Introduction
Urolithiasis is a common urinary disease, with
increasing incidence worldwide. The occurrence of urolithiasis
varies among geographical regions and ethnic groups. A high
incidence of urolithiasis has been observed in Xinjiang, China,
particularly among the Uyghur population of south Xinjiang that
follows a high-fat diet. High levels of blood lipids have been
reported to affect lipid metabolism and may be a risk factor for
urolithiasis (1,2). Blood lipid levels are affected by
genetic factors and lifestyle, and lipid metabolism processes are
regulated by a set of genes. Different blood lipid levels have been
detected among ethnic groups as early as childhood, which indicates
that the differences may be based on genetic factors (3). In addition, genetic factors have been
identified as a possible cause of a number of abnormalities in
blood lipid metabolism (4). The
present study focused on the apolipoprotein E (ApoE) gene, which is
one of the components of plasma lipoproteins. ApoE regulates blood
lipid metabolism by binding with a receptor protein (5). Epidemiological investigations have
revealed that ApoE gene polymorphisms are closely associated with
lipid metabolism abnormalities (6).
ApoE is a major plasma lipoprotein that plays an
important role in lipoprotein metabolism. Lipoproteins with
different ApoE isomers have been reported to exhibit distinct
kinetic characteristics and affect the blood lipid levels
differently (7). Kong et al
(8) reported that cholesterol
crystallization in the gall bladder was associated with ApoE
polymorphism, and hypothesized that ApoE may be a promoter of
nucleation, and thus, a susceptibility factor for cholesterol
crystallization in the gall bladder. In the present study, lipid
metabolism was investigated in urolithiasis patients among the
Uyghur population. Using polymerase chain reaction-restriction
fragment length polymorphism (PCR-RFLP) analysis, the associations
between ApoE gene polymorphisms and lipid metabolism abnormalities
were analyzed.
Materials and methods
Subjects
In total, 90 Uyghur patients with urolithiasis from
the Aksu Prefecture, hospitalized between January and July 2007,
were enrolled in this study (male, 51; female, 39; age range, 7–67
years). In addition, 90 healthy Uyghur individuals with no blood
relation to the patients were randomly selected as the control
group (male, 51; female, 39; age range, 8–69 years). Individuals
from the control group had similar occupations and resided in the
same area as the patient group individuals. B-type ultrasonography
was performed to ensure that the control group did not suffer from
a urinary calculus or any other relevant diseases. Patients
diagnosed with a urinary calculus who did not undergo removal of
the calculus, even following extracorporeal shock wave lithotripsy,
as well as patients with chronic urinary infections and renal
insufficiency, were excluded from the study. Qualitative analysis
of the calculus components was conducted using standard calculus
qualitative analytical chemical reagents supplied by the Institute
of Urology, Peking University (Peking, China). The reagents
included calcium phosphate, calcium oxalate, ammonium magnesium
phosphate, uric acid, carbapatite, and cystine. The stone samples
were powdered and analyzed by Fourier transform infrared
spectrophotometry (Tensor 27; Bruker Optics GmbH, Ettlingen,
Germany).
Prior written and informed consent was obtained from
all the patients and the study was approved by the Ethics Review
Board of Shihezi University (Shihezi, China).
Measurement of blood lipid profiles
Blood lipids levels were analyzed on an Olympus
AU400 Automated Chemistry analyzer (Olympus Optical Co., Ltd.,
Tokyo, Japan). Blood samples were collected from the
peripheral vein of each individual without fasting and frozen in
liquid nitrogen. Aliquots of frozen serum were thawed on ice for 2
h. The samples were thus frozen and thawed twice in total. Lipid
metabolites were extracted from 100 μl of serum. Blood levels of
cholesterol and triglycerides were analyzed in the patients and
control groups using the cholesterol oxidase method. In addition,
the levels of apolipoprotein A-I and total lipoprotein were
determined by an immunoturbidimetric assay. The levels of
high-density lipoprotein and low-density lipoprotein were measured
using a routine Hitachi 7600 autoanalyzer (Hitachi
High-Technologies Corporation, Tokyo, Japan).
