Introduction
Nuclear ubiquitous casein and cyclin-dependent
kinases substrate 1 (NUCKS1) is a nuclear DNA binding protein found
in almost all types of human cells (1). NUCKS1 was first described in 2001 by
Ostvold et al (2), who
isolated and characterized a cDNA encoding a mammalian nuclear
phosphoprotein NUCKS1, previously designated P1 (2). However, the biological role of NUCKS1
remains poorly understood. The structural similarity to the
high-mobility group A (HMGA) proteins indicates that NUCKS1 is
involved in the regulation of chromatin structure and activity
(3). Increased expression of HMGA
proteins has been found in a large number of tumor tissues,
including breast cancer tissues, whilst in normal tissues,
expression levels of HMGA proteins are low or almost undetectable
(4). High expression levels of
HMGA proteins correlate with poor prognostic factors and
metastasis; thus, HMGA may be used as a marker of tumor progression
(5). NUCKS1 may also be considered
to have a similar role in the histopathological diagnosis of
malignant tumors. NUCKS1 has been previously reported to be
involved in facilitating and maintaining the transcription activity
of certain genes. The abundance of NUCKS1 in rapidly growing cells,
and the overexpression of NUCKS1 mRNA in ovarian cancer, supports
this hypothesis (6). Recently,
NUCKS1 has been identified as a colorectal cancer prognostic marker
in a large cohort study (7).
Invasive breast carcinoma of no special type is distinguished by
its vast histopathological heterogeneity resulting from the
self-renewal and differentiation abilities, which have led to the
classification of invasive breast carcinoma of no special type into
several subtypes (8,9). The estrogen receptor (ER),
progesterone receptor (PR), human epidermal growth factor receptor
2 (HER2) and Ki-67 are the most important biological markers for
forming a prognosis and determining effective treatment methods for
patients with breast cancer. Therefore, in 2011, the St. Gallen
International Expert Consensus proposed a novel classification
system based on the expression of these markers. The classification
system divides invasive breast carcinoma into four molecular
subtypes: Luminal A, luminal B, HER2 and basal-like (triple
negative) (10); thus, the major
subtypes are defined by gene profile and histochemical biomarker
expression (11,12).
The expression of NUCKS1 in invasive breast
carcinoma of no special type has been previously investigated
(13); however, the previous
analysis included 26 cases and assessed the associations with the
histological grade of tumors and NUCKS1 overexpression only.
Therefore, the research was broadened to cover a larger range of
invasive breast carcinoma of no special type cases (14), analyzing the associations with
selected clinicopathological data and the well-known
immunohistochemical markers, Ki-67 (15) and basal marker, cytokeratin 5/6 (CK
5/6). The aim of the present study was to establish whether NUCKS1
expression may be considered as a prognostic marker of breast
carcinoma, and whether this marker correlates with other
clinicopathological features.
Materials and methods
Patients
The research group consisted of 90 female patients
with primary invasive breast carcinoma of no special type that had
been diagnosed and treated between 2003 and 2007 in the Sokołowski
Regional Hospital (Wałbrzych, Poland) or the Department of Surgical
Oncology of Wrocław Medical University (Wrocław, Poland). The study
was approved by the local Ethics Committee (Wrocław Medical
University, Wrocław, Poland) and written informed consent was
obtained from the patient. Patients were selected on the basis of
the availability of clinicopathological data, including information
regarding tumor grade, lymph node involvement and the presence of
metastasis. The characteristics of the patients are shown in
Table I. All the samples were
obtained following routine mastectomy and the patients received
adequate radio-, hormone- or chemotherapy and appropriate axillary
lymph node excision. The Nottingham Grading System (16) was used in the study for assessing
the tumor grade. Lymph node involvement was established by surgical
and histological evaluation, while distant metastases were assessed
by surgery and imaging studies (magnetic resonance imaging and/or
computed tomography). All the samples included in the study were
classified into four subtypes: (i) Luminal A (ER+,
PR+ or PR−, HER2− and a low Ki-67
index of <14%); (ii) luminal B with HER2−
(ER+, PR+ or PR−, HER2−
and a high Ki-67 index) and luminal B with HER2+
(ER+, PR+ or PR− and
HER2+); (iii) HER2 (ER−, PR− and
HER2+); and (iv) basal-like (triple negative;
ER−, PR− and HER2−).
 | Table IClinicopathological characteristics of
the study patients. |
Table I
Clinicopathological characteristics of
the study patients.
| Characteristics | Patients, n (%) |
|---|
| Aged 33–80 years
(mean, 56 years) | 90 (100.0) |
| Tumor grade |
| I | 28 (31.1) |
| II | 30 (33.3) |
| III | 32 (35.6) |
| Lymph node
involvement |
| Negative | 41 (45.6) |
| Positive | 49 (54.4) |
| Metastasis |
| M0 | 65 (72.2) |
| M1 | 25 (27.8) |
Immunohistochemistry
Formalin-fixed and paraffin-embedded (FFPE)
histological sections were used for immunohistochemistry. Blocks
were cut into 4-μm sections, deparaffinized in two changes of
xylene, rehydrated in alcohols (96, 80 and 70% for 1 min each),
washed in distilled water, stained in hematoxylin (Sigma-Aldrich,
Steinheim, Germany), washed in tap water for 5 min and then
counterstained with eosin (Sigma-Aldrich). Sections were then
washed in distilled water, dehydrated through alcohols and mounted
in mounting medium (Dako, Glostrup, Denmark). Sections stained with
hematoxylin and eosin (HE) were evaluated with regard to the
histopathological diagnosis (only the invasive breast carcinoma of
no special type was selected). Following histopathological analysis
of the HE-stained sections, the most representative area of the
tumor was marked, paraffin blocks were cut again into 4 μm-thick
slices and were stained using immunohistochemistry.
