Introduction
Condyloma acuminata (CA) are symptomatic genital
lesions caused by human papilloma virus (HPV). Patients who have CA
during pregnancy are a particular risk group. During pregnancy,
vaginal secretions contacting the skin and mucous membranes are
more abundant (1), meaning that the
vulva will remain in a moist and immersed state, which would be
problematic for CA patients. Several factors associated with
pregnancy can promote the growth of HPV-induced lesions, for
example, pregnancy hormones and reduced immunoresponsiveness. Cases
of CA in pregnancy are normally characterized by fast-growing
warts, and a reduced tolerance and poor compliance to treatment
(2).
Only a small number of treatments have been tested
and recommended in pregnancy; at present, bi- and tri-chloroacetic
acid (BCA/TCA), cryotherapy, electrocautery and surgical excision,
including laser treatment, are the only recommended treatments. In
addition to high recurrence rates, significant side effects have
been observed for these methods, including local ulceration and
scar formation, which may reduce a patient's compliance with
treatment requirements (3).
Moreover, medicine could potentially cause fetal malformation and
laser treatment and surgical excision may cause uterine
contraction, or even abortion (1,4).
Cryotherapy is widely used for the treatment of CA.
During the cryotherapy procedure, liquid nitrogen freezes the
tissue and thereby causes necrosis; the treatment also stimulates
specific immune responses, such as an immunomodulatory action of T
lymphocytes against the remaining viable wart tissue (5,6). The
advantages of cryotherapy are that it is simple, inexpensive,
rarely causes scarring or depigmentation, and is safe for use in
pregnancy.
Proanthocyanidins (PCs), extracted from ginkgo
leaves, lotus and other plants, are plant polyphenols with strong
antioxidant effects. PCs have been reported to exert antibacterial,
antiallergic and antigenotoxic effects, and to inhibit platelet
aggregation and capillary permeability (7–11).
Studies have shown that PCs can be safely used to treat infants,
pregnant women and the elderly, and are safe for application to the
face, perineum and breasts (12,13). PCs
have been found to be effective against redness, swelling, exudate,
itching and other symptoms associated with inflammation (14).
In the present study, liquid nitrogen cryotherapy
combined with PC treatment was applied to pregnant women with CA,
and the safety and efficacy of the treatment was investigated.
Materials and methods
Study group
This retrospective study analyzed the records of 46
pregnant women who presented with CA (localized or extended) that
were treated with liquid nitrogen cryotherapy combined with PC. The
patients were recruited from the dermatology clinic of the Maternal
and Child Health (MCH) Hospital of Shaanxi Province (Xi'an, China)
from May 2010 to February 2013. The mean age of the treated
patients was 27 years (range, 23–34 years) and the patients were
diagnosed with CA at a mean of 18 weeks (range, 10–26 weeks)
gestation. CA was confirmed by the acetic acid white assay
(15). The patients were made aware
of the advantages of liquid nitrogen cryotherapy combined with PC
treatment, and strongly requested to use it following the
consideration of abortion, long-term fertility problems, and other
relevant risks.
The study was approved by the Ethics Committee of
the Maternal and Child Health (MCH) Hospital of Shaanxi Province.
All participants signed an informed consent to participate in the
research.
Lesion characteristics
The number of lesions treated for each case ranged
from 5 to 18, with an average of 12.2±5.5 lesions per patient. The
warts differed in size, but each exhibited a broad pedicle, with a
clear boundary and smooth, moist surface. In certain cases, fused
lesions were present. The majority of lesions were gray-brown in
color, while a few were dark red. There were 12 cases of lesions
with a diameter >4 cm. The study group included 14 patients who
were treatment naive, while the remainder had received repeated
freezing, laser therapy, electrocautery and/or other treatments,
including 5% Imiquimod cream, surgery and interferon, for 2–10
months. Scar formation was evident in 4 cases. Patients at risk of
abortion were excluded from the study.
