Introduction
There are an estimated 400 million people with
chronic hepatitis B (CHB) worldwide, and ~8 million patients
succumb annually to severe CHB, hepatocellular carcinoma and
end-stage liver cirrhosis (1).
End-stage liver cirrhosis is one of the main causes of mortality in
CHB patients (1,2). It is widely recognized that
psychological factors influence the development and prognosis of
cirrhosis in patients with CHB. The repeated outbreaks and
protracted course of hepatitis B and liver cirrhosis result in
different degrees of mood disorders in some patients. The incidence
rate of negative emotions in patients with chronic hepatitis has
been reported to be 38.1–51.1%, among which 47% of patients have
anxiety problems and 68% of patients have mild-to-moderate
depression (3,4). When depression occurs in combination
with liver disease, it can affect the patient's quality of life,
the disease diagnosis and case fatality rate (4). Patients with end-stage liver disease
have committed suicide because of depression (4). The accurate proportion of patients with
hepatitis B and cirrhosis suffering from depression is unclear;
therefore, the evaluation of depression in such patients is very
important. For this reason, the present study assessed the
emotional state of 114 patients with hepatitis B and cirrhosis
using the Hamilton Depression Scale (HAMD) and Hamilton Anxiety
Scale (HAMA) to explore the effects of the severity of liver
cirrhosis on the depressive emotional state.
Patients and methods
Patients
A prospective cohort that included 114 hospitalized
patients (95 men and 19 women; mean age, 42.5±11.6 years) with
hepatitis B-associated liver cirrhosis was recruited from the
Department of Infectious Diseases of the Third Affiliated Hospital
of Sun Yat-Sen University (Guangzhou, China) between July 25, 2011
and December 15, 2013. The patients were divided into three groups
by the Child-Pugh classification standard (5) to evaluate the severity of illness.
These were the Child-Pugh grade (CPG)-A group including 42 patients
(35 men and 7 women), CPG-B group including 38 patients (32 men and
6 women) and CPG-C group including 34 patients (28 men and 6
women). There was no significant difference in gender, age and
educational level among the groups, and thus the cases were
comparable (Table I). The inclusion
criterion was patients who met the diagnostic criteria for
hepatitis B and cirrhosis of the liver according to consensus
recommendations of the Asian Pacific Association for the Study of
the Liver in 2009 (6). The exclusion
criteria were as follows: Patients with evidence of mental illness,
serious diabetes, thyroid disorders or other endocrine system and
cardiovascular system diseases; having a history of drug use or
drug addiction and alcohol dependence; pregnancy or lactation;
appearing to be affected by the third stage of hepatic
encephalopathy; unwilling to cooperate following communication with
the medical staff; history of psychiatric drug use in the previous
2 weeks or a family history of mental illness; co-infection with
other viruses (hepatitis A, E or C, or HIV); other causes of liver
cirrhosis (Wilson's disease, other hereditary metabolic liver
disease or autoimmune liver disease); co-existing hepatocellular
carcinoma; portal vein thrombosis; renal impairment; or serious
diseases in other organ systems. As there is a lack of liver
donors, liver transplantation was not used regularly in this study.
Therefore, patients who underwent liver transplantation were also
excluded.
 | Table I.Baseline characteristics of included
patients at admission. |
Table I.
Baseline characteristics of included
patients at admission.
| Characteristic | Child-Pugh A
(n=42) | Child-Pugh B
(n=38) | Child-Pugh C
(n=34) |
|---|
| Age | 41.6±9.7 | 42.75±10.37 | 42.79±11.2 |
| Gender
(male/female) | 35/7 | 32/6 | 28/6 |
| Educational level, n
(%) |
|
|
|
| Primary
school | 13 (30.95) | 11 (28.95) | 11 (32.35) |
| Middle
school | 26 (61.91) | 25 (65.79) | 22 (64.71) |
|
College | 3 (7.14) | 2 (5.26) | 1 (2.94) |
| ALT | 39.4±8.5 | 42.4±9.2 | 38.6±7.8 |
| TBil (µmol/l) | 19.73±9.25 | 24.43±9.80 | 25.95±10.32 |
| SCR (µmol/l) | 69.53±35.36 | 66.49±45.27 | 67.35±39.38 |
The study was performed according to the World
Medical Association Declaration of Helsinki, and the protocol was
approved by the medical ethics committee of the Third Affiliated
Hospital of Sun Yat-Sen University. Written informed consent was
obtained from all individuals included in this study.
