Introduction
Congenital agenesis of the unilateral adnexa is an
uncommon condition that has rarely been described in the
literature. In addition, the incidence of adnexal malformations is
difficult to determine. It has been suggested to be 1:11,240
(1). Etiologies of ipsilateral
ovarian and/or tubal agenesis remain unclear; however, a number of
studies have conducted research into this area (1–4). A
number of authors suggest that this abnormity is either a
congenital malformation or a result of an torsion that occurred to
the ovarian pedicle in birth, childhood or adult life (3,5).
Adnexal agenesis has always been associated with malformations of
the uterus and/or urinary tract. Unilateral absence of the adnexa
without a uterine deformity is rarely reported. The majority of
patients are asymptomatic and can be diagnosed incidentally
following a laparoscopy or laparotomy for various gynecological or
obstetric complications. The current study reports the case of a
26-year-old female who had been infertile for two years and had
been diagnosed with unilateral agenesis of the ovary and fallopian
tube during diagnostic laparoscopy and hysteroscopy. In the present
study, the literature was reviewed in order to identify possible
causes of these anomalies.
Case report
A 26-year-old nulligravida was admitted to the
Department of Gynecology at the Women’s Hospital of Zhejiang
University (Hangzhou, Zhejiang) with a diagnosis of primary
infertility. Informed consent was obtained from the patient for the
present study. The patient had not conceived despite regular
unprotected intercourse for two years. Menarche occurred at 12
years of age, and the menstrual cycle was regular with 27–28 day
intervals and a 5–6-day menstrual period without dysmenorrhea. The
