Introduction
Chronic liver disease is considered a major cause of
mortality worldwide, and particularly in Asia (1). The majority of chronic liver diseases
are initiated by hepatitis B virus (HBV) and hepatitis C virus
(HCV) infection (2,3). More than half a million people with HBV
infection die annually from complications of chronic hepatitis B,
such as hepatic cirrhosis and liver cancer (4). Liver transplantation has been shown to
be the most effective therapy for patients with advanced liver
disease (5). Transplantation offers
patients, whose lives have been severely restricted or almost
succumbed to the disease, a marked improvement in their health and
well-being; however, the demand for organ transplants outreaches
the number of donated organs (6).
Organ donation after cardiac death (DCD) could maximize the use of
these scarce resources. Previously known as non-heart-beating organ
donation, DCD has been an end-of-life option for >30 years in
the USA and Europe (7). DCD is
performed in cases where life support is withdrawn from a patient
after a physician has determined that there is no long-term
prognosis for recovery, or in patients who do not meet the criteria
for neurological death. The option of DCD should be offered prior
to life support withdrawal, but only after the decision to withdraw
has been reached (8).
Initially, DCD presented various limitations, such
as poor organ function following transplantation. However, advances
in medication and surgical techniques have markedly improved the
outcomes for recipients of DCD organs. These advances, along with
the severe shortage of donated organs promote DCD as an alternative
for patients and families (8).
The use of DCD organs has rapidly developed in China
since the establishment of DCD standard by the Red Cross Society
and Ministry of Health of China in 2010 (9). The aim of the present study was to
document successful liver transplantation using DCD organs and
promote the development of these transplantation techniques in
China.
The present single-centre study reports 6 liver
transplantations performed with DCD organs, including 5 liver
transplants and 1 liver-kidney combined transplant.
Case report
Between January 2011 and December 2013, 6 liver
transplantations (including 1 liver-kidney and 5 liver transplants)
were performed with DCD organs at the 303 Hospital of People's
Liberation Army (Nanning, China), with the approval of the Medical
Ethics Committee at this institution. Written informed consent was
obtained from all patients. Transplant decisions were made
according to the availability of donors, blood type and
cross-matching. The 6 transplant recipients were males aged 35–47
years, who suffered from cirrhosis-induced hepatic decompensation
(3 cases), primary liver cancer (2 cases) or hepatic decompensation
combined with renal failure (1 case). Table I lists information obtained from the
evaluation of the recipients.
 | Table I.Recipient information. |
Table I.
Recipient information.
| Recipient | Age, years | Gender | APACHE II score | MELD | Estimated mortality,
% |
|---|
| 1 | 42 | Male | 7 | 9 | 8 |
| 2 | 35 | Male | 14 | 38 | 12 |
| 3 | 37 | Male | 9 | 41 | 15 |
| 4 | 40 | Male | 11 | 34 | 11 |
| 5 | 47 | Male | 12 | 37 | 9 |
| 6 | 43 | Male | 6 | 13 | 25 |
Acute physiology and chronic health evaluation II
(APACHE II) scoring system and the model for end-stage liver
disease (MELD) were used to evaluate the severity of liver disease
in the recipients. APACHE II point scores are based upon values of
12 routine physiologic measurements, age and previous health
status, in order to provide a general measure of the severity of
disease (10). MELD predicts liver
disease severity based on serum creatinine, serum total bilirubin
and international normalized ratio (INR) (11).
In total, 42 DCD livers were collected between
January 2011 and December 2013 at the 303 Hospital of People's
Liberation Army from male patients aged 30–53 years, who succumbed
to cerebral hemorrhage (13 cases) or traumatic brain injury (29
cases). The donation procedure followed the DCD guidelines of China
(9). Of these, 32 donor livers were
not procured due to alcoholic cirrhosis, liver cancer, hepatic
distomiasis and long durations of hepatic warm ischemia (>30
min). Therefore, 10 DCD livers were successfully procured for
transplantation, 4 of which were distributed to other centers
through the Red Cross Society of China (Beijing, China).
Transplantations of the remaining 6 livers were performed at the
303 Hospital of People's Liberation Army.
Preoperative evaluation was performed on all donors,
and were found to be negative for human immunodeficiency virus,
hepatitis B surface antigen, HCV antibody and syphilis antibody
(12). The blood oxygenation status
and hemodynamics were maintained by the intensive care unit (ICU)
group. Based on the stability of hemodynamics and blood oxygenation
status, 5 donors were further supported with extracorporeal
membrane oxygenation (ECMO) for 6–10 h prior to organ retrieval.
