Introduction
Bladder cancer ranks ninth in cancer incidence
throughout the world with 380,000 new cases occurring every year.
The male to female ratio is 3.8:1 (1). According to the database of
Surveillance, Epidemiology and End Results, there has been no
significant change in mortality in the last 30 years (2). Bladder cancer is a heterogeneous
disease; 70% of patients present with superficial tumours, which
tend to recur but are generally not life threatening, and 30%
present with muscle-invasive disease, which is associated with a
high risk of mortality from distant metastases (3). The transitional cell cancers account
for >90% of bladder cancer cases, followed by squamous cell
cancer (5%), adenocancers (2%) and undifferentiated cancers
occurring in <1% of cases (3).
Of the patients that underwent radical cystectomy, 57% had
muscle-invasive bladder carcinoma (MIBC) at the time of diagnosis,
and the remaining 43% of the cases became muscle-invasive with the
progression of the superficial cancer (4). Approximately one-third of patients
diagnosed with MIBC have undetected metastases while undergoing
treatment for the primary tumour, and a quarter of patients who
undergo radical cystectomy also show lymph-node involvement at the
time of surgery (5). The standard
treatment strategy for MIBC is radical cystoprostatectomy for males
and anterior exenteration, including the bladder, urethra, uterus
and ventral vaginal wall, for females (3).
For patients with MIBC and nodal dissemination, the
frequency of metastasis was shown to be 92% in the regional
(perivesical or pelvic), 72% in the retroperitoneal and 35% in the
abdominal lymph nodes. A significant correlation was also found
between nodal metastases and concomitant distant
metastases(6). Standard
lymphadenectomy in patients with bladder cancer involves the
removal of nodal tissue cranially up to the common iliac
bifurcation, with the ureter forming the medial border, and
includes the internal iliac, presacral, obturator fossa and
external iliac nodes (6). Pelvic
lymphadenectomy is a part of the radical cystectomy procedure;
however, the borders of lymphadenectomy have not been clearly
described in the literature. A number of studies have recommended
limited lymphadenectomy but there are also studies suggesting the
survival benefit of more extensive lymphadenectomy (5,6).
Although radical cystectomy is the preferred treatment for MIBC,
metastases develop in ~25% of cases of tumours solely invading the
muscular layer and in ~50% of tumours extending into the
perivesical tissue (5).
Neoadjuvant or adjuvant chemotherapy can be used in the treatment
of high-risk patients with invasive bladder cancer; however,
systemic chemotherapy is the treatment of choice in metastatic
disease.
In the staging of MIBC, magnetic resonance imaging
(MRI) is superior to the computed tomography (CT) scan due to a
higher resolution in the soft tissue; however, the procedure is
accompanied by the disadvantage of low spatial resolution and the
side effect of systemic fibrosis. The accuracy of MRI for primary
tumour staging varies between 73 and 96% (mean, 85%), which is
10–33% higher (mean, 19%) than that obtained with CT (7). By contrast, CT offers higher
sensitivity in extravesical involvement (stages T3a and T3b). The
accuracy of CT in determining extravesical tumour extension varies
between 55 and 92% and increases with more advanced disease states
(8). Pelvic nodes >8 mm and
abdominal nodes >10 mm in maximum short-axis diameter, detected
by CT or MRI, should be considered to be pathologically enlarged.
The sensitivity for the detection of lymph-node metastases is low
(48–87%) due to the fact that pelvic lymph-node metastasis is
determined based on the size of the lymph nodes on CT and MR images
(9). It is well known that
metastasis can also occur in normal-sized lymph nodes. Positron
emission tomography (PET)/CT scans that combine anatomic and
functional images provide more sensitive data in the detection of
these lymph nodes.
At present, the detection of distant metastases and
local recurrence continues to be a significant problem following
radical cystectomy. Furthermore, there is a significant demand for
a diagnostic test offering high sensitivity and specificity in
predicting residual disease and monitoring the response to
treatment following radiotherapy and chemotherapy.
18F-fluorodeoxyglucose (18F-FDG)-PET/CT is
the most important diagnostic tool that allows the processing of
functional and anatomical images. The aim of the present study was
to retrospectively evaluate the effectiveness and diagnostic role
of 18F-FDG-PET/CT scans in restaging patients with MIBC
who underwent radical cystectomy. The histological findings (where
available) or the entire clinical and radiological workup
(multidetector computed tomography urography and MRI) were used as
a standard reference.
Materials and methods
Ethical approval and informed
consent
All procedures were performed in accordance with the
ethical standards of the World Medical Association committee on
human experimentation and with the 1975 Declaration of Helsinki, as
revised in 2000. Informed consent was obtained from all patients in
the study.
Patients
A total of 7,938 patients were evaluated and 10,553
18F-FDG-PET/CT scans were performed in the Department of
Nuclear Medicine of Sifa University (Izmir, Turkey) between July
2007 and April 2013. In this patient group, 51 patients underwent
radical cystectomy with the diagnosis of MIBC and
18F-FDG-PET/CT scans were obtained for restaging
purposes. The patient population comprised 45 males (88.2%) and six
females (11.8%) with a mean age of 62.3±9.79 years (range, 40–82
years).
