Introduction
Internal carotid artery dissection (ICAD) is a
significant cause of ischemic stroke, and accounts for ≤25% of
ischemic strokes in young and middle-aged patients (1). The majority (70%) of patients are
reported to be <50 years old, with a slight predominance of male
patients (2,3). Common symptoms of carotid artery
dissection include pain, partial Horner syndrome, cranial nerve
palsies and cerebral ischemia (4).
Obtaining a clinical diagnosis can be challenging; however, with an
increased awareness and the use of modern instruments of
investigation, such as magnetic resonance imaging and computed
tomography angiography, the diagnosis of carotid dissection has
become increasingly sophisticated (5). The prognosis of patients is variable;
the disease may be asymptomatic, but may cause profound
neurological deficits or even mortality (6). Medical treatment with anticoagulation
or antiplatelet therapy, such as warfarin, heparin, rivaroxaban and
aspirin, is the predominant treatment modality employed to prevent
thromboembolic complications from arterial dissections (1); however, they may be unsuitable in
certain cases of dissecting aneurysms (7,8). The
placement of a covered stent has emerged as a promising therapeutic
strategy for the treatment of aneurysms (9). In particular, minimally invasive
endovascular treatment with a Willis covered stent has been
proposed as a safe, durable and curative therapy for selected
intracranial aneurysms (10,11). However, to the best of our knowledge,
the use of a stent graft specifically designed for intracranial
vasculature, such as the Willis expanded
polytetrafluoroethylene-covered stent, has yet to be explored in
the treatment of patients with ICAD. The present study reports a
case of ICAD with the major complaint of recurrent left limb
weakness. As antithrombotic therapy resulted in no improvement,
Willis covered stent treatment was applied and resulted in an
improved outcome.
Case report
The present study was approved by the ethics
committee of Lishui Central Hospital (Lishui, China). A 52-year-old
male patient presented to our hospital on October 2, 2014, with the
primary complaint of recurrent left limb weakness for 2 months. The
patient had a history of hypertension for 5 years and was diagnosed
with transient cerebral ischemia in Qingtian People's Hospital
(Lishui, China) in September 2014. The patient was administered an
oral intensive therapy for 12 days in Qingtian People's Hospital,
including aspirin [100 mg once daily (qd); Bayer, Leverkusen,
Germany], clopidogrel (75 mg qd; Plavix; Sanofi S.A. Paris, France)
and atorvastatin (40 mg every night; Pfizer, Inc., Shanghai,
China), the patient's recurrent left limb weakness persisted. Upon
presentation to our hospital, blood pressure was recorded as
186/101 mmHg. This was treated with amlodipine (5 mg/day; China
