Introduction
The meniscus is a wedge-shaped fibrocartilaginous
structure that is involved in shock-absorption, load distribution
and knee joint stability. Due to its largely avascular nature, the
meniscus presents poor healing (1).
The loss of meniscal function caused by meniscal tears, partial and
total meniscectomy, and meniscal degeneration lead to the
development or progression of knee osteoarthritis (OA) (2,3).
Previous studies have confirmed the direct association of partial
or total meniscectomy with the development of OA. Therefore, it is
necessary to repair the damaged meniscus with restoration of its
structure and function.
For meniscal defects occurring subsequent to
meniscectomy or meniscal degeneration, meniscal graft or artificial
meniscus transplantation have been previously performed; however,
these methods remain controversial due to the invasiveness,
durability and safety of the transplant (4). In addition, the selection of the
appropriate allograft size is challenging (5,6).
Therefore, a novel strategy is required for meniscus
regeneration.
Mesenchymal stem cells (MSCs), which have high
potential for proliferation and chondrogenesis, and display a
multipotential differentiation capacity that allows development
along the chondrogenic lineage, are a potentially attractive cell
source for meniscus regeneration. Several studies have been
performed using the intra-articular injection of MSCs and have
shown promising results (7–9). Previous studies have reported that
intra-articular injection of 5 million synovial MSCs promoted
meniscal regeneration in rat models (10), whereas the injection of fewer cells
did not result in meniscal regeneration (11). Furthermore, there is frequently a
significant loss of cells when using single cell suspension
injection, with only a small percentage of cells remaining at the
target site. The use of MSC sheets may be a solution to these
issues, since cell sheets not only provide a large number of MSCs,
but can also be attached to host tissues and even wound sites,
covering the surface with minimal cell loss via their deposited
extracellular matrix (ECM).
The aim of the present study was to investigate the
effect of MSC sheet transplantation for meniscus regeneration and
OA prevention in a rat massive meniscectomized model.
Materials and methods
Isolation and culture of rat bone
marrow-derived MSCs
All animal experiments were performed according to
‘Guide for the Care and Use of Laboratory Animals’ (National
Institute of Health publication, 8th Edition 2011), as well as the
standard guidelines approved by the Ethics Committee of Zhejiang
University (Hangzhou, China).
Adult male Sprague-Dawley Rats (n=10) were obtained
from the Experimental Animal Centre of Zhejiang University,
(Hangzhou, China). The rats were bred and maintained under a
12-h-dark:light cycle with free access to food and a water. Room
temperature was set at 25±3°C and relative humidity at 60±15%. Rats
(n=2) were used as donors for transplantation of MSCs sheet, and 10
rats were used as recipients. Rats were euthanized with
CO2 inhalation, and then the femurs and tibias were
removed. The bones were washed in minimal essential medium α
(MEM-α) supplemented with 10% (v/v) penicillin and streptomycin
(Gibco; Thermo Fisher Scientific, Inc., Waltham, MA, USA). The ends
of the femurs and tibias were cut away from the epiphysis, and the
bone marrow was flushed out of the bone using 10 ml medium in a
syringe. Next, the cells were filtered through a 70 µm cell
strainer and centrifuged at 300 × g for 5 min. The cell pellet was
resuspended in 10 ml MEM-α supplemented with 10% fetal bovine serum
(Thermo Fisher Scientific, Inc.) and plated in a culture plate.
Cells were maintained at 37°C in a humidified atmosphere with 5%
CO2, and the medium was changed every 2 days. When
adherent cells reached 80–90% confluence, they were detached with
0.25% trypsin-EDTA (Thermo Fisher Scientific, Inc.) and replated at
a ratio of 1:3 in regular growth medium to allow for continued
passaging. In order to ensure the consistency of experiments in
vitro and in vivo, MSCs derived from rats bone marrow at
passage 3 were used in all further experiments A maximum of 6
doublings of the cells were performed during the expansion and
culturing procedures.
