Introduction
Currently, the incidence of diabetes is increasing
rapidly, leading to more cases of diabetic foot. Diabetic foot is
predominantly observed in males and elderly patients >60 years
of age (1). It has been reported
that the incidence rate of diabetic foot over the lifetime of a
patient with diabetes is 15–25% (2).
Diabetic foot is a chronic and progressive lesion, involving blood
vessels, nerves, tendons and bone (3,4).
Sclerosis, stenosis or occlusion in the arteries of the lower
extremities may affect blood supply to the limbs, particularly the
acral skin, frequently leading to ulcers and gangrene. Foot
infection and gangrene may result in amputation and disability,
while certain patients may succumb to the condition. Traditionally,
the treatment of diabetic foot consists primarily of medical
pharmacotherapy or surgical reconstruction of blood flow; however,
for patients with diabetic foot caused by arterial occlusion,
medication cannot fundamentally solve the underlying cause of the
condition. In addition, the lesions in the lower extremities of
such patients are typically segmental and involve the arteries of
the leg; due to the absence of the distal artery flow tract, such
patients may not be able to undergo an artery bypass or vascular
interventional treatment (5).
Recently, stem cell transplantation technology has
been increasingly studied worldwide, and human stem cell studies
have become a crucial new field in the life sciences. The emergence
of stem cell transplantation is among the most important
developments in life sciences at the end of the 20th century
(6). In 1998, Thomson et al
(7) isolated human embryonic stem
cells from the inner cell mass and observed that these cells
possessed self-renewal and multi-directional differentiation
potentials in vitro and in vivo. Stem cells have
subsequently become a key research tool in the biomedical sciences,
and show promise for the treatment of various intractable diseases.
It has been demonstrated that hematopoietic stem cells can be
induced to differentiate into vascular endothelial cells via
exposure to ischemic and anoxic environments (8), which promotes neovascularization in the
ischemic limb and improves blood supply, thereby treating limb
ischemia (9,10). In autologous stem cell
transplantation for the treatment of lower-limb ischemic diseases,
the majority of studies have used granulocyte colony stimulating
factor (G-CSF) at doses of 5 and 10 µg/kg/day for the stem cell
mobilization, and the stem cells have been harvested after 5 days;
however, whether this is the optimal mobilization and harvesting
time has not yet been verified (11,12). The
aim of the present study was to observe the mobilization effect of
autologous hematopoietic stem cells by applying different doses of
G-CSF at different times, in order to determine the optimal dose of
G-CSF and the optimal time for stem cell mobilization. Furthermore,
the clinical curative effect of autologous peripheral blood stem
cell transplantation in the treatment of diabetic foot gangrene was
investigated.
Materials and methods
Clinical data
A total of 127 patients with diabetic foot necrosis,
including 58 males and 69 females (mean age, 69 years; age range,
49–84 years) were enrolled in this study. This study was conducted
in accordance with the Declaration of Helsinki and with approval
from the Ethics Committee of Weifang People's Hospital (Weifang,
China). Written informed consent was obtained from all
participants. All patients presented with degree 3 to 4 diabetic
foot, and 98 patients exhibited pain at rest and/or intermittent
claudication (13). All patients
presented with different degrees of acral gangrene and ischemic
ulcers and/or pain at rest. The patients were eager to be relieved
of the intermittent claudication. A preoperative digital
subtraction angiography (DSA) examination confirmed the presence of
occlusive lesions in the main vessels of the patients. All cases
met the World Health Organization diagnostic criteria for diabetic
foot (14). Cases complicated with
seriously impaired function of the heart, lungs, brain, kidney and
other organs or patients who could not tolerate the surgery were
excluded.
