Introduction
Sensory Guillain-Barré syndrome (GBS) is an acute
demyelinating neuropathy that presents clinically with involvement
of the sensory peripheral nerve only. However, the existence of a
purely sensory form of GBS remains subject to controversy, since
these cases always demonstrate a degree of motor weakness or
abnormalities in motor nerve conduction studies (NCSs) and are
difficult to distinguish from acute sensory neuronopathy (1). To date, only a few cases of pure
sensory GBS have been reported (2–4),
with the majority of cases being anecdotal and few studies
describing a peripheral nerve pathology. Thus, the clinical and
pathological features of sensory variant GBS have not been well
characterized, and reduced awareness of these features has resulted
in delays in the diagnosis and treatment.
The current study reports the case of a 43-year-old
female who presented with symptoms consistent with a diagnosis of
pure sensory GBS. The patient exhibited satisfactory improvements
following one course of intravenous immunoglobulin. Diagnosing
sensory GBS is important since immunotherapy may positively
influence the prognosis, in contrast to the slow but steady
progression associated with idiopathic sensory neuropathy or
paraneoplastic sensory neuronopathy. Therefore, understanding the
pathological and clinical features may aid in the diagnosis of
complicated clinical cases and prevent unnecessary procedures.
Case report
A 43-year-old female developed numbness of the
distal lower limbs that extended to all the limbs over four days,