Thirty patients (58.8%) underwent Bricker ileal
conduit urinary diversion, 18 patients (35.2%) underwent the
W-configured orthotopic Hautmann ileal neobladder procedure and
three patients (6%) underwent ureterocutaneostomy. The results of
the pathological and immunohistochemical examinations and data on
the histological subtypes of MIBC were available for 48 patients
(94%): 47 patients (92.2%) had high-grade transitional cell
carcinomas; one (1.9%) had squamous cell carcinoma; and the data on
histological subtype for the remaining three patients (5.9%) were
not available. The patients were re-assessed with
18F-FDG-PET/CT scans for restaging due to suspicion of
disease recurrence or for routine follow-up. These patients were
retrospectively evaluated, and the pathological findings and
18F-FDG-PET/CT data were recorded. Baseline
characteristics of the patients are summarised in Table I.
 | Table IBaseline characteristics of the
patients (n=51). |
Table I
Baseline characteristics of the
patients (n=51).
| Patient
parameter | Value |
|---|
| Age, years |
| Mean | 62 |
| Range | 40–82 |
| Gender, n (%) |
| Male | 45 (88.2) |
| Female | 6 (11.8) |
| Histological type,
n (%) |
| Urothelial
carcinoma | 47 (92.2) |
| Squamous cell
carcinoma | 1 (1.9) |
| Unknown | 3 (5.9) |
| Urinary diversion
type, n (%) |
| Bricker ileal
conduit | 30 (58.8) |
| Hautmann
orthotopic neobladder | 18 (35.2) |
|
Ureterocutaneostomy | 3 (6.0) |
Imaging and interpretation of data
18F-FDG was synthesised using an in-house
cyclotron (RDS 111 Cyclotron; Siemens Healthcare, Erlangen,
Germany) and an automated synthesis system (CPCU-Chemical Process
Control Unit) according to an authorised procedure.
18O-H2O, used as a target for the synthesis
of 18F was supplied by Sharon Marshall Isotops, Ltd. (Tel Aviv,
Israel). The patients fasted for five hours, and then their blood
glucose level was measured. Each patient was subsequently
intravenously injected with 370 MBq 18F-FDG. One hour
after 18F-FDG injection, a CT scan without contrast
agent was performed, covering the area from the vertex to the
proximal thigh, and the images were used for attenuation correction
and image fusion. This was followed by whole-body
three-dimensional-PET acquisition with eight bed positions and 3
min emission scan time per position using a dedicated PET/CT
scanner (HI-REZ Biograph™ 6; Siemens Healthcare), which provides an
in-plane spatial resolution of 4.8 mm and an axial field view of
16.2 cm. The PET data were reconstructed using a Gaussian filter
with an ordered-subset expectation maximisation algorithm (three
iterations, eight subsets), re-oriented in transverse, coronal and
sagittal planes, and assessed through comparisons with
corresponding CT images.
A forced diuresis was performed on 18 patients
(35.2%) who underwent the orthotopic continent ileal neobladder
procedure. Those patients were instructed to drink an additional
500 ml water and to void frequently. Delayed pelvic images were
acquired 2.5–3.0 h after injection of 18F-FDG.
PET scans were analyzed visually and
semi-quantitatively using standardised uptake value
(SUV)max measurements. SUV was expressed in terms of
body weight (g/ml). Parameters such as the patient’s weight
(kg) and height (cm), the radioactivity during injection (MBq),
residual radioactivity (MBq) subsequent to the injection, starting
time of the injection and the half-life of the radioisotope (taken
as a standard 109.8 min for 18F-FDG) were calculated
automatically by PET syngo VG50A software (Siemens Biograph Mctx;
Siemens AG Healthcare Sector, Erlangen, Germany).
Two experienced nuclear medicine physicians blindly
and independently reviewed the hybrid 18F-FDG-PET/CT
scans as positive or negative for a primary tumour site. Every
focal tracer uptake that deviated from physiological distribution
was considered to be due to the disease spread. The background
deviation and activity difference between the suspected lesion and
the surrounding tissues was used to differentiate benign from
malignant lesions; therefore, SUVmax >2.5 threshold
was employed.
Statistical analysis
Numeric results with a normal distribution, and for
which parametric test methods were used, are expressed as the mean
± standard deviation, wheras those with a non-normal distribution,
for which non-parametric test methods were used, are expressed as
the median (min – max), and categorical results are presented as
the number (%). All analyses were performed according to the
intention-to-treat principle and all data analyses were performed
using SPS 16.0 statistical software (SPSS, Inc., Chicago, IL,
USA).
Results
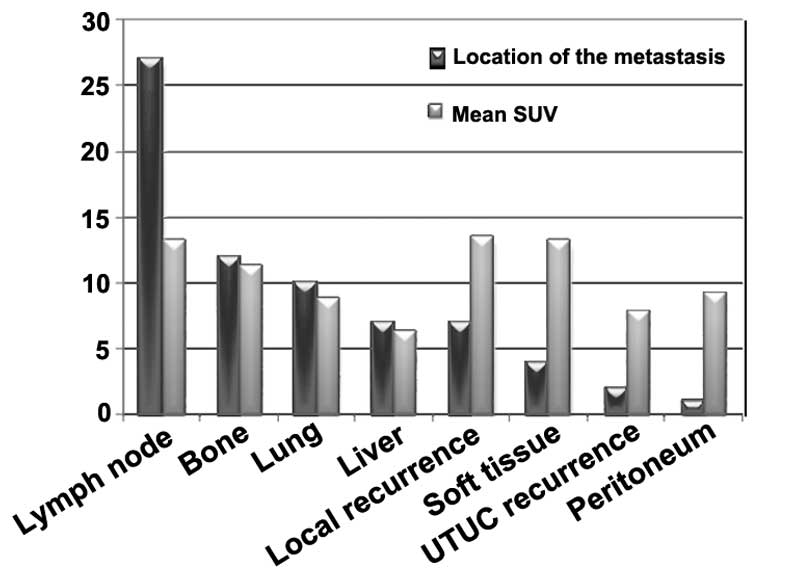
18F-FDG-PET/CT scans showed negative
findings in 13 patients (25.5%) and positive findings in 38
patients (74.5%). Seven patients (13.7%) had widespread metastases
with high SUV (mean, 8.2; range 3.5–14.7) involving at least three
organs (lungs or liver, bone, lymph nodes); 27 patients (52.9%) had
lymph node metastasis (mean SUV, 12.5); 12 patients (23.5%) had
bone metastasis (mean SUV, 11.2); 10 patients (19.6%) had lung
metastasis (mean SUV, 8.3); seven patients (13.7%) had liver
metastasis (mean SUV, 6.9); seven patients (13.7%) had local
recurrence (mean SUV, 13.5); four patients (7.8%) had soft tissue
metastasis (mean SUV, 13.2); two patients (3.9%) had recurrence of
upper urinary tract tumour (UTUC) (mean SUV, 7.9); and one patient
(1.9%) had peritonitis carcinomatosa (SUV, 9.2). The distribution
of the metastases and mean SUV of the metastatic foci are
summarised in Fig. 1.