Hematopoietic stem cell
mobilization
A total of 127 patients were divided into 2 groups
at random. Group A (n=63) received subcutaneous injections of 5
µg/kg/day recombinant human G-CSF (Filgrastim; Sandoz
Pharmaceuticals GmbH, Holzkirchen, Germany), twice per day. In
group A, 16 patients were treated for 4 days, 17 patients for 5
days, 16 cases for 6 days and 14 cases for 7 days. Group B (n=64)
received subcutaneous injections of 10 µg/kg/day Filgrastim, twice
per day. In group B, 16 patients received treatment for 4 days, 17
patients for 5 days, 16 patients for 6 days and 15 patients for 7
days. The peripheral blood mononuclear cells (PBMNCs) and
CD34+ cells were counted each day. When the PBMNC count
and CD34+ cell number reached a peak, peripheral blood
stem cells were collected. During the G-CSF mobilization,
low-molecular-weight heparin (5,000 IU; Sanofi-Aventis S.A., Paris,
France) was administered by subcutaneous injection every day, in
order to prevent a cerebrovascular accident induced by the
increased leukocyte count.
Collection of hematopoietic stem
cells
Venous blood was collected from the median cubital
vein of one of the upper extremities and directly entered into a
blood cell separator (Fresenius SE & Co. KGaA, Bad Homburg,
Germany) through a closed system. Subsequently, ~50 ml stem cell
suspension was filtered out, and the remaining blood was transfused
back to the patient via the median cubital vein of the other upper
extremity simultaneously. If necessary in certain patients, the
great saphenous vein or subclavian vein was used for puncture and
catheterization.
Determination of white blood cells
(WBCs), PBMNCs and CD34+ cells
WBCs and PBMNCs were counted using an automatic
blood analyzer (Beckman Coulter, Brea, CA, USA), and the peripheral
blood CD34+ cells prior to and following G-CSF
mobilization were detected using a flow cytometer, CD34+
monoclonal antibodies and a hemolytic agent (BD Biosciences,
Franklin Lakes, NJ, USA), according to the manufacturers
instructions.
Autologous peripheral blood stem cell
transplantation
Air disinfection of the operating theater was
performed for 30 min prior to transplantation. Simultaneously,
patients received an intramuscular injection of 100 mg pethidine
hydrochloride (Shenyang First Pharmaceutical Factory, Shenyang,
China) for analgesia. Following disinfection of the limb skin, stem
cell suspension fluid was injected into the ischemic lower
extremities at multiple points around the embolized blood vessels,
using a 23 G syringe. The puncture positions were pre-marked
between the foot and 3 cm above the knee, with intervals of 3 cm.
Subsequently, 2 ml stem cell suspension fluid was injected into
each marker point. For the ulcerated or necrotic areas, the stem
cell suspension fluid was injected around or at the bottom of the
lesion tissues by point injection. Following the transplantation,
the affected extremity received a protective pressure dressing.
Intermittent claudication distance (L)
scoring
The distance that the patient could walk prior to
experiencing claudication was scored as follows: 0 points, L ≥0.5
km with no pain; 1 point, 0.499≥ L ≥0.4 km with pain; 2 points,
0.399≥ L ≥0.3 km with pain; 3 points, 0.299≥ L ≥0.1 km with pain;
and 4 points, pain at rest and unable to walk, or walking distance
<0.1 km.
Skin temperature measurement
Skin temperature was measured at the skin outside
the third metatarsophalangeal joint at the dorsum of foot using an
SDW point digital thermometer (Tianjin Traffic Electronic
Instrument Experimental Factory, Tianjin, China). Temperatures were
measured and recorded at the same time each day in all
patients.
Ankle brachial index (ABI)
measurement
ABI was detected using a Doppler flow detector and
ABI check equipment (Beijing Gelin Dimei Technology Co., Ltd.,
Beijing, China).
Pain scoring
Patient pain was scored as follows: 0 points, no
pain; 1 point, mild and tolerable pain with no analgesic drugs
required; 2 points, moderate pain requiring oral analgesic drugs;
and 3 points, severe pain that was not relieved by general
analgesic drugs and required an analgesic injection.
DSA imaging of the lower
extremities
DSA of the lower extremities was performed using a
Siemens Duplex computer imaging system (Siemens Healthcare,
Erlangen, Germany) and the resulting images were scored as
followed: 0 points, no new collateral vessels; 1 point, little new
collateral circulation; 2 points, moderate new collateral
circulation; 3 points, abundant new collateral circulation.