and was admitted to the First Affiliated Hospital of Dalian Medical
University (Dalian, China) on April 26, 2011. The patient
experienced nonspecific flu-like symptoms and suffered from a mild
sore throat during the two weeks prior to admission. After a few
days, the patient developed numbness on the soles of both feet,
which progressed over two days to the knees; thus, the patient had
difficulty with walking due to poor balance. Subsequently, the
patient had a markedly unsteady gait and tingling sensations in the
distal lower limbs, which increased in intensity and extended more
widely. Clumsiness in the upper limbs and pseudoathetosis was
observed occasionally. The time when the symptoms of the disease of
the patient had reached their peak was achieved within three
weeks.
Routine laboratory tests were conducted on the
second day following admission. Cerebrospinal fluid (CSF) routing
revealed 1,194 mg/l of protein and a cell count of
2×106/l, while other issues were normal. Routine NCSs
revealed absent sensory potentials, while the motor NCS was normal
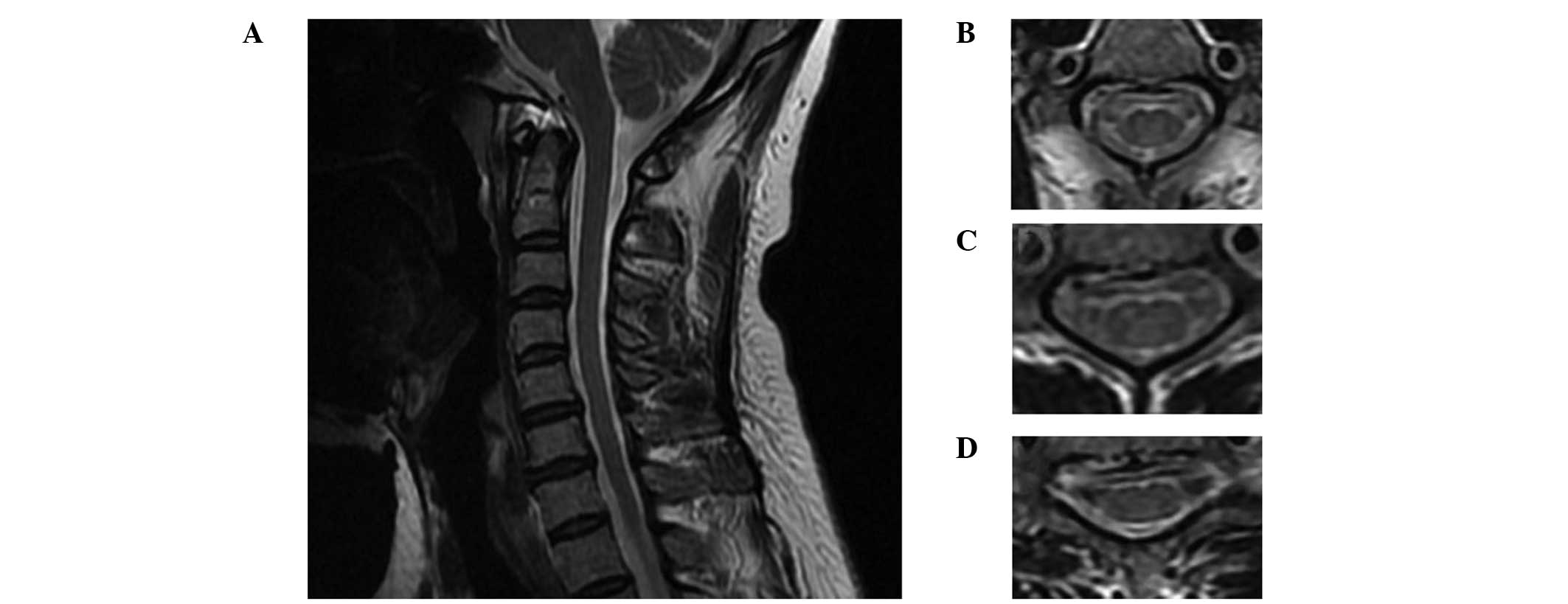
(Fig. 1). Sagittal T2-weighted
magnetic resonance imaging (MRI) scans (Fig. 2) of the cervical spine revealed a
normal appearance of the posterior column, despite a number of disc
osteophyte complexes with mild central canal stenosis at the
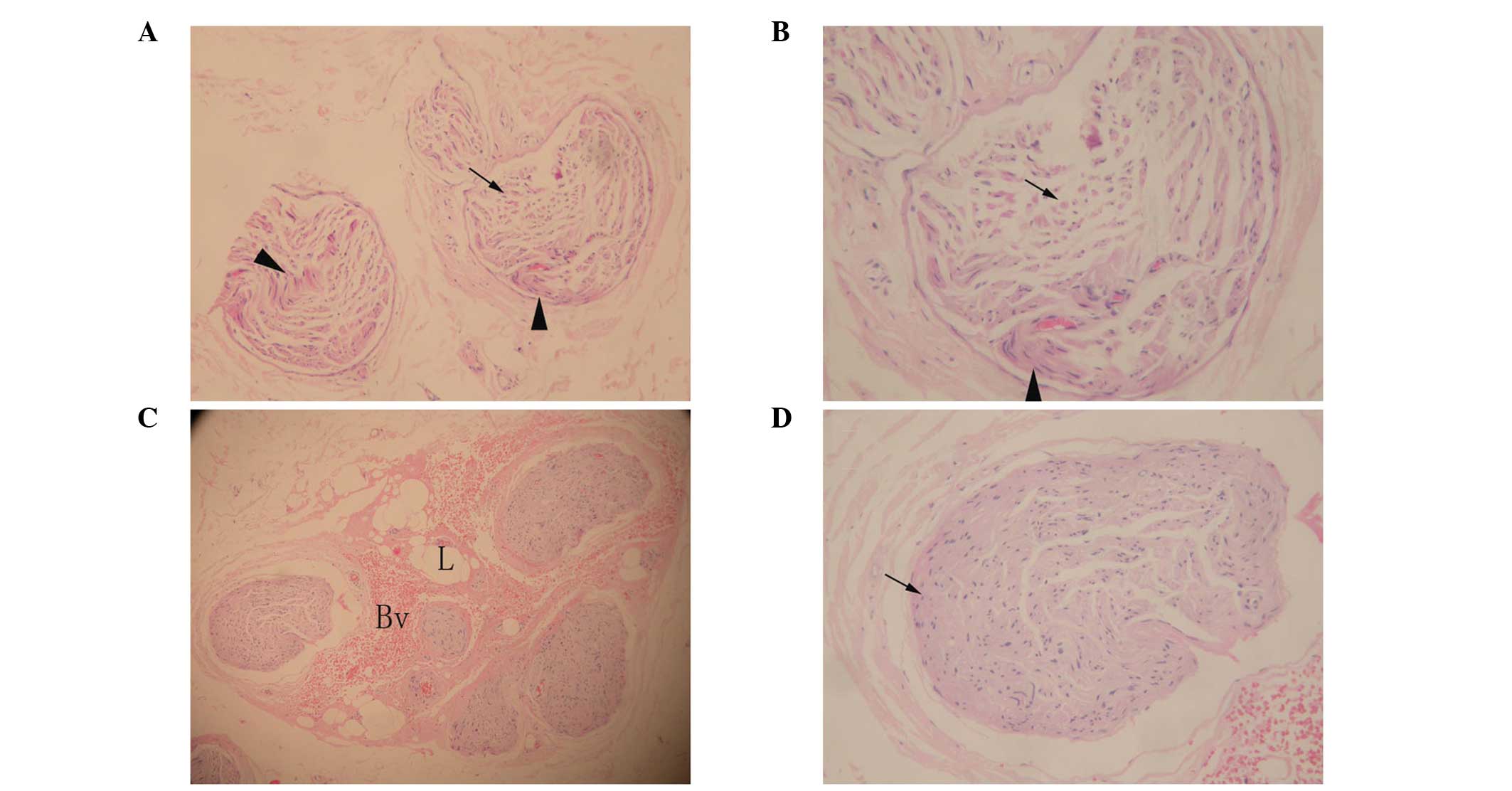
cervical level. Pathological observations of the sural nerve biopsy
were conducted. Light microscopy (Fig.