Immunohistochemical staining was performed using the labeled
streptavidin biotin (LSAB) method [LSAB+ System horseradish
peroxidase (HRP); Dako] with the following reagents: Peroxidase
blocking reagent, protein block reagent, antibody diluent with
background reducing components, biotinylated-conjugated antibody
and streptavidin-HRP and chromogen solution. Slides were
deparaffinized in two changes of xylene for 10 min, then rehydrated
in a series of graded alcohols (96, 80 and 70% ) for 3 min each.
Next, the specimens were washed twice for 4 min in distilled water,
and were microwaved in a citric buffer [0.1 M citric acid, 0.05%
Tween 20, (pH 6.0); Sigma-Aldrich] for 8 min for heat-induced
epitope retrieval. Following two washes in distilled water for 4
min, the specimens were incubated for 10 min with peroxidase
blocking reagent and rinsed twice for 5 min with phosphate-buffered
saline (PBS). Next, incubation with protein block reagent was
performed for 10 min, after which specimens were incubated with
primary antibodies and stored overnight at 4°C. Monoclonal
antibodies against ER, PR and HER2 were obtained from Dako as ready
to use solutions. Antibodies against CK 5/6 (Dako) were diluted at
1:50, Ki-67 (Dako) antibodies were diluted at 1:200, while NUCKS1
antibodies had a 1:200 dilution. The antibodies against NUCKS1 were
elicited in rabbits using synthetic peptides and purified as
previously described (13).
Following overnight incubation, the slides were incubated for 15
min with biotinylated-conjugated antibodies and streptavidin-HRP,
rinsing twice with PBS between and following the incubation. The
reaction was detected and visualized using 3,3′-diaminobenzidine
(DAB) in chromogen solution (Sigma-Aldrich). Finally, the samples
were counterstained with hematoxylin, dehydrated using the
aforementioned alcohols for 3 min each, cleared in two changes of
xylene for 5 min and mounted with xylene-based mounting medium
(Dako).
Negative controls were achieved by omitting the
first antibodies, whereas the positive controls for each antibody
consisted of invasive breast carcinoma of no special type known to
express the antigen of interest.
The immunoreactivity of HER2, ER, PR, CK 5/6, Ki-67
and NUCKS1 was evaluated using an Allred Score (17) by three independent pathologists.
For the ER and PR a score of >2 was recorded as positive,
whereas for NUCKS1 and CK 5/6 a score of >3 was considered as
positive. Staining for HER2 was considered as positive only when
the score was 6 (when strong staining was observed in ≥30% of
cancer cells). Positive immunoexpression for Ki-67 was evaluated
when the Ki-67 index was >14%, according to the guidelines of
the St. Gallen International Expert Consensus (10). Histological evaluation was
performed using light microscopy (magnification, ×200; CX41,
Olympus, Tokyo, Japan), and images were captured using a digital
camera (DP10; Olympus).
Fluorescence in situ hybridization
(FISH)
HER2 amplification was confirmed using FISH
(PathVysion Her-2 DNA Probe kit; Abbott Molecular, Des Plaines, IL,
USA) when the immunohistochemistry score was ≥2. The proper blocks
were sectioned into 4-μm thick slices, then deparaffinized,
rehydrated and air-dried. The sections were placed in 0.2 M HCl for
20 min, rinsed with deionized water for 3 min and washed twice in
saline-sodium citrate buffer (SSC) for 3 min. Subsequently, the
sections were pretreated with sodium thiocyanate solution at 80°C
for 30 min, followed by rinsing with deionized water for 1 min and
washing twice with SSC for 5 min. Next, the specimens were
subjected to protease digestion at 45°C for 45 min, washed twice in
SSC for 5 min, dehydrated and dried at room temperature. The
sections were denatured in SSC for 5 min at 75°C on a heater. The
PathVysion probe was applied and specimens were incubated overnight
at 37°C. Next, the sections were washed twice in SSC, followed by
SSC/0.3% NP40 for 1 min at 72°C. The sections were then dried,
counterstained with 4′,6-diamidino-2-phenylindole and analyzed
using an Olympus BX43 Fluorescence Microscope (Olympus). Samples
that were HER2+ following amplification were also
included in the HER2 positive group.
Western blot analysis
For western blot analysis, proper sections from the
FFPE tumor blocks were used. Samples were macrodissected,
deparaffinized and homogenized in a lysis buffer [0.1 M Tris-HCl
(pH 8.0), 0.1 M DTT and 4% SDS) using a MagNA Lyser (Roche Applied
Science, Penzberg, Germany). Following sonication with an
Ultrasonic Processor (Hielscher, Teltow, Germany), the samples were
lysed in a Thermomixer R (Eppendorf, Hamburg, Germany) with
agitation (20 × g) for 1 h. The crude extracts were then clarified
by centrifugation at 16,000 × g at 25°C for 10 min. The protein
concentration in the supernatant was measured at 280 nm using a
NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific, Inc.,
Waltham, MA, USA). For western blot analysis, NuPAGE Novex Bis-Tris
gels (4–12%), equipment, standards and buffers recommended by
Invitrogen Life Technologies (Carlsbad, CA, USA) were used.