Cell sheet preparation
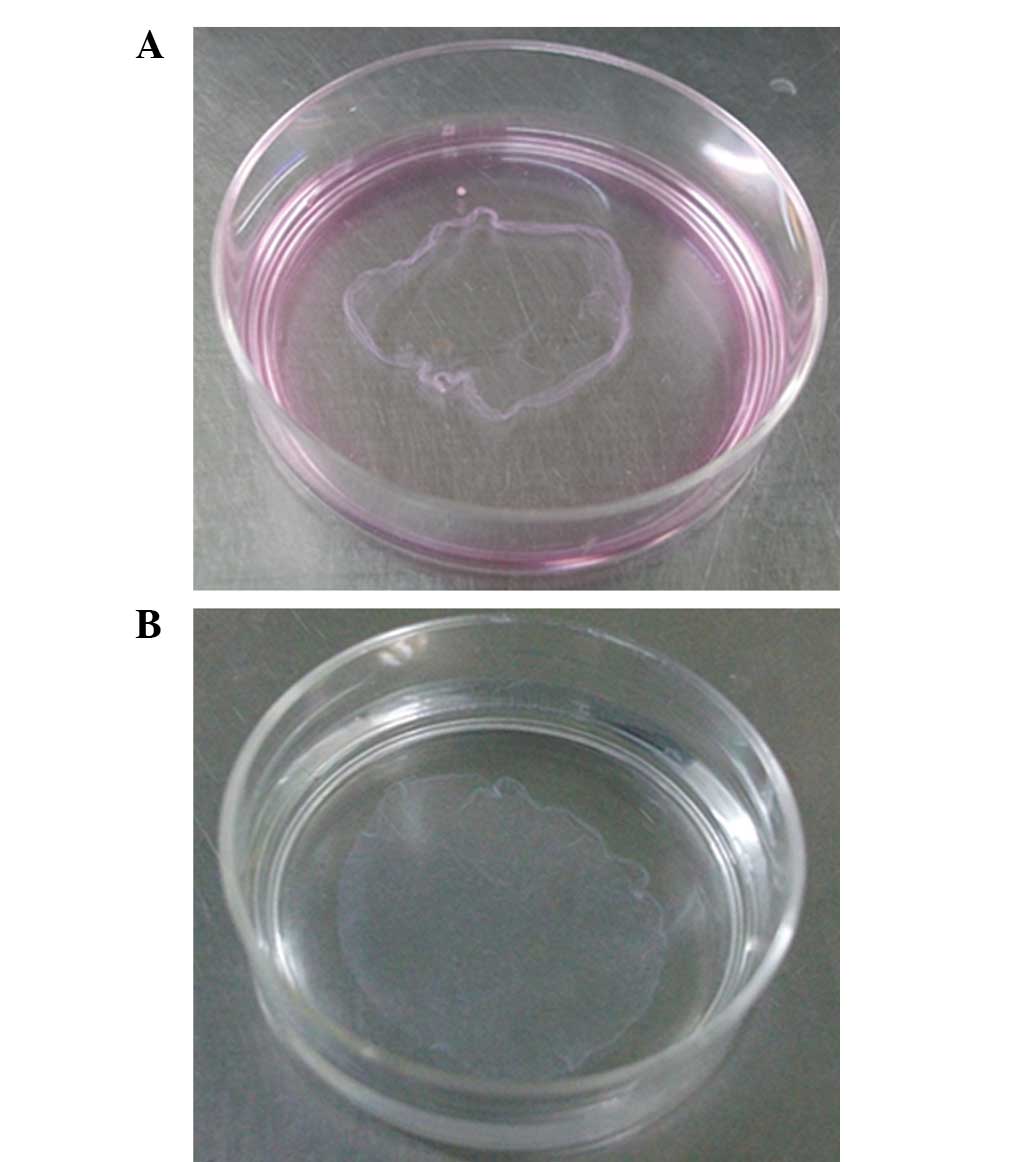
To create the cell sheet, the released cells were
seeded at 4×104 cells/cm2 into flasks
cultured in 10 ml of MEM-α supplemented with 10% FBS (Gibco, Thermo
Fisher Scientific Inc.) for a minimum of 1 week. Cells were
maintained at 37°C in a humidified atmosphere with 5%
CO2, and the medium was replaced daily. After 1 week,
the layered BMSCs were formed. The cells were then rinsed with
phosphate-buffered saline (Gibco) twice, and then lifted as a cell
sheet using a scraper (Fig. 1)
(12). Cell proliferation was
determined by DNA content assay using a fluorescent dye Hochest
33258 (Sangon Biotech Co., Ltd., Shanghai, China). The MSC sheets
were harvested and stored at −20°C until the assay was performed.
For the DNA content assay, the cells were thawed at room
temperature and homogenized in 1 ml of lysis buffer (50 mM
Tris-HCl, pH 7.6, 0.1% v/v Triton X-100; Sangon Biotech Co., Ltd.).
The lysate was sonicated on ice for 30 sec. After centrifugation,
the supernatant was collected for measurement. Cells
(~4.8×106) were contained within a single cell sheet, as
determined by DNA quantification using an PerkinElmer LS 55
Fluorescence(PerkinElmer, Inc., Waltham, MA, USA) and the
fluorescent dye, Hoechst 33258 (13).
Meniscectomy and MSC sheet
transplantation
A total of 10 male Sprague Dawley rats (age, 12–14
weeks) were used, which were divided into the MSC sheet
transplantation and untreated control groups. The knees of rats
were randomly used for transplantation of MSC sheet or untreated.
Rats were sacrificed at weeks 4 (n=5 knees) and 8 (n=5 knees) after
surgery in the two groups. The rats were anaesthetized by injection
of ketamine hydrochloride (2 mg/kg of body weight; China National
Medicines Corporation Ltd, Beijing, China) into the peritoneal
cavity. Under anesthesia, a straight incision was performed on the
anterior side of the bilateral knee, the anteromedial side of the
joint capsule was cut, and the anterior horn of the medial meniscus
was dislocated anteriorly with a forceps. The meniscus was then cut
vertically at the level of medial collateral ligament, and the
anterior half of medial meniscus was excised. Next, the dislocated
meniscus was removed. The MSC sheet was transplanted into the knee
joint of rats in the MSC sheet group, while no cells were
transplanted in the untreated control group. Subsequently, after
transplantation, fascia and skin were closed separately over the
wound, and the rats were allowed to walk freely. At 4 and 8 weeks
post-surgery, the rats were sacrificed by intraperitoneal injection
of 3% chloral hydrate (5 ml/kg body weight, Sangon Biotech Co.,
Ltd.).
Histological examination
Immediately after the rats were sacrificed, the
femoral condyle, medial meniscus and tibial plateau from the two
groups were collected and fixed in 4% paraformaldehyde for 3 days.
