Introduction
Primary pulmonary lymphoma (PPL) is an extremely
rare neoplasm, accounting for 0.4% of all malignant lymphomas, and
3–4% of extranodal non-Hodgkin's lymphomas (1). The majority of cases are of B-cell
origin (2). In comparison with
primary pulmonary B-cell lymphomas, T-cell lymphomas are rarely
reported (3). Although there have
been a few previous reports published on primary pulmonary T-cell
lymphomas, clinical features, optimal treatment and prognostic
factors were not well defined. Furthermore, the clinical
manifestations are not specific. Patients with primary pulmonary
T-cell lymphomas may have the first symptoms such as fever, cough,
and dyspnea. The radiographic features are various and cannot be
used to differentiate between T- and B-cell malignancies of the
lung. Effective treatment for primary pulmonary T-cell lymphomas
has not yet been established, although a CHOP chemotherapy regimen
has been used.
Pneumonia is an inflammation of the distal airway,
alveoli, and interstitium of the lung that could be associated with
pathogenic microorganisms, physical or chemical agents, immunologic
injury, allergic illnesses and medicine. The majority of pneumonias
are infectious, and the typical pneumonia is characterized by a
sudden onset of fever, cough production of purulent or bloody
sputum, with or without pleuritic chest pain, shortness of breath
or distress. Radiographic observations can range from patchy
airspace infiltrates to lobar consolidation with air bronchograms.
Additional findings may include pleural effusions and cavitation.
This case was initially viewed as a reaction to an infectious
process. However, its rapid progress revealed no response to the
treatment administered, which directed to possible pathogens. PPL
may share similar symptoms and radiographic observations with
pneumonia, which may confuse us for establishing accurate diagnosis
and treatment. Finally, a correct judgement may depend on the
biopsy.
Case report
A 62-year-old man was admitted to The First
Affiliated Hospital of Soochow University (Suzhou, China) on July
24, 2014 (day 0) with an 11-day history of cough, dyspnea and
fever, which had been unresponsive to antibiotic therapy at a local
clinic. No underlying disease was noted. Informed consent was
obtained from the patient's family. A chest computed tomography
(CT) scan (Somatom Definition Flash, Siemens AG, Munich, Germany)
showed bilateral pulmonary nodules, ground-glass opacities and
subpleural consolidation, but no mediastinal adenopathies.
Furthermore, cerebral, abdominal and pelvic CT scans detected no
abnormalities. A bronchofiberscopy was not performed due to patient
intolerance. The results of a blood gas analysis [PaO2
52 mmHg, PaCO2 33 mmHg (pH 7.44); GEM Premier 4000,
Werfen, Cheshire, UK] were indicative of type I respiratory
failure. A physical examination revealed bilateral moist rales of
the lower lobes. Therefore, the patient was initially diagnosed
with severe pneumonia and type I respiratory failure. The routine
blood test results were as follows: White blood cells,
3.14×109/l (normal level, 3.5–9.5×109/l);
neutrophils, 2.18×109/l (normal level,
1.8–6.3×109/l); and serum lactate dehydrogenase (LDH),
434 IU/l (normal level,) 100–225 IU/l. In addition, influenza viral
antigen (Flu A kit, Guangzhou Wondfo Biotech Co. Ltd., Guangzhou,
China), anti-nuclear antibodies (ANAs; ANA detection kit, Scimedx
Corporation, Dover, NJ, USA), anti-neutrophil cytoplasmic antibody
(ANCA; MPO antibody IgG detection kit, HOB Biotech Group, Suzhou,
China), and the T-cell spot test (Multiskan, MK3, Varioskan Lux,
ThermoFisher Scientific, Inc., Waltham, MA, USA), plasma 1–3-β-D
glucan test (MB-80 microbial dynamic detection system, Jinshanchuan
Co., Ltd., Beijing, China) and plasma galactomannan test (Multiskan
FC) were negative. Furthermore, tumor marker, bone marrow smear and
chromosome analyses, as well as immune cell typing and multiplex
polymerase chain reaction, were unable to detect any
abnormalities.
