Introduction
Tuberculous bronchitis is a submucosal tuberculosis
mainly found in bronchial mucosa and submucosa (1,2).
Tuberculous bronchitis has also been diagnosed in smooth muscle,
cartilage and outer membranes; thus it is termed tracheobronchial
tuberculosis (TBTB) (3). TBTB may
be misdiagnosed as bronchitis, asthma, bronchiectasis or lung
cancer (4,5). TBTB is present in 10%-40% of patients
with active pulmonary tuberculosis (6) and the incidence of TBTB has been
increasing in recent years (7).
TBTB is more common in young adults than older ones, and females
are more readily infected than males (8). The onset of TBTB may be concealed and
its clinical manifestations are not specific, which makes the
diagnosis of TBTB difficult. Clinically (9), TBTB patients may have systematic
respiratory symptoms such as severe cough, sputum, wheezing,
hemoptysis and paroxysmal dyspnea. In TBTB patients with stenosis
in the trachea, left and right main bronchus, and middle segment of
bronchus, the cough sounds like barking. In certain patients, these
symptoms may also be accompanied by systematic symptoms (such as
fever, night sweats, anorexia, fatigue, weight loss and irregular
menstruation) and allergic manifestations (such as allergic
arthritis and conjunctivitis).
In the present study, a retrospective analysis of
410 patients with TBTB was performed in order to investigate the
characteristics and risk factors associated with TBTB. The patients
selected for the present study were enrolled at Shandong Chest
Hospital (Jinan, China) between January and December 2012.
Materials and methods
Patients
The present study was approved by the Ethics
Committee of Shandong University (Jinan, China). All patients
provided written informed consent. None of the patients were
long-term users of hormones for the treatment of autoimmune
diseases, including cancer, AIDS, diabetes, systemic lupus
erythematosus and organ transplantation.
Diagnosis
All patients underwent sputum acid-fast bacilli
examination (three smears and one culture using the BACTEC method),
electronic bronchoscopy and a chest X-ray or computed tomography
(CT) scan. According to previously described criteria (3), the 410 patients met the following
criteria: i) typical lesions of TBTB identified by bronchoscopy and
ii) a positive sputum smear for acid-fast bacilli and/or a positive
sputum culture for Mycobacterium tuberculosis; or bronchial
brushing or bronchoalveolar lavage samples positive for acid-fast
bacilli; or tuberculous pathological changes identified using
bronchoscopic biopsy.
Treatment
Among the 410 patients with TBTB, 382 patients were
newly diagnosed. The remaining 28 cases were patients who required
retreatment. The registered patients adopted the 3HRZE/6HRE program
(H, isoniazid; R, rifampicin; Z, pyrazinamide; E, ethambutol). The
28 patients requiring retreatment received the 3HRZEL/6HREL program
supplemented with 0.2 g isoniazid inhalation therapy. The 410
patients were treated with endobronchial injection, clamping,
balloon dilatation, refrigeration and other treatments. The
patients with severe airway obstruction were administered
bronchoscopic therapy under general anesthesia 2–15 times. The
patients were followed up for between 3 and 9 months using
bronchoscopy.
Bronchoscopy and TBTB typing
The diagnosis of TBTB was performed using
bronchoscopy and bacteriological or pathological analysis results.
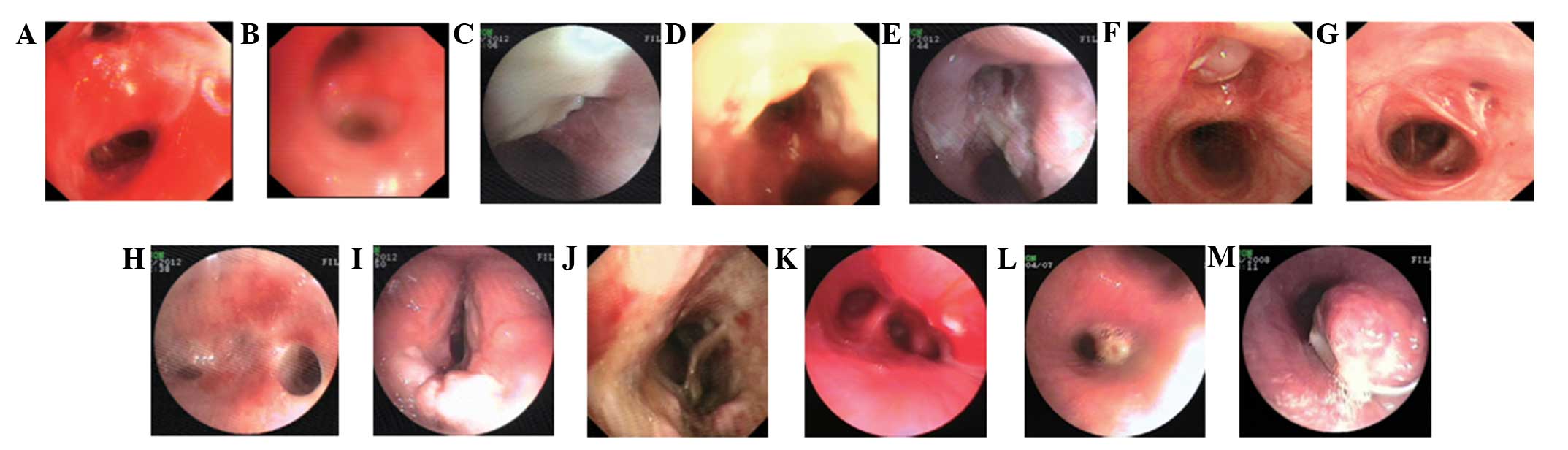
In China, TBTB is classified into six pathological types, including
the inflammatory infiltration type (Fig. 1A and B), the ulceration necrosis
type (Fig. 1C and D), the
proliferative granulation type (Fig.