PCR-RFLP analysis
A 5-ml blood sample was collected from the
peripheral vein of each individual and was anticoagulated with
EDTA. DNA was extracted from the blood sample using a Genomic DNA
Extraction kit (Sangon Biotech Co., Ltd., Shanghai, China),
according to the manufacturer’s instructions. The ApoE gene was
amplified in a total volume of 30 μl. The primerswere synthesized
by Sangon Biotech Co., Ltd. and their sequences as follows:
forward: 5′-ACA GAA TTC GCC CCG GCC TGG TAC AC-3′ and reverse:
5′-TAA GCT TGG CAC GGC TGT CCA AGG A-3′. Each PCR cycle included 3
μl 10X PCR buffer (with 15 mM MgCl2), 2 units Taq
DNA polymerase (Takara Bio, Inc., Tokyo, Japan), 2 μl dNTP (2.5
mM), 0.4 μl each of the forward and reverse primers (20 mM) and
0.5–0.6 μg DNA templates. The following PCR procedure was used:
initial denaturation at 97°C for 7 min; 35 cycles of denaturation
at 95°C for 45 sec; annealing at 65°C for 45 sec and extension at
72°C for 1 min; and a final extension at 72°C for 10 min. PCR was
performed in a C1000 Touch™ PCR thermal cycler (Bio-Rad,
Hercules, California, USA)
Following PCR, a 1-μg sample of the ApoE gene
amplification product was digested with 20 μl restriction
endonuclease (Sangon Biotech Co., Ltd.). Following digestion, the
DNA fragments were separated by electrophoresis on a polyacrylamide
gel for 2 h at 90 V. The genotypes were identified using a Gel
Doc™ XR gel imaging and analysis system (Bio-Rad). A
sample was randomly selected from each genotype identified during
the RFLP analysis, and sequenced by Sangon Biotech Co., Ltd.
Statistical analysis
The frequencies of the genotypes and gene alleles
were calculated separately in the patient and control groups using
a gene counting method as described previously (9). The data were tested for
Hardy-Weinberg equilibrium and statistical analysis was performed
using SPSS 17.0 software (SPSS, Inc., Chicago, IL, USA). The
genotypic and allelic differences between the control and patient
groups were examined with the χ2 test, where P<0.05
was considered to indicate a statistically significant
difference.
Results
Analysis of calculus composition
To determine the percentage of each component in the
calculi of the patients, calculus composition was analyzed using
standard calculus qualitative analytical chemical reagents. The
results indicated that the major component of the calculi was
calcium oxalate in 90.0% of the patients (81/90). Among the 81
patients with calcium oxalate calculi, the calculus composition
detected was as follows: Pure calcium oxalate (67.9%, 55/81);
calcium oxalate and calcium phosphate (4.9%, 4/81); calcium oxalate
and ammonium magnesium phosphate (2.5%, 2/81); calcium oxalate and
uric acid or ammonium urate (18.5%, 15/81); calcium oxalate,
ammonium magnesium phosphate and dahllite (2.5%; 2/81); calcium
oxalate and dahllite (2.5%, 2/81); and calcium oxalate and cystine
(1.2%, 1/81). Among the other nine urolithiasis cases, the calculus
composition included pure calcium phosphate (2.2%, 2/90), pure uric
acid (5.6%, 5/90) and pure ammonium magnesium phosphate (2.2%,
2/90). These results indicated that the major component of calculi
in urolithiasis cases among the Uyghur population of south Xinjiang
was calcium oxalate.