Nitrocellulose membranes were obtained from GE Healthcare (Little
Chalfont, UK). Following SDS-PAGE, the membranes were washed in
PBS, incubated with 2.5% glutaraldehyde (Sigma-Aldrich, Steinheim,
Germany) in PBS for 10 min and washed in PBS-Tween 0.5%. The
membranes were then blocked with 5% normal goat serum
(Sigma-Aldrich) in PBS-Tween 0.1% for 30 min, and then incubated
overnight with a rabbit primary antibody (1:250) against NUCKS1 at
4°C. Next, the membranes were washed with PBS-Tween 0.1% and
incubated with a peroxidase-conjugated secondary antibody (goat
polyclonal antibody against rabbit immunoglobulin G; Abcam,
Cambridge, UK). The specific protein bands were visualized by
reaction with DAB using a DAB Enhanced Liquid Substrate System for
Immunohistochemistry (Sigma-Aldrich) and the results were recorded
using Molecular Imager Gel Doc TMXR+ (Bio-Rad, Hercules, CA,
USA).
Statistical analysis
Associations between the various markers and
clinicopathological data were analyzed using the χ2 test
and Fisher’s exact test. The χ2 statistical test was
used assuming in hypothesis 0 that the expression of NUCKS1 and
other features of tumors are independent (18). P<0.05 was considered to indicate
a statistically significant difference. Statistical analysis was
performed by STATISTICA v.10.0 (StatSoft, Kraków, Poland).
Results
Expression of tumor markers
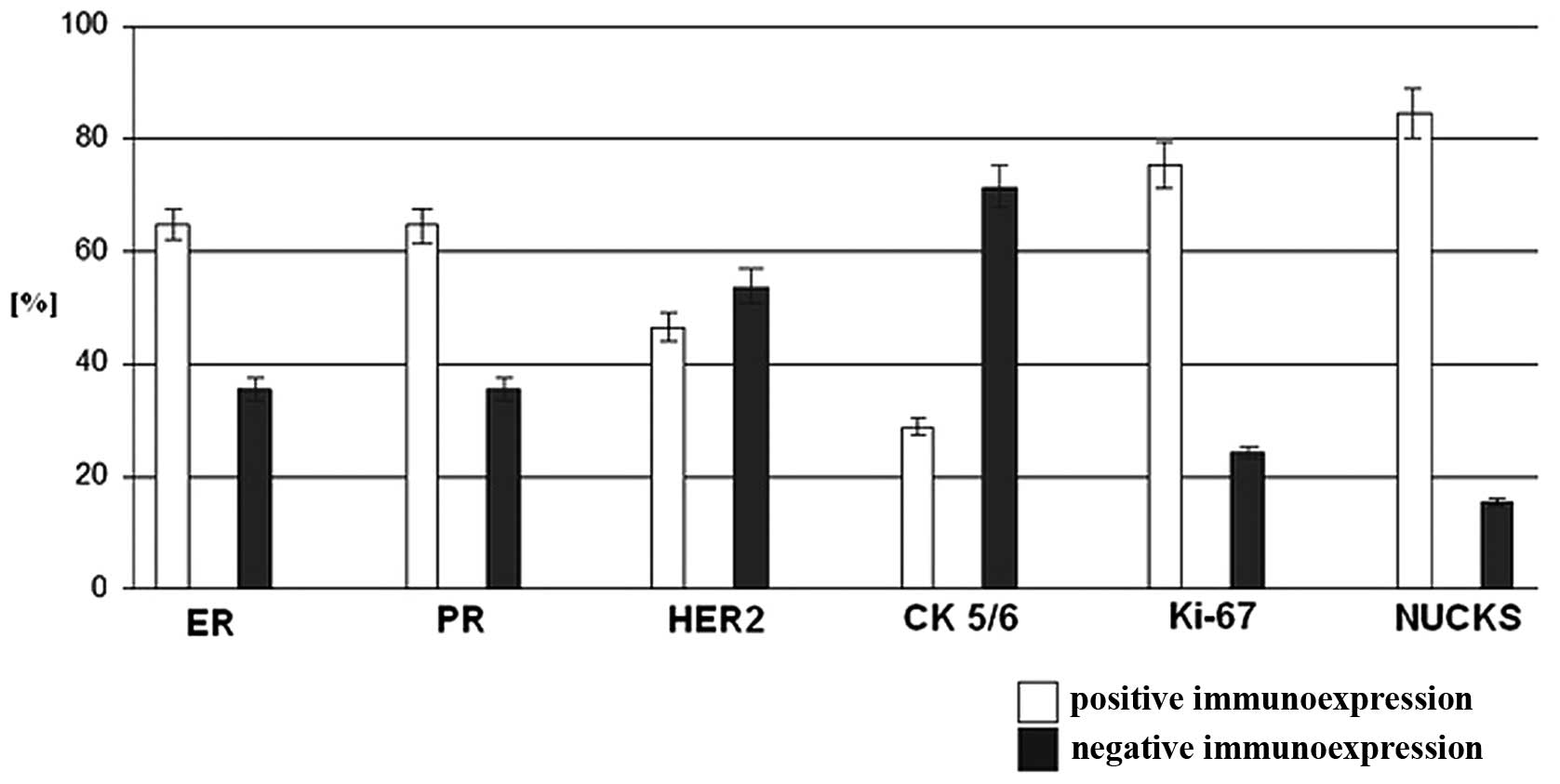
Immunoexpression levels of the analyzed markers are
shown in Fig 1. Reactivity for
NUCKS1, ER, PR and Ki-67 was observed in >50% of all the
examined samples, whereas the expression of HER2 and CK 5/6 was
below this level. The overall positive NUCKS1 expression was 84.4%,
which was higher compared with the other investigated markers,
including Ki-67 (75.6%), PR (64.4%), RR (64.4%), HER2 (46.7%) and
CK 5/6 (28.9%).