1E and F), the scar stenosis type (Fig. 1G and H), the wall softening type
(Fig. 1I and J) and the lymph
fistula type (Fig. 1K–M) (10).
Imaging analysis
Among the 410 patients with TBTB, 10 patients
received chest X-ray examination. The remaining 400 patients
underwent spiral CT examination of the chest and/or airway
reconstruction examinations.
Statistical analysis
SPSS software, version 21.0 (SPSS, Inc., Chicago,
IL, USA) was used for the statistical analyses. Student’s t-tests
and χ2 test were used for analysis of the differences
between groups. P<0.05 was considered to indicate a
statistically significant difference.
Results
Characteristics of patients
The present study included 109 male and 301 female
patients in the total 410 patients with TBTB (Table I). The difference (109/301) between
the number of males and the females was found to be significant
(t=-2.357; P<0.001). Among the patients, 10 underwent chest
X-ray, revealing two cases of atelectasis, eight cases of patch or
spot shadows, three cases of cavity, one case of nodule and one
patient with no abnormalities. The remaining 400 patients underwent
chest CT scan and/or airway reconstruction examination. The results
revealed 112 cases of partial or whole left lung atelectasis, 248
cases of bronchial stenosis, 135 cases of bronchial lumen
obstruction, 255 cases of patch shadows, 179 cases of spot shadows,
124 cases of cavity, 34 cases of nodules, 134 cases of hilar and
mediastinal lymph node enlargment, 65 cases of hilar or mediastinal
lymph node calcification and 10 patients with no abnormal
alterations.
 | Table IComparison of lesion types in the 410
patients with tracheobronchial tuberculosis enrolled in the present
study. |
Table I
Comparison of lesion types in the 410
patients with tracheobronchial tuberculosis enrolled in the present
study.
| Gender | Total number of
lesions, n (%) | Congestion, n
(%) | Granulation, n
(%) | Cavity, n (%) | Stenosis, n (%) | Scar, n (%) | χ2 | P-value |
|---|
| Male (n=109) | 111 (26.2) | 1 (0.2) | 16 (3.8) | 58 (13.7) | 29 (6.8) | 7 (1.7) | | |
| Female (n=301) | 313 (73.8) | 6 (1.4) | 33 (7.8) | 170 (40.1) | 80 (18.9) | 24 (5.7) | | |
| Total (n=410) | 424 (100) | 7 (1.7) | 49 (11.6) | 228 (53.8) | 109 (25.7) | 31 (7.3) | 1.858 | 0.762 |
The bronchoscopy results indicated that among the
109 male patients, there was 1 congestion lesion, 16 granulation
lesions, 58 cavity lesions, 29 stenosis lesions and 7 scar lesions
among the five lesion types. Among the 301 female patients, there
were 6 congestion lesions, 33 granulation lesions, 170 cavity
lesions, 80 stenosis lesions and 24 scar lesions. Among all the
lesion types, the cavity lesion type was found to be the most
likely to cause bronchial stenosis or obstruction (Table II), with statistically significant
differences observed compared with the congestion, stenosis and
scar lesion types (P<0.01; Table
II). These findings suggest that the cavity lesion type is the
predominant risk factor.
| Table IIChanges in the bronchial lumen caused
by tracheobronchial tuberculosis. |
Table II
Changes in the bronchial lumen caused
by tracheobronchial tuberculosis.