General management of patients
The 114 patients were given standard comprehensive
medical treatment (7) in accordance
with the Asia-Pacific consensus recommendations, including absolute
bed rest, intravenous antibiotics if required, a high calorie diet
(35–40 cal/kg/day), lactulose, bowel enemas, maintenance water,
electrolyte and acid-base equilibration, prevention and treatment
of complications, and intensive care monitoring. Patients also
received albumin, terlipressin, antiviral therapies (antiviral
treatment including lamivudine, adefovir dipivoxil, telbivudine and
entecavir were prescribed to the patients in whom hepatitis B virus
replication was activated). The start date of the antiviral
treatment was the date of diagnosis of hepatitis B cirrhosis among
58 patients, and 56 patients received antiviral therapy 2 years
prior to the diagnosis of hepatitis B cirrhosis. There were 9
patients with viral breakthrough who were treated with antiviral
drugs owing to unauthorized withdrawal prior to hospitalization,
and proton pump inhibitors were administered or plasma exchange was
performed if required. Orthotopic liver transplantation was not
adopted, mainly due to the cost and lack of available donors.
Evaluation of psychiatric
characteristics
The psychiatric characteristics of 114 cases of
hepatitis B with cirrhosis were assessed using the HAMA (8) and HAMD (9,10). The
HAMD is a multiple-choice questionnaire that clinicians use to rate
the severity of a patient's depression. A score of 0–7 is
considered to be normal, a score of ≥8 is considered to be a mood
disorder and a score of ≥20 indicates moderately severe depression.
The HAMA is a questionnaire used by clinicians to rate the severity
of a patient's anxiety. It contains 14 symptom-oriented questions.
Each of these symptoms is given a severity rating ranging from not
present (score 0) to very severe (score 4). Total scores of 0–17
are considered to indicate mild anxiety, those 18–25 mild to
moderate anxiety, and those 26–30 moderate to severe anxiety. Each
scale was jointly inspected and assessed by two staff who had
received formal training. They scored individually, and consistency
reached ≥90%. If third-stage hepatic encephalopathy occurred or the
patient succumbed in the process of treatment, the case was
removed.
Statistical analysis
Continuous values are expressed as the mean ±
standard deviation and categorical values are presented as count
and proportions. Between-group comparisons involving categorical
data were performed using the χ2 statistic corrected for
continuity; between-group comparisons involving continuous data
(age and socio-economic status) were calculated using one-way
analysis of variance and multiple comparisons. Data analysis was
performed using SPSS software, version 16.0 (SPSS, Inc., Chicago,
IL, USA). For all analyses, P<0.05 was considered to indicate a
statistically significant result.
Results
Baseline characteristics
In total, 114 patients with hepatitis B and liver
cirrhosis were studied. Baseline characteristics including gender,
educational level and basic information associated with liver and
kidney function were similar in every patient group (Table I). There were found to be no
significant differences in various baseline characteristics among
the three groups (P>0.05) as presented in detail in Table I.
HAMA and HAMD scores of patients with
hepatitis B and cirrhosis
Following psychological evaluation by HAMD and HAMA,
among the 114 cases of hepatitis B-associated cirrhosis of the
liver in outpatient and hospitalized patients, there were 76
patients without mood disorders, accounting for 66.7% and 38
patients with mood disorders, accounting for 33.3%. The results
showed that the HAMA and HAMD scores in the CPG-C group were
significantly higher than those in the CPG-A group (P<0.01), but
not significantly higher than those in the CPG-B group (P>0.05).