Number of cases with abnormal levels of
total cholesterol, triglycerides and high-density lipoproteins is
higher in urolithiasis patients
Blood lipid levels were measured to investigate the
role of blood lipids in urolithiasis. The blood lipids detected
included total cholesterol, triglycerides, high-density
lipoproteins, low-density lipoproteins, apolipoprotein A-I and
lipoproteins. As shown in Table I,
abnormal levels of total cholesterol were detected in 38
urolithiasis patients (42.2%) and 21 individuals from the control
group (23.3%). In addition, abnormal levels of triglycerides were
observed in 33 patients (36.7%) and 15 cases from the control group
(16.7%). In total, 29 cases (32.2%) in the patient group exhibited
abnormal levels of high-density lipoproteins, whereas abnormal
levels were detected in only 16 cases from the control group
(17.8%). Abnormal levels of apolipoprotein A-I were detected in 67
cases (74.4%) in the patient group and 60 cases (66.7%) in the
control group. The number of cases exhibiting abnormal levels of
low-density lipoproteins was 57 in the patient group (63.3%) and 53
in the control group (58.9%). Only one case (1.1%) was detected
with abnormal levels of lipoproteins in the patient group, while no
cases were detected in the control group. Statistically, the number
of cases with abnormal levels of total cholesterol, triglycerides
and high-density lipoproteins was significantly higher in the
patient group when compared with the control group. However, the
difference in the number of cases with abnormal levels of
apolipoprotein A-I, low-density lipoproteins and lipoproteins
between the two groups was not found to be statistically
significant. These results indicated that dyslipidemia may be a
significant factor in the development of urolithiasis among the
Uyghur population of south Xinjiang.
 | Table IBlood lipid level analysis in the
patient and control groups. |
Table I
Blood lipid level analysis in the
patient and control groups.
| Patient group, n
(n=90) | Control group, n
(n=90) | | |
|---|
|
|
| | |
|---|
| Parameters | Normal | Abnormal | Normal | Abnormal | χ2 | P-value |
|---|
| Total
cholesterol | 52 | 38 | 69 | 21 | 7.287 | 0.007a |
| Triglycerides | 57 | 33 | 71 | 19 | 5.300 | 0.021a |
| High-density
lipoproteins | 61 | 29 | 74 | 16 | 5.007 | 0.025a |
| Low-density
lipoproteins | 33 | 57 | 37 | 53 | 0.374 | 0.541 |
| Apolipoprotein
A-I | 23 | 67 | 30 | 60 | 1.310 | 0.252 |
| Lipoproteins | 89 | 1 | 90 | 0 | | |
Associations between ApoE gene
polymorphisms and the occurrence of urolithiasis
To determine the associations between the
polymorphisms of ApoE and the occurrence of urolithiasis, ApoE gene
polymorphisms were analyzed using PCR-RFLP. The ApoE gene was
successfully amplified in the 180 subjects (90 patients and 90
controls) and the product size of the gene was 244 bp. In theory,
due to the presence of different bases at sites 112 and 158 of the
ApoE gene, three alleles and six genotypes can be generated
following digestion with the Hha I restriction endonuclease.