3) showed moderate subperineurial edema, mild loss of
myelinated fibers and a few thinly myelinated fibers without
inflammatory changes. In particular, the form of regenerated nerve
fibers have complete structure of myelinated nerve fascicles, and
these myelinated nerve fibers are thicker than other parts of the
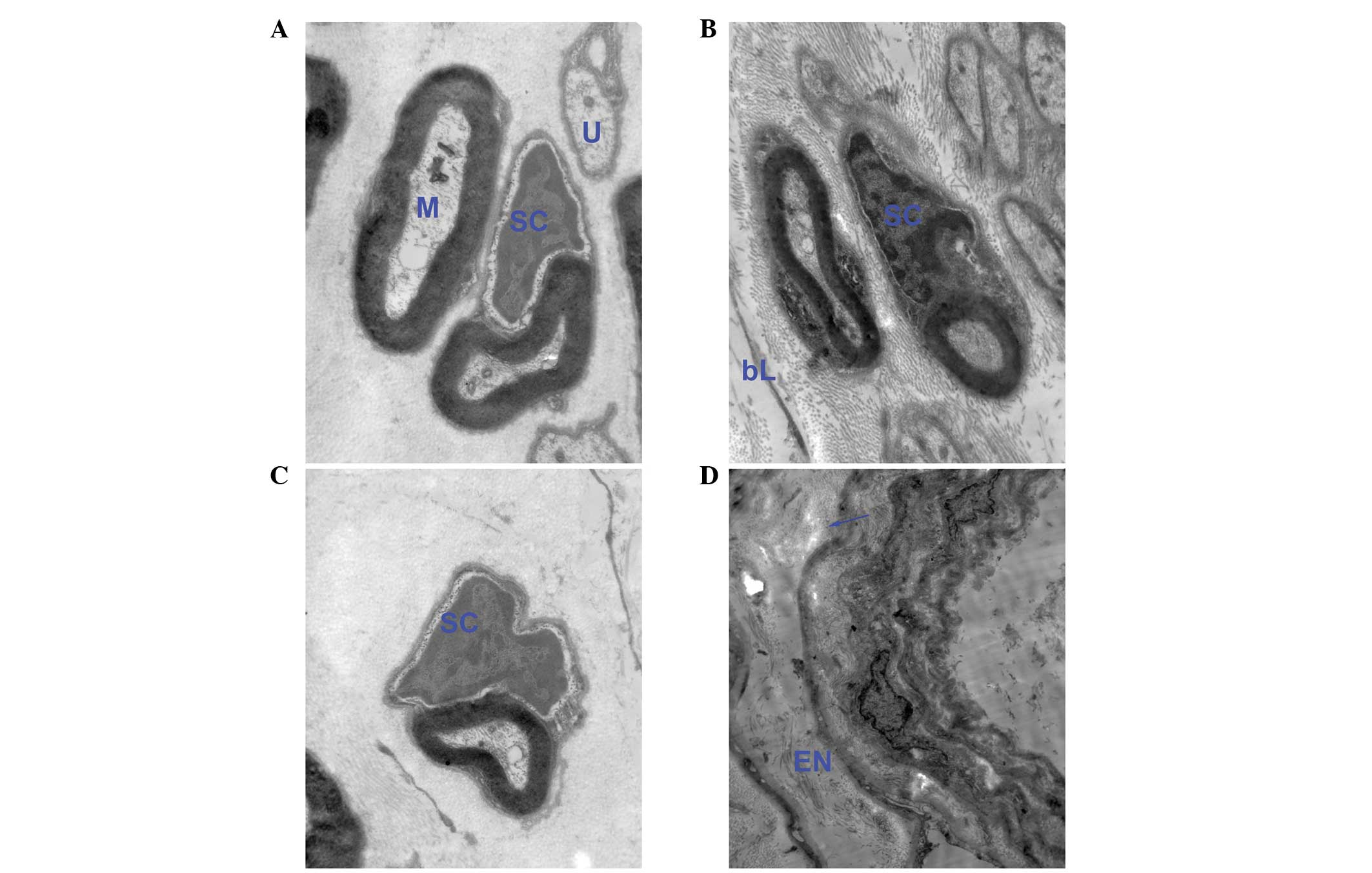
biopsy. Electron microscopy (Fig.