Statistical analysis
Data are presented as the mean ± standard deviation
and were analyzed using SPSS statistical software, version 19.1
(IBM SPSS, Armonk, NY, USA). Comparisons between the data prior to
and following the treatment were performed using the paired t-test.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Collection efficiency of stem cells is
closely correlated with the dosage and mobilization time of
G-CSF
With the prolongation of the hematopoietic stem cell
mobilization time, the WBC and PBMNC counts and the number of
CD34+ cells increased; however, the WBC count normalized
by day 3 after the mobilization was ceased. The WBC counts of
groups A and B reached 3.0×1010/l at days 4 and 3 of
mobilization, respectively. Furthermore, the PBMNC count and
CD34+ cell number of groups A and B peaked at days 5 and
4, respectively. On the fourth day of mobilization, the PBMNC count
of group B was (5.59±1.63)×109/l and the
CD34+ cell number was (3.57±1.56)×107/l; on
the fifth day of mobilization, the PBMNC count of group A was
(5.72±1.56)×109/l and the CD34+ cell number
was (4.26±1.21)×107/l. All patients in groups A and B
met the requirements for the stem cell collection. Therefore, In
group A, 16 cases underwent stem cell collection on day 4, 17 cases
on day 5, 16 cases on day 6 and 14 cases on day 7. In group B, 16
cases underwent stem cell collection on day 4, 17 cases on day 5,
16 cases on day 6 and 15 cases on day 7. The CD34+ cell
number increased with the increase in PBMNCs, and a positive
correlation was detected between these parameters (r=0.626,
P<0.05).
Blood circulation in the ischemic
area
At the early stage after injection with stem cell
suspension, the local skin temperature of the patients increased
significantly and blood oozing from the wound surface increased.
Granulation occurred at a significantly more rapid rate, and