The patient was treated with a wide-spectrum
antimicrobial combination for 10 days, including 3.0 g intravenous
(iv) drip of cefoperazone/sulbactam (Sulperazon, 3.0 iv. Q8h,
Pfizer Inc., New York, NY, USA) three times a day, 1.0 g iv drip of
vancomycin (Vancocin CP, 1.0 iv. Q12h, Eli Lilly and Company,
Basingstoke, UK) twice a day, 400 mg iv drip of voriconazole
(Vfend, 400 mg iv. Q12h, Pfizer) twice a day and 150 mg of oral
oseltamivir phosphate (Tamiflu, 150 mg po. Bid, Roche Pharma
(Schweiz) AG, Reinach, Switzerland) twice a day. The response was
disappointing, although treatment with a systemic corticosteroid
(Methylpredinisolone, Solu-medrol, 40 mg iv. qd, Pfizer) was shown
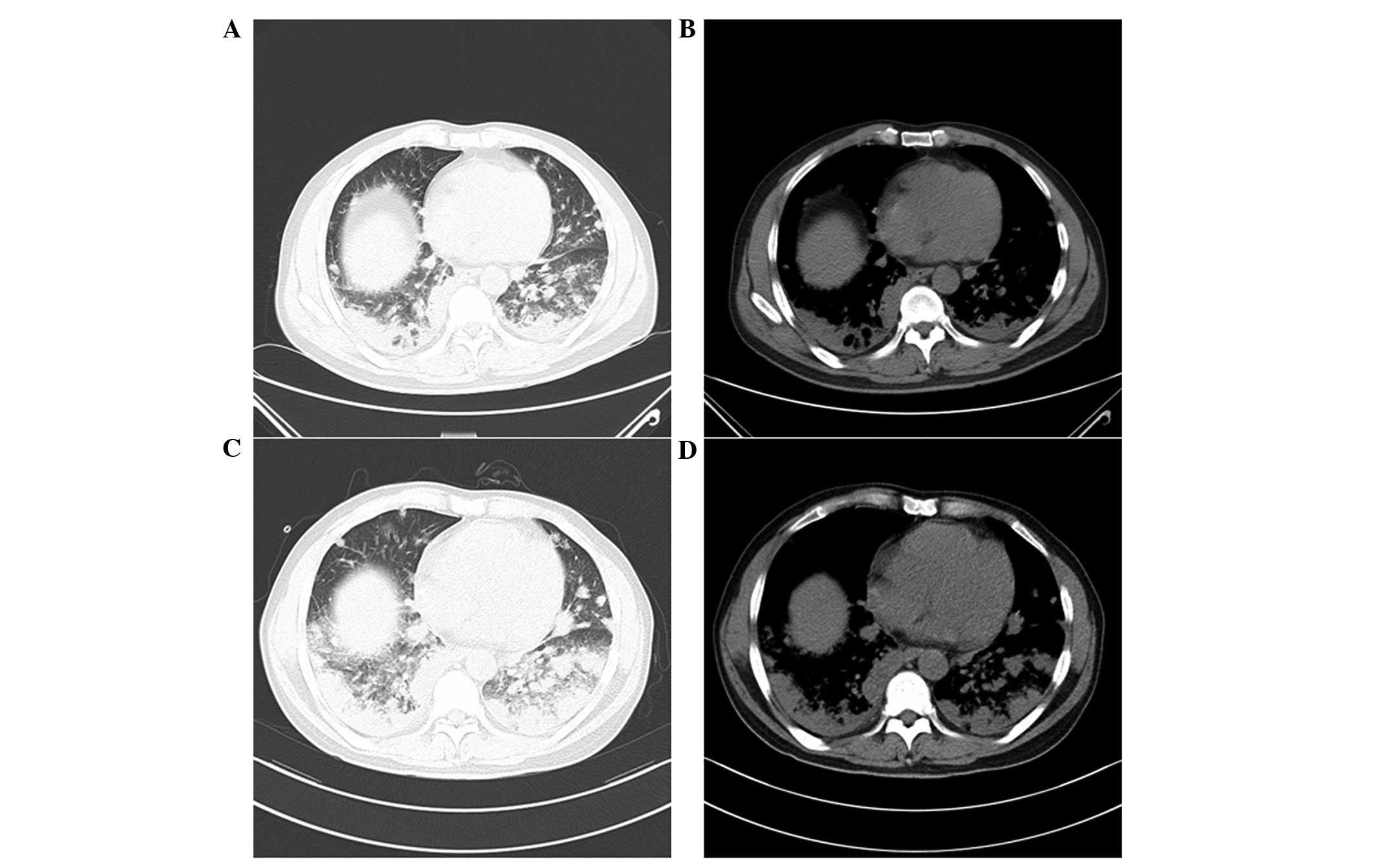
to alleviate hyperpyrexia transiently. During the course of
treatment, a chest CT scan was conducted twice on days 5 and 12,
and the images exhibited continuous progressive pulmonary lesions
(Fig. 1). The O2
saturation was 85–90%, despite the patient receiving 10 l/min
oxygen supplementation. On day 13 following admission, the patient
underwent a left lung biopsy via video-assisted thoracoscopic