The proportion of patients with mood disorders in the CPG-C group
was significantly higher than that in the CPG-B group and CPG-A
groups (P<0.05 and P<0.01, respectively; Table II).
| Table II.HAMA and HAMD scores and the incidence
of mood disorders. |
Table II.
HAMA and HAMD scores and the incidence
of mood disorders.
| Rating scale | Child-Pugh A
(n=42) | Child-Pugh B
(n=38) | Child-Pugh C
(n=34) |
|---|
| HAMA |
|
|
|
|
Physical |
9.70±3.12a |
11.32±2.36b |
13.43±3.16c |
| Mood |
13.43±2.86a |
16.51±2.99b |
21.26±3.59c |
|
Anxiety |
10.22±3.23a |
13.12±4.33b |
15.12±5.13c |
|
Weight |
1.11±0.09a |
1.41±0.09b |
1.91±0.29c |
| Cognitive
problems |
3.21±0.74a |
3.41±0.83b |
3.82±0.95c |
| HAMD |
|
|
|
| Diurnal
variation |
0.33±0.028a |
0.35±0.03b |
0.38±0.034c |
|
Lethargy |
8.06±2.04a |
8.26±2.13b |
8.56±3.34c |
| Sleep
disorder |
4.85±1.10a |
5.06±1.31b |
6.06±1.31c |
| Incidence of mood
disorder, n (%) | 10
(23.81)a | 12
(31.58)d | 16
(47.06)c |
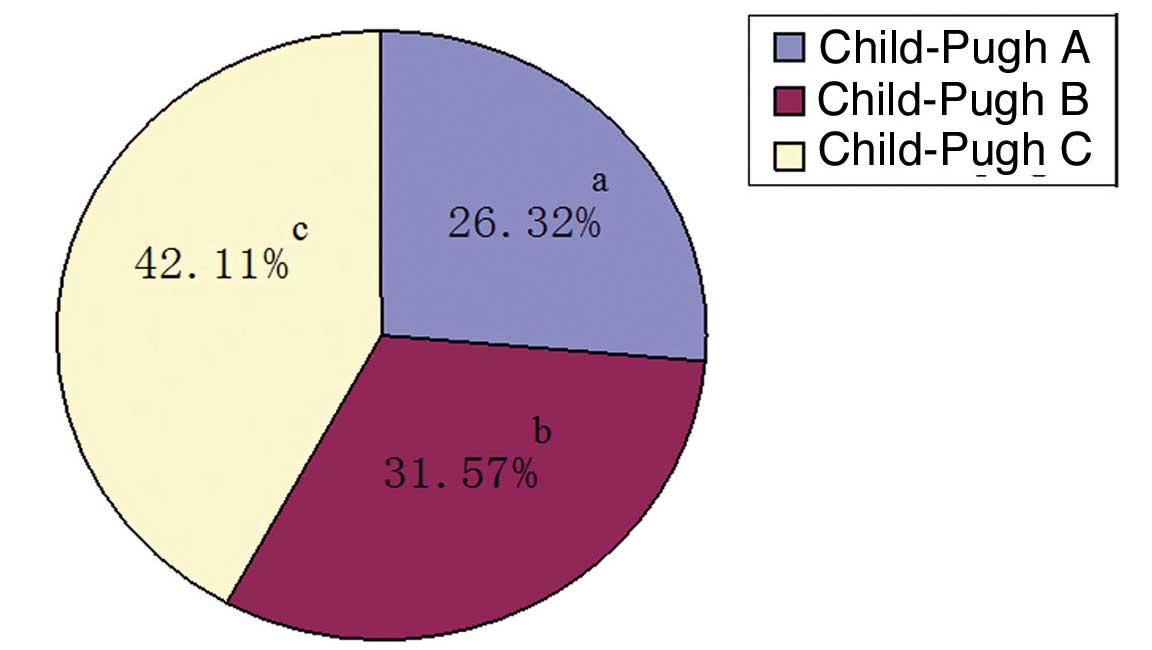
Incidence of mood disorders in
patients with hepatitis B and cirrhosis according to disease
severity
There were 76 cases without mood disorders,
including 32 cases in the CPG-A group, 26 cases in the CPG-B group
and 18 cases in the CPG-C group, accounting for 76.19, 68.42 and
52.94% of the respective CPG group. Among the 38 cases with mood
disorders, the CPG-A group had 10 cases, the CPG-B group had 12
cases and the CPG-C group had 16 cases, accounting for 26.32, 31.57
and 42.11% of the cases with mood disorders, respectively. The
prevalence of mood disorders in the CPG-C group of cirrhotic
hepatitis B patients was clearly higher than that in the CPG-A and
CPG-B groups (P=0.0336 for the latter). The proportion of patients
with mood disorders was higher in the CPG-B group than in the CPG-A
group, but the difference was not statistically significant
(P=0.4370). The rate of mood disorders in the CPG-A group was
significantly lower than that in the CPG-C group (P=0.0078). The
incidence of mood disorders in the three groups is presented in
Fig. 1.
Discussion
Hepatitis B is one of the most prevalent infectious
diseases in China (1). It is
strongly contagious with long duration, no special treatment and a
high cost of treatment (1,11). When CHB develops into liver
cirrhosis, it becomes an end-stage liver disease. Chronic liver
disease has the characteristics of long duration and poor prognosis
and it is harmful to patients' psychosomatic health. Furthermore,
when a patient with an end-stage liver disease has a mental health
problem, it is frequently misdiagnosed as a complication of hepatic