Suspicious recurrent or metastatic lesions were
confirmed by histopathology or by clinical follow-up. The results
for sensitivity, specificity, positive predictive value (PPV),
negative predictive value (NPV) and accuracy of
18F-FDG-PET/CT were 92, 83, 94, 77 and 90%,
respectively.
Discussion
MIBCs are associated with a poor prognosis. The
survival rate decreases parallel to the stage of the disease and
survival time decreases by more than half in the presence of
metastatic disease. The five-year recurrence-free survival in
node-positive patients who underwent cystectomy was 34–43%, which
was considerably lower than that in patients without lymph-node
involvement (5). In a surgery-only
study, the five-year recurrence-free survival was 76, 74, 52 and
36% in patients with pT1, pT2, pT3 and pT4 tumours, respectively
(5). Furthermore, according to a
multi-institutional database of 888 consecutive patients undergoing
radical cystectomy for bladder cancer, the five-year
recurrence-free survival was 58% and the cancer-specific survival
was 66% (10). At present, radical
cystectomy involving the excision of pelvic lymph nodes is the gold
standard treatment method in MIBC. Due to the fact that local
recurrence and metastatic disease significantly decrease survival
times in patients subsequent to radical cystectomy, it is of vital
importance to establish an accurate diagnosis and provide prompt
treatment at this stage of the disease. The restaging of the
disease, minimizing false positives and false negatives and, more
importantly, the recognition of metastatic disease, constitute the
most important and realistic components in determining the
treatment strategy. The detection of distant metastases and local
recurrence continues to be a significant problem following radical
cystectomy. Furthermore, there is considerable demand for a
diagnostic test offering high sensitivity and specificity in
predicting residual disease and monitoring treatment responses
following radiotherapy and chemotherapy. 18F-FDG-PET/CT
is the most important diagnostic tool that allows the processing of
functional and anatomical images.
The most distinctive feature of the cancer tissue is
that it shows a higher glucose metabolism than normal tissues
(Warburg effect) (11). PET
imaging with 18F-FDG, an analogue of glucose, tracks the
glucose metabolism of tissues. The integral role of
18F-FDG-PET in oncology is indisputable. The
hypermetabolism of malignancy is associated with an increased
expression of cellular membrane glucose transporters and enhanced
hexokinase enzymatic activity (12). A high uptake of 18F-FDG
in cancerous lesions of transitional cell carcinomas was first
demonstrated by Harney et al (13) in rats. Drieskens et al
(14) found that metabolism-based
anatomical information gathered by the addition of
18F-FDG-PET to CT provided high diagnostic accuracy in
the pre-operative staging of invasive transitional cancers,
particularly invasive bladder carcinoma. At present,
18F-FDG-PET combined with CT is an established standard
for pre-operative staging and detecting metastatic lesions of
bladder cancer (15–17).
18F-FDG in the systemic circulation
undergoes glomerular filtration; however, it is excreted in the
urine and not reabsorbed as glucose (18). This means that identifying kidney,
ureter, bladder and prostate tumours is problematic (19). Another limitation is the poor
18F-FDG uptake by certain malignant neoplasms, such as
renal, prostate and hepatocellular carcinomas. This has been
attributed to their high glucose-6-phosphatase activity, the enzyme
that converts 18F-FDG-6-phosphate back into
18F-FDG for excretion from the tumour cells (20). Another important reason for reduced
uptake is that primary tumours may express low levels of glucose
transporters, such as glucose transporter type 1, which are
responsible for the accumulation of 18F-FDG (21).
Kosuda et al (22) used retrograde saline irrigation of
the urinary bladder to remove 18F-FDG radioactivity;
however, tracer activity was not able to be reduced to background
levels and a 40% false-negative rate for the detection of recurrent
or residual tumour in the bladder was reported. Diuresis has been
shown to effectively decrease the background radioactivity in the
urinary tract, thus facilitating the identification of
hypermetabolic lesions on an 18F-FDG-PET scan (23). Anjos et al (24) reported a 54% sensitivity rate for
18F-FDG-PET/CT in the detection of malignant areas on
the bladder wall of 11 patients with MIBC. A similar study by
Harkirat et al (25) found
a sensitivity of 86.7% and a specificity of 100% for
18FDG-PET/CT scans in the detection of primary lesions
in 22 patients with MIBC. These two studies acquired late pelvic
images with hyperhydration and diuresis. Parallel to these two
studies late pelvic images were obtained with oral hyperhydration
2.5–3.0 h after the injection of 18F-FDG in 18 patients
(35.2%) that underwent orthotopic ileal continent neobladder
urinary diversion in the present study. This endeavour was to
overcome the disadvantages posed by urinary excretion of
18F-FDG.
Lodde et al (26) performed 18F-FDG-PET/CT
and forced diuresis in 44 patients with known MIBC and compared the
findings with those from standard CT. It was demonstrated that
18F-FDG-PET/CT was more sensitive (85 vs. 77%) but less
specific (25 vs. 50%) than CT alone for detecting primary tumours.
The use of CT alone for the detection of MIBC exhibited a
sensitivity of 46%, a specificity of 92% and an accuracy of 80%.