The 6 donors underwent controlled cardiac death, with planned
withdrawal of ventilatory and organ-perfusion support in the face
of catastrophic illness (Maastricht classification class III; 13).
The University of Wisconsin score (UW; 14) was found to be 21–23
(Table II). The cardiac death
occurred immediately following the withdrawal of life support, and
the warm ischemia time was kept to within 10 min. Following the
confirmation of cardiac death, the DCD organs were procured by a
combined abdominal organ retrieval procedure (15). Table
II lists the relevant information of all 6 donors.
| Table II.Donor information. |
Table II.
Donor information.
| Donor | Age, years | Gender | Cause of
mortality | UW score | WI length, min | CI, h |
|---|
| 1 | 32 | Male | Traumatic brain
injury | 21 | 5.6 | 6.8 |
| 2 | 30 | Male | Cerebral
hemorrhage | 22 | 6.1 | 8.3 |
| 3 | 37 | Male | Traumatic brain
injury | 23 | 6.7 | 9.5 |
| 4 | 53 | Male | Cerebral
hemorrhage | 22 | 7.9 | 7.8 |
| 5 | 42 | Male | Traumatic brain
injury | 23 | 8.4 | 8.1 |
| 6 | 43 | Male | Traumatic brain
injury | 21 | 9.5 | 9.5 |
Orthotopic liver transplantation (OLT) was then
performed in the 6 liver transplant recipients. Liver
transplantation by classical caval reconstruction was performed on
3 of the recipients (nos. 1, 3 and 6; Table I), while 2 recipients (nos. 2 and 4)
received non-bypass OLT and 1 recipient (no. 5) underwent the
piggy-back technique.
The immunity of the recipient was suppressed through
the induction of rabbit anti-human T lymphocyte immunoglobulinG
CD25 polyclonal antibody (100 mg/5 ml saline; S20090069; Fresenius
Biotech GmBH, Grafelfing, Germany), followed by tacrolimus (0.15