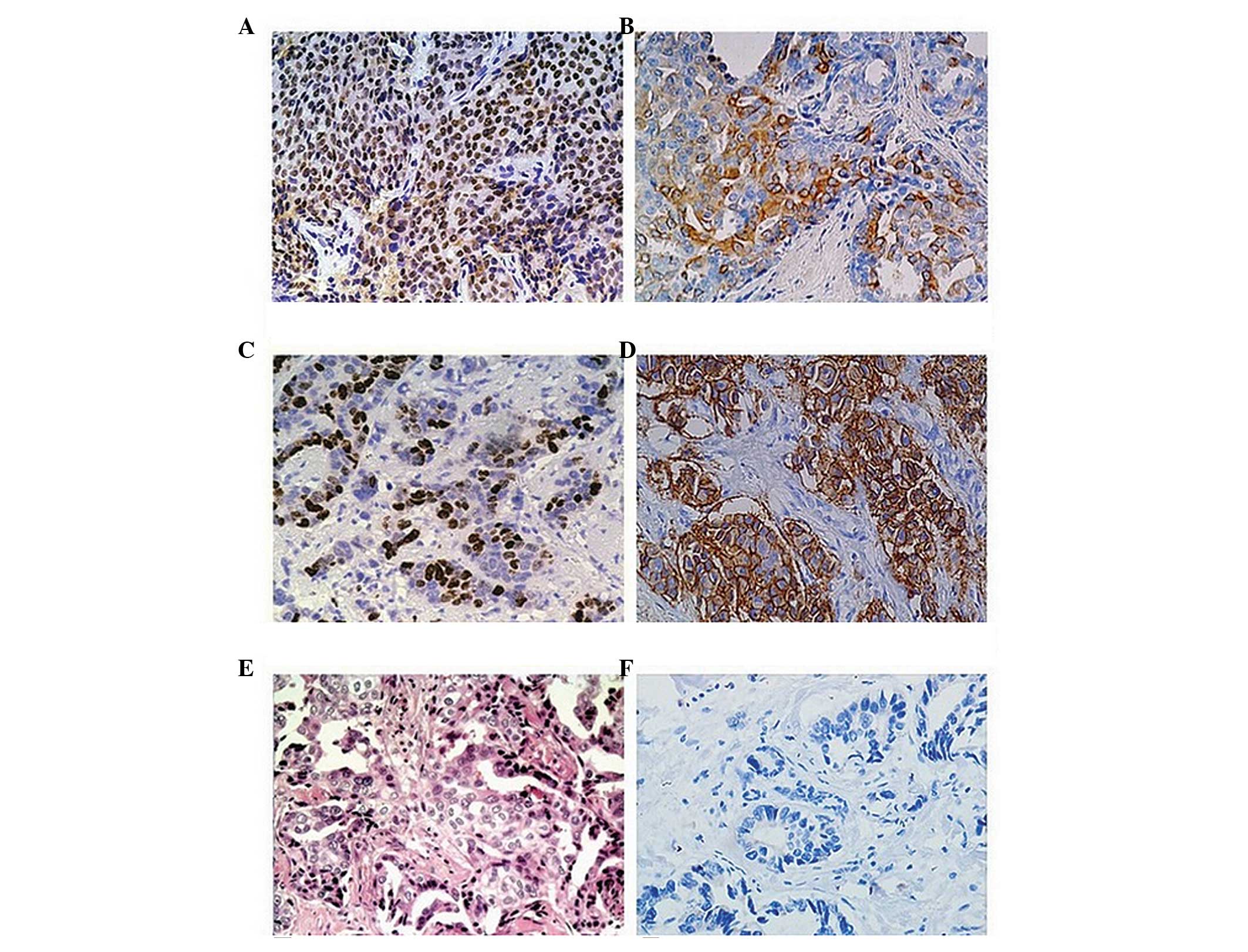
Staining for NUCKS1 was predominantly nuclear, and
cytoplasmic to a lesser extent (Fig
2A), whereas the pattern of immunohistochemical staining was
cytoplasmic for CK 5/6 (Fig 2B).
Immunostaining for Ki-67 (Fig 2C)
was exclusively nuclear, while HER2 staining was observed in the
membranes (Fig 2D).
Association of tumor markers with
different tumor subtypes
In Table I, the
clinicopathological characteristics of the 90 patients involved in
the study are described. According to the recent criteria (10), the cases of invasive breast
carcinoma of no special type were classified into four subtypes. In
total, seven (7.7%) tumors were assessed as luminal A subtype, 51
cases (56.7%) were classified as luminal B subtype, 15 tumors
(16.7%) were of the HER2 subtype and 17 cases (18.9%) were
classified into the basal-like (triple negative) subgroup (Table II).
| Table IIBiological subtypes in the group of 90
cases of invasive breast carcinoma of no special type based on the
occurrence of ER, PR and HER2. |
Table II
Biological subtypes in the group of 90
cases of invasive breast carcinoma of no special type based on the
occurrence of ER, PR and HER2.
| Subtypes | Patients, n (%) |
|---|
| Luminal A
(HER2−, ER+, PR+) | 7 (7.7) |
| Luminal B
(HER2+, ER+, PR+) | 51 (56.7) |
| HER2
(HER2+, ER−, PR−) | 15 (16.7) |
| Triple negative
(HER2−, ER−, PR−) | 17 (18.9) |
Immunohistochemical analysis of NUCKS1, Ki-67 and CK
5/6 in the various subtypes of invasive breast carcinoma of no
special type is shown in Table
III. The results demonstrated that NUCKS1 expression was
observed in >86% of luminal B, HER2 and basal-like subtypes,
while in the luminal A subgroup, the reactivity to the specific
antibody was the lowest (42.9%). Ki-67 high expression (Ki-67 index
of >14) was observed in 68 (75.5%) of the examined tumors. Ki-67
was frequently observed in the luminal B subtype (94.1%), whereas
the expression in the HER2 and basal-like subtypes was 60 and
64.7%, respectively. For CK 5/6, immunoreactivity was ~50% in the
HER2 and basal-like subgroups, whereas in the luminal A and B
subtypes, immunoreactivity was 14.3 and 13.7%, respectively.