Treatment of the lesions
The lesions were first swabbed with 0.02%
povidone-iodine solution. Then, liquid nitrogen was sprayed onto
the lesions using a HX17-YDQ-500 liquid nitrogen gun (Far Western
Science and Technology Co. Ltd., Beijing, China). The distance from
the nozzle to lesions was 2–3 cm and the spray time was >60 sec
and continued until the nozzle frosted (~2 min) and the nitrogen
spray was no longer able to focus on the lesions. Spraying was also
stopped if the patient felt pain. When the pain had lessened, the
lesions were sprayed again until the color of the wart changed from
flesh colored to purple. The Velvet Feeling (comprising PCs as the
active ingredient; Lanke Hengye Medical Technology Co. Ltd.,
Changchun, China) was sprayed onto non-woven fabric or single-layer
gauze was then applied to the affected area for 20 min, 2–3 times a
day and for a period of one week.
Before the patient left the clinic, the clinician
confirmed that the patient was able to see their lesions, and that
examination with a hand-held mirror was possible. The patients were
informed that they should examine the treated areas daily and
advised to look for any symptoms of infection, including increased
redness, swelling or discharge, with malodorous discharge or any
other sign of infection, including fever, to be reported to the
clinician immediately.
In the majority of cases, the necrotic tissue of the
wart began to drop off 3 days after the treatment and the wart had
completely dropped off by 1 week. In cases where the wart had not
dropped off, varying degrees of narrowing of the wart were
observed, and the clinician administered repeated treatments using
the aforementioned method. The treatment was stopped when no wart
was detectable.
Patient follow-up
Photographic images of the lesions were captured
prior to treatment and at each return visit. At 1 and 3 months
following the liquid nitrogen cryotherapy, the patients were
followed up for clinical evaluation. This included checking for
lesion recurrence, encrustation, scab detachment, scar formation,
changes in skin pigmentation and tolerance to pain. At each of
these visits, the patient's satisfaction with the treatment results
was surveyed. Each patient was asked to state whether they
considered the treatment to be ‘very satisfactory’, ‘fairly
satisfactory’ or ‘unsatisfactory’.
Results
In general, the lesions were healed 5 days after the
treatment. All patients reported no discomfort, with the exception
of mild-to-moderate pain. No visible warts remained following the
treatment. All patients were able to follow the treatment protocol,
and responded to the survey with 94% satisfaction at 1 month and
87% satisfaction at 3 months after the completion of treatment. The
patients who answered ‘very satisfactory’ and ‘fairly satisfactory’
were included in these calculations.
In some patients, various degrees of edema and
erythema accompanied by mild-to-moderate burning pain occurred
around the treatment area. However, the patients were able to
tolerate these symptoms and successfully completed the treatment.
Blisters in the treated area ruptured in 4 patients. The ruptured
tissues healed within 4 days after the PC treatment. These events
did not affect any subsequent treatments.