surgery (VATS; IMAGE 1 SPIES, TC200EN, KARL STORZ GmbH & Co.
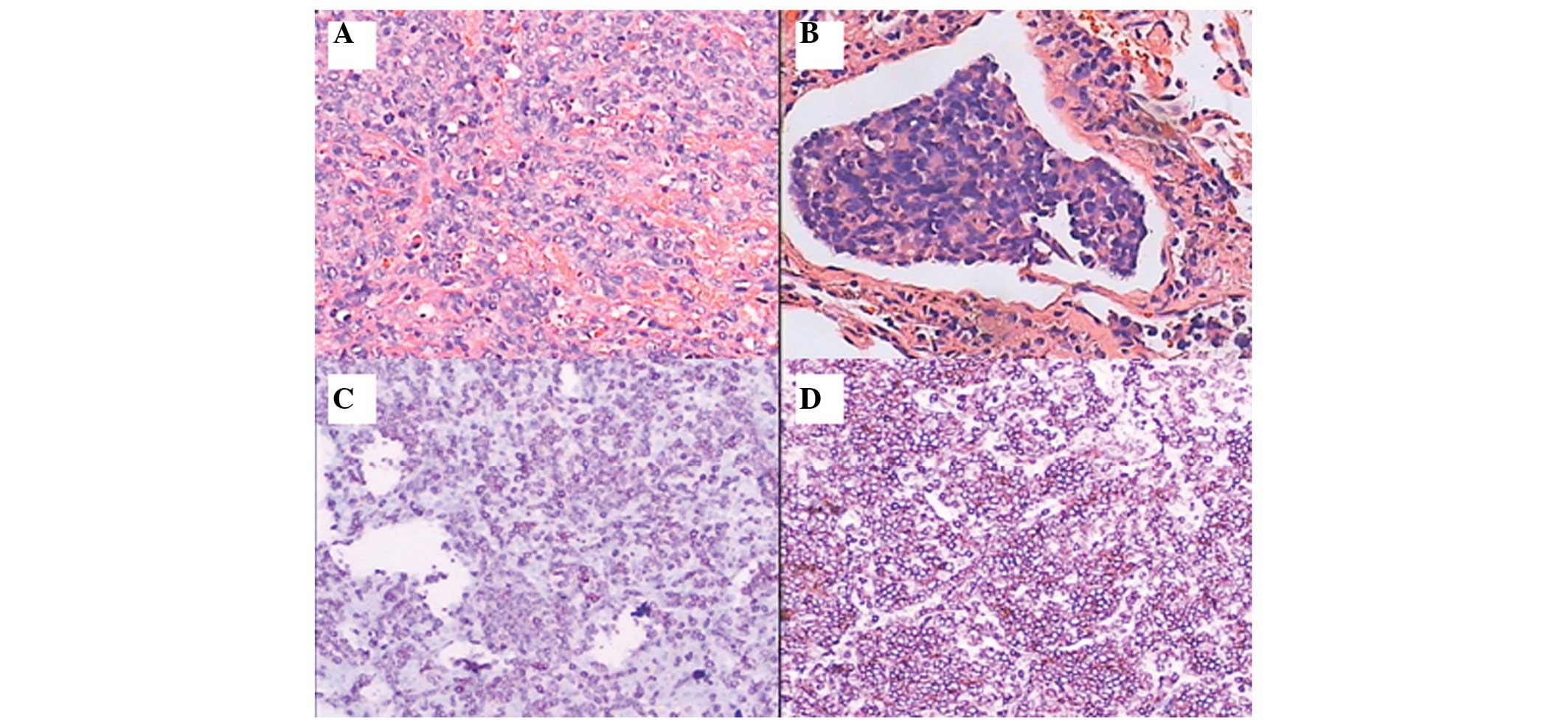
KG, Tuttlingen, Germany). The lymphoma cells expressed T cell
markers, including CD2, CD3 and CD43, whereas B cell markers were
negative. These pathological results led to a diagnosis of
malignant T-cell lymphoma, with tumor thrombus observed in the
blood vessels (Fig. 2A and B).
Immunohistochemical analyses were conducted in order to confirm the
diagnosis. Cluster of differentiation (CD)2 (16A30101; ZSGB-Bio,
Beijing, China), CD3 (1:50; 20025165; DAKO Agilent Pathology
Solutions, Ely, UK) and CD43 (20013550; DAKO Agilent Pathology
Solutions) immunostaining showed a positive and diffuse pattern
(Fig. 2C and D), and multiple
myeloma oncogene staining showed a positive and sporadic pattern.
In addition, Ki-67 (1:100; 2015120902; Genetech, Shanghai, China)
staining was positive (60%), whereas staining for B-cell lymphoma
(BCL)-2 (1:50; 20011864; DAKO Agilent Pathology Solutions), BCL-6
(1:100; 2015102101; Genetech), myeloperoxidase (15701C12;
ZSGB-Bio), CD10 (1:50; 20026145; DAKO), CD20 (1:200; 0009151;
DAKO), CD79a (1:50; 20010965; DAKO), CD5 (1:50; GM363329;
Genetech), cyclin D1 (1:50; 16610201; ZSGB-Bio), cytokeratin
(1:150; 10095919; DAKO) and CD30 (1:50; 20014851; DAKO) were
negative. Unfortunately, on day 18, the patient succumbed as a
result of progressive respiratory failure and a thoracic hemorrhage
that may have occurred as a result of the fragility of the lung
vessels and tissue caused by PPL.
Discussion
Due to the rarity of PPL, the patient in the present
study was initially diagnosed with pneumonia. Broad-spectrum
antimicrobial agents, which are effective against rare pathogens
including Mycobacterium tuberculosis, influenza virus and
fungi, were selected to treat the patient due to a lack of response
to antibiotics at a local hospital and the rapid progression of the
disease. However, treatment of the patient with a broad-spectrum
antimicrobial combination was ineffective. Furthermore, negative
results were obtained for ANA and ANCA assays, which eliminated the
possibility that the patient was affected by a connective tissue
disease. Therefore, a malignancy was suspected, although evidence
in support of this was only obtained upon VATS.