Lodde et al (26)
demonstrated that, regarding the detection of pelvic node
metastasis, 18F-FDG-PET/CT was more sensitive than CT
(57 vs. 33%) with a specificity and PPV of 100% for both imaging
techniques. Drieskens et al (14) reported 60, 88 and 78% sensitivity,
specificity and accuracy, respectively, for
18F-FDG-PET/CT in the detection of metastatic disease in
55 patients with MIBC. In a study by Swinnen et al (27) of 55 patients with MIBC in whom
radical cystectomy was planned, the results of
18F-FDG-PET/CT scans were compared with the results of
pathological examination following radical cystectomy and extended
pelvic lymph node dissection. 18F-FDG-PET/CT achieved a
sensitivity, specificity, and accuracy of 46, 97 and 84%,
respectively. Kibel et al (16) studied 43 patients with a T2-3N0M0
stage tumour who underwent radical cystectomy, and reported a
sensitivity of 70%, a specificity of 94%, a PPV of 78% and an NPV
of 91% for 18F-FDG-PET/CT. Occult metastatic disease was
found in seven out of 42 patients, and it was revealed that
pre-operative 18F-FDG-PET/CT could affect the treatment
selection prior to radical cystectomy (16). The same study also evaluated the
association between PET findings and survival. The rate of 24-month
recurrence-free survival was 24% in patients with positive PET
findings and 55% in patients with negative PET findings. The
disease-specific survival rates in these patients were 23 and 58%,
respectively.
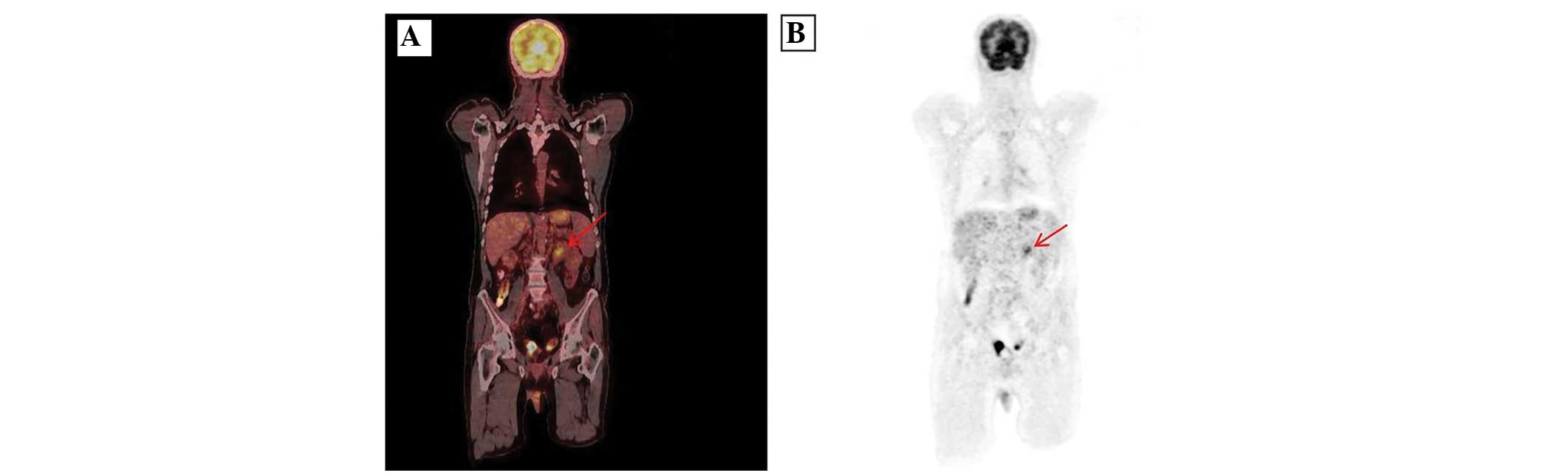
Parallel to these findings, we consider that urinary
excretion of 18F-FDG partially eliminated the