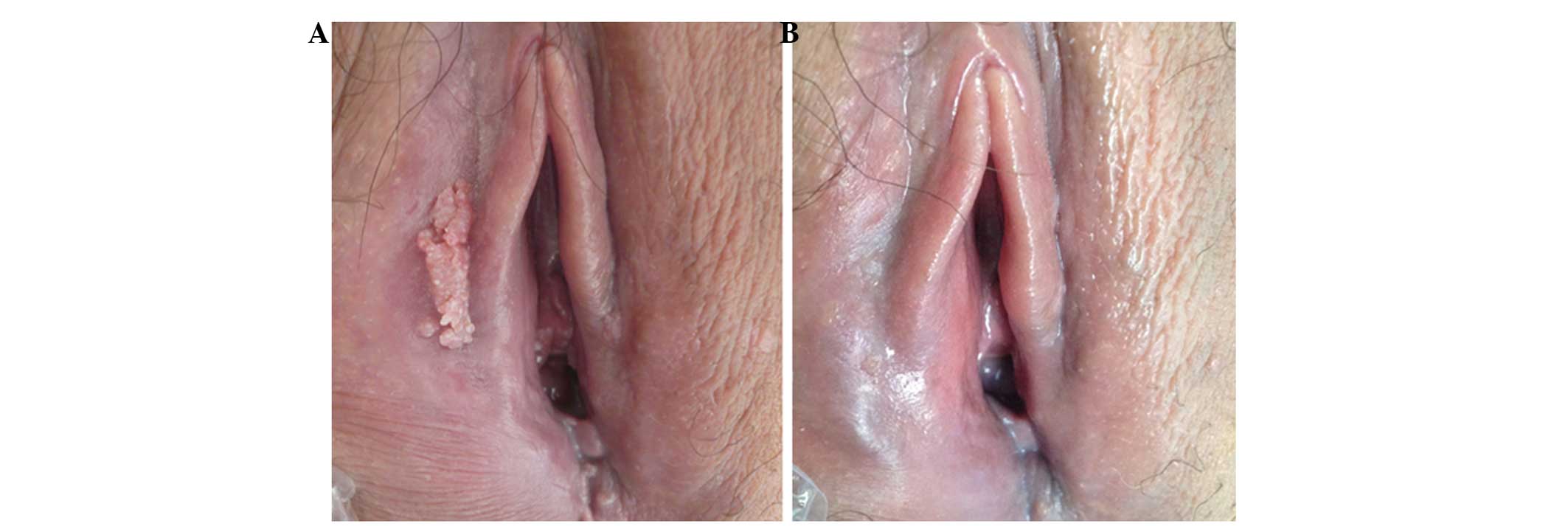
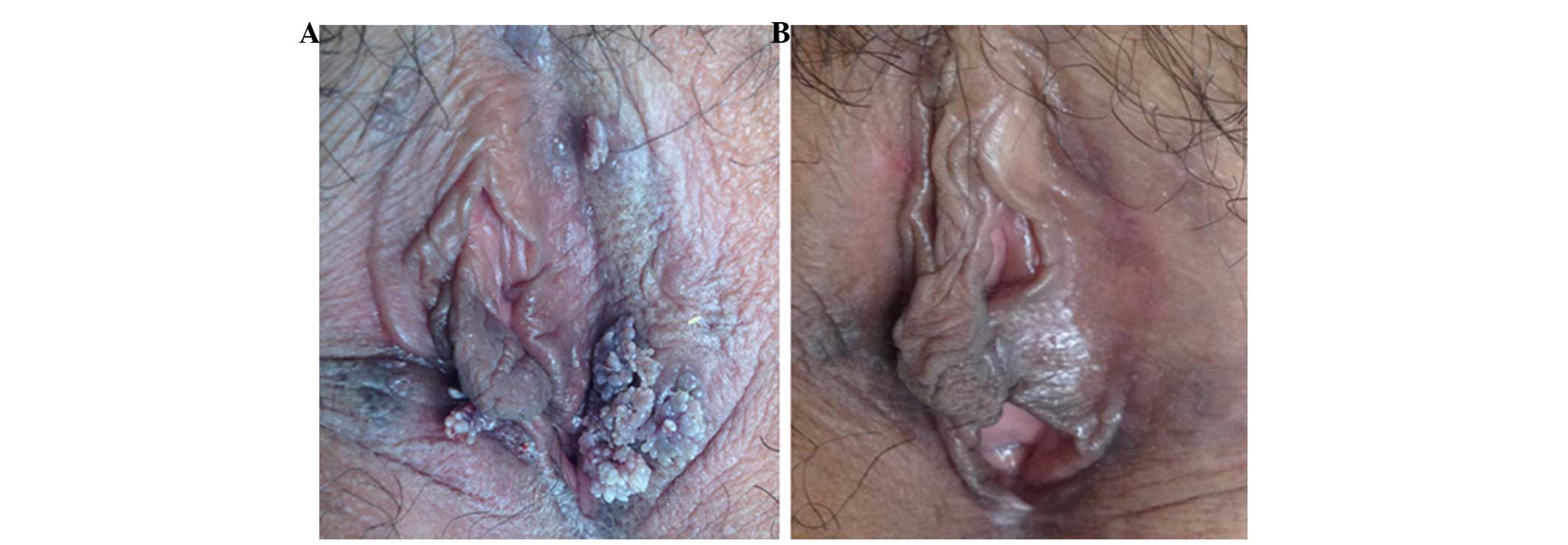
No depigmentation or scar formation was observed,
and no patients reported any severe adverse events. Each pregnancy
resulted in a healthy live birth without delivery complications.