In the present study, the following criteria were
used to diagnose PPL (4):): 1) The
lung, bronchus or both are involved without evidence of mediastinal
adenopathy or a mass on the chest radiographs; 2) extrathoracic
lymphoma was not previously diagnosed and 3) there was no evidence
of extrathoracic lymphoma or lymphatic leukemia at the time that
primary lymphoma of the lung was diagnosed, Furthermore, for making
a diagnosis of PPL, the disease is not present outside of the
thorax for >3 months after the initial diagnosis. The patient
succumbed to the disease only 7 days following a definitive
diagnosis and, therefore, patient follow-up was impossible.
However, according to all other criteria, the patient could be
diagnosed with PPL. Using key words to search the PubMed database
(http://www.ncbi.nlm.nih.gov/pubmed),
including ‘T-cell lymphoma’, ‘primary’ and ‘pulmonary’, the present
study identified that only 15 cases of T-cell PPL have previously
been reported (5–19).
The radiological presentation of PPL is
non-specific, and thus, it is challenging to diagnose PPL by
imaging only. Patients with PPL may present with a single type of
imaging characteristic, whereas others may present with mixed
features. In the 15 cases reviewed, lung abnormalities consisted of
multiple nodules (8/15), masses (2/15), consolidations (2/15),
pleural effusion (1/15), patchy infiltration (1/15), ground-glass
opacities (1/15), reticular shadows (1/15) and emphysema (1/15)
(5–19). Furthermore, the predominant
radiographical findings were multiple nodules (53.3% of all
patients). In the present study, multiple nodules, ground-glass
opacities, patchy infiltration and subpleural consolidation were
detected by chest CT scanning, and these may have been caused by
invasion of the tumor embolus into the vascular lumen.
The majority of patients with PPL are required to
undergo surgical procedures, either open lung biopsy or VATS, in
order for a definitive diagnosis to be established. However, the
diagnostic yield via bronchoscopy is low (20). In the reviewed literature, only three
cases were diagnosed by a transbronchial biopsy (5,16,18); all
other diagnoses were confirmed by an open lung biopsy or VATS,
which permit the acquisition of adequate viable tissues for
morphological and immunohistochemical analyses. Immunohistochemical
techniques are considered the most accurate method for
differentiating between benign and malignant lymphoproliferative
disorders (21). In a recent review,
diagnoses were confirmed by immunohistochemical analyses, in
particular when the quantity of the specimen was insufficient
(22). The patient in the present
study was unable to tolerate a bronchoscopy due to severe
respiratory failure. Ultimately, owing to the deteriorating
condition of the patient, VATS was considered the most suitable
procedure for determining the final diagnosis.
T-cell lymphomas are associated with a poor outcome;
only 25% of patients survive >5 years following diagnosis
(22). The T-cell phenotype is now
considered to be an independent and significant poor prognostic
factor (23). The prognosis of
patients with non-Hodgkin lymphoma is typically assessed using the
International Prognostic Index (IPI). This is the following by the
following criteria: i) Age >60 years old; ii) elevated serum
level of lactate dehydrogenase; iii) poor performance status
(either ≥2 in the ECOG scale or ≤70 in the Karofsky scale;
(24); iv) stage III or IV disease
(Ann-Arbor Staging); and v) >1 site of extraodal involvement. It
has been proven to be a powerful predictor of the outcome for all
subtypes of non-Hodgkisn lymphoma (25). In the present case, the patient was
62 years old and levels of LDH were elevated. During
hospitalization, the patient was immobile due to severe dyspnea.
The patient was classified with Stage IV disease using the Ann
Arbor System (25) and due to the
diffused extranodal lesions in the lungs. Thus, the patient in the
present study had an IPI score of 4, which is considered high
risk.
A definitive diagnosis was not obtained until VATS
was performed. The aggressiveness of PPL, and its delayed
diagnosis, may result in a fatal outcome. In the present study, a
definitive diagnosis was obtained after 12 days via biopsy,
following the failure of broad-spectrum antibiotics and antifungal
agents. However, the patient lost the opportunity for further
treatment due to suffering from respiratory failure and a thoracic
hemorrhage.
