Introduction
In Japan, the number of deaths associated with
pneumonia is increasing, and pneumonia is now the third leading
cause of mortality worldwide, causing ~10% of all mortalities
(1–3). Patients aged ≥65 years account for
>95% of pneumonia-associated mortalities, and aspiration
pneumonia is common in elderly patients (1,3–5). Although the typical symptoms of
aspiration pneumonia are fever, coughing and sputum, non-specific
symptoms, including appetite loss and impaired consciousness, are
also important. The risk of mortality caused by pneumonia increases
with age, and the number of elderly patients with aspiration
pneumonia is expected to rapidly increase as the human life
expectancy increases (1,4).
At present, aspiration pneumonia combined with
pulmonary tuberculosis is a major concern in elderly patients
(6). Between 1900 and 1950, the
prevalence of tuberculosis in Japan was recorded as >500 per
100,000 of the population (7).
Although the prevalence of tuberculosis was subsequently reduced to
16.7 per 100,000 of the Japanese population in 2012, this figure
remains 3–4 times higher than the prevalence of tuberculosis in
Europe and North America (8). In
Japan, one reason for the relatively high prevalence of
tuberculosis is the aging of individuals who were previously
infected with the disease (9).
In the present study, the diagnostic delay of
pulmonary tuberculosis in two patients with aspiration pneumonia,
who developed acute respiratory distress syndrome (ARDS) according
to the American-European Consensus Conference (AECC) criteria, is
described (10). The patients were
diagnosed with active pulmonary tuberculosis following discharge
from the hospital. Failure to recognize active pulmonary
tuberculosis delays the commencement of anti-tuberculous therapy
and may cause nosocomial transmission of pulmonary
tuberculosis.
Case report
The present study was approved by the Ethics
Committee of Kainan Hospital, Aichi Prefectural Welfare Federation
of Agricultural Cooperatives (Yatomi, Japan).
Case 1
A 92-year-old woman was transported to Kainan
Hospital (Yatomi, Japan) by ambulance on September 10th 2013
complaining of vomiting, a high fever and impaired consciousness.
The patient had developed aspiration pneumonia 4 months previously,
which had successfully been treated with antibiotic therapy [2 g
ampicillin plus 1 g sulbactam sodium (Meiji Seika Pharma, Co.,
Ltd., Tokyo, Japan) every 12 h]. On arrival at our hospital, the
patient presented with the following signs: Temperature, 39.2°C;
pulse rate, 103 beats/min; blood pressure, 92/59 mmHg; and coarse
crackles over the bilateral lungs. Blood test results reported an
increase in the percentage of neutrophils [white blood cells:
8,100/mm3 (normal range, 4,000–9,000/mm3);
95.9% neutrophils) and elevated fibrinogen [519 mg/dl (normal
range, 200–400 mg/dl)] and C-reactive protein [7.5 mg/dl (normal
range, 0.0–0.3 mg/dl)]. In addition, the patient presented with
anemia [hemoglobin, 9.2 g/dl (normal range, 11.5–14.9 mg/dl)] and
low serum albumin [2.1 g/dl (normal range, 4.0–5.0 mg/dl)]. Blood
gas analysis recorded a pH of 7.463, CO2 partial
pressure (PaCO2) of 40.8 mmHg, PaO2 of 68.4
mmHg and O2 saturation (SaO2) of 93.4%. The
aforementioned results were determined by oxygen inhalation through
a mask with a reservoir bag (10 l/min). The ratio of
PaO2 and fraction of inspired O2
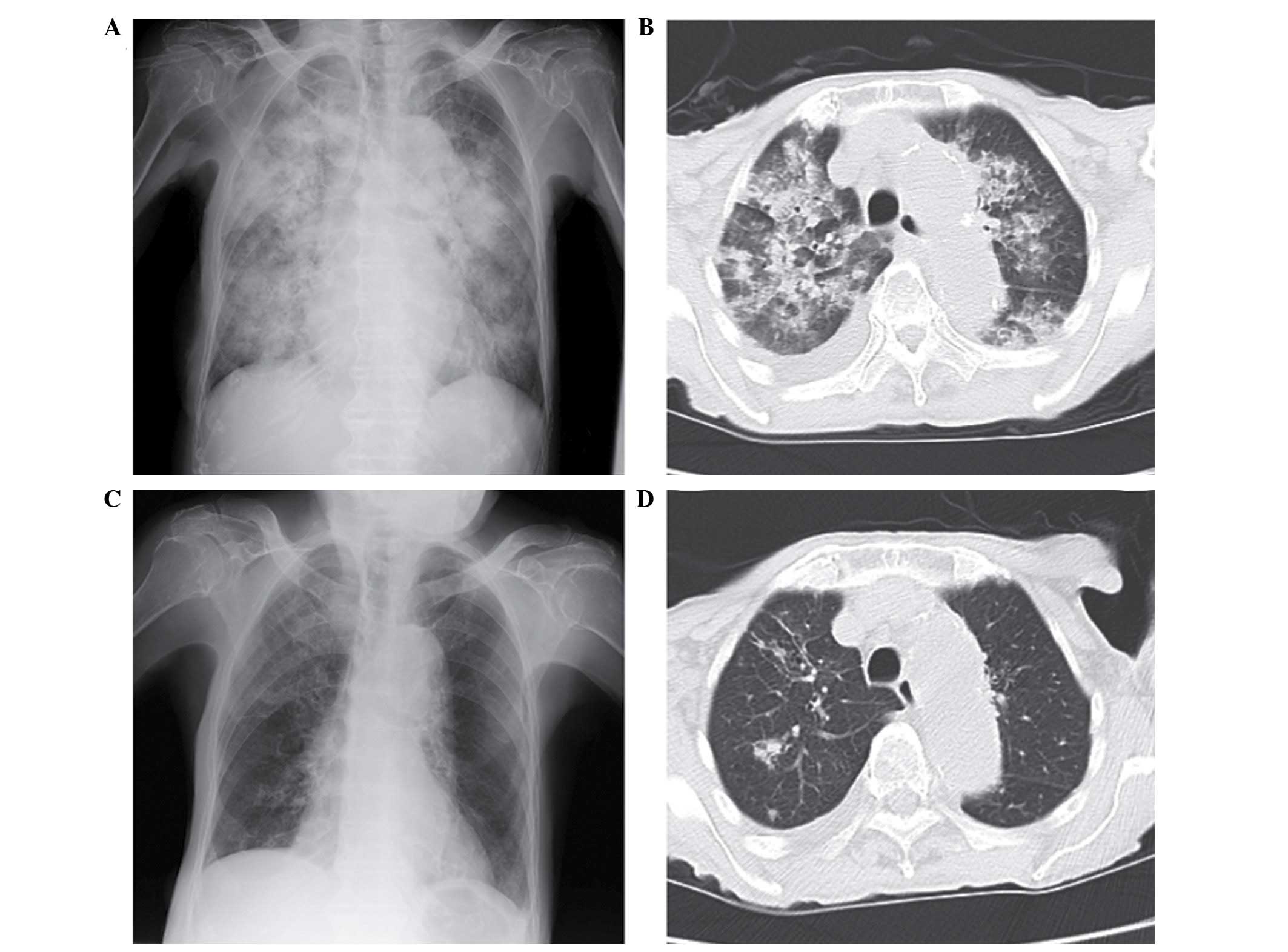