The therapeutic efficacy is demonstrated for two specific patients
by photographic images in Figs. 1
and 2.
At the 1-month follow-up, only 1 case of recurrence
was identified, corresponding to a recurrence rate of 2.2%. At 3
months, 5 cases of recurrence were identified, and the recurrence
rate was 10.9%. These results are summarized in Table I.
 | Table I.Clinical characteristics of pregnant
women with CA. |
Table I.
Clinical characteristics of pregnant
women with CA.
| Clinical
characteristic | Number of patients
(%) |
|---|
| Delivery mode |
|
| Natural
childbirth | 19 (41.3) |
| Cesarean
section | 27 (58.7) |
| Birth weight, g |
|
|
<2,500 | 1 (2.2) |
|
2,500–4,000 | 41 (89.1) |
|
>4,000 | 4 (8.7) |
| Gestational age,
weeks |
|
|
<36 | 4 (8.7) |
|
37–41 | 39 (84.8) |
|
>42 | 3 (6.5) |
| Cases of
recurrence |
|
| 1
month | 1 (2.2) |
| 3
month | 5 (10.9) |
Discussion
In pregnancy, CA is characterized by the rapid
growth of warts and adverse responses to treatments have greater
severity compared with those in non-pregnant patients. This may be
because of reduced immunity during pregnancy, changes in hormone
levels (for example, elevated progesterone levels), and increased
vaginal discharge resulting in a more moist local environment
(16).
The few treatments that have been tested and
recommended for use in pregnancy are BCA/TCA, cryotherapy,
electrocautery and surgical excision, including laser treatment.
One of the treatment options for CA is imiquimod, an
immunomodulatory agent; however, treatment with 5% imiquimod cream
has been associated with mild to severe erythema, localized
erosion, itching and burning sensations; in addition, irritation,
induration, scabbing, tenderness and pain are less frequently
reported adverse effects (17). In
clinical trial subjects treated with 5% imiquimod cream,
recurrences were reported in 13–19% of cases (18). The safety of imiquimod treatment
during pregnancy has not been clarified.
Treatment options further include topical therapies,
for example, with salicylic acid, cantharidin, podophyllotoxin,
5-fluorouracil or bleomycin; other immunomodulatory treatments
(interferons); physical destruction (surgical excision,
cryotherapy, electrodessication or laser therapy) and homoeopathic
therapy (19–21). Cryotherapy causes tissue necrosis and
stimulates a specific immune responses (19,20). As
aforementioned, cryotherapy is a simple, inexpensive treatment that
rarely causes scarring or depigmentation, and is safe in
pregnancy.
In the present study, the spray freezing method was
used to treat the warts. The liquid nitrogen injection time and
dose were easily controlled, with a longer freezing time providing
more thorough removal of the wart. During treatment, liquid
nitrogen came into contact with normal skin and mucous membranes.
This did not cause severe damage; only minor swelling and very
superficial erosion were observed. The wart undergoes necrosis at
low temperatures. In addition, cryotherapy treatment is able to
induce an antigen-specific immune response and cytokine release
(16).