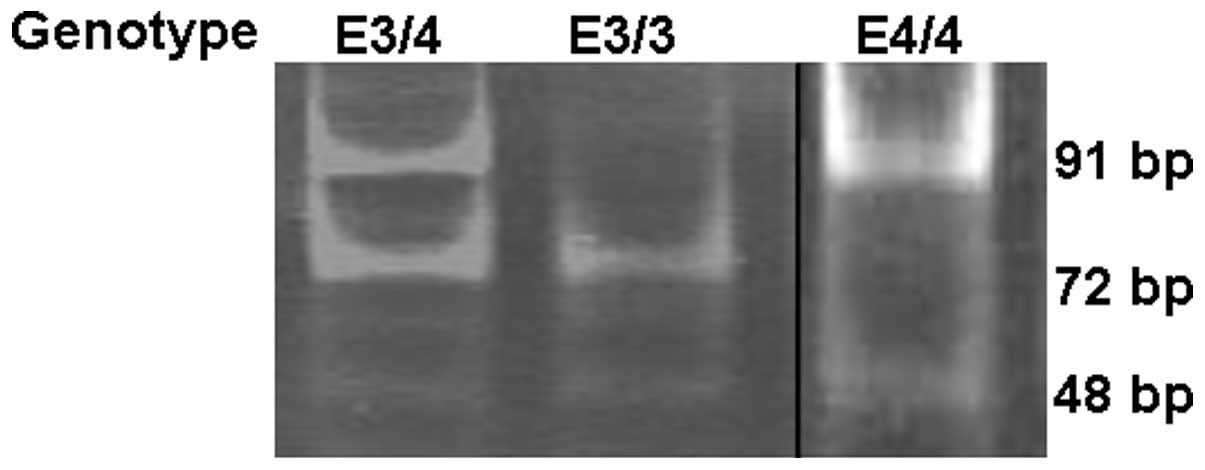
However, in this study, only three genotypes were identified in the
subjects, namely, the E3/3, E4/4 and E3/4 genotypes (Fig. 1). Through Hardy-Weinberg
equilibrium testing, these genotypes of ApoE were found to be
consistent with the theoretical expectations.
The associations between ApoE gene polymorphisms and
the occurrence of urolithiasis were analyzed. As shown in Table II, 28 cases with E3/3 (30.1%), 58
cases with E3/4 (64.4%) and four cases with the E4/4 genotype
(4.5%) were detected in the patient group. By contrast, 52
individuals with E3/3 (57.8%), 35 individuals with E3/4 (38.9%) and
three individuals with the E4/4 genotype (3.3%) were identified in
the control group. The frequency of the E3/4 genotype in the
patient group was significantly higher when compared with the
control group (χ2=12.96; P<0.001). The number of E3
and E4 alleles in the patient group was 114 (64.8%) and 62 (35.2%),
respectively, while the number of these alleles in the control
group was 139 (79.0%) and 41 (21.0%), respectively. Statistically,
the frequency of the E4 allele in the patient group was
significantly higher when compared with the control group
(χ2=6.61; P<0.025). The results indicated that the
E3/4 genotype and E4 allele may be susceptibility factors for
urolithiasis among the Uyghur population of south Xinjiang.
| Table IIAssociations between ApoE gene
polymorphisms and the occurrence of urolithiasis. |
Table II
Associations between ApoE gene
polymorphisms and the occurrence of urolithiasis.
| Genotype frequency, %
(n) | Allele frequency, %
(n) |
|---|
|
|
|
|---|
| Group | E3/3 | E3/4 | E4/4 | E2 | E3 | E4 |
|---|
| Patient | 30.1 (28) | 64.4a (58) | 4.5 (4) | 0 | 64.8 (114) | 35.2b (62) |
| Control | 57.8 (52) | 38.9 (35) | 3.3 (3) | 0 | 79.0 (139) | 21.0 (41) |
Discussion
The occurrence of urolithiasis has been shown to
increase with age and the increasing incidence of obesity (10). In addition to the high risk of
developing obesity, coronary heart disease, dyslipidemia and
abnormal glucose tolerance, individuals with metabolic syndromes
also experience a high risk of urolithiasis (11). Zhang (12) reported that high levels of
triglycerides, high-density lipoproteins, cholesterol and ApoE in
the blood were risk factors for developing urolithiasis. Clinical
control of urolithiasis may relieve the symptoms, promote the
removal of calculi, lower the risk of recurrence and reduce the
effect on the kidneys. Accordingly, the present study revealed that
the levels of triglycerides, high-density lipoproteins and
cholesterol were significantly higher in the urolithiasis patient
group when compared with the control group.
A previous study demonstrated that ApoE
polymorphisms were associated with human longevity in a Han Chinese
population (13). In the current
study, however, the association between ApoE polymorphisms and the
age of the patients was not analyzed. In another study, the allele
frequencies of the ApoE polymorphism in Zambian populations were
13.8, 59.5 and 26.7% for the E2, E3 and E4 alleles, respectively
(14). Genotype frequencies of
E3/3 were 32.8% in Zambian populations. The allele and genotype
frequencies in Uyghur populations were different to those in
Zambian populations. This may be due to the difference in ethnic
background.