The images of the tissues were obtained after 4 and 8 weeks. Next,
tissues were decalcified in 20% EDTA solution for 14 days and then
embedded in paraffin wax. The specimens were sectioned in a
sagittal plane at 5 µm, and stained with safranin-o and fast green
(both Sangon Biotech Co., Ltd.). Stained histological sections were
observed using a BX53 microscope (Olympus Corp., Tokyo, Japan). The
modified Pauli's histological scoring system was used to evaluate
the regenerated meniscus, with the maximum score being 18 and lower
scores indicating values closer to the normal meniscus (14). The degree and quality of cartilage
were assessed and scored by an observer blinded to the study groups
using a cartilage repair grading system, adapted from the study by
O'Driscoll et al (15).
Statistical analysis
The obtained Pauli's scores were analyzed by
Student's t-test and the statistically significant differences were
determined at P<0.05. Data analyses were performed using the
SPSS software (version 15.0; SPSS, Inc., Chicago, IL, USA). Data
are presented as mean ± standard deviation.
Results
Clinical observations
No evidence of infection was observed in any of the
animals prior to and following the experiments. All animals
maintained their weight subsequent to surgery, and there was no
evidence of local inflammation or immobilization of the joint.
Meniscal regeneration by
transplantation of MSC sheet
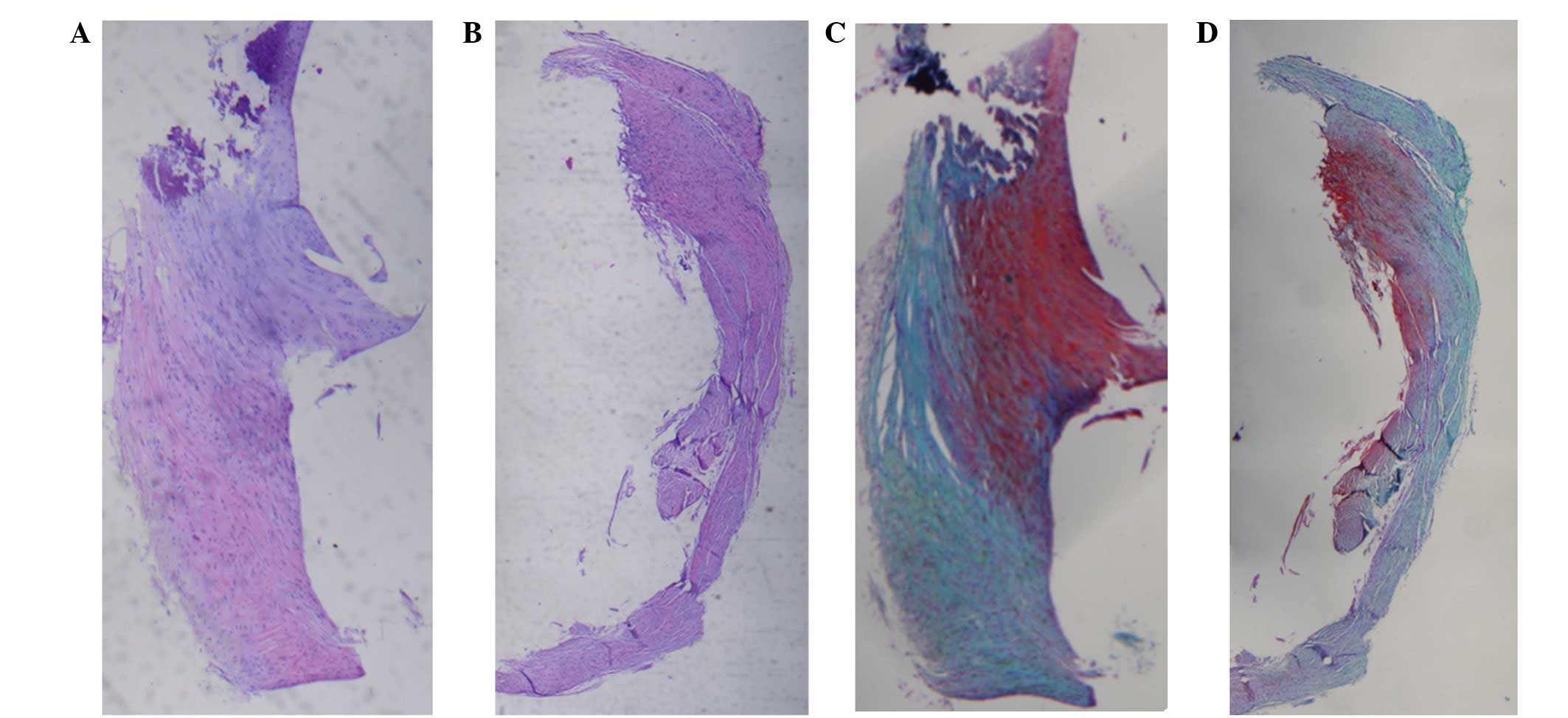
At 4 weeks after surgery, the shape of the meniscus
in the untreated group was not altered and even presented some
atrophy at the border. In the MSC sheet group, the new
hypercellular fibrocartilaginous tissue regenerated at the outside
of the host meniscus, stained with rich glycosaminoglycan (GAG)
content in the matrix (Fig. 2).