4) revealed normal myelinated and unmyelinated axons, however,
the Schwann cell nucleui were broken down and the cytoplasm of the
Schwann cells were pale watery moderately.
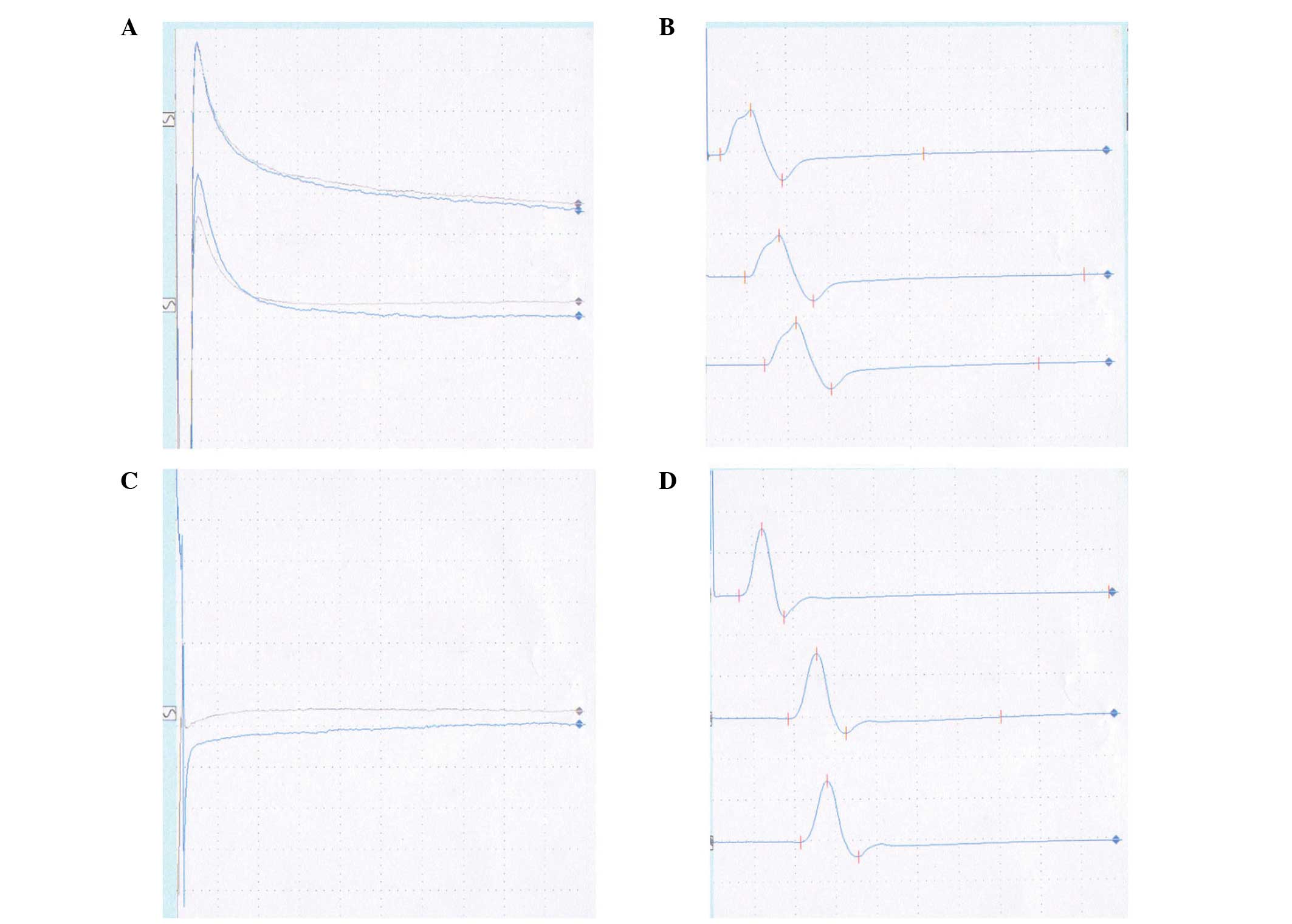 | Figure 1Results from the NCSs showing (A)
sensory, left ulnar, absent sensory potentials, (B) motor, left
ulnar, normal motor potentials, (C) sensory, right sural, absent
sensory potentials and (D) motor, right peroneal, normal motor
potentials. NCSs, nerve conduction studies. |