overall health of the patient was good and there was no history of
abdominopelvic surgery or pelvalgia. On physical examination, no
surgical scars were observed. The external genitalia, vagina,
cervix and uterus appeared normal on gynecological examination, and
the results of sex hormone analysis were also normal. The patient’s
husband submitted a semen analysis, which was within the normal
limits. Transvaginal ultrasonography revealed that the uterus and
ovaries (only the right ovary was visualized) were normal.
Hysterosalpingography was performed in the Wenling Ruoheng Hospital
(Wenling, China) additional local hospital, which revealed a normal
uterine cavity; however, the fallopian tubes did not fill
bilaterally; the hysterosalpingography was not repeated.
Furthermore, genetic analysis revealed a normal karyotype
(46,XX).
Subsequently, a diagnostic laparoscopy and
hysteroscopy were performed. During the hysteroscopy, the
endometrial cavity was observed to be normal, as well as the left
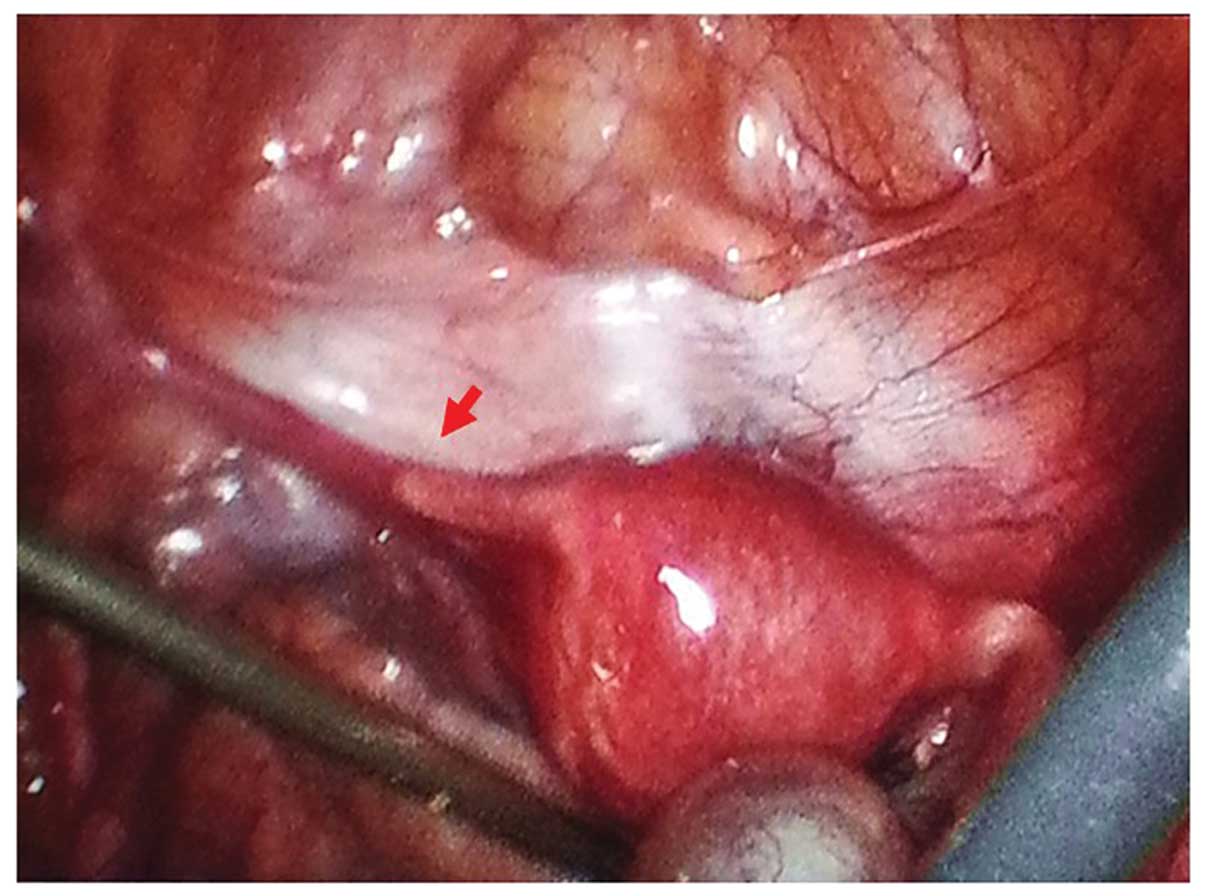
and right tubal ostia. The laparoscopy revealed a single,
normal-sized uterus with a smooth surface. No adhesion between the
uterus and the intestinal serosa, the cecum and the pelvic wall was
observed. The rectouterine pouch was inspected and no ectopic
tissues were identified. The left adnexa was not completely
visualized; however, a 2-cm tubal remnant with an intact left round
ligament was observed. The right fallopian tube, right ovary (with
a corpus luteum) and right round ligament were found to be normal
(Fig. 1). The broad ligaments were
also normal without any adhesions. In addition, the peritoneal and
omental surfaces were analyzed and no ectopic tissues or remnant