Positive area of S-O staining is indicative of GAG content
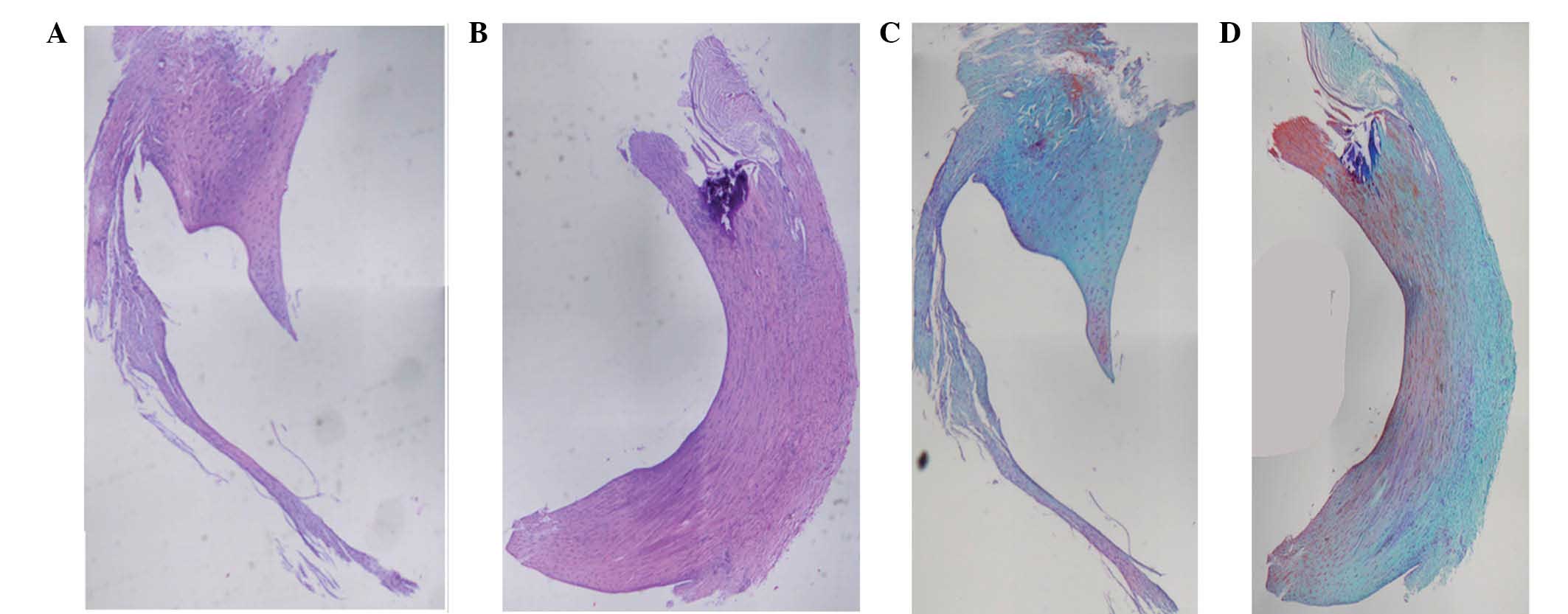
At 8 weeks after surgery, the meniscus appeared to
be degenerated and atrophied in the control group. The meniscus
size was smaller and filled with fibroblastic cells and a reduced
amount of ECM. In addition, a thin meniscus-like tissue regenerated
at outside of host meniscus. By contrast, in the MSC sheet group,
the anterior portion of meniscus was regenerated, similar to the
native meniscus and showed typical fibrochondrocytes surrounded by
a richer ECM. Furthermore, predominant collagen-rich matrix
bridging the interface was observed, and the neo-meniscus
integrated well with its host meniscus (Fig. 3).
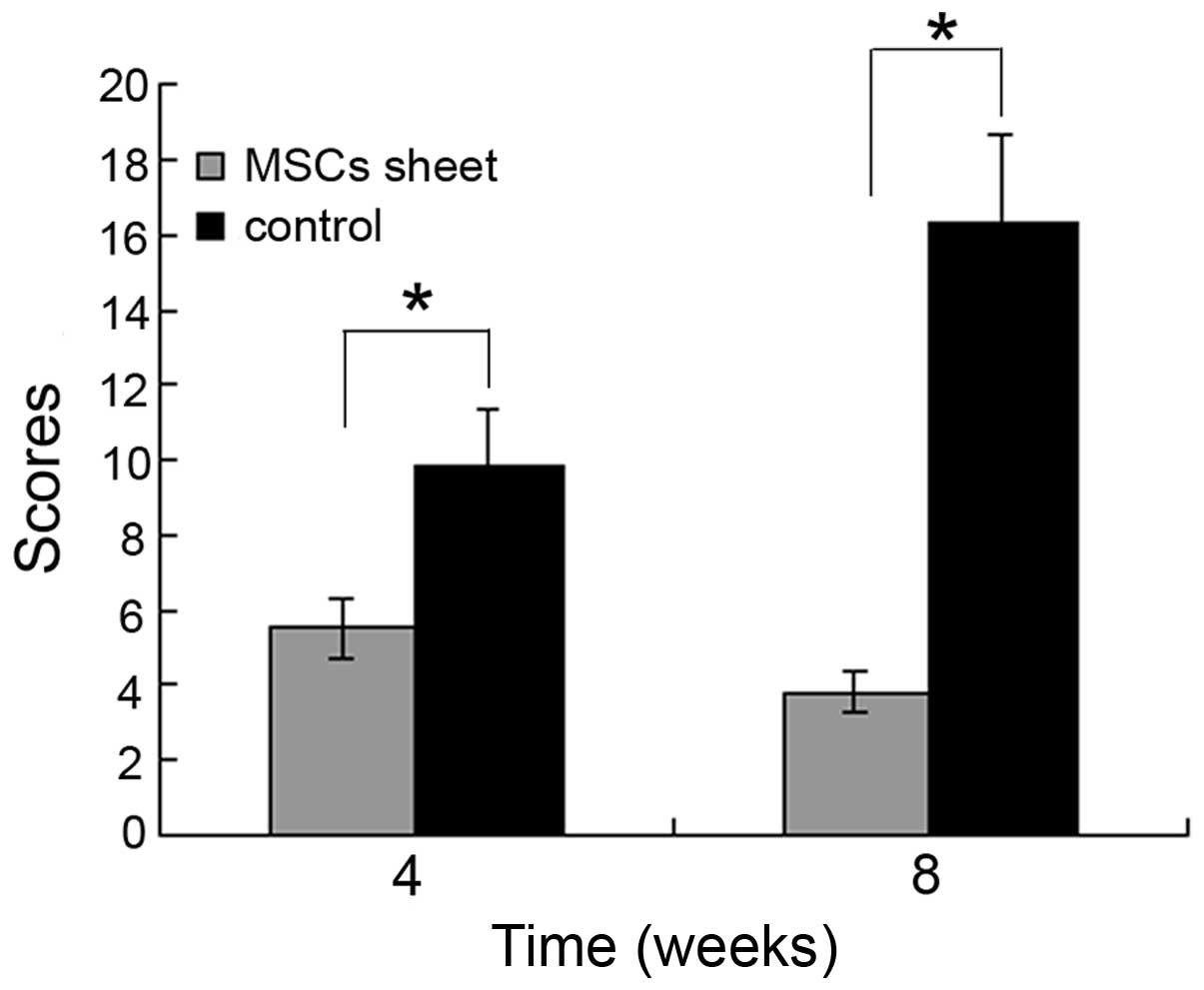
Histological scores
The histological scores for the regenerated meniscus