disadvantages of the method in patients that underwent radical
cystectomy due to MIBC. In the present study, the use of
18F-FDG may have been disadvantageous in the 35% of
patients (n=18) who underwent the ileal continent orthotopic
neobladder procedure; however, the authors attempted to overcome
these limitations by administering oral hyperhydration and
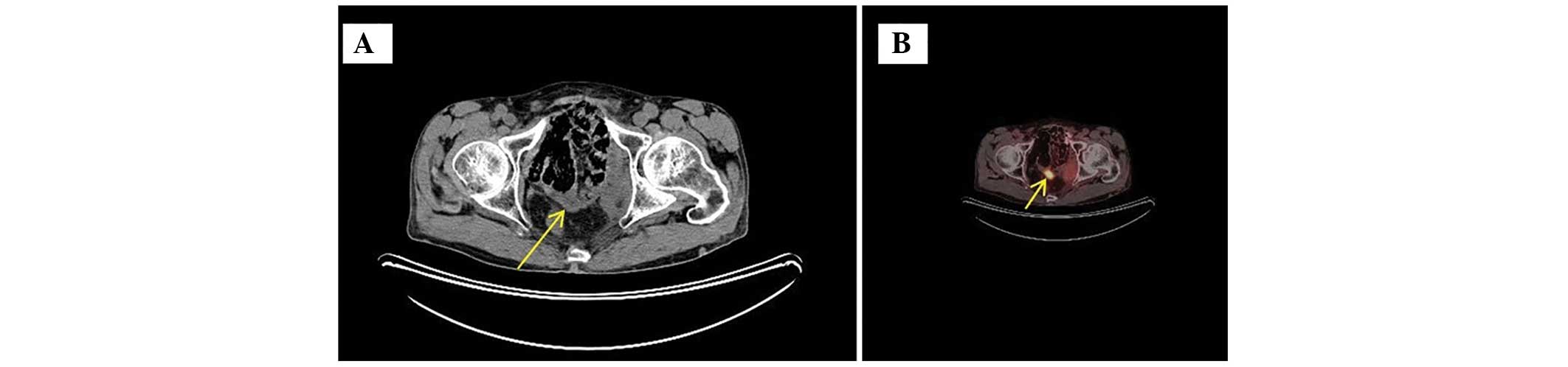
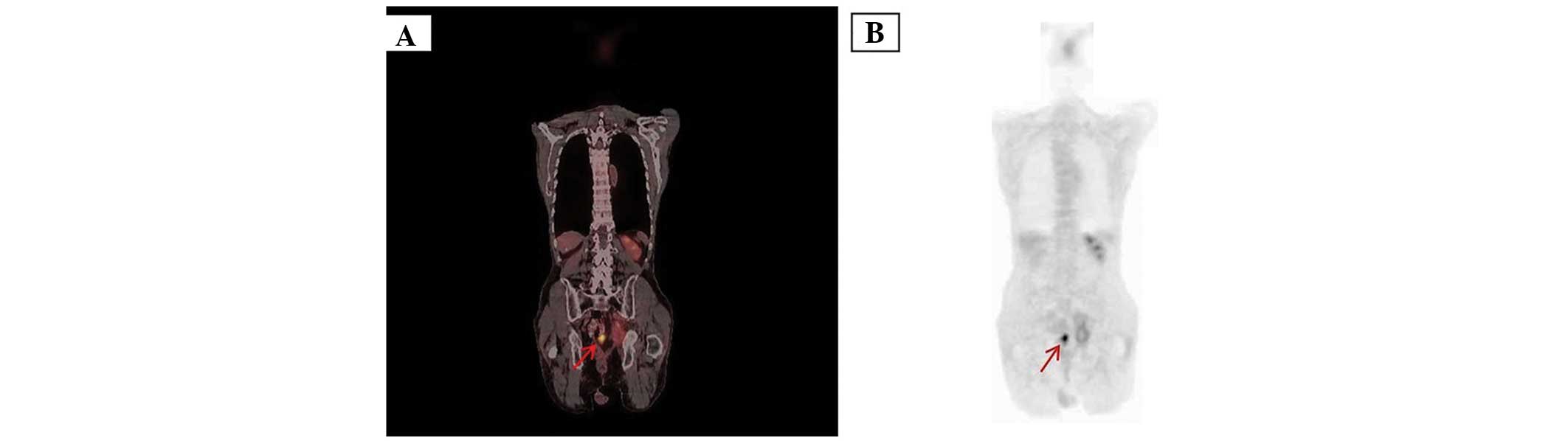
acquiring late pelvic images. 18F-FDG activity in
orthotopic continent neobladder may produce problems in detecting
pelvic recurrence. The acquisition of late pelvic images and
emptying the neobladder through catheterisation allowed
visualisation of the pelvic lymph-node metastasis and recognition
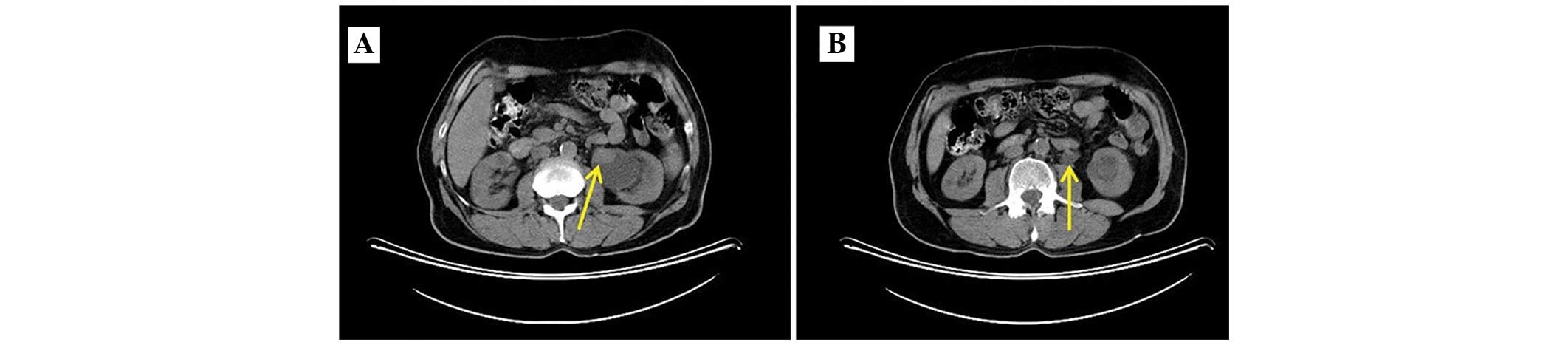
of the solitary lymph-node metastasis (Figs. 2 and 3). In the present study, the recurrences
of UTUC could have produced problems due to urinary activity of
18F-FDG. UTUC recurrence was detected in only 3.9% (n=2)
of the patients in the present study (Figs. 4 and 5). The high SUV (mean, 7.9) of these
lesions allowed visualisation on the detector. The detection of
low-grade UTUC with low metabolism continues to be a significant
problem using 18F-FDG-PET/CT scans. Although survival
data are not available in the present study, other parameters are
in line with those reported in the literature (14–16).
According to these data from the literature,
18F-FDG-PET/CT scans prior and subsequent to cystectomy
are considered to play an important role in the planning of
treatment strategies.