structures were observed. Methylene blue chromopertubation did not
result in spill from the right fallopian tube and the postoperative
course was uneventful.
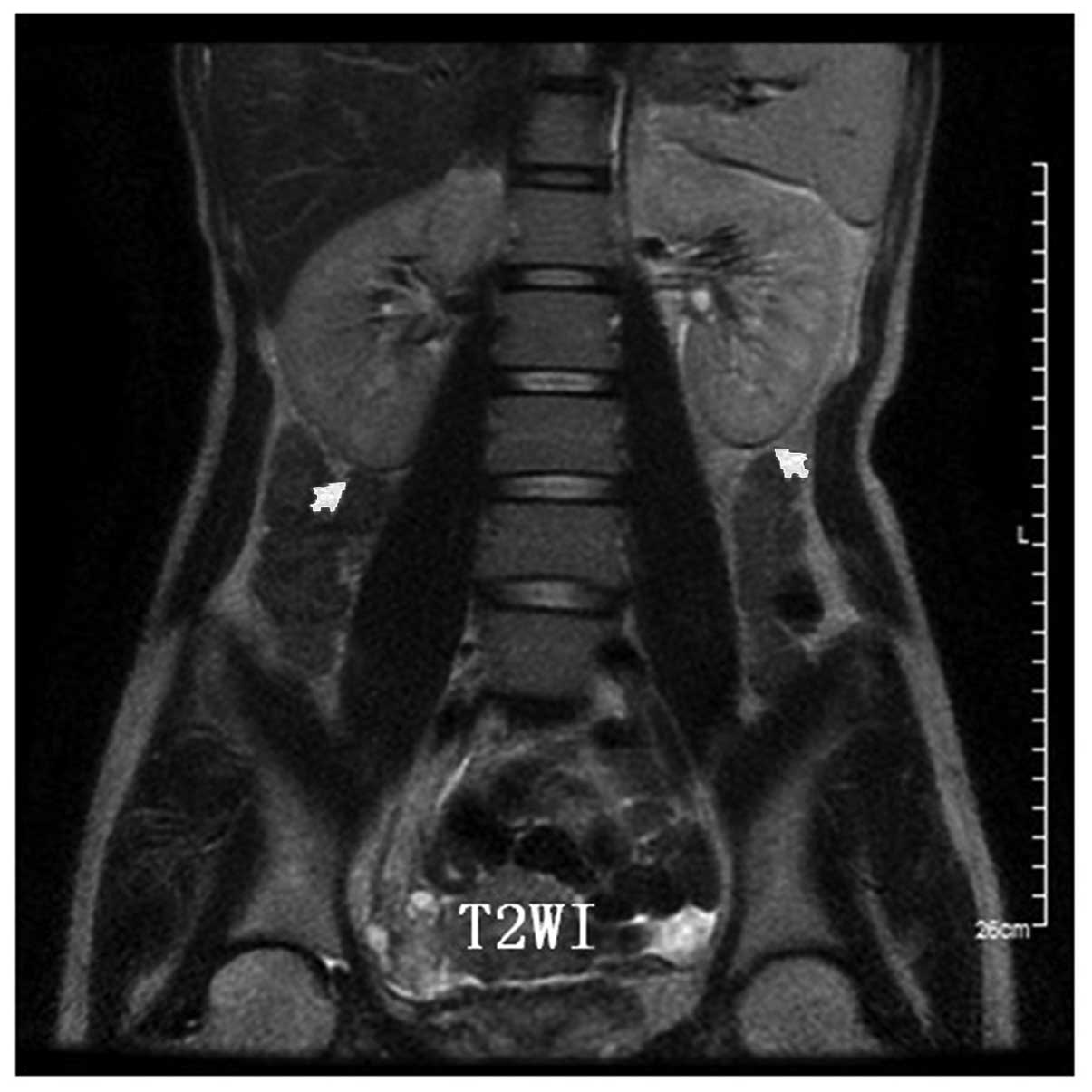
Since adnexal agenesis often coexists with
malformations of the urinary tract, abdominopelvic magnetic
resonance imaging (MRI) was performed to investigate the urinary
system. The MRI scan revealed that the kidneys and ureters were
normal bilaterally, while the left ovary was unable to be imaged
(Fig. 2).
Unilateral absence of the adnexa is rarely reported
without a uterine deformity. Therefore, the present case report
prompted a comprehensive literature review. Similar cases reported
in the literature, describing unilateral agenesis or the absence of
the ovary and fallopian tube without uterine anomalies, are
presented in Table I. A total of
25 cases were identified, of which nine cases were diagnosed with
primary infertility and seven cases had undergone normal
deliveries. In particular, one patient was single, one had
contraception by drugs, one had an extrauterine pregnancy and the
fertility of the other six cases were not mentioned in the
literature. Among the nine nulligravidas, three individuals had
obstructed contralateral fallopian tubes, three patients had
unobstructed tubes and the condition of the other three were not
mentioned in the literature. In certain cases, dysmorphosis of the
genital tract coexists with urinary tract anomalies. Two cases were
found to be associated with ipsilateral absence of the kidney,
while in six cases, urinary tract anomalies were not mentioned.
 | Table IAbsence of ovaries and/or fallopian
tubes with a normal uterus. |
Table I
Absence of ovaries and/or fallopian
tubes with a normal uterus.