Resources Saike Pharmaceutical Co., Ltd., Beijing, China) and
benazepril (10 mg/day; Shenzen Xinlitai Pharmaceutical Industry,
Ltd., Shenzen, China). The patient had not experienced any recent
injury or infections and revealed no other symptoms, such as pain
or dysphasia. Physical examination revealed no abnormalities of the
nervous system. Furthermore, laboratory tests and head magnetic
resonance imaging revealed no further abnormalities. The limb
muscle strength at the time of presentation was grade I–II
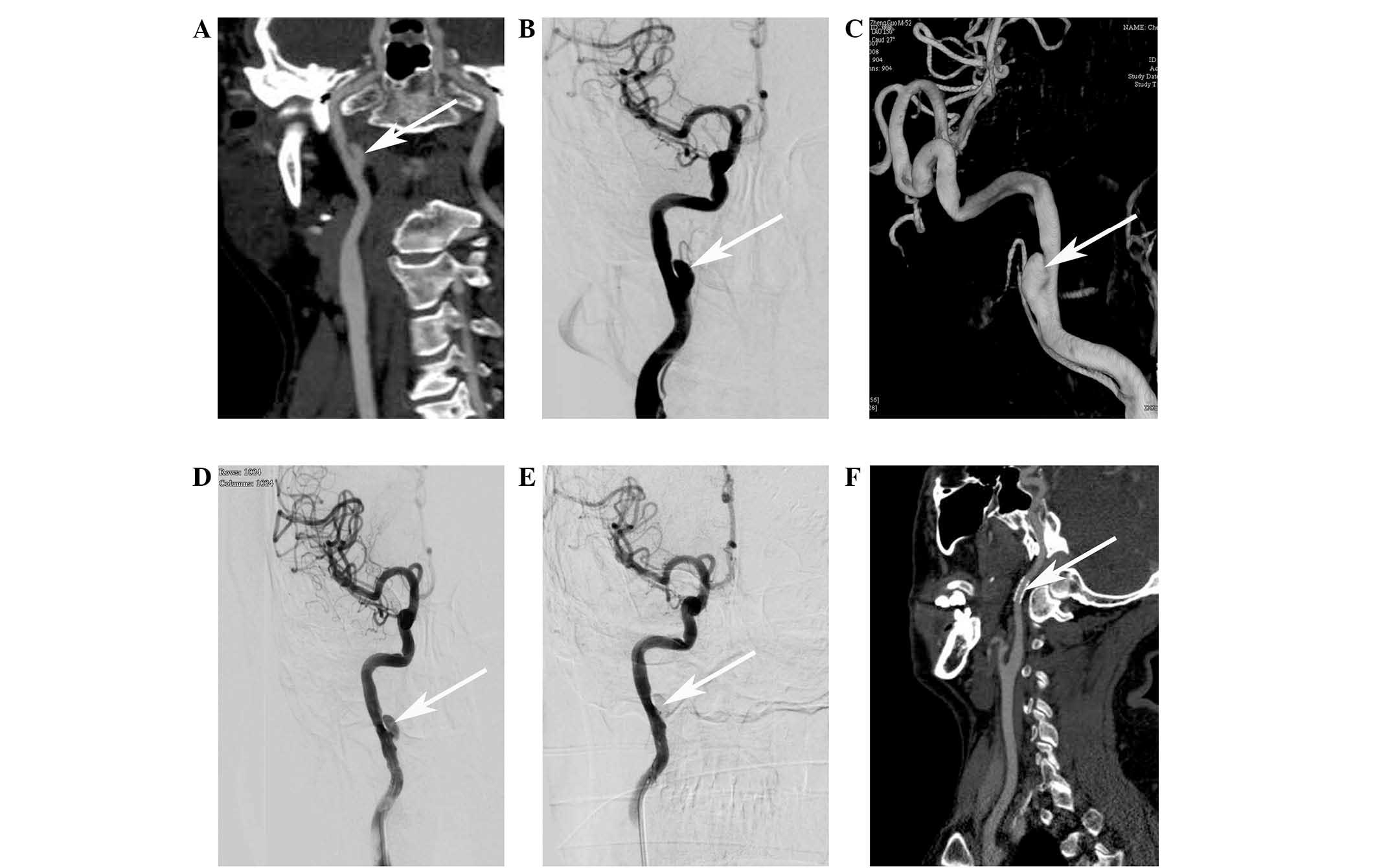
(12). Computed tomography
angiography (CTA) revealed a right ICAD located in the
oropharyngeal segment (Fig. 1A).
Digital subtraction angiography (DSA) was performed to further
assess the oropharyngeal segment of the right ICAD (Fig. 1B and C). The aneurysm measured 10 mm
in length and 5 mm in diameter, and was accompanied by a narrowed
internal carotid artery (ICA) lumen. Due to the risk of rupture and
bleeding with dissecting aneurysms or cerebral infarction by
arterial occlusion, in addition to the poor efficacy of
chemotherapy (13,14), endovascular interventional therapy
was performed using a Willis covered stent (MicroPort Medical Co.,
Ltd., Shanghai, China).
An endovascular procedure was performed under
regional anesthesia and full heparinization (6,000 units;
intravenous injection 5 min prior to surgery) of the patient. A
6-French Envoy guiding catheter (Codman & Shurtleff, Inc.,
Raynham, MA, USA) was placed in the proximal cervical segment of
the right ICA and a loach guidewire (Stryker Neurovascular, West
Valley City, UT, USA) was navigated into a distal branch of the
ICA. Using roadmap guidance, the Willis covered stent (4×16 mm;
MicroPort Medical Co., Ltd.) was navigated over the micro guidewire
and bridged the aneurysm orifice. DSA was performed to confirm the
positioning. The stent was then deployed with 10 atm pressure. DSA
was performed immediately after deflation of the balloon to confirm
the correct placement of the stent and minimal endoleakage was
observed (Fig. 1D). The graft was
re-inflated with 12 atm pressure to cover the orifice of the
dissecting aneurysm and to completely eliminate the endoleakage.
Repeated DSAs were performed immediately after the procedure to
confirm the disappearance of the residual cavity of the aneurysm
(Fig. 1E). During and after surgery,
the patient did not complain of discomfort and no neurological
deficits or complications were observed. Low molecular weight
heparin (4,000 units; Jiangsu Wanbang Biochemical Pharmaceuticals
Co., Ltd., Xuzhou, China) was subcutaneously injected 4 h after the
surgery and every 12 h thereafter for 3 days, and the patient was
then prescribed with oral clopidogrel (75 mg/day) and aspirin (100
mg/day) for 6 months. Follow-up CTA obtained 3 months after the
procedure revealed complete exclusion of the aneurysm and patency
of the parental artery (Fig.