patients experienced a local burning pain. After 4 weeks, patients
were followed-up for a DSA re-examination. DSA indicated that the
collateral circulation in the affected lower extremity was
established. The volume of blood flow to the acral skin increased
markedly compared with that prior to transplantation. Local pain
was alleviated and the patients felt improvements in their
condition. The numbness disappeared and the intermittent
claudication symptom was improved. In addition, patients were able
to walk for increased distances (Table
I).
 | Table I.Comparisons of the evaluation
indicators of the patients with diabetes prior to and following
stem cell transplantation. |
Table I.
Comparisons of the evaluation
indicators of the patients with diabetes prior to and following
stem cell transplantation.
| Parameter |
Pre-transplantation |
Post-transplantationa | t value | P-value |
|---|
| Intermittent
claudication score |
3.31±0.62 |
1.17±0.66 |
7.630 | <0.01 |
| Skin temperature
(°C) | 31.45±1.36 | 32.11±1.23 |
7.625 | <0.01 |
| Ankle brachial
index |
0.28±0.98 |
0.50±0.12 | −9.427 | <0.01 |
| Pain score |
2.30±0.89 |
1.79±0.38 | −3.539 | <0.01 |
| CTA score |
1.22±0.15 |
2.35±0.784 |
6.348 | <0.01 |
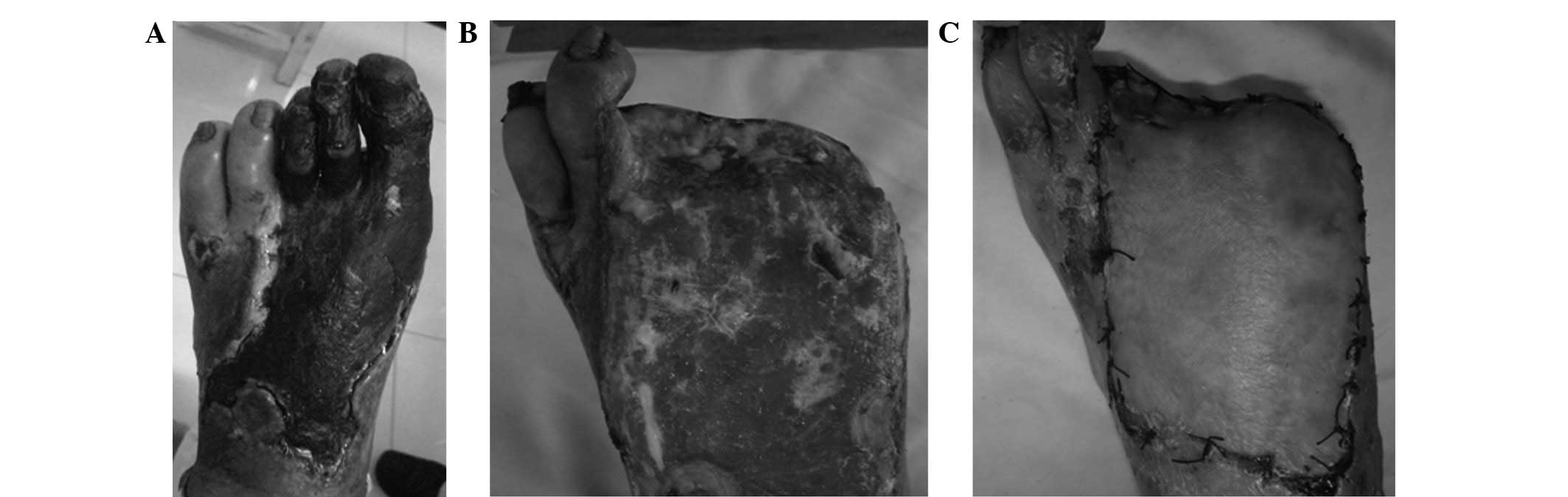
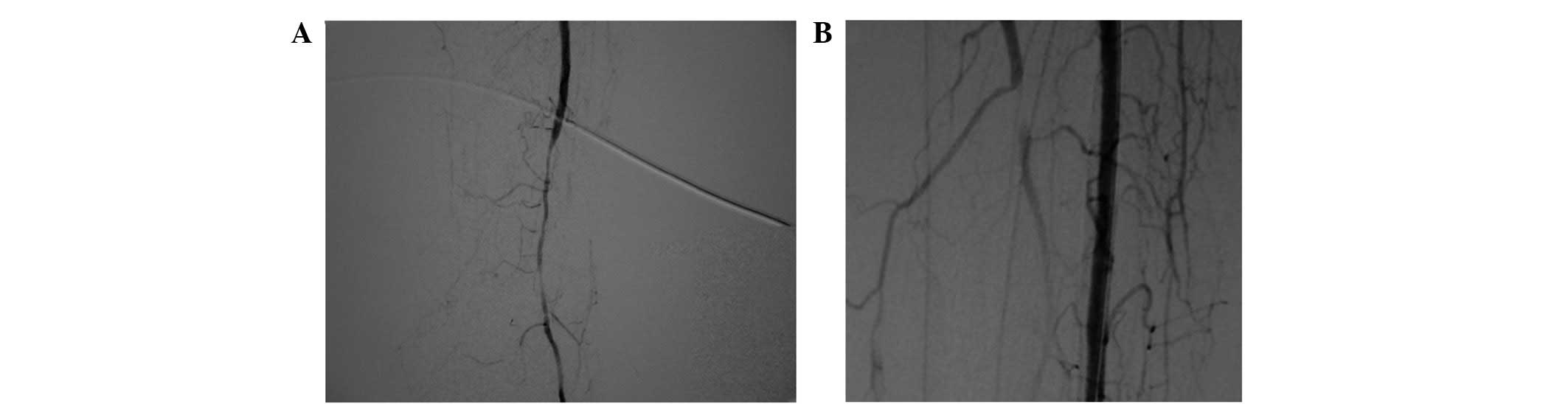
Report of a typical case
Patient A was a 75 year-old male with a 32-year
history of diabetes, who was admitted to the Weifang People's
Hospital due to a left diabetic foot gangrene concurrent infection
(Fig. 1A). Preoperative
lower-extremity DSA showed that the blood vessels below the
popliteal artery branch were occluded extensively with no distal
outflow; however, small amounts of local collateral circulation
remained (Fig. 2A). The patient
additionally exhibited coronary heart disease, hypertension,
cerebrovascular disease, transient ischemic attack and cerebral
infarction. Patient A was thus unable to undergo amputation.