| First author
(reference) | Ovarian and/or tubal
anomalies | Urinary anomaly | Fertility | Other notable
observations |
|---|
| Elkington N (21) | Absent left tube and
ovary | No | Normal delivery | |
| Pabuccu E (10) | Absent left tube and
ovary | No | Primary
infertility | |
| Vaiarelli A (4) | Complete absence of
right ovary; 2-cm proximal stump of the right tube | NM | Primary
infertility | History of acute
pelvic pain 10 years previously |
| Gursoy AY (8) | Absence of left ovary
and tube | Absence of left
kidney | Normal delivery | |
| Eustace DL (3) |
| Case 1 | Absent right tube and
ovary | No | Primary
infertility | |
| Case 2 | Absent right tube and
ovary | NM | Normal delivery | |
| Sivanesaratnam V
(6) |
| Case 1 | Absent left ovary and
tube | No | NM | |
| Case 2 | Absent right ovary
and tube | No | Primary
infertility | Blocked right
tube |
| Mylonas I (5) |
| Case 1 | Absent right ovary
and tube | No | Normal delivery | |
| Case 2 | Absent right ovary
and tube | No | Contraception by
drugs | |
| Case 3 | Absence right
adnexa | No | Primary
infertility | Blocked left
tube |
| Muppala H (9) | Absent right ovary,
tube and round ligament | Right renal
agenesis | NM | Pyloric stenosis |
| Uckuyu A (14) |
| Case 1 | Absent left distal
tubal segment, streak left ovary | No | Primary
infertility | Unilateral tubal
patency |
| Case 2 | Absent right distal
tubal segment, normal right ovary | No | Primary
infertility | Unilateral tubal
patency |
| Case 3 | Twisted left tube,
absent right ovary | No | Primary
infertility | Unilateral tubal
patency |
| Case 4 | Left ovarian
agenesis | No | | |
| Tzitzimikas S
(22) | Absence of the left
ovary and the distal part of the ipsilateral tube | No | NM | |
| Gotti G (23) | Absent right ovary
and tube | No | Extrauterine
pregnancy | |
| Rapisarda G (1) | Absent left ovary and
tube | NM | Primary
infertility | Obstructed right
tube |
| Sirisena LA (2) | Absent left ovary and
distal tube | No | NM | |
| Georgy FM (13) | Absent left ovary and
tube | No | NM | |
| Guan Q (15) | Absent right ovary
and tube | NM | Normal delivery | Teratomas on the
uterine surface |
| Liu Q (16) | Absent right ovary
and tube | No | NM | Extraperitoneal huge
serous cystadenoma |
| Ma CL (17) |
| Case 1 | Absent left
ovary | NM | Normal delivery | Teratomas on the
great omentum |
| Case 2 | Absent left ovary and
tube | NM | Normal delivery | Teratomas on the
great omentum |
Discussion
Congenital absence of the ovary is a rare condition,
with one in every 11,240 individuals affected (6); however, the incidence may be higher
as it is difficult to estimate the number of cases since the
majority are asymptomatic and go unreported. All cases reported in
the literature were diagnosed incidentally following a laparoscopy
or laparotomy for various gynecological or obstetric complications.
The first published case of unilateral ovarian absence was reported
in 1923 (7). In recent years,
several similar cases have been reported (1,4,8,9),
which may be due to the widespread use of laparoscopy for
diagnostic purposes; however, the total number of cases remains
small.
Adnexal agenesis is often associated with
malformations of the uterus and/or urinary tract, including a
unicornuate uterus and unilateral renal agenesis (10). Congenital absence of the ovary may
be accompanied with total or partial absence of the ipsilateral
fallopian tube. However, unilateral absence of the adnexa without a
uterine deformity is rarely reported. In the present case report,
the uterus was considered normal in shape and structure during
diagnostic laparoscopy and hysteroscopy. The literature was
reviewed and a number of similar cases without uterine anomalies
were identified (Table I). A
number of studies have also evaluated the urinary tract in patients
with ovarian agenesis (8,9). Among the cases listed, there were two
patients with unilateral renal agenesis. In the present case, the
results from the MRI scan revealed that the kidneys were
normal.
The true etiology of ipsilateral ovarian and/or
tubal absence has yet to be elucidated (1–3). The
two most likely causes of ipsilateral ovarian and/or tubal absence
may include an asymptomatic torsion of the adnexa with consequent
organ ischemia and reabsorption (3,5,11),
or a defect in the development of the Mullerian and gonadal
structures (3,6,12)
underlying vascular anomalies (11).
A number of studies have indicated that unilateral
absence of the fallopian tube and ovary is the result of adnexal
torsion with necrosis and resorption, which may occur antenatally
or postnatally (3,5). Furthermore, it has been suggested
that symptoms may be minimal or absent, although severe pain in the
lower abdomen is a typical symptom of adnexal torsion (3). In 1974, Georgy and Viechnicki
(13) reported a case with the
absence of an ovary and uterine tube. This case supported the
torsion hypothesis since a calcific ovary was situated in the
Douglas cul-de-sac. The study by Uckuyu et al (14) also supported the torsion hypothesis
since separated tubal and ovarian tissue remnants were observed in
the abdominal cavity. In addition, Vaiarelli et al (4) reported a case where the ovary and
ipsilateral fallopian tube were absent. The patient had presented
with acute, transient right-sided pelvic pain 10 years previously,
which was not diagnosed as adnexal torsion following medical
attention. In retrospect, this acute pain may have represented
torsion of the right adnexa.
A number of previous cases have demonstrated that
unilateral ovarian absence coexists with teratomas on the great
omentum or the uterine surface (15–17).