in the MSC sheet group were found to be 5.5±0.8 and 3.8±0.6 at 4
and 8 weeks after surgery, respectively. These scores were
significantly lower compared with those in the untreated control
group, which were found to be 9.8±1.5 and 16.3±2.4 at 4 and 8 weeks
after surgery, respectively (P<0.05; Fig. 4).
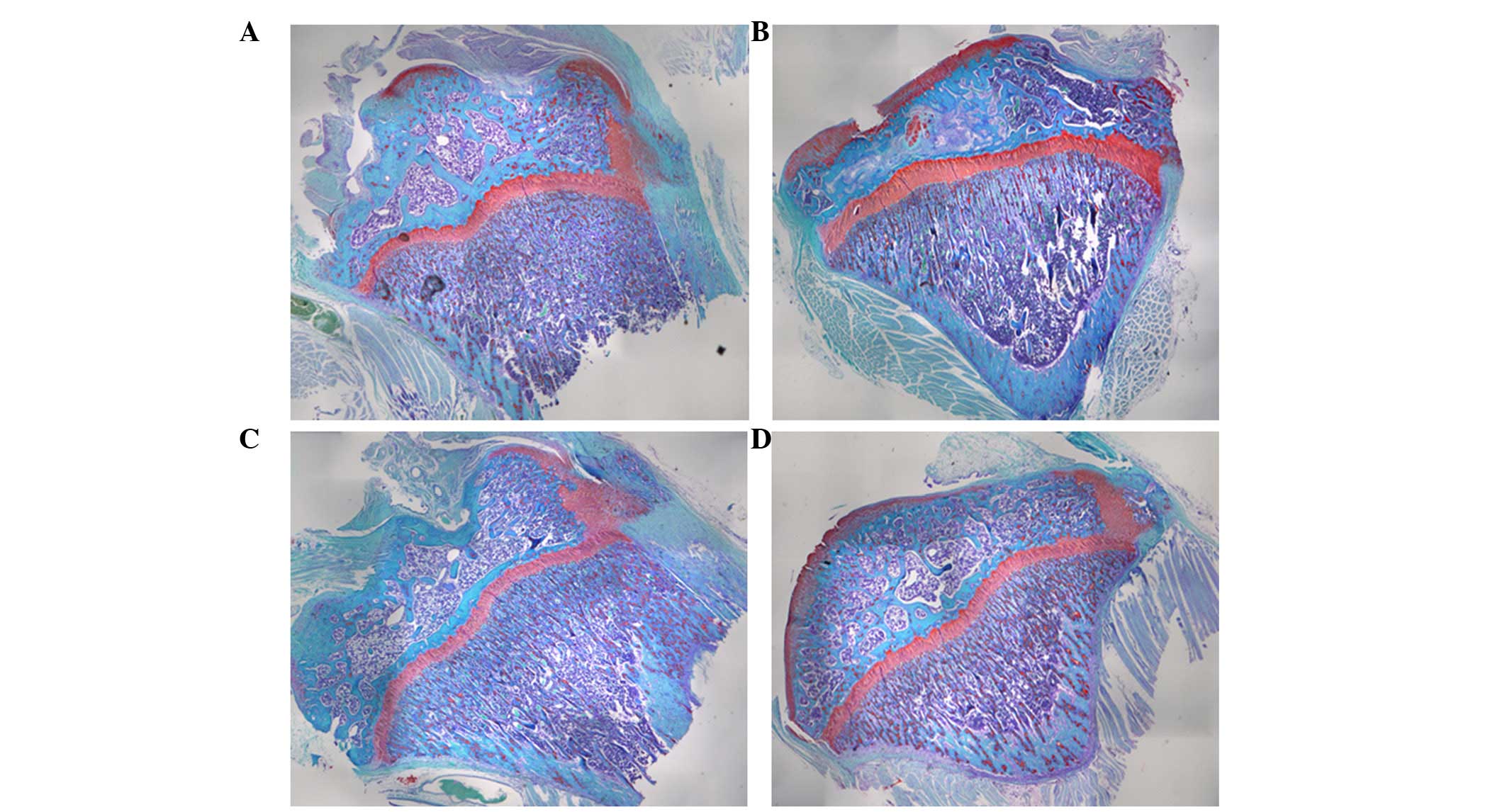
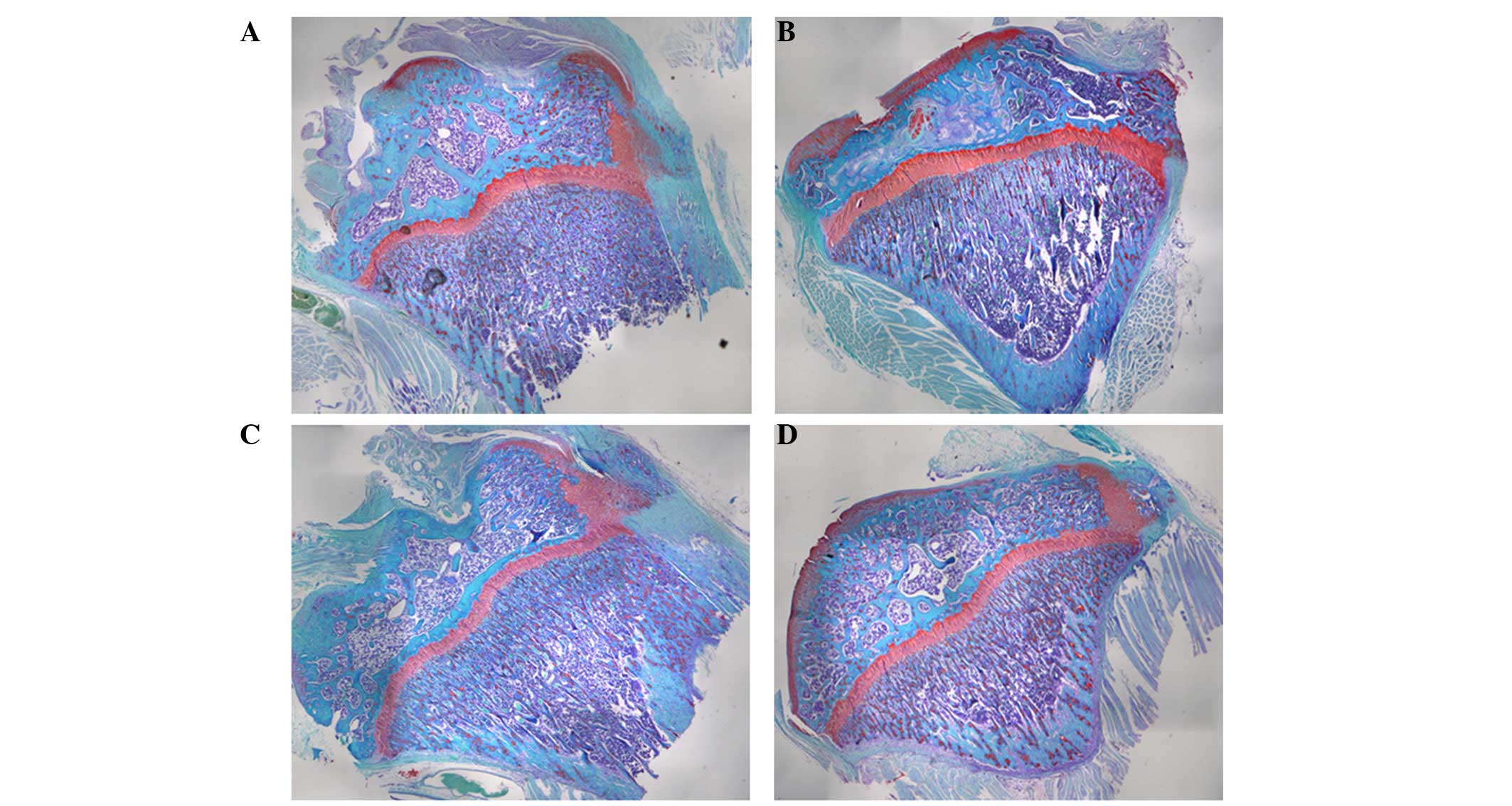
Prevention of cartilage degeneration
by transplantation of MSC sheet
Beside meniscal regeneration, degenerative changes
on the surface of the medial femoral condyle and medial tibial
plateau were evaluated, such as cartilage erosion and osteophyte
formation (Figs. 5 and 6). No chondral lesions were detected at the
time of transplantation surgery. Subsequent to surgery, chondral
damages on the surface of tibial plateau were detected, which were
more severe compared with those on the surface of femoral condyle
in the two groups.
At 4 weeks after surgery, a large area of focal
articular lesions was seen on the surface of tibial plateau in the
control group. Only a small area was covered by cartilage tissue
(Fig. 5A). By contrast, in the MSC
sheet-treated joints, no focal articular lesions were detected on
the surface of tibial plateau at 4 weeks, and cartilage
degeneration of the edge of tibial plateau was observed (Fig. 5B). At 8 weeks, the severity of tibial
plateau chondral damage increased in the control group, with almost
no cartilage observed on the surface of tibial plateau, while the
surface was rugged (Fig. 5C). In the
MSC sheet group, the surface of tibial plateau was slightly coarse,
with some cracks and a decreased GAG content at 8 weeks after
surgery (Fig. 5D).