| Changes in the
bronchial lumen | | |
|---|
|
| | |
|---|
| Lesion type | No stenosis, n
(%) | Stenosis, n (%) | Obstruction, n
(%) | Total, n (%) | χ2 | P-value |
|---|
| Cavity | 34 (5.1) | 228 (34.4) | 166 (25.1) | 428 (64.7) | | |
| Congestion | 4 (0.6) | 3 (0.5) | 0 (0) | 7 (1.1) | 21.940 | <0.001 |
| Granulation | 8 (1.2) | 26 (3.9) | 15 (2.3) | 49 (7.4) | 4.283 | 0.117 |
| Stenosis | 0 (0) | 109 (16.5) | 38 (5.7) | 147 (22.2) | 24.976 | <0.001 |
| Scar | 11 (1.7) | 18 (2.7) | 2 (0.3) | 31 (4.7) | 30.743 | <0.001 |
| Total | 57 (8.6) | 384 (58.0) | 221 (33.4) | 662 (100) | 85.583 | <0.001 |
Comparison of the bronchoscopic
therapies
The 410 patients with TBTB all received the
aforementioned local treatments. There were statistically
significant differences in the bronchial lumen for the granulation,
cavity and congestion lesion types prior to and following therapy
(P<0.01; Table III). However,
there were no significant differences in bronchial lumen for the
fibrous stenosis and scar lesions types prior to and following
therapy, as shown in Table III.
For the cavity type, there were 194 sites of obstruction prior to
therapy and only 23 sites of obstruction following therapy
(Table III). Furthermore, there
were 34 sites without stenosis prior to therapy and 205 sites
without stenosis following therapy. These results suggest that the
cavity type is the most sensitive to therapy among the five lesion
types. Moreover, the number of sites of obstruction was
significantly decreased and the number of sites without stenosis
was relatively increased following therapy.
| Table IIIChanges in the bronchial lumen prior
to and following therapy. |
Table III
Changes in the bronchial lumen prior
to and following therapy.
| Lesion type | -Lesion number (total
424) | Prior to therapy | Following
therapy | χ2 | P-value |
|---|
|
|
|---|
| No stenosis, n
(%) | Stenosis and/or
obstruction, n (%) | No stenosis, n
(%) | Stenosis and/or
obstruction, n (%) |
|---|
| Cavity | 228 | 34 (8.0) | 194 (45.8) | 205 (48.3) | 23 (5.4) | | |
| Congestion | 7 | 4 (0.9) | 3 (0.7) | 7 (1.7) | 0 (0) | 470.000 | <0.001 |
| Granulation | 49 | 8 (1.9) | 41 (9.7) | 44 (10.4) | 5 (1.2) | 554.000 | 0.009 |
| Stenosis | 109 | 0 (0) | 109 (25.7) | 58 (13.7) | 51 (12.0) | 674.000 | <0.001 |
| Scar | 31 | 11 (2.6) | 20 (4.7) | 11 (2.6) | 20 (4.7) | 518.000 | <0.001 |
Discussion
In the present study, 400 patients underwent chest
CT scan and/or airway reconstruction examinations, including 112
cases of partial or left whole lung atelectasis, 248 cases of
bronchial stenosis and 135 cases of bronchial obstruction. X-ray
examinations have no specificity for the diagnosis of TBTB
(10,11). However, chest CT scans with airway
reconstruction techniques are able to show stenosis and obstruction
in the bronchial lumen and clearly demonstrate the extent and scope
of the bronchial stenosis or obstruction, revealing the changes in
the bronchial walls more clearly. In addition, using this method,
it is possible to determine whether the hilar and mediastinal lymph
nodes are enlarged or have calcification (6,13).
Thus, CT scans with airway reconstruction techniques have clinical
value for TBTB diagnosis.
In the present study, all patients underwent sputum
smear microscopy three times in order to detect acid-fast bacilli
and sputum culture once using the BACTEC method. There were 135
cases that were sputum smear positive and 177 cases that were
sputum culture positive. All patients also underwent bronchoscopy
and brushing for acid-fast bacilli sputum smear and mycobacterial
culture one week following admission. There were 78 cases of
patients who were acid-fast bacilli smear positive and 169 cases of
patients who were brush mycobacterial culture positive among the
410 cases. There was no significant difference in the tuberculosis
positive rate between the male and female patients.
TBTB is capable of invading bronchial tissue,
submucosa, muscle, bronchial cartilage and outer membranes at many
sites (3,14–16).