In conclusion, according to the present case and the
reviewed literature, the diagnosis of primary pulmonary T-cell
lymphoma is challenging. The majority of cases have initially been
diagnosed as pneumonia and treated with various antibiotics.
Furthermore, the diagnosis of PPL is typically dependent on an
immunohistochemical analysis of specimens obtained via an open lung
biopsy or VATS (4). A common
therapeutic strategy for the effective treatment of PPL has not yet
been established, although the use of a cyclophosphamide,
doxorubicin, vincristine and prednisolone (CHOP) chemotherapy
regimen has been reported in the literature (26). The majority of the patients in the
reviewed literature presented with symptoms of fever (6/15), a
cough (5/15) and dyspnea (4/15), which may be mistaken for
pneumonia at the initial presentation. Therefore, lymphoma should
be considered in patients presenting with these symptoms when
combination therapy involving numerous antimicrobial agents has
failed.
References
|
1
|
Cadranel J, Wislez M and Antoine M:
Primary pulmonary lymphoma. Eur Respir J. 20:750–762. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nicholson AG, Wotherspoon AC, Diss TC,
Hansell DM, Du Bois R, Sheppard MN, Isaacson PG and Corrin B:
Reactive pulmonary lymphoid disorders. Histopathology. 26:405–412.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ferraro P, Trastek VF, Adlakha H,
Deschamps C, Allen MS and Pairolero PC: Primary non-Hodgkin's
lymphoma of the lung. Ann Thorac Surg. 69:993–997. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cordier JF, Chailleux E, Lauque D,
Reynaud-Gaubert M, Dietemann-Molard A, Dalphin JC, Blanc-Jouvan F
and Loire R: Primary pulmonary lymphomas: A clinical study of 70
cases in nonimmunocompromised patients. Chest. 103:201–208. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Maehara T, Kobayashi H, Kaneko K and
Naruse T: A case of T-cell lymphoma of the lung. Nihon Kyobu
Shikkan Gakkai Zasshi. 29:469–476. 1991.(In Japanese). PubMed/NCBI
|
|
6
|
Boon ES, Graal MB and van Noord JA:
Primary extranodal non Hodgkin's lymphoma of the lung presenting
with bilateral, patchy infiltrates dramatically improving after
corticosteroid therapy. Chest. 104:1292–1293. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Maejima S, Kitano K, Ichikawa S, Kaneko T,
Saito H, Kiyosawa K and Furuta S: T-cell non-Hodgkin's lymphoma of
the lung. Intern Med. 32:403–407. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fujihara T, Mori F, Kawano K, Yoshioka Y,
Tamura Y and Okita I: A case of T-cell type malignant lymphoma of
the lung. Nihon Kyobu Geka Gakkai Zasshi. 41:258–261. 1993.(In
Japanese). PubMed/NCBI
|
|
9
|
Hanada N, Abe T, Katagiri M, Yanase N,
Yamashita E, Shionoya S, Yoshimura H, Kasai K, Kameya T and Tomita
T: A case of T-cell lymphoma showing multiple nodular shadows and
an elevated titer of human T-lymphotropic virus type I
(HTLV-1)antibody. Nihon Kyobu Shikkan Gaakkai Zasshi. 31:231–234.
1993.(In Japanese).
|
|
10
|
Sasaki Y, Yamagishi F, Suzuki K, Miyazawa
H, Sugimoto N and Abe Y: Primary pulmonary malignant lymphoma of
the T-cell type. Nihon Kyobu Shikkan Gakkai Zasshi. 33:1454–1458.