In the femoral condyle region, the GAG content
decreased gradually between weeks 4 and 8 in the two groups
(Fig. 6). In the control group, the
cartilage from the femoral condyle region exhibited apparent
degeneration at 4 and 8 weeks (Fig. 6A
and C). In the MSC sheet group, the cartilage from the femoral
condyle region exhibited no apparent or slight degeneration at 4
weeks (Fig. 6B), while part of
cartilage area appeared degenerated at 8 weeks.
Based on the ICRS scores (15) of the cartilage from the femoral
condyle region, the MSC sheet-treated group presented higher scores
(18.5±3.3 at 4 weeks and 14.9±2.4 at 8 weeks) when compared with
the control group (12.3±1.8 at 4 weeks and 9.6±0.6 at 8 weeks). All
the results indicated that transplantation of MSC sheet resulted in
a certain degree of protection against OA development in the
rats.
Discussion
In the present study, transplantation of MSC sheet
was demonstrated to promote meniscus regeneration, while reducing
efficiently OA of knee joint. Through the use of MSC sheet
transplantation, the number of MSCs attached to the meniscal defect
can be higher, compared with cell suspension. Furthermore, the MSC
sheet is visible and can be placed around the meniscal defect
directly, filling the space caused by meniscectomy and avoiding
loss of MSCs from targeted defects.
Studies has previously reported the effect of
injection of MSCs on the retardation of articular cartilage
degeneration and meniscus regeneration in massive meniscectomized
models of large animals (16,17).
However, cell suspension injection can cause cell loss and
untargeted organ immigration. In the study of Mizuno et al
(11), 1 million cells were
intra-articular injected into the knee joint in a rat cylindrical
meniscus defect model, and only a faint fluorescence signal was
visible. Therefore, MSCs arranged in a three-dimensional structure
of sheets or aggregates have an improved effect and were found to
be superior to the use of cell suspensions. Katagiri et al
(18) reported that transplantation
of synovial MSC aggregates regenerated the meniscus more
effectively compared with intra-articular injection of synovial
MSCs using the same number of MSCs as a cell suspension in a rat
massive meniscectomized model. The aforementioned results were in
accordance with the findings of the present study, in which MSC
sheet transplantation greatly promoted meniscus regeneration.
The MSC sheet is able to achieve highly efficient
cell delivery (19) and effectively
preserve the cell-cell interaction and the ECM (12). Through direct cell-cell interaction
or the secretion of a broad spectrum of bioactive molecules with
immunoregulatory and/or regenerative activities, the MSC sheet can
exert a significant effect on local tissue repair by modulating the
local environment and activating endogenous meniscus progenitor
cells (20). Furthermore, the cells
in the MSC sheet may be directly involved in meniscus regeneration
due to the site-specific differentiation of MSCs (21).
When the meniscus is injured, the adjacent synovial
tissue can be induced and contribute to the meniscal repair during
the natural period of meniscal healing (22). This was also seen in the results of
the present study. In the untreated control group, a thin
meniscus-like tissue was regenerated on the outside of the host
meniscus at 8 weeks, induced by synovial tissue. By contrast, in
the MSC sheet group, a similar meniscus-like tissue formed at the
outside of the host meniscus at 4 weeks after surgery. These
findings suggest that the transplanted MSC sheet also expressed
trophic factors and stimulated the adjacent synovial tissue, and
subsequently progenitors of meniscus were induced, thus
contributing to the meniscal regeneration.
In the current study, MSC sheet transplantation
reduced the degree of cartilage degeneration, osteophyte formation
and subchondral sclerosis, when compared with the control group, in
accordance with the findings of previous studies of intra-articular
injection of MSC suspensions (17,23,24). Two
possible reasons may explain the results. Firstly, the regenerated
immature meniscus may protect the articular cartilage and suppress
OA progression. In addition, the injected MSC sheet may produce
trophic factors to inhibit progression of articular cartilage
degeneration by inhibiting inflammatory cytokines.
In terms of clinical application, there are several
limitations to the present study. Allogeneic MSC sheets were used
for transplantation; however, autologous MSCs can be easily
obtained from the bone marrow of patients, and then expanded in
culture to construct cell sheets, which can be easily applied in
clinical practice. Therefore, the use of MSC sheet is practically
convenient for meniscal regeneration. However, the observation time
in the current study was too short to evaluate the final outcome of
the meniscus. The time period for neo-meniscus degeneration
requires further investigation. Furthermore, tissue samples were
only analyzed histologically in the present study, with no
biomechanical tests performed on the regenerated meniscus, and thus
the properties of the regenerated meniscus were not investigated.
In spite of these limitations, the present study demonstrated a
novel treatment of MSC sheet transplantation for regeneration of a
massive meniscal defect. This method has the potential to
regenerate the meniscus and inhibit the progression of OA.
In conclusion, transplantation of MSC sheets may
efficiently promote meniscus regeneration, while also inhibit the
progression of OA of the knee joint in a rat massive
meniscectomized model. This transplantation technique using MSC
sheets may have a great potential in meniscus regeneration in
clinical practice.
Acknowledgements
The study was supported by grants from the Natural
Science Youth Foundation of Zhejiang Province (no. LQ14H060001) and
the Natural Science Youth Foundation of China (no. 81401779).