Distant metastases were found to be most frequent in luminal B
subtypes, while in the luminal A tumors, metastases were not
detected. With regard to the lymph node status, nodal metastases
most frequently occurred in the triple negative group, but were not
observed in the luminal A subtypes.
| Table IIIComparison of the occurrence of NUCKS,
Ki-67, CK 5/6, metastases and the five-year survival rates in the
various subtypes of invasive breast carcinoma of no special type in
the group of 90 patients. |
Table III
Comparison of the occurrence of NUCKS,
Ki-67, CK 5/6, metastases and the five-year survival rates in the
various subtypes of invasive breast carcinoma of no special type in
the group of 90 patients.
| Marker | Luminal A, n (%) | Luminal B, n (%) | HER2, n (%) | Triple negative, n
(%) |
|---|
| NUCKS |
| Positive | 3 (42.9) | 44 (86.3) | 13 (86.7) | 16 (94.1) |
| Negative | 4 (57.1) | 7 (13.7) | 2 (13.3) | 1 (5.9) |
| Ki-67 |
| Positive | 0 (0) | 48 (94.1) | 9 (60.0) | 11 (64.7) |
| Negative | 7 (100) | 3 (5.9) | 6 (40.0) | 6 (35.3) |
| CK 5/6 |
| Positive | 1 (14.3) | 7 (13.7) | 8 (53.3) | 10 (58.8) |
| Negative | 6 (85.7) | 44 (86.3) | 7 (46.7) | 7 (41.2) |
| Metastasis |
| M1 | 0 (0) | 18 (35.3) | 4 (26.7) | 3 (17.6) |
| M0 | 7 (100) | 33 (64.7) | 11 (73.3) | 14 (82.4) |
| Lymph node
involvement |
| Yes | 0 (0) | 27 (52.9) | 9 (60.0) | 13 (76.5) |
| No | 7 (100) | 24 (47.1) | 6 (40.0) | 4 (23.5) |
Association of the various markers with
clinocopathological features
Statistical analysis of the associations between the
various markers and clinicopathological features are presented in
Table IV. NUCKS1 positive
expression was found to be significantly associated with certain
clinicopathological characteristics, including the tumor grade,
lymph node involvement and the presence of distant metastases.
Furthermore, a statistically significant association was observed
between NUCKS1 immunoreactivity and Ki-67 and CK 5/6 positive
expression. However, no association between NUCKS1 immunoreactivity
and other breast cancer markers, including ER, PR and HER2, was
observed.
| Table IVCorrelation between the
clinicopathological features of the tumors and NUCKS
expression. |
Table IV
Correlation between the
clinicopathological features of the tumors and NUCKS
expression.
| | NUCKS
expression | |
|---|
| |
| |
|---|
|
Characteristics | Cases, n | Positive, n
(%) | Negative, n
(%) | P-value |
|---|
| Tumor grading |
| I | 28 | 20 (71.4) | 8 (28.6) | 0.025a |
| II | 30 | 25 (83.3) | 5 (16.7) | |
| III | 32 | 31 (96.6) | 1 (3.1) | |
| Lymph node
involvement |
| Yes | 49 | 46 (93.35) | 3 (6.1) | 0.009b |
| No | 41 | 30 (73.2) | 11 (26.8) | |
| Distant
metastasis |
| Yes | 25 | 25 (100) | 0 (0) | 0.009b |
| No | 65 | 51 (78.5) | 14 (21.5) | |
| ER/PR |
| Positive | 58 | 47 (81.0) | 11 (19.0) | 0.363b |
| Negative | 32 | 29 (90.6) | 3 (9.4) | |
| HER2 |
| Positive | 42 | 34 (81.0) | 8 (19.0) | 0.573a |
| Negative | 48 | 42 (87.5) | 6 (12.5) | |
| Ki-67 |
| Positive | 68 | 61 (89.7) | 7 (10.3) | 0.037a |
| Negative | 22 | 15 (68.2) | 7 (31.8) | |
| CK 5/6 |
| Positive | 26 | 16 (57.7) | 10 (42.3) | <0.001b |
| Negative | 64 | 60 (93.7) | 4 (6.3) | |
A statistically significant association between
NUCKS1 immunoreactivity and grading was identified in the study.
The number of cases with positive NUCKS1 reactivity varied between
71.4% for grade I and 96.9 % for grade III. With regard to the
occurrence of lymph node metastasis, NUCKS1 positive expression was
observed in 93.4% of cases with lymph node involvement. Similarly,
in 100% of the samples where the presence of distant metastasis was
confirmed, NUCKS1 positive expression was also detected. In
addition, the results confirmed that NUCKS1 immunoreactivity was
associated with positive Ki-67 reactivity, with 89.7% of the tumor
samples with positive NUCKS1 expression showing a high Ki-67 index
(14%). With regard to CK 5/6, expression was shown to be negatively
associated with NUCKS1 immunoreactivity, with 93.7% of NUCKS1
positive tumors identified as CK 5/6 negative.