encephalopathy, which results in ineffective treatments being
administered and delays the diagnosis and treatment of the
emotional disorder (9). There are
some patients with end-stage liver disease who are suicidally
depressed (10). Therefore, the
psychological problems affecting patients with hepatitis
B-associated liver cirrhosis require greater clinical
attention.
The new biopsychosocial medical model encourages a
greater focus of attention on the effect of psychological factors
on physical disease. In particular, emotional disorders
accompanying chronic disease, especially depression, have an
apparent adverse influence on the treatment and prognosis of
chronic disease. However, doctors typically ignore the diagnosis
and treatment of depression when diagnosing physical diseases. This
may owe to certain doctors habitually focusing on the diagnosis of
physical disease and lacking knowledge of depression; in addition,
the symptoms of depression can be covert and overlap with the
symptoms of physical diseases (12).
Anxiety and depression are protective reactions
produced and experienced by humans. Studies have indicated that
psychological barriers clearly exist in patients with CHB,
particularly anxiety and depression. Anxiety and depression are
important factors that influence the clinical course of the disease
and rehabilitation, and the occurrence of negative emotions in CHB
cases is evident (3,13).
The current treatments for hepatitis B are unable to
eliminate the hepatitis virus from the body completely (14), which often causes patients to feel
depressed about the incurable nature of the disease. Patients often
worry excessively about their prognosis, which brings enormous
psychological pressure and anxiety; in addition to the economic
pressures of long-term treatment, patients are also concerned about
the progress and infectivity of the disease. Furthermore,
misunderstandings of the infectivity of hepatitis B and
discrimination in society also increase the psychological pressure
on patients with hepatitis B and liver cirrhosis, thus promoting
the development of mental disorders or depression (3,4,15). This is more apparent in patients with
end-stage liver disease, which results from its long disease course
and high case fatality rate, and the majority of patients feels
down to various degrees and may experience depression (16). Therefore, the evaluation and judgment
of depression in patients with end-stage liver disease is key to
improving patients' confidence in conquering the disease and may be
combined with other comprehensive therapies in order to improve the
curative effect.