mg/kg per day; Astellas Pharma China, Inc., Shanghai, China) and
mycophenolate mofetil (3 mg/day; Roche Diagnostics, Shanghai,
China). Postoperatively, all patients were maintained in the ICU
for 5–10 days and received routine monitoring of vital signs and
organ functions. The anastomotic sites of the transplanted livers
were regularly monitored using color Doppler sonography. With
regard to the patient that received the liver-kidney combined
transplant, the renal artery resistance index and renal blood
supply of the transplanted kidney were regularly examined.
Recipients were administered 0.15 mg/kg micafungin sodium (Astellas
Pharma China, Inc.) daily for the first 7–14 days following
transplantation in order to prevent and treat inflammation.
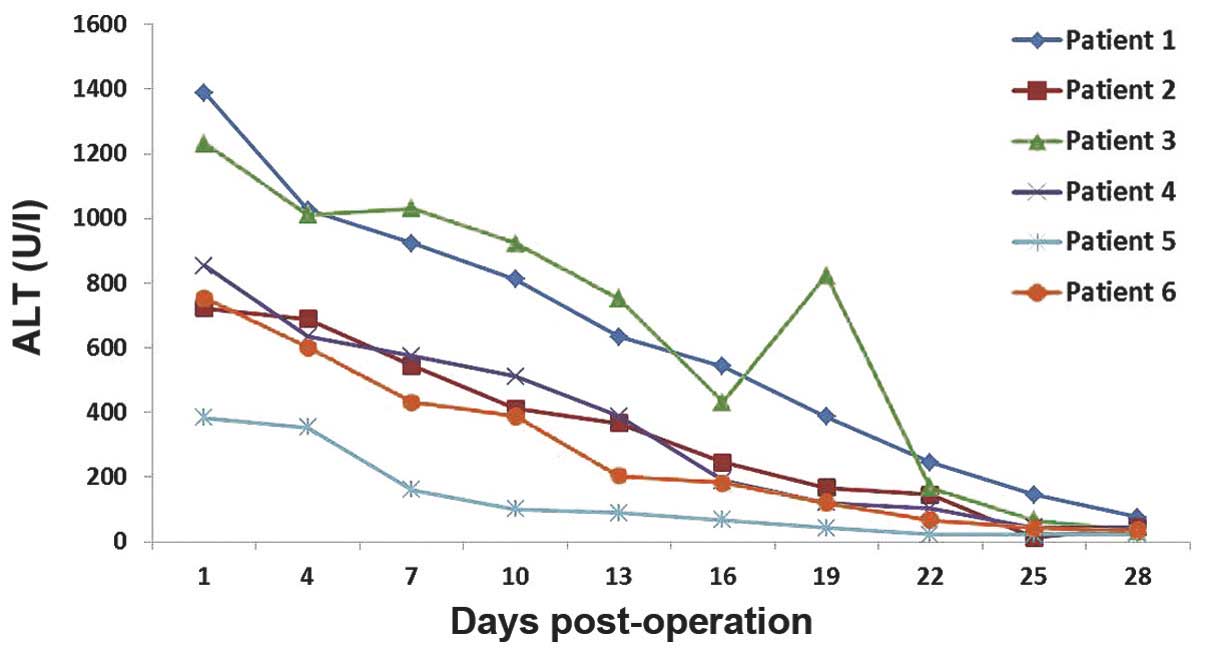
The 6 recipients recovered considerably well without
significant complications, such as primary graft failure,
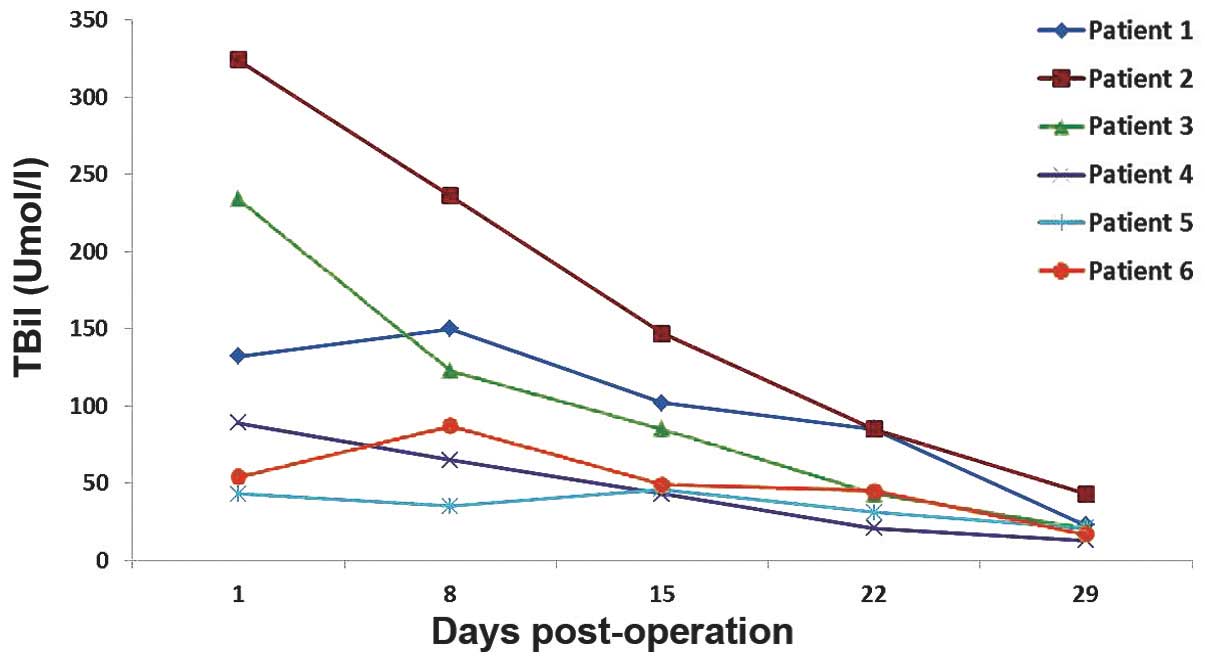
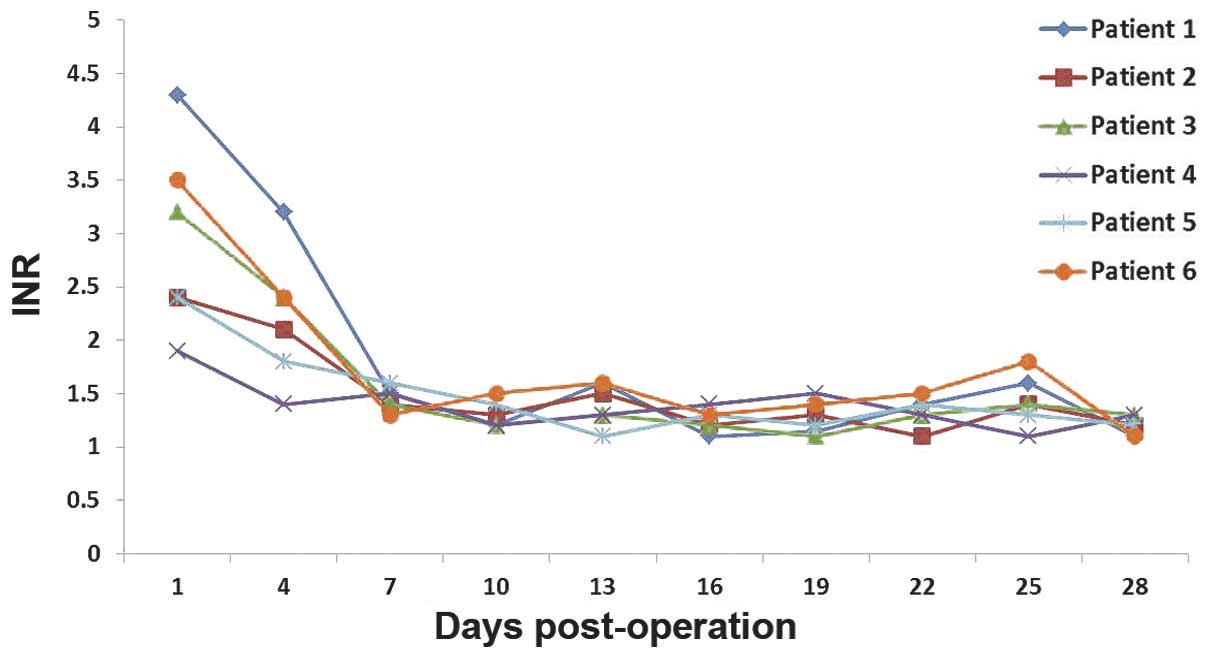
thrombosis, graft rejection or biliary stricture. The dynamic
changes of serum alanine transaminase (ALT; Fig. 1), total bilirubin (TBil; Fig. 2) and INR (Fig. 3) were routinely recorded. The patient
that received the liver-kidney combined transplant presented normal
urine levels immediately following surgery (2,500 mlday) and the
serum creatinine (Cr) levels had returned to the normal values
within 7 days. All liver recipients were discharged from the
hospital within 20–30 days after the transplantation. Their liver
function remained normal during the entire follow-up period, which
lasted up to 24 months.
Discussion
At present, the data for the long-term outcomes of