Following extensive debridement, the patient received the
autologous peripheral blood stem cell transplantation. After 3
weeks, fresh granulation growth was observed when the patient
returned to the hospital for further debridement (Fig. 1B). The patient subsequently underwent
an in situ dermatoplasty. At 2 weeks after this skin graft,
the wounds appeared to be healing well (Fig. 1C). Postoperative CTA examination
showed that extensive collateral circulation was widely established
along the lesion vessels (Fig. 2B).
At a 3-year follow-up examination, the local wound of the patient
was observed to have healed well and the walking function of the
lower extremities was predominantly maintained.
Discussion
When the body is in an ischemic state, new blood
vessels are generated as a compensatory mechanism. This
neoangiogenesis includes two key processes: Angiogenesis and
vascularization. Vascularization refers to the generation of new
blood vessels through the differentiation and interaction of
endothelial progenitor cells (EPCs) and hematopoietic stem cells,
in environments with no original vascular system. It is
conventionally believed that the further differentiation of EPCs
into vascular endothelial cells to form a new vascular system does
not occur in vivo following birth. In 1997, however, Asahara
et al (15) observed that
EPCs are present in the blood circulation, exhibiting chemotaxis
and homing abilities to the ischemic tissues and differentiating to
form new blood vessels. These results verified the existence of
‘postnatal vascularization’. Ischemic animal model studies indicate
that endothelial progenitor cells are able to enter a vascularizing
area and increase the generation of collateral vessels in ischemic
tissues (16–18).
In 1997, Asahara et al (15) were the first to identify that
peripheral blood CD34+ and vascular endothelial growth
factor receptor 2+ (VEGFR-2+) cells are able
to proliferate in vitro and transform into vascular
endothelial cells. It has subsequently been generally accepted that
CD133+, VEGFR-2+ and CD34+ bone
marrow-derived cells possess the ability to differentiate into EPCs
(19). During the differentiation of
such cells, the expression of CD133 is gradually downregulated and
the expression levels of CD31, von Willebrand factor and cadherin
in vascular endothelial cells increase gradually, facilitating the
formation of mature endothelial cells (20).
It is currently believed that vascularization and
angiogenesis coexist in the embryonic development period, in
addition to participating in numerous physiological and
pathological processes following birth (21). These processes are involved in the
dynamic maintenance and physiological reconstruction of blood
vessels and are dependent on the postnatal angiogenic activity of
EPC. The concept of ‘therapeutic angiogenesis’ refers to the
application of exogenous vasoformative factors and/or the
transfusion of vasoformative cells into ischemic tissues to promote
angiogenesis and the formation of collateral vessels, in order to
improve blood supply and treat ischemic diseases (22). This therapeutic approach is a
physiological strengthening treatment, which utilizes the presence
of EPCs in the adult blood circulation and the fact that these EPCs
exhibit the biological characteristics of chemotaxis and homing
abilities to ischemic tissues, as well as their differentiation to
form new blood vessels.
Stem cell transplantation may involve a variety of
cell types, including autologous peripheral blood, bone marrow
mesenchymal (23), autologous bone
marrow (24) and umbilical cord
blood (25,26) stem cells. The collection of bone
marrow requires epidural anesthesia or general anesthesia and is
more stressful for the general condition of a patient. In addition,
large quantities of bone marrow (≤500 ml) may be required, and
therefore certain patients are physically and psychologically
unable to undergo this treatment. In recent years, studies
concerning autologous peripheral blood stem cell transplantation
have achieved marked progress (27–29). The
autologous peripheral blood stem cell transplantation procedure is
simple and readily accepted by patients. In order to increase the
content of stem cells and improve the curative effect of stem cell
transplantation, recombinant human G-CSF can be used to stimulate
the proliferation of bone marrow stem cells and promote their
release into the peripheral blood. Recently, the wide application
of cytokines and blood cell separation techniques has facilitated
the mobilization of bone marrow hematopoietic stem cells into the
peripheral blood circulation, as well as their purification. Due to
the mobilization of bone marrow, blood cell separation and
centrifugal concentration, the concentration and number of stem
cells available for use in treatment have been markedly increased.