1F).
Discussion
ICAD is most frequently observed in young to
middle-aged patients, and is an important cause of ischemic stroke.
It may occur spontaneously or have a traumatic etiology. The
reported incidence of symptomatic spontaneous dissection is
~3/100,000 per year (15). Systemic
vascular disorders or vasculitides, infections, smoking, diabetes
mellitus and hypertension have been reported as intrinsic
etiological factors (16). As
aforementioned, there is a male predominance regarding ICAD
incidence rates (17). Furthermore,
the clinical presentation of ICAD is variable: Patients may be
asymptomatic or present with various symptoms, including pain,
tinnitus, Horner's syndrome, contralateral limb weakness, and
retinal or cerebral ischemic symptoms (16). The diagnosis of ICAD is generally
made by CTA or magnetic resonance angiography, in combination with
confirmation by DSA (18). The
current study reported the case of 52-year-old male patient who
presented with the primary symptom of left limb weakness and no
typical clinical signs, such as pain, carotid territory ischemia or
Horner syndrome. However, the patient had a history of
hypertension. The ICAD was restricted to the oropharyngeal segment
of the right ICA, as demonstrated by CTA and DSA.
Current therapeutic strategies for ICAD include
medical anticlotting therapy, endovascular treatment or surgery;
however, the selection of an appropriate therapy remains
controversial (4). Anticoagulant
therapy in the acute stage is justified based on the presumed
embolic mechanism, and antiplatelet agents, including aspirin or
clopidogrel, have also been used for residual luminal irregularity
or in cases of ICAD without ischemic symptoms (2). Endovascular treatments, including
angioplasty or stenting, may be considered if the patient has
persistent high grade stenosis despite adequate anticoagulation and
a persisting or newly developed aneurysm of the dissected internal
carotid, or is contraindicated for anticoagulation therapy
(3). Willis covered stent is an
expandable balloon-covered stent specifically developed for
intracranial vessels (19). It has
been previously used for treatment of patients with intracranial
aneurysms, internal carotid artery aneurysms and pseudoaneurysms,
and has been suggested to be a safe, durable and efficacious option
(20,21). However, endoleakage is a frequent
problem following initial implantation (10), and in the case of a tortuous parent
artery or potential side branch coverage, using a Willis covered
stent is not recommended (22). In
the present case, medical therapy with aspirin, clopidogrel and
atorvastatin resulted in no obvious improvement of the recurrent
contralateral limb weakness, therefore, endovascular reconstruction
of the right ICAD was performed using a Willis covered stent;
expandable balloon-covered stent specifically developed for
intracranial vessels (14). The
stent was successfully deployed and anchored at the targeted vessel
segment and the performance of the patient was markedly improved
thereafter. Antiplatelet therapy was reported to be important
following the use of the device (23). Thus, the patient received an
antiplatelet protocol and no significant in-stent stenosis was
identified on the follow-up DSA. However, endoleakage following
placement of the covered stent is a risk that needs to be carefully
monitored.
In conclusion, present study revealed the
significant role of interventional procedures using the Willis
covered stent in the treatment of unilateral ICAD when medical
therapy has proven ineffectual.
References
|
1
|
Vicenzini E, Ricciardi MC, Sirimarco G, Di
Piero V and Lenzi GL: Bilateral spontaneous internal carotid artery
dissection with both early and very late recanalization: A case
report. J Clin Ultrasound. 39:48–53. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Soong B, Chan H and Ng F: A case of young
man with stroke caused by internal carotid artery dissection. Hong
Kong J Emerg Med. 19:492012.
|
|
3
|
Kim Y-K and Schulman S: Cervical artery
dissection: Pathology, epidemiology and management. Thromb Res.