Apolo et al (15) evaluated the role of
18F-FDG-PET/CT in a series of 47 patients with
metastatic MIBC and reported a sensitivity of 88% and a specificity
of 87%. The patient-based analyses found that
18F-FDG-PET/CT scans may change the treatment plan in
68% of the patients due to a 40% higher detection rate compared
with that of conventional CT and MRI. 18F-FDG-PET/CT has
additionally been found to provide diagnostic data relevant to the
clinical management of the disease due to its higher sensitivity
and specificity in metastatic MIBC (28). Jadvar et al (29) retrospectively evaluated the
diagnostic performance of PET/CT in patients with MIBC, and they
reported that the method changed the clinical management in 17% of
the patients. In a meta-analysis by Lu et al (17), 18F-FDG-PET/CT scans were
found to provide sufficient diagnostic accuracy in the staging and
restaging of patients with MIBC and metastatic bladder cancer;
however, 18F-FDG-PET/CT scans did not show sufficient
diagnostic performance in the detection of primary bladder cancer
on the bladder wall. The study revealed that the method may not
provide sufficient data regarding the T stage of the bladder and
detrusor lesions due to urinary excretion of 18F-FDG,
but 18F-FDG-PET/CT can be used for staging purposes and
the detection of metastatic disease (17). 18F-FDG-PET/CT scans
provide valuable data in the detection of metastatic disease and in
the evaluation of the response to systemic chemotherapy and
detection of residual disease. In addition,
18F-FDG-PET/CT is used to evaluate insufficient response
to cisplatin-based chemotherapy in patients with lung and
lymph-node metastases after radical cystectomy.
Recently, Goodfellow et al (30) evaluated the efficiency of
18F-FDG-PET/CT compared with CT in patients in whom
radical cystectomy was planned due to MIBC. Although PET/CT had
certain advantages in detecting distant metastases, CT offered 45%
sensitivity and 98% specificity in detecting pelvic lymph nodes;
the combination of 18F-FDG-PET/CT increased sensitivity
to 69%, while the specificity was 95%. It was suggested that the
use of 18F-FDG-PET/CT instead of CT provided a slight
improvement in the pre-operative diagnosis of MIBC, but that
improvement did not justify the increasing costs of the diagnostic
workup; therefore, it was recommended that this method be used only
in selected patients (30). In a
recent study, Mertens et al (31) evaluated the association between
18F-FDG-PET/CT results and mortality in patients with
MIBC. In the study (n=211), the median follow-up period was 18
months and the disease-specific survival was 50 months in
PET-negative patients; this rate decreased to 16 months in
PET-positive patients. The presence of extravesical disease was
found to be an independent prognostic factor for mortality in
PET-positive patients (31).
Due to the physiological activity of
18F-FDG in the urinary tract, 11C-choline,
11C-acetate and 11C-methionine have been used
in an attempt to overcome the diagnostic limitations of
18F-FDG-PET/CT. 11C-choline is minimally
excreted in the urine and is incorporated into tumour cells by
conversion into 11C-phosphorlycholine, which is trapped
inside the cell (32). A study
that evaluated 11C-choline PET/CT in patients with MIBC
reported a sensitivity, specificity, PPV, NPV and accuracy of 58,
66, 39, 81 and 64%, respectively (33). A study by Golan et al
compared 11C-choline-PET/CT with
18F-FDG-PET/CT reported that 11C-choline was
not advantageous compared with other methods (34). In the study by Golan et al
(34), which evaluated 51 lesions
with abnormal activity in 20 patients, the PPV for all lesions was
found to be 84.7% for 11C-choline-PET/CT and 90.7% for
18F-FDG-PET/CT. In the evaluation of extravesical
lesions, the PPV was 79.4% and 88.2%, respectively. Despite the
disadvantage of partial histopathological correlation,
11C-choline-PET/CT was not found to be superior to
18F-FDG-PET/CT in detecting metastatic bladder carcinoma
(34). The diagnostic performances
of 18F-FDG-PET/CT and 11C-choline-PET/CT
reported in the literature are summarised in Table II. 11C-methionine
uptake is proportional to the amino acid transport and, to a
certain extent, protein synthesis. In cancer, methionine levels
have been correlated with the amount of viable tumour tissue
(33). Ahlström et al
(35) found that
11C-methionine was superior to 18F-FDG in
patients with MIBC. Schöder et al (36) investigated the utility of
11C-acetate-PET/CT for the staging of MIBC and the
assessment of response subsequent to neoadjuvant chemotherapy. A
total of 17 patients underwent 11C-acetate-PET/CT prior
to radical cystectomy and pelvic lymph-node dissection. It was
concluded that 11C-acetate-PET/CT offered high
sensitivity in the detection of lymph-node metastases; however,
inflammation and granulomatous infections and false-positive
results following intravesical Bacillus Calmette-Guerin therapy
were reported as the limitations of this method (36).
| Table IIThe diagnostic performance of
18F-FDG-PET/CT and 11C-choline-PET/CT studies
in the literature. |
Table II
The diagnostic performance of
18F-FDG-PET/CT and 11C-choline-PET/CT studies
in the literature.
| First author
(reference) | Modality | n | Status of the
BCa | Sensitivity
(%) | Specificity
(%) | PPV (%) | NPV (%) | Accuracy (%) |
|---|
| Harkirat (25) |
18F-FDG-PET/CT | 22 | Primary BCa | 86.7 | 100 | - | - | - |
| Lodde (26) |
18F-FDG-PET/CT | 44 | Primary BCa | 77 | 50 | 100 | - | - |
| Drieskens (14) |
18F-FDG-PET/CT | 55 | Metastatic BCa | 60 | 88 | - | - | 78 |
| Apollo (15) |
18F-FDG-PET/CT | 47 | Metastatic BCa | 88 | 87 | - | - | - |
| Swinnen (27) |
18F-FDG-PET/CT | 55 | MIBC, before
cystectomy | 46 | 97 | - | - | 84 |
| Goodfellow
(30) |
18F-FDG-PET/CT | - | MIBC, before
cystectomy | 68 | 95 | - | - | - |
| Maurer (33) |
11C-choline-PET/CT | 44 | MIBC, before
cystectomy | 58 | 66 | 39 | 81 | 64 |
| Kibel (16) |
18F-FDG-PET/CT | 43 | MIBC, before
cystectomy | 70 | 94 | 78 | 91 | - |
| Present study |
18F-FDG-PET/CT | 51 | MIBC, after
cystectomy | 92 | 83 | 94 | 77 | 90 |
The metabolic rate of low-grade transitional cell
carcinomas is close to that of normal tissues. The increased
glucose metabolism in patients with high-grade MIBC allows
visualisation of the lesions on the detector due to increased
18F–FDG uptake.