In the present study, following peripheral blood stem cell
transplantation, symptoms including pain, cold sensations in the
affected limb, intermittent claudication and ulcers were notably
improved. At 1 month after transplantation, the peripheral blood
flow amplitude and blood perfusion volume, detected by laser
Doppler scanning, were improved significantly compared with the
results prior to the transplantation. DSA imaging of the lower
artery showed that new collateral vessel formation had increased
significantly. Based on the comprehensive assessment of the
indicators of the patients prior to and following stem cell
transplantation, the present study indicates that autologous
peripheral blood stem cell transplantation is able to effectively
increase the blood flow in the lower limbs, which may permit
certain patients to avoid amputation or reduce the height along the
limb at which amputation is conducted.
Stem cells are predominantly located in the bone
marrow. Stem cells in the peripheral blood are equivalent to 0.1–1%
of the stems cells in the bone marrow, and CD34+ cells
account for 0.01–0.1% of PBMNCs. In order to increase the content
of stem cells, G-CSF is used to stimulate the proliferation of stem
cells in the bone marrow and subsequently promote their release
into the peripheral blood. This is the primary method used in stem
cell transplantation treatments to mobilize stem cells, and may be
used in peripheral blood stem cell transplantations for the
treatment of ischemic disease of the lower extremities.
Furthermore, it represents a mature method of mobilization.
Generally, 4–5 days after the administration of G-CSF, the number
of CD34+ cells in the peripheral blood can reach 40- to
80-fold of that prior to mobilization; however, if the
administration of G-CSF is discontinued for 1 week, the number of
CD34+ cells in the peripheral blood is gradually
restored to the baseline level. In addition, G-CSF can mobilize
bone marrow-derived EPCs into the peripheral blood circulation and
promote the angiogenesis in the ischemic area.
In summary, the results of the present study
demonstrate that treating ischemia of the lower extremities with
recombinant human G-CSF-mobilized peripheral blood stem cell
transplantation is able to effectively increase the blood supply of
the lower extremities in patients with diabetic foot. In the short
term following stem cell transplantation, pain in the affected limb
was relieved and the cold sensations in the limbs were gradually
mitigated. Clinical symptoms were evidently improved and the ulcers
healed gradually. The quality of life of the patients improved
notably. Thus, we suggest that the improvement of blood supply in
the short term may result from the locally increased quantities of
blood caused by the aseptic inflammation following transplantation,
while the continuous improvement in the local blood supply of the
patients may be associated with EPC-related angiogenesis. Two
dosages of G-CSF (5 and 10 µg/kg/day) were used to mobilize the
stem cells for 4–7 days in this study. The adverse reactions that
occurred in the process of mobilization and the collection stage,
including mild pain, were within tolerable limits for the patients.
Furthermore, no adverse reaction was observed during the clinical
follow-up. The application of 5 and 10 µg/kg/day G-CSF for 4 or 5
days may be a clinically useful approach, therefore, for the
mobilization and gathering of stem cells.
Acknowledgements
This study was supported by the 2012 Plan Projects
of the Development of Science and Technology of Weifang City (no.
20121188).