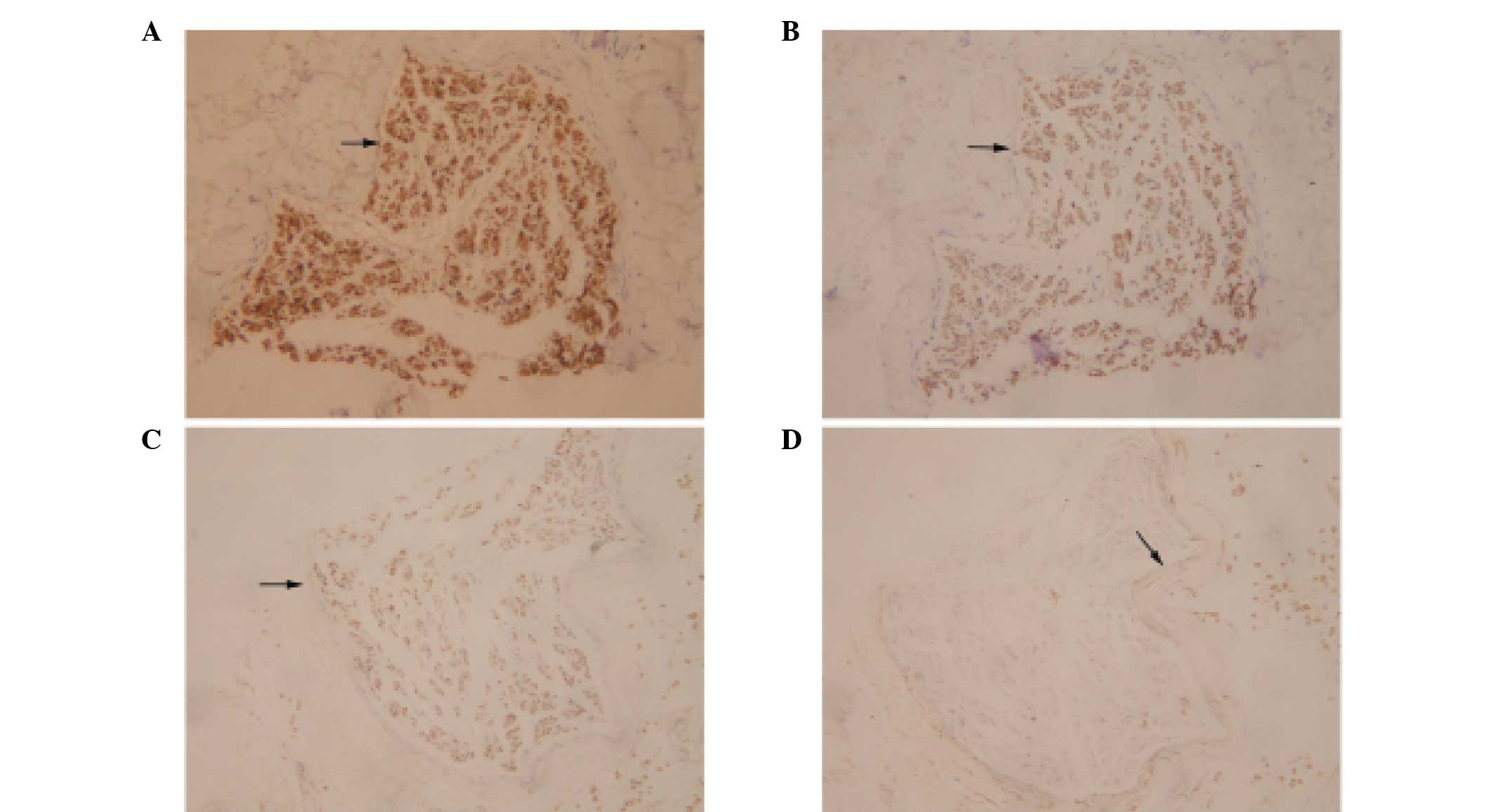
Immunohistochemical analysis (Fig. 5) demonstrated that the majority of
the cells within the nerve fascicles were strongly positive for
S-100, moderately positive for neuron-specific enolase (NSE) and
mildly positive for neurofilament (NF), while the perineurium was
mildly positive for epithelial membrane antigen (EMA). No
anatomical abnormalities were observed and the density of the
fibers moderately decreased.