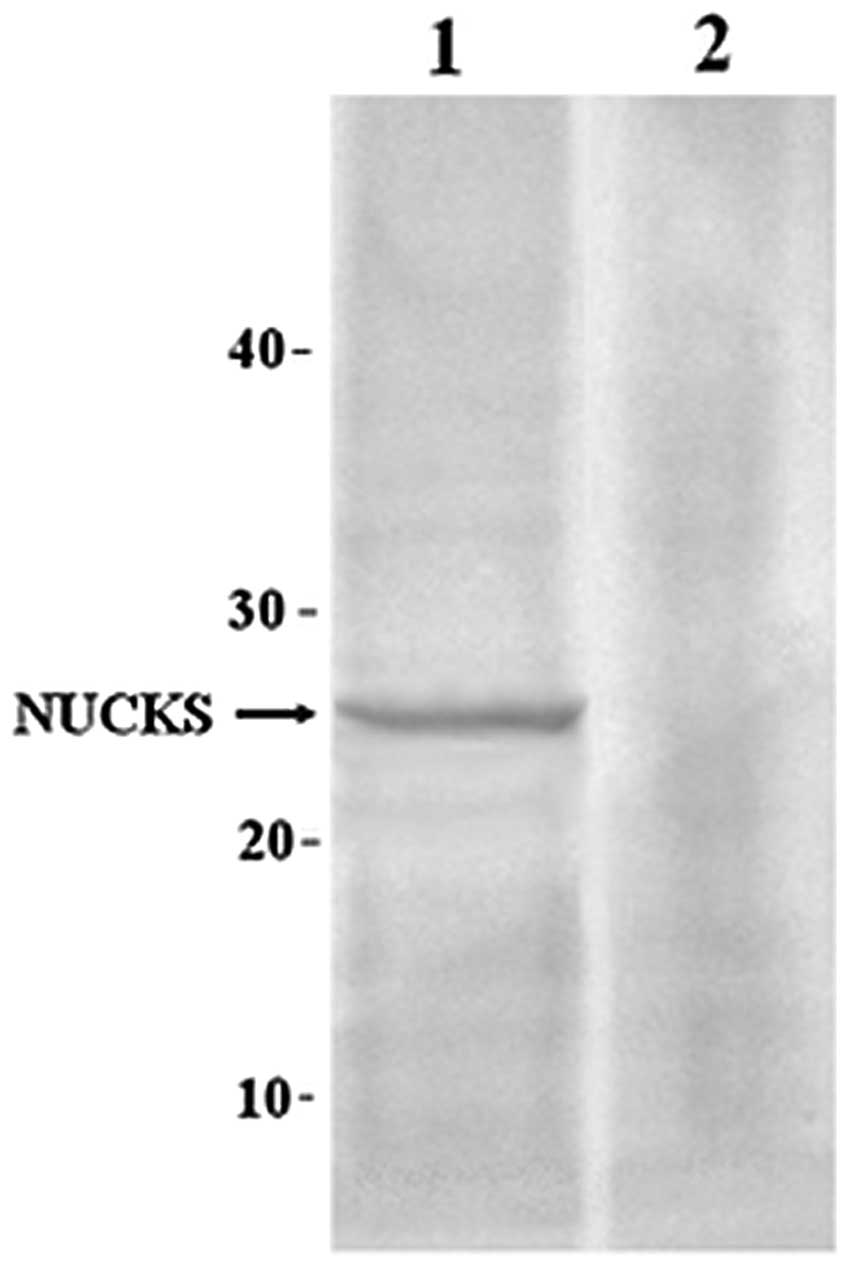
NUCKS1 protein expression
Western blot analysis was used to confirm NUCKS1
expression in FFPE tumor samples and adjacent normal samples.
Strong NUCKS1 overexpression was observed in the samples of
invasive breast carcinoma of no special type when compared with the
adjacent normal tissue (Fig.
3).
Discussion
Novel markers for the evaluation of breast carcinoma
are being increasingly studied (19). Research into novel markers for the
diagnosis of breast cancer has allowed verification of the
prognostic value of the proliferation marker, phosphohistone H3, in
luminal, basal-like and triple negative breast cancers, in which
the histone has been evaluated as the strongest prognostic
indicator in breast cancer (20).
In the present study, a routine immunohistochemical method was used
to analyze the expression of ER, PR, CK 5/6, HER2 and Ki-67, as
well as a novel hypothetical marker, NUCKS1, in 90 cases of
invasive non-specific breast carcinoma. The presence of NUCKS1 in
rapidly growing cells, including breast cancer cells, was
previously confirmed using a variety of biochemical and
immunochemical methods (13,21,22).
The breast cancer classification system proposed by
the St. Gallen International Expert Consensus in 2011 has become
commonly used in clinical practice. Luminal groups were found to be
the most frequent immunohistochemical types in the present study,
which is in accordance with the results of a previous study
(23). To the best of our
knowledge, the present study is the first to investigate NUCKS1
immunoreactivity regarding cell proliferation activity in
immunohistochemistry-based subtypes. The results demonstrated that
NUCKS1 was frequently expressed in all the subgroups of
non-specific invasive breast carcinoma, with the lowest expression
frequency in the luminal A subtype. Furthermore, the Ki-67 antigen
was found to be the most highly expressed in the luminal B group,
which is in accordance with the results of the study by Yanagawa
et al (24).
The triple negative subgroup comprised a
heterogeneous group of breast cancers with various disease courses.
Certain triple negative tumors are more aggressive and have a poor
prognosis, while other triple negative tumors have a better
prognosis compared with hormone receptor positive breast cancers
(25). Our studies have
demonstrated that the triple negative subgroup was positive for
NUCKS in the majority of cases [positive cases 16]. These
observations demonstrate that NUCKS1 may contribute to the
invasiveness of triple negative cancers; however, the results of
the present study require validation by larger cohort studies.
To verify the prognostic value of NUCKS1, the
expression was correlated with clinicopathological features,
including grading, lymph node involvement, distant metastasis and
the presence of other breast cancer markers (PR, ER, HER2, Ki-67
and CK 5/6). In the present study, the overall positive expression
of NUCKS1 was higher compared with the other investigated markers.