123:810–821. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Patel RR, Adam R, Maldjian C, Lincoln CM,
Yuen A and Arneja A: Cervical carotid artery dissection: Current
review of diagnosis and treatment. Cardiol Rev. 20:145–152. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mohan IV: Current optimal assessment and
management of carotid and vertebral spontaneous and traumatic
dissection. Angiology. 65:274–283. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bayır A, Aydoğdu Kıreşi D, Söylemez A and
Demirci O: Cerebral infarction caused by traumatic carotid artery
dissection. Ulus Travma Acil Cerrahi Derg. 18:347–350. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nakiri GS, Al-Khawaldeh M, Parente B,
Kessler I, Gory B, Riva R and Mounayer C: Treatment of ruptured
intra-cranial internal carotid artery dissection using a
flow-diverter stent. J Neuroradiol. 39:271–275. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Feugier P, Vulliez A, Bina N, Floccard B
and Allaouchiche B: Urgent endovascular covered-stent treatment of
internal carotid artery injury caused by a gunshot. Eur J Vasc
Endovasc Surg. 34:663–665. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhu YQ, Li MH, Lin F, Song DL, Tan HQ, Gu
BX, Zhang HQ, Leng B and Zhang PL: Frequency and predictors of
endoleaks and long-term patency after covered stent placement for
the treatment of intracranial aneurysms: A prospective,
non-randomised multicentre experience. Eur Radiol. 23:287–297.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tan HQ, Li MH, Li YD, Fang C, Wang JB,
Wang W, Wang J, Zhang PL and Zhu YQ: Endovascular reconstruction
with the Willis covered stent for the treatment of large or giant
intracranial aneurysms. Cerebrovasc Dis. 31:154–162. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhu YQ, Gu BX, Li MH, Wang W, Cheng YS,
Tan HQ, Wang JB, Zhang PL and Ma LT: Safety, feasibility, and
mid-term follow-up of Willis stent graft placement in the treatment
of symptomatic complicated intra-or extra-cranial aneurysms: A
multicenter experience. Minim Invasive Ther Allied Technol.
19:320–328. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ping JJ, Di CS and Ying CL: Neurology
(7th). People's Medical Publishing House. Shelton, CT: 2013.
|
|
13
|
Bogousslavsky J and Pierre P: Ischemic
stroke in patients under age 45. Neurol Clin. 10:113–124.
1992.PubMed/NCBI
|
|
14
|
Touzé E, Gauvrit JY, Moulin T, Meder JF,
Bracard S and Mas JL: Multicenter Survey on Natural History of
Cervical Artery Dissection: Risk of stroke and recurrent dissection
after a cervical artery dissection: A multicenter study. Neurology.
61:1347–1351. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Debette S and Leys D: Cervical-artery
dissections: Predisposing factors, diagnosis, and outcome. Lancet
Neurol. 8:668–678. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Salvati B, Tesori MC, Lombardo F, Donello
C, Lange KJ and Capoano R: Surgical treatment of spontaneous common
carotid dissection: A case report. Ann Ital Chir. 85(ePub):
852014.PubMed/NCBI
|
|
17
|
Metso AJ, Metso TM, Debette S,
Dallongeville J, Lyrer PA, Pezzini A, Lichy C, Kloss M, Brandt T,
Touzé E, et al: CADISP Group: Gender and cervical artery
dissection. Eur J Neurol. 19:594–602. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hassan AE, Zacharatos H, Rodriguez GJ,
Suri MF, Tariq N, Vazquez G, Tummala RP and Qureshi AI: Long-term
clinical and angiographic outcomes in patients with spontaneous
cervico-cranial arterial dissections treated with stent placement.
J Neuroimaging. 22:384–393. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tan HQ, Li MH, Zhang PL, Li YD, Wang JB,
Zhu YQ and Wang W: Reconstructive endovascular treatment of
intracranial aneurysms with the Willis covered stent: Medium-term
clinical and angiographic follow-up. J Neurosurg. 114:1014–1020.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wang W, Li MH, Li YD, Gu BX, Wang J, Zhang
PL and Li M: Treatment of traumatic internal carotid artery
pseudoaneurysms with the Willis covered stent: A prospective study.
J Trauma. 70:816–822. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhu YQ, Li MH, Fang C, et al: Application
of the Willis covered stent in the treatment of aneurysm in the
cisternal segment of the internal carotid artery: a pilot
comparative study with midterm follow-up. J. Endovasc Ther.
17:55–65. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Li M-H, Gao B-L, Wang Y-L, Fang C and Li
Y-D: Management of pseudoaneurysms in the intracranial segment of
the internal carotid artery with covered stents specially designed
for use in the intracranial vasculature: Technical notes.
Neuroradiology. 48:841–846. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wang JB, Li MH, Fang C, Wang W, Cheng YS,
Zhang PL, Du ZY and Wang J: Endovascular treatment of giant
intracranial aneurysms with willis covered stents: Technical case
report. Neurosurgery. 62:E1176–E1177. 2008. View Article : Google Scholar : PubMed/NCBI
|