According to the results of the present study, there
was no significant difference in the baseline data, such as gender,
age, educational level, and liver and kidney function, among the
groups, ruling out any interference due to inter-group differences.
There were 38 patients in the study that also had mood disorders,
which accounted for an incidence of mood disorders of approximately
one-third. This result indicates that in addition to physical
illness, a certain proportion of patients with hepatitis B and
cirrhosis also have mood disorders, and indirectly implies that
mood disorders develop in such patients not only because of hepatic
encephalopathy but also because of the disease itself. These
results are consistent with the findings of Song et al
(13). The HAMA and HAMD scale
scores of the patients with hepatitis B and cirrhosis in the
present study had a tendency to increase as the severity of the
hepatitis B-associated cirrhotic liver disease increased. It may be
hypothesized that this is due to the severity of the liver disease
increasing or the long course of the disease. However, there was
only a statistically significant difference in HAMA and HAMD scale
scores between the patients in the CPG-A and CPG-C groups, which is
consistent with the results of previous studies (17,18).
Mood disorders were identified in 23.81% of patients in the CPG-A
group, 31.58% of the CPG-B group and 47.06% of the CPG-C group. The
proportion of patients affected by mood disorders increased as the
severity of the disease worsened. Compared with the CPG-A group,
the incidence of mood disorder in the CPG-C group was increased
significantly. These results were consistent with the HAMA and HAMD
scale scores. It may be hypothesized that the incidence of
depression increases as the illness is exacerbated because the
treatments for hepatitis B-induced cirrhosis do not have a total
curative effect; this increases depression and causes patients to
lose hope (19). This is associated
with the disease being chronic and difficult to treat, and the
patients becoming anxious and confused regarding the long-term
treatment and recurring effects. Therefore, it is recommended that
for patients who experience such emotions, in addition to treating
the liver disease, psychological care should also be
strengthened.
In conclusion, in patients with hepatitis
B-associated liver cirrhosis, depression is closely associated with
the severity of the cirrhosis; patients with end-stage liver
disease in particular, have a higher incidence of depression. It is
recommended that importance should be attached to the assessment
and treatment of emotional disorders when positively protecting the
liver with comprehensive medical treatment. The results of this
study should help to improve the success rate of the treatment of
end-stage liver disease, for decompensated hepatitis B-associated
liver cirrhosis in particular, and improve the quality of life
patients with this disease.
Acknowledgements
The present study was supported by the Science and
Technology project (grant no. 2014A020212059) and the Natural
Science Fund (grant no. 2015A030313172) of Guangdong province, the
Guangzhou city Science and Technology project entitled ‘Receptor
interacting protein-3 (RIP3) in the early warning role of
aggravation of acute-on-chronic hepatitis B liver failure’, and the
Guangzhou city Science and Technology project (grant no.
1561000155). The authors thank all staff members of the Department
Of Infectious Diseases of the Third Hospital of Sun Yat-Sen
University.
References
|
1
|
Cornberg M, Jaroszewicz J, Manns MP and
Wedemeyer H: Treatment of chronic hepatitis B. Minerva
Gastroenterol Dietol. 56:451–465. 2010.PubMed/NCBI
|
|
2
|
Wiersma ST, McMahon B, Pawlotsky JM, Thio
CL, Thursz M, Lim SG, Ocama P, Esmat G, Mendy M, Bell D, et al:
Treatment of chronic hepatitis B virus infection in
resource-constrained settings: Expert panel consensus. Liver Int.
31:755–761. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shen CZ, Shao AX, Ni JP, Zheng XH and Wang
XY: Analysis on psychological status of patients with chronic
hepatitis B. Hulixue Zazhi. 19:11–13. 2004.(In Chinese).
|
|
4
|
Chen Q, Jin GX and He ZB: Analysis on the
depressive state of the patients with chronic hepatitis and nursing
care. Hulixue Zazhi. 16:466–468. 2001.(In Chinese).
|
|
5
|
Sarin SK, Kumar A, Almeida JA, Chawla YK,
Fan ST, Garg H, de Silva HJ, Hamid SS, Jalan R, Komolmit P, et al:
Acute-on-chronic liver failure: Consensus recommendations of the
Asian Pacific Association for the Study of the Liver (APASL).