In addition, a significant association was observed between NUCKS1
immunoreactivity and grading; low grade carcinoma correlates with
weaker NUCKS1 expression, as compared with high grade carcinoma.
These results indicate that NUCKS1 is involved in the tumor growth
process. Furthermore, a strong association between positive NUCKS1
expression in patients with metastases in the lymph nodes and the
formation of distant metastases (M1) was established, indicating
that this protein may be a novel candidate marker of progression in
invasive breast carcinoma of no special type.
With regard to the well-known breast cancer markers,
an association between NUCKS1 immunoexpression and CK 5/6 and Ki-67
was observed. CK 5/6 is usually found in benign and malignant
tumors of epidermal, squamous mucosal and myoepithelial origins.
High expression levels of CK 5/6 have been reported in breast
adenocarcinoma (26), and are
associated with high histological grade (27), poor prognosis, ER negativity and
younger patient age (28).
Furthermore, according to pathological features, the expression of
basal CKs among triple negative carcinomas defines a more
aggressive group of tumors, regardless of the immunohistochemical
profile (14). However, in the
present study, <60% of triple negative tumors exhibited CK 5/6
immunoreactivity, while NUCKS1 expression was positive in the
majority of the cases. These observations indicate that the
assessment of CK 5/6 and NUCKS1 immunoexpression for triple
negative tumors should be considered. However, in the present
study, only a small number of triple negative tumors were
evaluated; thus, further investigations with a larger number of
samples are required.
Ki-67 is a cellular marker of proliferation, and the
role of Ki-67 as a predictive and prognostic marker in breast
cancer has been widely investigated. Ki-67 expression has been
demonstrated to be associated with poor prognosis and metastatic
potential in a number of tumors, including breast carcinoma
(15). The results of the present
study confirm that NUCKS1 and Ki-67 immunoexpression are
associated, which may indicate a potential role of NUCKS1 in cell
proliferation. In addition, strong NUCKS1 expression was found in
specimens where lymph node involvement and distant metastases were
observed. Furthermore, a significant association between NUCKS1 and
tumor grade was found. These results indicate that poor prognosis
for patients with breast cancer may also depend on NUCKS1 positive
expression; however, further studies are required to confirm this
hypothesis.
In conclusion, the present study has demonstrated
the significance of NUCKS1 expression in the tumor nucleus and the
associations with certain clinicopathological features (nuclear
grading, lymph node involvement and distant metastasis) and Ki-67
and CK 5/6, well-known markers of invasive breast carcinoma of no
special type. These results, along with the results of previous
studies, indicate that immunohistochemical analysis may be a
cost-effective method for determining the prognosis of patients
with breast cancer in a clinical setting. Therefore, NUCKS1 may be
considered as an additional prognostic marker in the
histopathological evaluation of invasive breast carcinoma of no
special type. Furthermore, this novel marker may lead to other
studies investigating new therapeutic strategies.
Acknowledgements
The present study was co-financed by the European
Union as part of the European Social Fund.
References
|
1
|
Grundt K, Haga IV, Aleporou-Marinou V,
Drosos Y, Wanvik B and Østvold AC: Characterization of the NUCKS
gene on human chromosome 1q32.1 and the presence of a homologous
gene in different species. Biochem Biophys Res Comm. 323:796–801.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ostvold AC, Norum JH, Mathiesen S, Wanvik
B, Sefland I and Grundt K: Molecular cloning of a mammalian nuclear
phosphoprotein NUCKS, which serves as a substrate for Cdk1 in vivo.
Eur J Biochem. 268:2430–2440. 2001. View Article : Google Scholar
|
|
3
|
Wiśniewski JR and Schwanbeck R: High
mobility group I/Y: multifunctional chromosomal proteins causally
involved in tumor progression and malignant transformation
(review). Int J Mol Med. 6:409–419. 2000.
|
|
4
|
Fusco A and Fedele M: Roles of HMGA
proteins in cancer. Nat Rev Cancer. 7:899–910. 2007. View Article : Google Scholar
|
|
5
|
Belge G, Meyer A, Klemke M, Burchardt K,
Stern C, Wosniok W, Loeschke S and Bullerdiek J: Upregulation of
HMGA2 in thyroid carcinomas: a novel molecular marker to
distinguish between benign and malignant follicular neoplasias.
Genes Chromosomes Cancer. 47:56–63. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Schaner ME, Ross DT, Ciaravino G, Sorlie
T, Troyanskaya O, Diehn M, Wang YC, Duran GE, Sikic TL, Caldeira S,
Skomedal H, Tu IP, Hernandez-Boussard T, Johnson SW, O’Dwyer PJ,
Fero MJ, Kristensen GB, Borresen-Dale AL, Hastie T, Tibshirani R,
van de Rijn M, Teng NN, Longacre TA, Botstein D, Brown PO and Sikic
BI: Gene expression patterns in ovarian carcinomas. Mol Biol Cell.