In the present study, the polymorphisms of ApoE were
investigated among the Uyghur population of south Xinjiang using
PCR-RFLP analysis. The number of cases with the E3/4 genotype was
significantly higher in the patient group when compared with the
control group (χ2=12.96; P<0.001). In addition, the
number of cases with the E4 allele was significantly higher in the
patient group when compared with the control group
(χ2=6.61; P<0.025). Therefore, the E4 allele of the
ApoE gene may be used as a potential indicator in the diagnosis and
screening of urolithiasis.
Acknowledgements
This study was supported by a grant from the
Xinjiang Production and Construction Corps Doctor Fund (no.
2007JC14).
References
|
1
|
Gu Y, Wang GZ, He W, Zhang J, Yang JW,
Yang F and Ye M: Analysis of relative factors of urinary stones
between patients of urinary stone and the health people in Shanghai
Pudong area. Lin Chang Mi Niao Wai Ke Za Zhi. 26:702–705. 2011.(In
Chinese).
|
|
2
|
Li LD: A primer on causes, prevention and
treatment of urolithiasis. Hang Kong Hang Tian Yi Xue Za Zhi.
22:688–689. 2011.(In Chinese).
|
|
3
|
Ye RG: Dyslipidemia and
Dyslipoproteinemia. Internal Medicine. 5th Edition. People’s
Medical Publishing House; Beijing: pp. 834–837. 2002
|
|
4
|
Wilkinson IB, Prasad K, Hall IR, et al:
Increased central pulse pressure and augmentation index in subjects
with hypercholesterolemia. J Am Coll Cardiol. 39:1005–1011. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Evans RM, Hui S, Perkins A, Lahiri DK,
Poirier J and Farlow MR: Cholesterol and APOE genotype interact to
influence Alzheimer disease progression. Neurology. 62:1869–1871.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lin SK, Kao JT, Tsai SM, Tsai LY, Lin MN,
Lai CJ and Zhong WL: Association of apolipoprotein E genotypes with
serum lipid profiles in a healthy population of Taiwan. Ann Clin
Lab Sci. 34:443–448. 2004.
|
|
7
|
Rall SC Jr and Mahley RW: The role of
apolipoprotein E genetic variants in lipoprotein disorders. J
Intern Med. 231:653–659. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kong FM, Guo RX and Liu YC: The study of
relationship between cholesterol crystalization and ApoE. Zhonghua
Shi Yan Wai Ke Za Zhi. 17:520–521. 2000.(In Chinese).
|
|
9
|
Thomas A: Accelerated gene counting for
haplotype frequency estimation. Ann Hum Genet. 67:608–612. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Abate N, Chandalia M, Cabo-Chan AV Jr, Moe
OW and Sakhaee K: The metabolic syndrome and uric acid
nephrolithiasis: novel features of renal manifestation of insulin
resistance. Kidney Int. 65:386–392. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Daudon M, Traxer O, Conort P, Lacour B and
Jungers P: Type 2 diabetes increases the risk for uric acid stones.
J Am Soc Nephrol. 17:2026–2033. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhang GH: Risk factors of blood lipid
level in urinary calculi. Zhongguo Xing Ke Xue. 21:34–37. 2012.(In
Chinese).
|
|
13
|
Lu F, Guan H, Gong B, Liu X, et al:
Genetic variants in PVRL2-TOMM40-APOE region are associated with
human longevity in a Han Chinese population. PLoS One.
9:e995802014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Atadzhanov M, Mwaba MH, Mukomena PN, Lakhi
S, et al: Frequency of APOE, MTHFR and ACE polymorphisms in the
Zambian population. BMC Res Notes. 7:1942014. View Article : Google Scholar : PubMed/NCBI
|