Bronchiolar involvement has been found to be common in the main
bronchus and upper lobe bronchus, and is more common in the left
than in the right (13). In the
present study, bronchoscopy revealed that among the patients with
TBTB, 193 patients had lesions located in one site and 217 cases
had lesions in multiple sites, predominantly in the left main
bronchus (32.7%). A moderate number of lesions were observed in the
left upper lobe bronchus and the lowest number was found in the
right lower lobe bronchus.
Among the five types of lesion, bronchoscopy
examination in the present study revealed 7 congestion lesions, 49
granulation lesions, 228 cavity lesions, 109 stenosis lesions and
31 scar lesions. Furthermore, cavity lesions were found to be
significantly more common than the other types of lesions
(P<0.01).
In conclusion, the incidence of TBTB is associated
with gender and age. Young women usually have a higher incidence
and more serious disease. Among all the types of lesions, the
cavity lesion type has the highest incidence. In addition, the
cavity type is more likely to cause bronchial stenosis or
obstruction. Bronchoscopy is an effective means for the diagnosis
and treatment of TBTB and early bronchoscopy intervention is likely
to achieve better results.
Acknowledgements
This study was supported by a grant from the
Medicine and Health Care Technology Development Project of Shandong
Province (grant no. 2013WS0147).
References
|
1
|
Chung HS and Lee JH: Bronchoscopic
assessment of the evolution of endobronchial tuberculosis. Chest.
117:385–392. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wang WB, Zhao Q, Yuan ZA, Jiang WL, Liu ML
and Xu B: Deaths of tuberculosis patients in urban China: a
retrospective cohort study. Int J Tuberc Lung Dis. 17:493–498.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chinese Medical Association Tuberculosis
Branch; Editorial Board of The Journal of Tuberculosis and
Respiratory Disease. Tracheobronchial tuberculosis diagnosis and
treatment guidelines (Trial). Chinese Journal of Tuberculosis and
Respiratory Diseases. 35:581–587. 2012.(In Chinese).
|
|
4
|
Ehrlich RI, Adams S, Baatjies R and
Jeebhay MF: Chronic airflow obstruction and respiratory symptoms
following tuberculosis: a review of South African studies. Int J
Tuberc Lung Dis. 15:886–891. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Watanabe A: Clinical manifestation of Q
fever and tuberculosis, similarly caused by intracellular
parasites. Kekkaku. 81:543–549. 2006.(In Japanese).
|
|
6
|
Kashyap S, Mohapatra PR and Saini V:
Endobronchial tuberculosis. Indian J Chest Dis Allied Sci.
45:247–256. 2003.
|
|
7
|
Xue Q, Wang N, Xue X and Wang J:
Endobronchial tuberculosis: an overview. Eur J Clin Microbiol
Infect Dis. 30:1039–1044. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rikimaru T: Endobronchial tubereulosis.
Expert Rev Anti Infect Ther. 2:245–251. 2004. View Article : Google Scholar
|
|
9
|
He RX and Zhao SY: Analysis of clinical
manifestations and diagnosis of 102 children with bronchial
tuberculosis. Zhonghua Er Ke Za Zhi. 50:737–739. 2012.(In
Chinese).
|
|
10
|
Tang SJ, Xiao HP, Hu HL, et al: Clinical
characteristic, diagnostic standard and types of endobronchial
tuberculosis: An analysis of 278 cases. Chinese Journal of
Clinicians (Electronic Edition). 3:32–40. 2009.(In Chinese).
|
|
11
|
Jung SW, Kim MW, Cho SK, et al: A case of
endobronchial aspergilloma associated with foreign body in
immunocompetent patient without underlying lung disease. Tuberc
Respir Dis (Seoul). 74:231–234. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Verma A, Park HY, Lim SY, et al:
Posttuberculosis tracheobronchial stenosis: use of CT to optimize
the time of silicone stent removal. Radiology. 263:562–568. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhu XH, Shao J, You ZQ, et al: The
diagnostic value of multi-slice spiral CT in endobronchial
tuberculosis. Chinese Journal of Radiology. 38:26–29. 2004.(In
Chinese).
|
|
14
|
Jiang HN, Zuo JM and He LX: The diagnosis
and therapy advancement of tracheo-bronchial tuberculosis. Bulletin
of the Chinese Antituberculosis Association. 22:50–54. 2000.(In
Chinese).
|
|
15
|
Iwamoto Y, Miyazawa T, Kurimoto N, et al:
Interventional bronchoscopy in the management of airway stenosis
due to tracheobronchial tuberculosis. Chest. 126:1344–1352. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chhajed PN, Malouf MA and Glanville AR:
Bronchoscopic dilatation in the management of benign
(non-transplant) tracheobronchial stenosis. Intern Med J.
31:512–516. 2001. View Article : Google Scholar : PubMed/NCBI
|