1995.(In Japanese). PubMed/NCBI
|
|
11
|
Kohler CA, Gonzalez-Ayala E, Rowley P,
Malamud F and Verghese A: Primary pulmonary T-cell lymphoma
associated with AIDS: The syndrome of the indolent pulmonary mass
lesion. Am J Med. 99:324–326. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hanawa T, Chiba W, Fujimoto T, Wazawa H,
Yamashita N, Yasuda Y, Matsubara Y, Hatakenaka R, Funatsu T and
Ikeda S: T-cell lymphoma presenting as recurrent bilateral
pulmonary infiltrates over five years. Nihon Kyobu Shikkan Gakkai
Zasshi. 34:363–368. 1996.(In Japanese). PubMed/NCBI
|
|
13
|
Kawashima O, Sakata S, Kamiyoshihara M,
Maeshima A, Ishikawa S and Morishita Y: Primary pulmonary collision
tumor including squamous cell carcinoma and T-cell lymphoma. Lung
Cancer. 23:67–70. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
De Torres JP, Kenney L and Celli B:
Primary T-cell pulmonary lymphoma. A case report and review of the
literature. Arch Bronconeumol. 38:596–598. 2002.(In Spanish).
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Miyahara H, Itou H, Sekine A, Taniyama D,
Katsui T, Tanaka W, Satou R, Kurihara A, Satou Y and Sakamaki F: A
case of adult T-cell leukemia/lymphoma with primary lung cancer.
Nihon Kokyuki Gakkai Zasshi. 47:342–346. 2009.(In Japanese).
PubMed/NCBI
|
|
16
|
Bernabeu Mora R, Sánchez Nieto JM and
Nieto Olivares A: Bilateral pulmonary nodules as a manifestation of
primary pulmonary T-cell lymphoma. Int J Hematol. 90:153–156. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Shin CH, Paik SH, Park JS, Kim HK, Park
SI, Cha JG and Koh ES: Primary pulmonary T-cell lymphoma: A case
report. Korean J Radiol. 11:234–238. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Minomo S, Takimoto T, Morimura O, Watanabe
A, Nagate Y, Kotake T, Inoue T, Terada H, Nakata S and Abe K:
Primary pulmonary T-cell lymphoma in a human T-lymphotropic virus
type-1 carrier showing atypical shadow. J Thorac Oncol. 5:558–559.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Choe JY, Bisig B, de Leval L and Jeon YK:
Primary γδT cell lymphoma of the lung: Report of a case with
features suggensting derivation from intraepithelial γδ T
lymphocytes. Virchows Arch. 465:731–736. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kim JH, Lee SH, Park J, Kim HY, Lee SI,
Park JO, Kim K, Kim WS, Jung CW, Park YS, et al: Primary pulmonary
non-Hodgkin's lymphoma. Jpn J Clin Oncol. 34:510–514. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee KS, Kim Y and Primack SL: Imaging of
pulmonary lymphomas. AJR Am J Roentgenol. 168:339–345. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Laohaburanakit P and Hardin KA: NK/T cell
lymphoma of the lung: a case report and review of literature.
Thorax. 61:267–270. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Melnyk A, Rordriguez A, Pugh WC and
Cabannillas F: Evaluation of the Revised European-American Lymphoma
classification confirms the clinical relevance of immunophenotype
in 560 cases of aggressive non-Hodgkin's lymphoma. Blood.
89:4514–4520. 1997.PubMed/NCBI
|
|
24
|
Kelly CM and Shahrokni A: Moving beyond
Karnofsky and ECOG Performance Status Assessments with New
Technologies. J Oncol. 6186543doi: 10.1155/2016/6186543. Epub. 2016
Mar 15;PubMed/NCBI
|
|
25
|
Lee HJ, Im J-G and Goo JM: Peripheral
T-cell lymphoma: spectrum of imaging findings with clinical and
pathologic features. Radiographics. 23:7–26. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fisher RI, Gaynor ER, Dahlberg S, Oken MM,
Grogan TM, Mize EM, Glick JH, Coltman CA Jr and Miller TP:
Comparison of a standard regimen (CHOP) with three intensive
chemotherapy regimens for advanced non-Hodgkin's lymphoma. N Engl J
Med. 328:1002–1006. 1993. View Article : Google Scholar : PubMed/NCBI
|