References
|
1
|
Tepper OM, Galiano RD, Kalka C and Gurtner
GC: Endothelial progenitor cells: The promise of vascular stem
cells for plastic surgery. Plast Reconstr Surg. 111:846–854. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shintani S, Murohara T, Ikeda H, Ueno T,
Honma T, Katoh A, Sasaki K, Shimada T, Oike Y and Imaizumi T:
Mobilization of endothelial progenitor cells in patients with acute
myocardial infarction. Circulation. 103:2776–2779. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tepper OM, Galiano RD, Capla JM, Kalka C,
Gagne PJ, Jacobowitz GR, Levine JP and Gurtner GC: Human
endothelial progenitor cells from type II diabetics exhibit
impaired proliferation, adhesion and incorporation into vascular
structures. Circulation. 106:2781–2786. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tavakoli M, Boulton AJ, Efron N and Malik
RA: Increased Langerhan cell density and corneal nerve damage in
diabetic patients: Role of immune mechanisms in human diabetic
neuropathy. Cont Lens Anterior Eye. 34:7–11. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Georgiadis GS, Georgakarakos EI, Antoniou
GA, Panagoutsos S, Argyriou C, Mourvati E, Passadakis P and
Lazarides MK: Correlation of pre-existing radial artery
macrocalcifications with late patency of primary radiocephalic
fistulas in diabetic hemodialysis patients. J Vasc Surg.
60:462–470. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Pittengey MF, Mackay AM, Beck SC, Jaiswal
RK, Douglas R, Mosca JD, Moorman MA, Simonetti DW, Craig S and
Marshak DR: Multilineage potential of adult human mesenchymal stem
cells. Science. 284:143–147. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Thomson JA, Itskovitz-Eldor J, Shapiro SS,
Waknitz MA, Swiergiel JJ, Marshall VS and Jones JM: Embryonic stem
cell lines derived from human blastocysts. Science. 282:1145–1147.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lawall H, Bramlage P and Amann B:
Treatment of peripheral arterial disease using stem and progenitor
cell therapy. J Vasc Surg. 53:445–453. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Van Duong Huyen JP, Smadia DM, Bruneval P,
Gaussem P, Dal-Cortivo L, Julia P, Fiessinger JN, Cavazzana-Calvo
M, Aiach M and Emmerich J: Bone marrow-derived mononuclear cell
therapy induces distal angiogenesis after local injection in
critical leg ischemia. Modern Pathol. 21:837–846. 2008. View Article : Google Scholar
|
|
10
|
Li H, Chen X, Zhou B, Feng L, Xiao P and
Wu W: Stem cell mobilization and collection for autologous
peripheral blood stem cells transplantation in diabetic foot
treatment. Zhong Guo Zu Zhi Gong Cheng Yan Jiu Yu Lin Chuang Kang
Fu. 15:8508–8512. 2011.(In Chinese).
|
|
11
|
To LB, Haylock DN, Simmons PJ and Juttner
CA: The biology and clinical uses of blood stem cells. Blood.
89:2233–2258. 1997.PubMed/NCBI
|
|
12
|
Kalka C, Masuda H, Takahashi T, Kalka-Moll
WM, Silver M, Kearney M, Li T, Isner JM and Asahara T:
Transplantation of ex vivo expanded endothelial progenitor cells
for therapeutic neovascularization. Proc Natl Acad Sci USA.
97:3422–3427. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ahmad W, Khan IA, Ghaffar S, Al-Swailmi FK
and Khan I: Risk factors for diabetic foot ulcer. J Ayub Med Coll
Abbottabad. 25:16–18. 2013.PubMed/NCBI
|
|
14
|
Alberti KG and Zimmet PZ: Definition,
diagnosis and classification of diabetes mellitus and its
complications. Part 1: Diagnosis and classification of diabetes
mellitus provisional report of a WHO consultation. Diabet Med.