Omental cystic teratomas are rare. The authors analyzed the torsion
of the ovarian tumors that ruptured and parasitized on the greater
omentum (15–17), and it was hypothesized that the
incidence may be associated with embryonic developmental
abnormalities. While this torsion hypothesis appears plausible,
there is no evidence of its occurrence in the present case report.
The patient had no history of unexplained abdominal pain, and
during laparoscopic surgery, no ectopic tissues or remnant
structures on the peritoneal or omental surfaces were observed.
However, the absence of symptoms does not exclude the possibility
of torsion antenatally.
Developmental abnormalities have been observed in
the female reproductive tract, including the fallopian tubes,
ovaries, uterus, cervix, vagina and external genitalia. Usually,
abnormalities include organs that originate from the Mullerian
ducts. In the sixth week of gestation, the bilateral Mullerian
ducts migrate towards the midline, meet, form luminal structures,
fuse and finally form the uterus and upper one-fifth of the vagina.
Rostrally, the Mullerian ducts form fallopian tubes. Any
disturbance in the migration, fusion or resorption of these ducts
may result in a Mullerian anomaly (18). Paternoster et al (12) presented two cases of absent
fallopian tubes, and hypothesized that partial or total unilateral
defects of the paramesonephric duct were more common than aplasia
of the two ducts. Therefore, a unicornuate uterus, one fallopian
tube and one rudimentary or ectopic kidney indicates a defect in
the development of all Mullerian structures.
In comparison to Mullerian duct-derived organs,
congenital defects of the ovary are rare. Gonadal development
depends on accurate germ cell migration, as well as appropriate
formation of the urogenital ridge. These processes are regulated by
multiple factors and genes (19),
and a unilateral defect at any point during this process may
prevent ovarian formation. Unilateral ovarian agenesis coexisting
with an ipsilateral fallopian tube and a normal uterus is a
complicated condition. It has been hypothesized that a defect
localized to the region of the genital ridge and the caudal area of
the Mullerian duct (5,20) reflects improper development of the
urogenital ridge, which affects the development of the fallopian
tube in that region. A number of studies have indicated that an
inadequate blood supply during the descent into the pelvis of the
caudal section of the paramesonephric duct may lead to adnexal
agenesis (3,5,12);
however, a clear developmental explanation for this malformation
has not yet been elucidated. The patient in the current study
presented for evaluation with a normal uterus and right adnexa
observed during diagnostic laparoscopy and hysteroscopy; thus,
excluding the possibility of a unicornuate uterus. Furthermore, the
normal karyotype did not support the diagnosis of a chromosomal
condition associated with the absence of the fallopian tube and
ovary; for example, pure or mixed gonadal dysgenesis (46XY or
45X0/46XY).
A number of similar patients have been reported in
the literature, with anatomic abnormalities observed during
evaluations for primary infertility. It is unknown whether
unilateral adnexal absence may be a cause of infertility. Several
authors have hypothesized that unilateral adnexal absence does not
diminish female fertility, particularly when the condition is not
accompanied by a uterine malformation (9). Uckuyu et al (14) also investigated the function of the
contralateral tube and concluded that unilateral agenesis is a
possible factor in patients with infertility. Unilateral absence of
the adnexa may reduce the probability of becoming pregnant;
however, pregnancy remains possible if there is a functional
fallopian tube. Previously, a patient with this condition was
reported who had four normal pregnancies that resulted in normal
vaginal deliveries (8). The
patient presented in the current study was found to have an absent
left adnexa and an obstructed right fallopian tube during
laparoscopic examination, with no passage of methylene blue
solution from the lumen of the right tube; however, the uterus and
right ovary were normal. Previous studies have described
contralateral occluded tubes (1,6,5). We
hypothesized that contralateral tubal pathology may contribute to
sterility. However, whether unilateral congenital tubal and ovarian
anomalies affect the function of the other tube and the pelvic
microenvironment remains unclear.
In conclusion, unilateral ovarian and fallopian tube
agenesis is a rare condition. The true etiology of adnexal
anomalies remain unclear, although torsion or congenital defects
may be the most likely explanations. In addition, the observations
of the present study indicate that contralateral tubal pathologies
may contribute to infertility.
Acknowledgements
The study was supported by grants from the Zhejiang
Provincial Natural Science Foundation of China and the Subject Fund
of Zhejiang Province Department of Education (nos. Y13H040005 and
Y201121826, respectively).
