (4 patients). Three patients were
assessed by typical ‘crazy paving’ in a HR-CT scan.
Among the symptoms presented at the time of
diagnosis, the majority of patients with PAP complained about
cough, sputum and dyspnea, which is consistent with the results
observed in Germany and Japan (9,12).
The DSS is a useful tool to assess disease severity, as previously
described by Inoue et al (8,9) and
Bonella et al (12). In the
present study, the majority of patients had a DSS of 4 and 5, which
indicated a worsened disease severity of PAP patients.
Given the recent insights into the pathogenesis of
the disorder and the role of GM-CSF in the pathophysiology of PAP
(14), novel targeted biological
therapies have been proposed and have been reported in previous
studies (15,16). In China, investigation into GM-CSF
therapy is ongoing.
The success rate for GM-CSF is not yet sufficient to
replace WLL therapy, despite increasing evidence suggesting that
GM-CSF therapy may be beneficial for patients with PAP (12). As mentioned above, WLL to date
represents the conventional therapeutic treatment for PAP (17–20).
There are no clearly established criteria for when
to perform WLL; all patients with PAP who had hypoxia or worsening
disease were recruited, and the majority of patients had DSSs of 4
and 5 in the present study.
In the present study, the WLL technique was
performed at Wuxi People’s Hospital Affiliated to Nanjing Medical
University under general anesthesia in an operating room. The
patient was intubated with a double lumen endotracheal tube and
fiber-optic bronchoscopy was performed to confirm the appropriate
tube placement. The patient was placed in the lateral decubitus
position and the lung was lavaged in the uppermost position, while
the non-lavaged lung was mechanically ventilated. The injection of
warmed (37°C) saline into the lung was performed and, following
opening the outflow tube, the fluid was collected. In order to
improve drainage, manual chest percussion, which significantly
augments the removal of proteinaceous material, may be performed.
Chest wall percussion was conducted once the outflow, which was
initially milky, became clear. Lavage and percussion continued
until the outflow fluid became definitively clear.
The efficacy of WLL in the present study was
evaluated by analyzing the patient symptoms, DSS, arterial blood
gas, pulmonary function tests and radiological findings. All
patients showed symptomatic, radiographic and functional
improvement following WLL. Subsequent to the therapeutic lavage,
oxygenation parameters, including PaO2 and
D(A-a)O2, markedly improved in comparison with the
initial examinations, which is consistent with results observed in
previous studies by Byun et al (21) and Bonella et al (12). The DSS distribution of the patients
also improved, with the majority of the patients having a DSS of 3.
Although the data from the present study revealed that the
diffusing capacity of the lung was improved but not the
ventilation, due to the small sample size, further studies are
required with a larger sample size over a longer time period to
confirm the present results. WLL can reduce the area of
high-density reflection on CT scans. All patients with PAP who
underwent WLL survived to the end of the present study. In
addition, in a long-term follow up of the 11 patients with PAP
(collected between 2003 and 2011), it was found that WLL was safe
and efficacious, providing long lasting benefits.
In conclusion, WLL improves the survival rate and is
an effective approach for the treatment of PAP, which may
significantly improve clinical symptoms, blood gas analysis and
radiographic features.
References
|
1
|
Rosen SH, Castleman B and Liebow AA:
Pulmonary alveolar proteinosis. N Engl J Med. 258:1123–1142. 1958.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Trapnell BC, Whitsett JA and Nakata K:
Pulmonary alverolar proteinosis. N Engl J Med. 349:2527–2539. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mazone P, Thomassen MJ and Kavuru M: Our
new understanding of pulmonary alveolar proteinosis: what an
internist needs to know. Cleve Clin J Med. 68:977–978. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kitamura T, Tanaka N, Watanabe J, et al:
Idiopathic pulmonary alveolar proteinosis as an autoimmune disease
with neutralizing antibody against granulocyte/macrophage
colony-stimulating factor. J Exp Med. 190:875–880. 1999. View Article : Google Scholar
|
|
5
|
Tanaka N, Watanabe J, Kitamura T, et al:
Lungs of patients with idiopathic pulmonary alveolar proteinosis
express a factor which neutralizes granulocyte-macrophage colony
stimulating factor. FEBS Lett. 442:246–250. 1999. View Article : Google Scholar
|
|
6
|
Luisetti M, Kadija Z, Mariani F, et al:
Therapy options in pulmonary alveolar proteinosis. Ther Adv Respir
Dis. 4:239–248. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ramirez J, Schultz RB and Dutton RE:
Pulmonary alveolar proteinosis: a new technique and rationale for
treatment. Arch Intern Med. 112:419–431. 1963. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Inoue Y, Trapnell BC, Tazawa R, et al:
Characteristics of a large cohort of patients with autoimmune
pulmonary alveolar ptoteinosis in Japan. Am J Respir Crit Care Med.
177:752–762. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Inoue Y, Nakata K, Arai T, et al:
Epidemiological and clinical features of idiopathic pulmonary
alveolar ptoteinosis in Japan. Respirology. 11:S55–S60. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Seymour JF, Presneill JJ, Schoch OD, et
al: Therapeutic efficacy of granulocyte macrophage
colony-stimulating factor in patients with idiopathic acquired
alveolar proteinosis. Am J Respir Crit Care Med. 163:524–531. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Xu Z, Jing J, Wang H, et al: Pulmonary
alveolar proteinosis in China: a systematic review of 241 cases.
Respirology. 14:761–766. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bonella F, Bauer PC, Griese M, et al:
Pulmonary alveolar proteinosis: new insights from a single-center
cohort of 70 patients. Respir Med. 105:1908–1916. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Campo I, Mariani F, Rodi G, et al:
Assessment and management of pulmonary alveolar proteinosis in a
reference center. Orphanet J Rare Dis. 8:402013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Uchida K, Nakata K, Trapnell BC, et al:
High-affinity autoantibodies specifically eliminate
granulocyte-macrophage colony-stimulating factor activity in the
lungs of patients with idiopathic pulmonary alveolar proteinosis.
Blood. 103:1089–1098. 2004. View Article : Google Scholar
|
|
15
|
Seymour JF, Dunn AR, Vincent JM, et al:
Efficacy of granulocyte-macrophage colony-stimulating factor in
acquired alveolar proteinosis. N Engl J Med. 335:1924–1925. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wang Y, Thomson CA, Allan LL, et al:
Characterization of pathogenic human monoclonal autoantibodies
against GM-CSF. Proc Natl Acad Sci USA. 110:7832–7837. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Seymour JF and Presneill JJ: Pulmonary
alveolar proteinosis: progress in the first 44 years. Am J Respir
Crit Care Med. 166:215–235. 2002.PubMed/NCBI
|
|
18
|
Huizar I and Kavuru MS: Alveolar
proteinosis syndrome: pathogenesis, diagnosis, and management. Curr
Opin Pulm Med. 15:491–498. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Campo I, Kadija Z, Mariani F, et al:
Pulmonary alveolar proteinosis: diagnostic and therapeutic
challenges. Multidiscip Respir Med. 7:42012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Beccaria M, Luisetti M, Rodi G, et al:
Long-term durable benefit after whole lung lavage in pulmonary
alveolar proteinosis. Eur Respir J. 23:526–531. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Byun MK, Kim DS, Kim YW, et al: Clinical
features and outcomes of idiopathic pulmonary alveolar ptoteinosis
in Korean population. J Korean Med Sci. 25:393–398. 2010.
View Article : Google Scholar : PubMed/NCBI
|