False-positive or false-negative results in
18F-FDG uptake cannot be explained solely by the glucose
metabolism of tumour tissue. Studies have demonstrated that
18F-FDG-PET/CT scans can provide information only in the
presence of a high number of tumour cells with abnormal glucose
metabolism (104–107) (11,15,16).
Such diagnostic failures are particularly important in solid organ
metastasis, such as in the lungs and liver. In general,
18F-FDG-PET/CT cannot accurately evaluate metastasis
measuring <5 mm in size. It is unknown why lung lesions below
this threshold do not produce high SUVs. This could be caused by
motion artifacts and low metabolic activity of the metastatic
lesion. Reducing the motion artifacts using certain techniques,
achieving an enhanced spatial resolution and finding higher cut-off
SUV values for such lesions could increase diagnostic accuracy
(37).
The findings of PET/CT scans must be verified by
histopathological work-up in order to confirm disease recurrence.
Theoretically, this remains the gold standard. In daily practice,
however, this is seldom possible due to clinical reasons, the
feasibility of the procedure and the effective advantages of this
approach in the absence of a radical surgical intent. In the
present study histological confirmation was available for 15
patients, while the remainder relied on the comparison with
clinical and radiological findings.
The limitation of the present study was its
retrospective nature. Selection bias may have been present as it is
likely that only those patients with MIBC and suspected to have
recurrence were referred for PET/CT.
In conclusion, 18F-FDG-PET/CT images
provide complementary structural-metabolic information and have the
potential to significantly reduce the false positives of PET and CT
performed separately. Despite the limitations of the present study,
due to the retrospective type of analysis and the absence of
systematic histological confirmation of pathological uptake, the
results were in agreement with those of previous studies and
suggest that 18F-FDG-PET/CT is characterised by a high
sensitivity and PPV and could be useful in restaging patients with
MIBC following radical cystectomy. This procedure could play an
important role in rendering decisions regarding radiotherapy,
chemotherapy and post-operative follow-up.
References
|
1
|
Ploeg M, Aben KK and Kiemeney LA: The
present and future burden of urinary bladder cancer in the world.
World J Urol. 27:289–293. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Abdollah F, Gandaglia G, Thuret R, et al:
Incidence, survival and mortality rates of stage-specific bladder
cancer in United States: a trend analysis. Cancer Epidemiol.
37:219–225. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kaufman DS, Shipley WU and Feldman AS:
Bladder cancer. Lancet. 374:239–249. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Vaidya A, Soloway MS, Hawke C, et al: De
novo muscle invasive bladder cancer: is there a change in trend? J
Urol. 165:47–50. 2001. View Article : Google Scholar
|
|
5
|
Stein JP, Lieskovsky G, Cote R, et al:
Radical cystectomy in the treatment of invasive bladder cancer:
long-term results in 1,054 patients. J Clin Oncol. 19:666–675.
2001.PubMed/NCBI
|
|
6
|
Simone G, Papalia R, Ferriero M, et al:
Stage-specific impact of extended versus standard pelvic lymph node
dissection in radical cystectomy. Int J Urol. 20:390–397. 2013.
View Article : Google Scholar
|
|
7
|
Barentsz JO, Jager GJ, Witjes JA and Ruijs
JH: Primary staging of urinary bladder carcinoma: the role of MR
imaging and a comparison with CT. Eur Radiol. 6:129–133. 1996.
View Article : Google Scholar
|
|
8
|
Kundra V and Silverman PM: Imaging in
oncology from the University of Texas M. D. Anderson Cancer Center.
Imaging in the diagnosis, staging, and follow-up of cancer of the
urinary bladder. AJR Am J Roentgenol. 180:1045–1054. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Barentsz JO, Engelbrecht MR, Witjes JA, et
al: MRI of the male pelvis. Eur Radiol. 9:1722–1736. 1999.
View Article : Google Scholar
|
|
10
|
Shariat SF, Karakiewicz PI, Palapattu GS,
et al: Outcomes of radical cystectomy for transitional cell
carcinoma of the bladder: a contemporary series from the Bladder
Cancer Research Consortium. J Urol. 176:2414–2422. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gillies RJ, Robey I and Gatenby RA: Causes
and consequences of increased glucose metabolism of cancers. J Nucl
Med. 49(Suppl 2): 24S–42S. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Smith TA: Mammalian hexokinases and their
abnormal expression in cancer. Br J Biomed Sci. 57:170–178.
2000.PubMed/NCBI
|
|
13
|
Harney JV, Wahl RL, Liebert M, Kuhl DE,
Hutchins GD, Wedemeyer G and Grossman HB: Uptake of 2-deoxy,
2-(18F) fluoro-D-glucose in bladder cancer: animal
localization and initial patient positron emission tomography. J
Urol. 145:279–283. 1991.PubMed/NCBI
|
|
14
|
Drieskens O, Oyen R, Van Poppel H, Vankan
Y, Flamen P and Mortelmans L: FDG-PET for preoperative staging of
bladder cancer. Eur J Nucl Med Mol Imaging. 32:1412–1417. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Apolo AB, Riches J, Schöder H, Akin O,
Trout A, Milowsky MI and Bajurin DF: Clinical value of fluorine-18
2-fluoro-2-deoxy-D-glucose positron emission tomography/computed
tomography in bladder cancer. J Clin Oncol. 28:3973–3978. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kibel AS, Dehdashti F, Katz MD, Klim AP,
Grubb RL, Humphrey PA, et al: Prospective study of [18F]
fluorodeoxyglucose positron emission tomography/computed tomography
for staging of muscle-invasive bladder carcinoma. J Clin Oncol.