OLT using DCD livers are controversial. Certain studies using
pooled registry data (16,17) have reported inferior transplant
outcomes of DCD compared with donation following brain death (DBD),
while single-center studies have shown comparable survival outcomes
for the two types of organ donation (18,19).
Since a DBD program has not yet been established in China, the use
of DCD as a strategy to increase the limited availability of donor
livers is critical.
In the present study, controlled class III cardiac
death was observed in the 6 donors. The relatively short warm
ischemia time was ensured by a high-risk UW score following the
withdrawal of life support. The warm ischemia time of these 6
donors was found to be <10 min. Recent reports have indicated
that the survival of DCD grafts, as well as their recipients, are
significantly affected by complications, including primary
non-function, hepatic artery thrombosis and ischemic cholangiopathy
(20,21). Such complications, however, did not
occur in any of the 6 recipients of the present study. Recipient 2
exhibited a high TBil, which may be associated with his
preoperative status (MELD 38) or the quality of the transplanted
liver. MELD is widely used to predict the severity of liver disease
and is proportionally correlated with mortality risk (11). The high TBil of recipient 3 was due
to the moderate steatosis observed in the DCD liver. A rapid
decease in TBil was observed in recipients 1, 4, 5 and 6, who had
low MELD scores and did not present liver steatosis. In recipients
2 and 3, the increase in INR may have been due to the high MELD
scores and presence of liver steatosis.