PCs extracted from ginkgo leaves, lotus, grape seed
and other plants, are plant polyphenols with strong antioxidant
effects. Studies have shown that PCs can inhibit nuclear factor-κB
DNA binding activity, and thereby block inflammatory cellular
pathways to achieve anti-inflammatory effects (22,23).
Structurally, PCs comprise at least one aromatic ring and at least
one hydroxyl group, which can readily combine with free radicals to
form resonance-stabilized phenoxyl radicals (24). As aforementioned, PCs have been
demonstrated to be safe for use in pregnant women, and to be
effective against redness, swelling, exudate, itching and other
symptoms of inflammation.
In the present study, all warts were removed
following the treatments. The recurrence rates were 2.2% at 1 month
after treatment and 10.9% at 3 months of follow-up. No ulcers or
scars were observed in any of the cases, which further confirmed
the safety of this combination therapy. In addition, an 87% patient
satisfaction rate was achieved at 3 months after treatment.
This study had certain limitations. Firstly, the
medical records were reviewed retrospectively, and patients were
not seen at final follow-up specifically for this study. Secondly,
the follow-up ranged from 1.2 to 3.4 years, and so the long-term
clinical outcome is not known in terms of recurrence rate, and
other possible problems.
In conclusion, liquid nitrogen cryotherapy combined
with PC appears to be an effective treatment for pregnant women
with CA. The results of this study showed that the recurrence rate
of CA was relatively low, and no effect was evident on the fetus.
Liquid nitrogen cryotherapy combined with PC may serve as a
treatment option for pregnant women with CA.
References
|
1
|
Cohen E, Levy A, Holcberg G, Wiznitzer A,
Mazor M and Sheiner E: Perinatal outcomes in condyloma acuminata
pregnancies. Arch Gynecol Obstet. 283:1269–1273. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wiley DJ, Douglas J, Beutner K, Cox T,
Fife K, Moscicki AB and Fukumoto L: External genital warts:
Diagnosis, treatment and prevention. Clin Infect Dis. 35(Suppl 2):
S210–S224. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lacey CJ and Fairley I: Medical therapy of
genital human papilloma virus-related disease. Int J STD AIDS.
6:399–407. 1995.PubMed/NCBI
|
|
4
|
Yang YG, Zou XB, Zhao H, Zhang YJ and Li
HJ: Photodynamic therapy of condyloma acuminata in pregnant women.
Chin Med J (Engl). 125:2925–2928. 2012.PubMed/NCBI
|
|
5
|
Gilson RJ, Ross J, Maw R, Rowen D, Sonnex
C and Lacey CJ: A multicentre, randomised, double-blind, placebo
controlled study of cryotherapy versus cryotherapy and
podophyllotoxin cream as treatment for external anogenital warts.
Sex Transm Infect. 85:514–519. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mi X, Chai W, Zheng H, Zuo YG and Li J: A
randomized clinical comparative study of cryotherapy plus
photodynamic therapy vs. cryotherapy in the treatment of multiple
condylomataacuminata. Photodermatol Photoimmunol Photomed.
27:176–180. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li S, Chen L, Yang T, Wu Q, Lv Z, Xie B
and Sun Z: Increasing antioxidant activity of procyanidin extracts
from the pericarp of Litchi chinensis processing waste by
two probiotic bacteria bioconversions. J Agric Food Chem.