References
|
1
|
Rapisarda G, Pappalardo EM, Arancio A and
La Greca M: Unilateral ovarian and fallopian tube agenesis. Arch
Gynecol Obstet. 280:849–850. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sirisena LA: Unexplained absence of an
ovary and uterine tube. Postgrad Med J. 54:423–424. 1978.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Eustace DL: Congenital absence of
fallopian tube and ovary. Eur J Obstet Gynecol Reprod Biol.
46:157–159. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Vaiarelli A, Luk J and Patrizio P: Ectopic
pregnancy after IVF in a patient with unilateral agenesis of the
fallopian tube and ovary and with endometriosis: search of the
literature for these associations. J Assist Reprod Genet.
29:901–904. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mylonas I, Hansch S, Markmann S, Bolz M
and Friese K: Unilateral ovarian agenesis: report of three cases
and review of literature. Arch Gynecol Obstet. 268:57–60.
2003.PubMed/NCBI
|
|
6
|
Sivanesaratnam V: Unexplained unilateral
absence of ovary and fallopian tube. Eur J Obstet Gynecol Reprod
Med. 22:103–105. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Alexander HD: True unicornuate uterus and
total absence of left broad ligament, round ligament, salpinx,
ovary, kidney and ureter. Can Med Assoc J. 56:5391947.PubMed/NCBI
|
|
8
|
Gursoy AY, Akdemir N, Hamurcu U and
Gozukucuk M: Incidental diagnosis of unilateral renal and adnexal
agenesis in a 46-year-old multiparous woman. Am J Case Rep.
14:238–240. 2013.PubMed/NCBI
|
|
9
|
Muppala H, Sengupta S and Martin JE:
Unilateral absence of tube and ovary with renal agenesis and
associated pyloric stenosis: communication. Eur J Obstet Gynecol
Reprod Biol. 137:1232008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pabuccu E, Kahraman K, Taskın S and
Atabekoglu C: Unilateral absence of fallopian tube and ovary in an
infertile patient. Fertil Steril. 96:e55–e57. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Dahan MH, Burney R and Lathi R: Congenital
interruption of the ampullary portion of the fallopian tube. Fertil
Steril. 85:1820–1821. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Paternoster DM, Costantini W, Uglietti A,
Vasile C and Bocconi L: Congenital or torsion-induced absence of
fallopian tubes. Two case reports. Minerva Ginecol. 50:191–194.
1998.PubMed/NCBI
|
|
13
|
Georgy FM and Viechnicki MB: Absence of an
ovary and uterine tube. Obstet Gynecol. 44:441–442. 1974.PubMed/NCBI
|
|
14
|
Uckuyu A, Ozcimen EE and Sevinc Ciftci FC:
Unilateral congenital ovarian and partial tubal absence: report of
four cases with review of literature. Fertil Steril. 91:936 e5–e8.
2009.PubMed/NCBI
|
|
15
|
Guan Q and Wu YZ: A full-term pregnancy
complicated with uterine mature teratoma and one adnexal absence.
Chin J Obstet Gynecol. 41:4122006.
|
|
16
|
Liu Q and Sun XB: A retroperitoneal giant
serous cystadenoma with unilateral adnexal absence: a case report
and review of literature. Chin J Obstet Gynecol. 48:136–137.
2013.
|
|
17
|
Ma CL: Greater omental teratoma with
congenital absence of the left ovarian: report of 2 cases. Chin J
Clin Obstet Gynecol. 7:3022006.
|
|
18
|
Simpson JL: Genetics of the female
reproductive ducts. Am J Med Genet. 89:224–239. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Saitou M, Barton SC and Surani MA: A
molecular programme for the specification of germ cell fate in
mice. Nature. 418:293–300. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Dare FO, Makinde OO, Makinde ON and
Odutayo R: Congenital absence of an ovary in a Nigerian woman. Int
J Gynaecol Obstet. 29:377–378. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Elkington N and Rahman R: Unexplained
unilateral absence of fallopian tube and ovary. The Internet
Journal of Gynecology and Obstetrics. 11: View Article : Google Scholar : 2008.
|
|
22
|
Tzitzimikas S, Fragkos M and Karavida A:
Unilateral ovarian absence. Gynecol Surg. 10:93–95. 2013.
View Article : Google Scholar
|
|
23
|
Gotti G, Ferrone R, Andreoli M, Turini A,
Russo P and Di Donato P: Agenesia o assenza annessiale
monolaterale? Descrizione di uncaso clinic. It J Gynaecol Obstet.
20(2): 87–89. 2008.
|