The use of fatty livers (with steatosis) as grafts
is relatively risky, since it has been found that the incidence of
primary non-function in transplant recipients with liver steatosis
is considerably higher compared with that in patients with normal
livers (22). The early malfunction
of grafted livers is proportionally associated with the extent of
liver steatosis (23). A comparative
study on the 3-month survival rate following liver implantation,
length of stay in the ICU and hospital, as well as Child-Pugh
evaluation (24) and liver function,
demonstrated that the prognosis was not significantly affected by
mild (10–30%) or moderate (30–60%) steatosis of the grafted liver
(25). Kwon et al (26) analyzed 245 liver transplants with
mild steatosis between 1999 and 2005, and divided the liver
recipients into three groups, according to the degree of liver
steatosis (the 0–9, 10–19 and 20–30% groups). No statistically
significant differences were observed in detected parameters,
including length of surgery, blood loss, peak value of TBil, serum
aspartate aminotransferase and incidence of complications, among
the three groups. The results were similar to those observed in 30
and 50% alcoholic cirrhosis livers (27). In the present study, 3 liver
transplant recipients with moderate hepatic steatosis (recipients
4, 5 and 6) exhibited high ALT and TBil levels, which returned to
the normal levels on day 17 following transplantation. In patients
with normal liver grafts (recipients 1 and 2), ALT reached 200–400
Ul and returned to its normal levels on days 7 (recipient 1) and 9
(recipient 2) following transplantation. Notably, recipient 3
exhibited a fast recovery of liver function without any indication
of hepatic steatosis.
China is of the counties with the highest demands of
liver transplants worldwide, mainly due to the extremely high
incidence of HBV and liver cancer (28). The appropriate application of DCD may
be able to maximize the use of these scarce resources, in order to
save more lives. In the present study, the transplantation of DCD
livers with moderate steatosis indicated that controlled class III,
high UW score and short warm ischemia time are essential factors in
determining the success of transplantation. ECMO was able to
maintain steady hemodynamics and high blood oxygenation, thereby
improving donor liver function prior to organ retrieval, which
played an important role in the successful short- and long-term
outcomes of liver transplantation.
Acknowledgements
This study was supported by grants from the Guangxi
Natural Science Foundation (no. 2013GXNSFAA019253) and Guangxi
Science and Technology Development Project (no. 14124003-8).
References
|
1
|
Wang FS, Fan JG, Zhang Z, Gao B and Wang
HY: The global burden of liver disease: The major impact of China.
Hepatology. 60:2099–2108. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lai CL, Ratziu V, Yuan MF and Poynard T:
Viral hepatitis B. Lancet. 362:2089–2094. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Poynard T, Yuan MF, Ratziu V and Lai CL:
Viral hepatitis C. Lancet. 362:2095–2100. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cholongitas E, Tziomalos K and Pipili C:
Management of patients with hepatitis B in special populations.
World J Gastroenterol. 21:1738–1748. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Watt KD: Keys to long-term care of the
liver transplant recipient. Nat Rev Gastroenterol Hepatol.
12:639–648. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hackl C, Schlitt HJ, Kirchner GI, Knoppke
B and Loss M: Liver transplantation for malignancy: Current
treatment strategies and future perspectives. World J
Gastroenterol. 20:5331–5344. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Morrissey PE and Monaco AP: Donation after
circulatory death: current practices, ongoing challenges, and
potential improvements. Transplantation. 97:258–264. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Manara AR, Murphy PG and O'Callaghan G:
Donation after circulatory death. Br J Anaesth. 108(Suppl 1):
i108–i121. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Liu Y: Establishment of human organ
donation system in China - resolving the issues of organ sources
and standardizing the procedures of organ transplantation. Zhong
Hua Qi Guan Yi Zhi Za Zhi. 31:390–392. 2010.(In Chinese).
|
|
10
|
Knaus WA, Draper EA, Wagner DP and
Zimmerman JE: APACHE II. A severity of disease classification
system. Crit Care Med. 13:818–829. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wiesner R, Edwards E, Freeman R, Harper A,
Kim R, Kamath P, Kremers W, Lake J, Howard T, Merion RM, et al:
United Network for Organ Sharing Liver Disease Severity Score
Committee: Model for end-stage liver disease (MELD) and allocation
of donor livers. Gastroenterology. 124:91–96. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liu YF: Assessment of organs from cardiac
death donors and in vitro preparation. Zhong Hua Qi Guan Yi Zhi Za
Zhi. 31:393–396. 2010.(In Chinese).
|
|
13
|
Kootstra G, Daemen JH and Oomen AP:
Categories of non-heart-beating donors. Transplant Proc.