61:2506–2512. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Llópiz N, Puiggròs F, Céspedes E, Arola L,
Ardévol A, Bladé C and Salvadó MJ: Antigenotoxic effect of grape
seed procyanidin extract in Fao cells submitted to oxidative
stress. J Agric Food Chem. 52:1083–1087. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Oyedemi SO and Afolayan AJ: Antibacterial
and antioxidant activities of hydroalcoholic stem bark extract of
Schotia latifolia Jacq. Asian Pac J Trop Med. 4:952–958.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dauer A, Hensel A, Lhoste E, Knasmuller S
and Mersch-Sundermann V: Genotoxic and antigenotoxic effects of
catechin and tannins from the bark of Hamamelis virginiana
L. in metabolically competent, human hepatoma cells (Hep G2)
using single cell gel electrophoresis. Phytochemistry. 63:199–207.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chang WC and Hsu FL: Inhibition of
platelet aggregation and arachidonate metabolism in platelets by
procyanidins. Prostaglandins Leukot Essent Fatty Acids. 38:181–188.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schmidt CA, Murillo R, Heinzmann B, Laufer
S, Wray V and Merfort I: Structural and conformational analysis of
proanthocyanidins from Parapiptadenia rigida and their
wound-healing properties. J Nat Prod. 74:1427–1436. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Khanna S, Venojarvi M, Roy S, Sharma N,
Trikha P, Bagchi D, Bagchi M and Sen CK: Dermal wound healing
properties of redox-active grape seed proanthocyanidins. Free Radic
Biol Med. 33:1089–1096. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jhun JY, Moon SJ, Yoon BY, Byun JK, Kim
EK, Yang EJ, Ju JH, Hong YS, Min JK, Park SH, Kim HY and Cho ML:
Grape seed proanthocyanidin extract-mediated regulation of STAT3
proteins contributes to Treg differentiation and attenuates
inflammation in a murine model of obesity-associated arthritis.
PLos One. 8:e788432013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wikstrom A, Hedblad MA, Johansson B,
Kalantari M, Syrjanen S, Lindberg M and von Krogh G: The acetic
acid test in evaluation of subclinical genital papillomavirus
infection: a comparative study on penoscopy, histopathology,
virology and scanning electron microscopy findings. Genitourin Med.
68:90–99. 1992.PubMed/NCBI
|
|
16
|
Le Poole C, Denman CJ and Arbiser JL:
Immunosuppression may be present within condyloma acuminata. J Am
Acad Dermatol. 59:967–974. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Edwards L, Ferenczy A, Eron L, Baker D,
Owens ML, Fox TL, Hougham AJ and Schmitt KA: Self-administered
topical 5% imiquimod cream for external anogenital warts. HPV Study
Group. Human PapillomaVirus. Arch Dermatol. 134:25–30. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Buck HW, Fortier M, Knudsen J and Paavonen
J: Imiquimod 5% cream in the treatment of anogenital warts in
female patients. Int J Gynaecol Obstet. 77:231–238. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lopaschuk CC: New approach to managing
genital warts. Can Fam Physician. 59:731–736. 2013.PubMed/NCBI
|
|
20
|
Stefanaki C, Katzouranis I, Lagogianni E,
Hadjivassiliou M, Nicolaidou E, Panagiotopoulos A, Anyfantakis V,
Bethimoutis G, Rallis E, Antoniou C and Katsambas A: Comparison of
cryotherapy to imiquimod 5% in the treatment of anogenital warts.
Int J STD AIDS. 19:441–444. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Simonart T and de Maertelaer V: Systemic
treatments for cutaneous warts: A systematic review. J Dermatolog
Treat. 23:72–77. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Subarnas A and Wagner H: Analgesic and
anti-inflammatory activity of the proanthocyanidin shellegueain A
from Polypodium feei METT. Phytomedicine. 7:401–405. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ahmad SF, Zoheir KM, Abdel-Hamied HE,
Ashour AE, Bakheet SA, Attia SM and Abd-Allah AR: Grape seed
proanthocyanidin extract has potent anti-arthritic effects on
collagen-induced arthritis by modifying the T cell balance. Int
Immunopharmacol. 17:79–87. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Puiggros F, Llópiz N, Ardévol A, Blade C,
Arola L and Salvadó MJ: Grape seed procyanidins prevent oxidative
injury by modulating the expression of antioxidant enzyme systems.
J Agric Food Chem. 53:6080–6086. 2005. View Article : Google Scholar : PubMed/NCBI
|