References
|
1
|
Englund M, Roemer FW, Hayashi D, Crema MD
and Guermazi A: Meniscus pathology, osteoarthritis and the
treatment controversy. Nat Rev Rheumatol. 8:412–419. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Song Y, Greve JM, Carter DR and Giori NJ:
Meniscectomy alters the dynamic deformational behavior and
cumulative strain of tibial articular cartilage in knee joints
subjected to cyclic loads. Osteoarthritis Cartilage. 16:1545–1554.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lohmander LS, Englund PM, Dahl LL and Roos
EM: The long-term consequence of anterior cruciate ligament and
meniscus injuries: Osteoarthritis. Am J Sports Med. 35:1756–1769.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tucker B, Khan W, Al-Rashid M and
Al-Khateeb H: Tissue engineering for the meniscus: A review of the
literature. Open Orthop J. 6:348–351. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lee AS, Kang RW, Kroin E, Verma NN and
Cole BJ: Allograft meniscus transplantation. Sports Med Arthrosc.
20:106–114. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lee DH, Kim JM, Lee BS, Kim KA and Bin SI:
Greater axial trough obliquity increases the risk of graft
extrusion in lateral meniscus allograft transplantation. Am J
Sports Med. 40:1597–1605. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Maumus M, Guérit D, Toupet K, Jorgensen C
and Noël D: Mesenchymal stem cell-based therapies in regenerative
medicine: Applications in rheumatology. Stem Cell Res Ther.
2:142011. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Centeno CJ, Busse D, Kisiday J, Keohan C,
Freeman M and Karli D: Increased knee cartilage volume in
degenerative joint disease using percutaneously implanted,
autologous mesenchymal stem cells. Pain Physician. 11:343–353.
2008.PubMed/NCBI
|
|
9
|
Csaki C, Schneider PR and Shakibaei M:
Mesenchymal stem cells as a potential pool for cartilage tissue
engineering. Ann Anat. 190:395–412. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Koga H, Shimaya M, Muneta T, Nimura A,
Morito T, Hayashi M, Suzuki S, Ju YJ, Mochizuki T and Sekiya I:
Local adherent technique for transplanting mesenchymal stem cells
as a potential treatment of cartilage defect. Arthritis Res Ther.
10:R842008. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mizuno K, Muneta T, Morito T, Ichinose S,
Koga H, Nimura A, Mochizuki T and Sekiya I: Exogenous synovial stem
cells adhere to defect of meniscus and differentiate into cartilage
cells. J Med Dent Sci. 55:101–111. 2008.PubMed/NCBI
|
|
12
|
Nakamura A, Akahane M, Shigematsu H,
Tadokoro M, Morita Y, Ohgushi H, Dohi Y, Imamura T and Tanaka Y:
Cell sheet transplantation of cultured mesenchymal stem cells
enhances bone formation in a rat nonunion model. Bone. 46:418–424.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hong Y, Song H, Gong Y, Mao Z, Gao C and
Shen J: Covalently crosslinked chitosan hydrogel: Properties of in
vitro degradation and chondrocyte encapsulation. Acta Biomater.
3:23–31. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pauli C, Grogan SP, Patil S, Otsuki S,
Hasegawa A, Koziol J, Lotz MK and D'Lima DD: Macroscopic and
histopathologic analysis of human knee menisci in aging and
osteoarthritis. Osteoarthritis Cartilage. 19:1132–1141. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
O'Driscoll SW, Keeley FW and Salter RB:
The chondrogenic potential of free autogenous periosteal grafts for
biological resurfacing of major full-thickness defects in joint
surfaces under the influence of continuous passive motion. An
experimental investigation in the rabbit. J Bone Joint Surg Am.
68:1017–1035. 1986.PubMed/NCBI
|
|
16
|
Murphy JM, Fink DJ, Hunziker EB and Barry
FP: Stem cell therapy in a caprine model of osteoarthritis.
Arthritis Rheum. 48:3464–3474. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Al Faqeh H, Nor Hamdan BM, Chen HC,
Aminuddin BS and Ruszymah BH: The potential of intra-articular
injection of chondrogenic-induced bone marrow stem cells to retard
the progression of osteoarthritis in a sheep model. Exp Gerontol.
47:458–464. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Katagiri H, Muneta T, Tsuji K, Horie M,
Koga H, Ozeki N, Kobayashi E and Sekiya I: Transplantation of
aggregates of synovial mesenchymal stem cells regenerates meniscus
more effectively in a rat massive meniscal defect. Biochem Biophys
Res Commun. 435:603–609. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yang J, Yamato M, Kohno C, Nishimoto A,
Sekine H, Fukai F and Okano T: Cell sheet engineering: Recreating
tissues without biodegradable scaffolds. Biomaterials.
26:6415–6422. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Koelling S and Miosge N: Stem cell therapy
for cartilage regeneration in osteoarthritis. Expert Opin Biol
Ther. 9:1399–1405. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chen FH and Tuan RS: Mesenchymal stem
cells in arthritic diseases. Arthritis Res Ther. 10:2232008.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Katagiri H, Muneta T, Tsuji K, Horie M,
Koga H, Ozeki N, Kobayashi E and Sekiya I: Transplantation of
aggregates of synovial mesenchymal stem cells regenerates meniscus
more effectively in a rat massive meniscal defect. Biochem Biophys
Res Commun. 435:603–609. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
González MA, Gonzalez-Rey E, Rico L,
Büscher D and Delgado M: Treatment of experimental arthritis by
inducing immune tolerance with human adipose-derived mesenchymal
stem cells. Arthritis Rheum. 60:1006–1019. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tuan RS: Stemming cartilage degeneration:
Adult mesenchymal stem cells as a cell source for articular
cartilage tissue engineering. Arthritis Rheum. 54:3075–3078. 2006.
View Article : Google Scholar : PubMed/NCBI
|