27:2893–2894. 1995.PubMed/NCBI
|
|
14
|
Lewis J, Peltier J, Nelson H, Snyder W,
Schneider K, Steinberger D, Anderson M, Krichevsky A, Anderson J,
Ellefson J and D'Alessandro A: Development of the University of
Wisconsin donation After Cardiac Death Evaluation Tool. Prog
Transplant. 13:265–273. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Issa S and Al-Bishri S: The role of early
identification of superior mesenteric artery in a modified
technique for retrieval of abdominal organs for transplantation.
Saudi J Kidney Dis Transpl. 19:389–396. 2008.PubMed/NCBI
|
|
16
|
Johnson RJ, Bradbury LL, Martin K and
Neuberger J: UK Transplant Registry: Organ donation and
transplantation in the UK-the last decade: A report from the UK
national transplant registry. Transplantation. 97(Suppl 1): S1–S27.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Callaghan CJ, Charman SC, Muiesan P,
Powell JJ, Gimson AE and van der Meulen JH: UK Liver Transplant
Audit: Outcomes of transplantation of livers from donation after
circulatory death donors in the UK. A cohort study. BMJ Open.
3:e0032872013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Dubbeld J, van Hoek B and Ringers J: Use
of a liver from donor after cardiac death: Is it appropriate for
the sick or the stable? Curr Opin Organ Transplant. 16:239–242.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Grewal HP, Willingham DL, Nguyen J, Hewitt
WR, Taner BC, Cornell D, Rosser BG, Keaveny AP, Aranda-Michel J,
Satyanarayana R, et al: Liver transplantation using controlled
donation after cardiac death donors: An analysis of a large
single-center experience. Liver Transpl. 15:1028–1035. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jay C, Ladner D, Wang E, Lyuksemburg V,
Kang R, Chang Y, Feinglass J, Holl JL, Abecassis M and Skaro AI: A
comprehensive risk assessment of mortality following donation after
cardiac death liver transplant - an analysis of the national
registry. J Hepatol. 55:808–813. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Foley DP, Fernandez LA, Leverson G,
Anderson M, Mezrich J, Sollinger HW and D'Alessandro A: Biliary
complications after liver transplantation from donation after
cardiac death donors: An analysis of risk factors and long-term
outcomes from a single center. Ann Surg. 253:817–825. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Neuberger J: Transplantation: Assessment
of liver allograft steatosis. Nat Rev Gastroenterol Hepatol.
10:328–329. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ureña MA, Ruiz-Delgado FC, González EM,
Segurola CL, Romero CJ, García IG, González-Pinto I and Sanz Gómez
R: Assessing risk of the use of livers with macro and
microsteatosis in a liver transplant program. Transplant Proc.
30:3288–3291. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Pugh RN, Murray-Lyon IM, Dawson JL,
Pietroni MC and Williams R: Transection of the oesophagus for
bleeding oesophageal varices. Br J Surg. 60:646–649. 1973.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nikeghbalian S, Nejatollahi SM, Salahi H,
Bahador A, Sabet B, Jalaeian H, Geramizadeh B, Dehghani SM and
Malek-Hosseini SA: Does donor's fatty liver change impact on early
mortality and outcome of liver transplantation? Transplant Proc.
39:1181–1183. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kwon CH, Joh JW, Lee KW, Kim SJ, Han YS,
Park JW, Kim DJ, Park JB and Lee SK: Safety of donors with fatty
liver in liver transplantation. Transplant Proc. 38:2106–2107.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cho JY, Suh KS, Kwon CH, Yi NJ, Kim MA,
Jang JJ, Minn KW and Lee KU: Auxiliary partial orthotopic living
donor liver transplantation in a patient with alcoholic liver
cirrhosis to overcome donor steatosis. Transpl Int. 19:424–429.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chen JG and Zhang SW: Liver cancer
epidemic in China: Past, present and future. Semin Cancer Biol.
21:59–69. 2011. View Article : Google Scholar : PubMed/NCBI
|