Following intravenous immunoglobulin refusion
treatment, the patient was administered one course of small-dose
(20 mg/day) prednisone, but without any benefit. Next, the patient
received a five-day course of intravenous immunoglobulin (400
mg/kg/day). The clinical symptoms, including numbness and ataxia,
began to improve two weeks after admission. Follow-up examinations
for 30 months revealed only generalized areflexia without
ataxia.
Discussion
Wartenberg (3)
discussed the concept of a sensory equivalent to the ascending
paralysis of GBS in 1958, while the study by Asbury (5) provided diagnostic criteria for a
sensory loss and areflexia variant in 1981. However, whether their
clinical and electrodiagnostic features are pathognomonic of acute
sensory neuronopathy or sensory GBS remains controversial. To date,
reported clinical cases meeting these criteria have been scarce,
for which there are two main reasons. Firstly, these cases always
demonstrate a degree of motor weakness or abnormalities in motor
NCSs, which suggests that the cases are predominantly sensory GBS,
rather than purely sensory GBS. Secondly, acute sensory neuropathy
represents two clinical syndromes: Acute sensory neuronopathy
involving the dorsal root ganglia and sensory GBS, an acute
demyelinating neuropathy that presents clinically with involvement
of the sensory peripheral nerve only. The total protein in the CSF
is not useful for distinguishing sensory GBS from sensory
neuronopathy since the protein level may be elevated in the two
disorders.
Demonstrating electrophysiological evidence of
sensory demyelination in GBS may be difficult, with the exception
of usual presentation, where there is evidence of demyelination on
motor NCSs (4). Sensory
neuronopathy can be differentiated by the absent sensory nerve
action potentials in the presence of normal motor conduction
(6). In the present case, the
regenerated nerve fibers were observed via light microscopy of the
sural nerve specimen and the sagittal T2-weighted MRI scan of the
cervical spine, which demonstrated a normal appearance of the
posterior column.
Furthermore, immunohistochemical analysis of the
sural nerve specimen may be useful in distinguishing sensory GBS
from sensory neuronopathy (7). NF,
NSE and S-100b proteins are nervous system-specific proteins
(8), and EMA is a
perineurial-specific protein. An increase in NF and NSE levels
reflect axonal damages in radices, while that of S-100b indicates
Schwann cell damage associated with demyelination. A number of
studies have indicated that the majority of patients with normal
NSE and S-100b levels demonstrate a good recovery, while markedly
high levels of NSE are associated with long-term recovery and
residual disability (9,10,11,12,13).
An additional study demonstrated that high NF levels in the CSF,
indicating proximal axonal damage, at disease onset are a robust
predictor of poor motor recovery (14).
In the present study, immunohistochemical analysis
revealed that the majority of cells within the nerve fascicles were
strongly positive for S-100, moderately positive for NSE and mildly
positive for NF, while the perineurium was mildly positive for EMA.
Moderate positivity for NSE and mild positivity for NF indicated
that the axonal damages were not in radices, while the strong
positivity for S-100 indicated Schwann cell damage associated with
demyelination. In addition, electron microscopy revealed normal
myelinated and unmyelinated axons with Schwann cell nucleus
breakdown, which confirmed the outcome of the immunohistochemical
analyses. Furthermore, the perineurial cell proliferated and
retained its EMA immunoreactivity within the dermal nerve sheath
myxomas, Morton’s metatarsalgia and traumatic neuromas. It should
be possible to immunohistochemically ‘dissect’ the structure of the
peripheral nerve and its lesions by EMA and S-100, since EMA is
used to indicate perineurial cells and S-100 to identify Schwann
cells (15). In the present study,
the perineurium revealed strong S-100 protein expression but mild
EMA immunoreactivity, which may reflect normal perineurial
structures or a mild lesion.