Hepatol Int. 3:269–282. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Soga K, Tomikashi K, Miyawaki K, Fukumoto
K, Wakabayashi N, Konishi H, Mitsufuji S, Yoshida N, Kokura S,
Naito Y, et al: MELD score, Child-Pugh score and decreased albumin
as risk factors for gastric variceal bleeding.
Hepatogastroenterology. 56:1552–1556. 2009.PubMed/NCBI
|
|
7
|
Zheng YB, Xie SB, Xie DY, Peng L, Lei ZY,
Deng H, Lin BL, Lin CS, Zhao ZX, Ke WM and Gao ZL: A Novel
prognostic scoring system to predict 3-month mortality risk in
patients with acute-on-chronic liver failure in hepatitis B: A
retrospective cohort study. Hepatol Int. 6:727–734. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hamilton M: The assessment of anxiety
states by rating. Br J Med Psychol. 32:50–55. 1959. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hamilton M: A rating scale for depression.
J Neurol Neurosurg Psychiatry. 23:56–62. 1960. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mowla A, Kalantarhormozi MR and Khazraee
S: Clinical characteristics of patients with major depressive
disorder with and without hypothyroidism: A comparative study. J
Psychiatr Pract. 17:67–71. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pan C, Gu Y, Zhang W, Zheng Y, Peng L,
Deng H, Chen Y, Chen L, Chen S, Zhang M and Gao Z: Dynamic changes
of lipopolysaccharide levels in different phases of acute on
chronic hepatitis B liver failure. PLoS One. 7:e494602012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhang M: Diagnosis and treatment of
psychologic disorders in outpatients in general hospitals. Zhonghua
Yi Xue Za Zhi. 79:325–326. 1999.(In Chinese). PubMed/NCBI
|
|
13
|
Song JX, Liu XD, Qi JY and Tian DY: The
survey of psychiatric disorders among the patients with chronic
viral hepatitis and treatment measures. Tong Ji Yi Ke Da Xue Xue
Bao. 30:266–268. 2001.(In Chinese).
|
|
14
|
Fan ZP, Wang FS, Xu DP, Chu FL, Shi M,
Zhou Y and Zhang LX: Detection of HBcAg-specific cytotoxic
lymphocytes and their association with clinical status in patients
with hepatitis B. Zhonghua Yi Xue Za Zhi. 84:2073–2076. 2004.(In
Chinese). PubMed/NCBI
|
|
15
|
Tu B and Shao W: Chronic hepatitis B with
depression treatment efficacy ademetionine. Zhong Xi Yi Jie He Gan
Bing Za Zhi. 19:174–175. 2009.(In Chinese).
|
|
16
|
Novelli G, Rossi M, Ferretti G, Pugliese
F, Ruberto F, Lai Q, Novelli S, Piemonte V, Turchetti L, Morabito
V, et al: Predictive criteria for the outcome of patients with
acute liver failure treated with the albumin dialysis molecular
adsorbent recirculating system. Ther Apher Dial. 13:404–412. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lu MY and Zheng DR: The psychological care
of the patients with chronic hepatitis B. Zhongguo Yiyao Daobao.
8:192–193. 2011.(In Chinese).
|
|
18
|
Xu HY: Advances in the treatment of
depression in chronic liver medicine. Beijing Zhong Yi. 32:9–10.
2013.(In Chinese).
|
|
19
|
Li XQ, Cai X, Pei B, Chen CS and Xu Z:
Investigation on mental status of chronic hepatitis B patients. Di
4 Jun Yi Da Xue Xue Bao. 28:1802–1804. 2007.(In Chinese).
|