14:4376–4386. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kikuchi A, Ishikawa T, Mogushi K, Ishiguro
M, Iida S, Mizushima H, Uetake H, Tanaka H and Sugihara K:
Identification of NUCKS1 as a colorectal cancer prognostic marker
through integrated expression and copy number analysis. Int J
Cancer. 132:2295–2302. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Smalley M and Ashworth A: Stem cells and
breast cancer: a field in transit. Nat Cancer. 3:832–844. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Weigelt B, Geyer FC, Horlings HM, Kreike
B, Halfwerk H and Reis-Filho JS: Mucinous and neuroendocrine breast
carcinomas are transcriptionally distinct from invasive ductal
carcinomas of no special type. Mod Pathol. 22:1401–1414. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Goldhirsch A, Wood WC, Coates AS, Gelber
RD, Thürlimann B and Senn HJ; Panel members. Strategies for
subtypes - dealing with the diversity of breast cancer: highlights
of the St. Gallen international expert consensus on the primary
therapy of early breast cancer 2011. Ann Oncol. 22:1736–1747. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Carey LA, Perou CM, Livasy CA, Dressler
LG, Cowan D, Conway K, Karaca G, Troester MA, Tse CK, Edmiston S,
Deming SL, Geradts J, Cheang MC, Nielsen TO, Moorman PG, Earp HS
and Millikan RC: Race, breast cancer subtypes and survival in the
Carolina Breast Cancer Study. JAMA. 295:2492–2502. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Perou CM, Sørlie T, Eisen MB, van de Rijn
M, Jeffrey SS, Rees CA, Pollack JR, Ross DT, Johnsen H, Akslen LA,
Fluge O, Pergamenschikov A, Williams C, Zhu SX, Lønning PE,
Børresen-Dale AL, Brown PO and Botstein D: Molecular portraits of
human breast tumors. Nature. 406:747–752. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ziółkowski P, Gamian E, Osiecka B, Zougman
A and Wiśniewski JR: Immunohistochemical and proteomic evaluation
of nuclear ubiquitous casein and cyclin-dependent kinases substrate
in invasive ductal carcinoma of the breast. J Biomed Biotechnol.
2009:9196452009.PubMed/NCBI
|
|
14
|
Fernandes RC, Bevilacqua JL, Soares IC,
Siqueira SA, Pires L, Hegg R and Carvalho FM: Coordinated
expression of ER, PR and HER2 define different prognostic subtypes
among poorly differentiated breast carcinomas. Histopathology.
55:346–352. 2009. View Article : Google Scholar
|
|
15
|
Cheang MC, Chia SK, Voduc D, Gao D, Leung
S, Snider J, Watson M, Davies S, Bernard PS, Parker JS, Perou CM,
Ellis MJ and Nielsen TO: Ki-67 index, HER2 status and prognosis of
patients with luminal B breast cancer. J Natl Cancer Inst.
101:736–750. 2009. View Article : Google Scholar
|
|
16
|
Elston CW and Ellis IO: Pathological
prognostic factors in breast cancer. I The value of histological
grade in breast cancer: experience from a large study with
long-term follow-up. Histopathology. 19:403–410. 1991. View Article : Google Scholar
|
|
17
|
Allred DC, Harvey JM, Berardo M and Clark
GM: Prognostic and predictive factors in breast cancer by
immunohistochemical analysis. Mod Pathol. 111:155–168.
1998.PubMed/NCBI
|
|
18
|
McClave JT, Benson PG and Sincich T: A
First Course in Business Statistics. 17th edition. Prentice-Hall,
Inc; New York, NY: 1998
|
|
19
|
Hwang-Verslues WW, Kuo WH, Chang PH, Pan
CC, Wang HH, Tsai ST, Jeng YM, Shew JY, Kung JT, Chen CH, Lee EY,
Chang KJ and Lee WH: Multiple lineages of human breast cancer
stem/progenitor cells identified by profiling with stem cell
markers. PLoS One. 4:e83772009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Skaland I, Janssen EA, Gudlaugsson E, Hui
Ru Guo L and Baak JP: The prognostic value of the proliferation
marker phosphohistone H3 (PPH3) in luminal, basal-like and triple
negative phenotype invasive lymph node-negative breast cancer. Cell
Oncol. 31:261–271. 2009.
|
|
21
|
Grundt K, Skjeldal L, Anthonsen HW, Skauge
T, Huitfeldt HS and Østvold AC: A putative DNA-binding domain in
the NUCKS protein. Arch Biochem Biophys. 407:168–175. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wiśniewski JR, Zougman A, Krüger S,
Ziółkowski P, Pudełko M, Bebenek M and Mann M: Constitutive and
dynamic phosphorylation and acetylation sites on NUCKS, a
hypermodified nuclear protein, studied by quantitative proteomics.
Proteins. 73:710–718. 2008.PubMed/NCBI
|
|
23
|
Bernardi MA, Logullo AF, Pasini FS,
Nonogaki S, Blumke C, Soares FA and Brentani MM: Prognostic
significance of CD24 and claudin-7 immunoexpression in ductal
invasive breast cancer. Oncol Rep. 27:28–38. 2012.PubMed/NCBI
|
|
24
|
Yanagawa M, Ikemot K, Kawauchi S, Furuya
T, Yamamoto S, Oka M, Oga A, Nagashima Y and Sasaki K: Luminal A
and luminal B (HER2 negative) subtypes of breast cancer consist of
a mixture of tumors with different genotype. BMC Res Notes.
5:3762012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cheang MCU, Voduc D, Bajdik C, Leung S,
McKinney S, Chia SK, Perou CM and Nielsen TO: Basal-like breast
cancer defined by five biomarkers has superior prognostic value
than triple-negative phenotype. Clin Cancer Res. 14:1368–1376.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chu PG and Weiss LM: Expression of
cytokeratin 5/6 in epithelial neoplasms: an immunohistochemical
study of 509 cases. Mod Pathol. 15:6–10. 2012.
|
|
27
|
Khilko N, Wang J, Wei B, Hicks DG and Tang
P: Invasive lobular carcinomas do not express basal cytokeratin
markers CK 5/6, CK 14 and CK 17. Breast Cancer (Auckl). 21:49–55.
2010.PubMed/NCBI
|
|
28
|
Abd El-Rehim DM, Pinder SE, Paish CE, Bell
J, Blamey RW, Robertson JF, Nicholson RI and Ellis IO: Expression
of luminal and basal cytokeratins in human breast carcinoma. J
Pathol. 203:661–671. 2004.PubMed/NCBI
|