In conclusion, the aforementioned observations
indicated that the present case was most likely pure sensory GBS,
not sensory neuronopathy; thus, had a good prognosis. However, mild
numbness and generalized areflexia symptoms remained with the
patient. This is characteristic of GBS, which residual sensory
deficit is present in a considerable number of patients and
frequently has a disruptive effect, even several years following
the onset of GBS (16).
Acknowledgements
The authors are grateful to all the individuals
participating in the present study. The study would not have been
possible without the cooperation of the patient and her families.
The authors would like to thank all the doctors from the
Departments of Neurology of the First Affiliated Hospital of Dalian
Medical University (Dalian, Liaoning, China) for the help and
suggestions provided in the diagnosis and treatment of the
patient.
References
|
1
|
Lee SS and Lee SH: Does sensory
Guillain-Barré syndrome exist without any abnormalities in motor
nerve conduction? Neurology. 66:947–948. 2006.
|
|
2
|
Miralles F, Montero J, Reñe R and Martinez
Matos JA: Pure sensory Guillain-Barré syndrome. J Neurol Neurosurg
Psychiatry. 55:411–412. 1992.
|
|
3
|
Wartenberg R: Sensory polyneuritis.
Neuritis, Sensory Neuritis, Neuralgia. Oxford University Press; New
York, NY: pp. 160–162. 1958
|
|
4
|
Oh SJ, LaGanke C and Claussen GC: Sensory
Guillain-Barré syndrome. Neurology. 56:82–86. 2001.
|
|
5
|
Asbury AK: Diagnostic considerations in
Guillain-Barré syndrome. Ann Neurol. (9 Suppl): 1–5. 1981.
|
|
6
|
Kuntzer T, Antoine JC and Steck AJ:
Clinical features and pathophysiological basis of sensory
neuronopathies (ganglionopathies). Muscle Nerve. 30:255–268. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Maxwell GD, Whitehead MC, Connolly SM and
Marangos PJ: Development of neuron-specific enolase
immunoreactivity in avian nervous tissue in vivo and in vitro.
Brain Res. 255:401–418. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Stefansson K, Wollmann RL and Moore BW:
Distribution of S-100 protein outside the central nervous system.
Brain Res. 234:309–317. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mokuno K, Kiyosawa K, Sugimura K, Yasuda
T, Riku S, Murayama T, Yanagi T, Takahashi A and Kato K: Prognostic
value of cerebrospinal fluid neuron-specific enolase and S-100b
protein in Guillain-Barré syndrome. Acta Neural Scand. 89:27–30.
1994.PubMed/NCBI
|
|
10
|
Parry GJ and Sumner AJ: Diseases of the
peripheral nervous system. Evans RW, et al: Prognosis of
neurological disorders New York: Oxford University Press; pp.
375–380. 1992
|
|
11
|
Gibbels E and Giebisch U: Natural course
of acute and chronic monophasic inflammatory demyelinating
polyneuropathies (IDP). A retrospective analysis of 266 cases. Acta
Neurol Scand. 85:282–291. 1992. View Article : Google Scholar
|
|
12
|
de Jager AE and Minderhoud JM: Residual
signs in severe Guillain-Barré syndrome: analysis of 57 patients. J
Neurol Sci. 104:151–156. 1991.PubMed/NCBI
|
|
13
|
Winer JB, Hughes RA, Greenwood RJ, Perkin
GD and Healy MJ: Prognosis in Guillain-Barré syndrome. Lancet.
1:1202–1203. 1985.
|
|
14
|
Petzold A, Brettschneider J, Jin K, Keir
G, Murray NM, Hirsch NP, Itoyama Y, Reilly MM, Takeda A and Tumani
H: CSF protein biomarkers for proximal axonal damage improve
prognostic accuracy in the acute phase of Guillain-Barré syndrome.
Muscle Nerve. 40:42–49. 2009.PubMed/NCBI
|
|
15
|
Theaker JM and Fletcher CD: Epithelial
membrane antigen expression by the perineurial cell: further
studies of peripheral nerve lesions. Histopathology. 14:581–592.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bernsen RA, Jager AE, Schmitz PI and van
der Meché FG: Long-term sensory deficit after Guillain-Barré
syndrome. J Neurol. 248:483–486. 2001.PubMed/NCBI
|