15:539–535. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Asahara T, Murohara T, Sullivan A, Silver
M, van der Zee R, Li T, Witzenbichler B, Schatteman G and Isner JM:
Isolation of putative progenitor endothelial cells for
angiogenesis. Science. 275:964–967. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yamamoto K, Kondo T, Suzuki S, Izawa H,
Kobayashi M, Emi N, Komori K, Naoe T, Takamatsu J and Murohara T:
Molecular evaluation of endothelial progenitor cells in patients
with ischemic limbs: Therapeutic effect by stem cell
transplantation. Arterioscler Thromb Vasc Biol. 24:e192–e196. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kim J, Kim M, Jeong Y, Lee WB, Park H,
Kwon JY, Kim YM, Hwang D and Kwon YG: BMP9 induces cord
blood-derived endothelial progenitor cell differentiation and
ischemic neovascularization via ALK1. Arterioscler Thromb Vasc
Biol. 35:2020–2031. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liang CJ, Shen WC, Chang FB, Wu VC, Wang
SH, Young GH, Tsai JS, Tseng YC, Peng YS and Chen YL: Endothelial
progenitor cells derived from Whartons jelly of human umbilical
cord attenuate ischemic acute kidney injury by increasing
vascularization and decreasing apoptosis, inflammation, and
fibrosis. Cell Transplant. 24:1363–1377. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Urbich C and Dimmeler S: Endothelial
progenitor cells: Characterization and role in vascular biology.
Circ Res. 95:343–353. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Schatteman GC and Awad O: Hemangioblasts,
angioblasts and adult endothelial cell progenitors. Anat Rec A
Discov Mol Cell Evol Biol. 276:13–21. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rousseau B, Larrieu-Lahargue F, Bikfalvi A
and Javerzat S: Involvement of fibroblast growth factors in
choroidal angiogenesis and retinal vascularization. Exp Eye Res.
77:147–156. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gluckman E and Rocha V: History of the
clinical use of umbilical cord blood hematopoietic cells.
Cytotherapy. 7:219–227. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lu D, Chen B, Liang Z, Deng W, Jiang Y, Li
S, Xu J, Wu Q, Zhang Z, Xie B and Chen S: Comparison of bone marrow
mesenchymal stem cells with bone marrow-derived mononuclear cells
for treatment of diabetic critical limb ischemia and foot ulcer: A
double-blind, randomized, controlled trial. Diabetes Res Clin
Pract. 92:26–36. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tateishi-Yuyama E, Matsubara H, Murohara
T, Ikeda U, Shintani S, Masaki H, Amano K, Kishimoto Y, Yoshimoto
K, Akashi H, et al: Therapeutic Angiogenesis using Cell
Transplantation (TACT) Study Investigators: Therapeutic
angiogenesis for patients with limb ischaemia by autologous
transplantation of bone marrow cells: A pilot study and a
randomized controlled trial. Lancet. 360:427–435. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Quirici N, Soligo D, Caneva L, Servida F,
Bossolasco P and Deliliers GL: Differentiation and expansion of
endothelial cells from human bone marrow CD133(+) cells. Br J
Haematol. 115:186–194. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pesce M, Orlandi A, Iachininoto MG,
Straino S, Torella AR, Rizzuti V, Pompilio G, Bonanno G, Scambia G
and Capogrossi MC: Myoendothelial differentiation of human
umbilical cord blood derived stem cells in ischemic limb tissues.
Circ Res. 93:51–62. 2003. View Article : Google Scholar
|
|
27
|
Alonso S, Cabrero M, Caballero JC, Dávila
J, de la Calle VG, López-Godino O, López-Corral L, Pérez E, Vázquez
L, Corral R, et al: Acute graft-versus-host disease and
bronchiolitis obliterans after autologous stem cell transplantation
in a patient with multiple myeloma. Clin Case Rep. 3:370–375. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hayase T, Morimoto A, Kawahara Y, Yagi M,
Kanai N, Nobusawa S, Hirato J and Gomi A: An infant with
medulloepithelioma successfully treated by high-dose chemotherapy
followed by autologous peripheral blood stem cell transplantation
without radiotherapy. J Pediatr Hematol Oncol. 37:e394–e398. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Eid KA, Miranda EC and Aguiar Sdos S:
Mobilization and collection of CD34(+) cells for autologous
transplantation of peripheral blood hematopoietic progenitor cells
in children: analysis of two different granulocyte-colony
stimulating factor doses. Rev Bras Hematol Hemoter. 37:160–166.
2015. View Article : Google Scholar : PubMed/NCBI
|