27:4314–4320. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lu YY, Chen JH, Liang JA, Wang HY, Lin CC,
Lin WY and Kao CH: Clinical value of FDG PET or PET/CT in urinary
bladder cancer: a systemic review and meta-analysis. Eur J Radiol.
81:2411–2416. 2012. View Article : Google Scholar
|
|
18
|
Gallagher BM, Fowler JS, Gutterson NI,
MacGregor RR, Wan CN and Wolf AP: Metabolic trapping as a principle
of radiopharmaceutical design: some factors responsible for the
biodistribution of [18F] 2-deoxy-2-fluoro-D-glucose. J
Nucl Med. 19:1154–1161. 1978.PubMed/NCBI
|
|
19
|
Kumar R, Zhuang H and Alavi A: PET in the
management of urologic malignancies. Radiol Clin North Am.
42:1141–1153. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Caracó C, Aloj L, Chen LY, Chou JY and
Eckelman WC: Cellular release of
[18F]2-fluoro-2-deoxyglucose as a function of the
glucose-6-phosphatase enzyme system. J Biol Chem. 275:18489–18494.
2000. View Article : Google Scholar
|
|
21
|
Lin EC and Alavi A: Urologic tumors. PET
and PET/CT: A Clinical Guide. 2nd edition. Thieme; New York, NY:
pp. 204–211. 2009
|
|
22
|
Kosuda S, Kison PV, Greenough R, Grossman
HB and Wahl RL: Preliminary assessment of fluorine-18
fluorodeoxyglucose positron emission tomography in patients with
bladder cancer. Eur J Nucl Med. 24:615–620. 1997.PubMed/NCBI
|
|
23
|
López-Gandul S, Pérez-Moure G,
García-Garzón JR, et al: Intravenous furosemide injection during
18F-FDG PET acquisition. J Nucl Med Technol. 34:228–231.
2006.
|
|
24
|
Anjos DA, Etchebehere EC, Ramos CD, Santos
AO, Albertotti C and Camargo EE: 18F-FDG PET/CT delayed
images after diuretic for restaging invasive bladder cancer. J Nucl
Med. 48:764–770. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Harkirat S, Anand S and Jacob M: Forced
diuresis and dual-phase F-fluorodeoxyglucose-PET/CT scan for
restaging of urinary bladder cancers. Indian J Radiol Imaging.
20:13–19. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lodde M, Lacombe L, Friede J, Morin F,
Saourine A and Fradet Y: Evaluation of fluorodeoxyglucose
positron-emission tomography with computed tomography for staging
of urothelial carcinoma. BJU Int. 106:658–663. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Swinnen G, Maes A, Pottel H, Vanneste A,
Billiet I, et al: FDG-PET/CT for the preoperative lymph node
staging of invasive bladder cancer. Eur Urol. 57:641–647. 2010.
View Article : Google Scholar
|
|
28
|
Bouchelouche K, Turkbey B and Choyke PL:
PET/CT and MRI in bladder cancer. J Cancer Sci Ther. (Suppl
14)30:76922012.
|
|
29
|
Jadvar H, Quan V, Henderson RW and Conti
PS: [F-18]-Fluorodeoxyglucose PET and PET-CT in diagnostic imaging
evaluation of locally recurrent and metastatic bladder transitional
cell carcinoma. Int J Clin Oncol. 13:42–47. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Goodfellow H, Viney Z, Hughes P, Rankin S,
Rottenberg G, Hughes S, et al: Role of fluorodeoxyglucose positron
emission tomography (FDG PET)-computed tomography (CT) in the
staging of bladder cancer. BJU Int. 114:389–395. 2014.
|
|
31
|
Mertens LS, Mir MC, Scott AM, Lee ST,
Fioole-Bruining A, Vegt E, et al:
18F-fluorodeoxyglucose--positron emission
tomography/computed tomography aids staging and predicts mortality
in patients with muscle-invasive bladder cancer. Urology.
83:393–398. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Jana S and Blaufox MD: Nuclear medicine
studies of the prostate, testes, and bladder. Semin Nucl Med.
36:51–72. 2006. View Article : Google Scholar
|
|
33
|
Maurer T, Souvatzoglou M, Kübler H,
Opercan K, Schmidt S, et al: Diagnostic efficacy of
[11C]choline positron emission tomography/computed
tomography compared with conventional computed tomography in lymph
node staging of patients with bladder cancer prior to radical
cystectomy. Eur Urol. 61:1031–1038. 2012. View Article : Google Scholar
|
|
34
|
Golan S, Sopov V, Baniel J and Groshar D:
Comparison of 11C-choline with 18F-FDG in
positron emission tomography/computerized tomography for staging
urothelial carcinoma: a prospective study. J Urol. 186:436–441.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Ahlström H, Malmström PU, Letocha H,
Andersson J, Långström B and Nilsson S: Positron emission
tomography in the diagnosis and staging of urinary bladder cancer.
Acta Radiol. 37:180–185. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Schoder H, Ong SC, Reuter VE, Cai S,
Burnazi E, et al: Initial Results with [11]C-acetate
positron emission tomography/computed tomography (PET/CT) in the
staging of urinary bladder cancer. Mol Imaging Biol. 14:245–251.
2012. View Article : Google Scholar
|
|
37
|
El Fakhri G, Surti S, Trott CM, et al:
Improvement in lesion detection with whole-body oncologic
time-of-flight PET. J Nucl Med. 52:347–353. 2011. View Article : Google Scholar : PubMed/NCBI
|