(FiO2) was 68.4. Chest X-ray film and computerised
tomography (CT) presented diffuse bilateral consolidation and right
pleural effusion (Fig. 1A and B).
The sputum test for acid-fast bacilli at the time of admission was
smear negative. No evidence of left atrial hypertension was
detected by ultrasonic cardiography. Therefore, a diagnosis of ARDS
due to aspiration pneumonia was clinically established according to
the AECC criteria (10).
The patient was treated with 4 g piperacillin and
0.5 g tazobactam (both Taiho Pharmaceutical, Co., Ltd., Tokyo,
Japan) antibiotics every 8 h for 10 days, in addition to
O2 therapy and intravenous feeding. The treatments
proved successful; improved oxygenation and a reduced fever were
observed. Therefore, the patient was discharged to a nursing home
on September 26th. A chest X-ray film obtained at the time of
discharge revealed that the diffuse bilateral consolidation had
almost completely disappeared; however, a pale patchy shadow
remained in the right upper lung field (Fig. 1C). On October 3rd, an acid-fast
bacillus examination of the sputum obtained from the patient upon
admission presented with culture-positive results, and a polymerase
chain reaction (PCR) analysis for Mycobacterium tuberculosis
returned positive. The patient was then readmitted to hospital, and
underwent sputum tests for acid-fast bacillus and a chest CT scan.
The chest CT scan identified a nodular opacity with small satellite
nodules in the right upper lobe; these nodules were suspected to be
the focus of the tuberculosis infection (Fig. 1D). Based on the chest CT images and
the results of the acid-fast bacillus re-examination of the sputum,
the patient was diagnosed with smear-negative, active pulmonary
tuberculosis. Treatment was initiated with once daily 200 mg
isoniazid (Daiichi Sankyo Group, Tokyo, Japan), 300 mg rifampicin
(Sandoz K.K., Tokyo, Japan) and 500 mg ethambutol (Kaken
Pharmaceutical, Co., Ltd., Tokyo, Japan), and the patient was
transferred to the Chronic Care Institution for the Aged.
Case 2
An 85-year-old woman was transported to Kainan
Hospital by ambulance on 23rd March 2014 complaining of a high
fever and chest tightness. In addition, the patient had been
experiencing episodes of difficulty in swallowing for 1 month. The
patient history included hypertension, atrial fibrillation, chronic
kidney disease, pulmonary embolism and angina; these conditions
were controlled by medication and an inferior vena cava filter. No
clinical evidence of left atrial hypertension was detected by an
ultrasonic cardiography performed on admission. The patient
presented with the following signs: Temperature, 38.3°C; pulse
rate, 119 beats/min; blood pressure, 86/54 mmHg; and coarse
crackles over the bilateral lungs. Edema in the legs was not
detected on physical examination. Blood tests reported an increased
percentage of neutrophils (white blood cells, 7,800/mm3;
94.2% neutrophils) and elevated levels of creatinine [2.47 mg/dl
(normal range, 0.4–0.7 mg/dl)], urea nitrogen [75.3 mg/dl (normal
range, 8.0–22.0 mg/dl)], lactate dehydrogenase [510 IU/l (normal
range, 119–229 IU/l)] and C-reactive protein (12.09 mg/dl). In
addition, the patient had low total protein [5.8 g/dl (normal
range, 6.7–8.3 IU/l)]and serum albumin (2.4 g/dl) levels. A blood
gas analysis revealed pH 7.467, 23.5 mmHg PaCO2, 107
mmHg PaO2 and 99% SaO2 with oxygen inhalation
through a mask with a reservoir bag (6 l/min). The
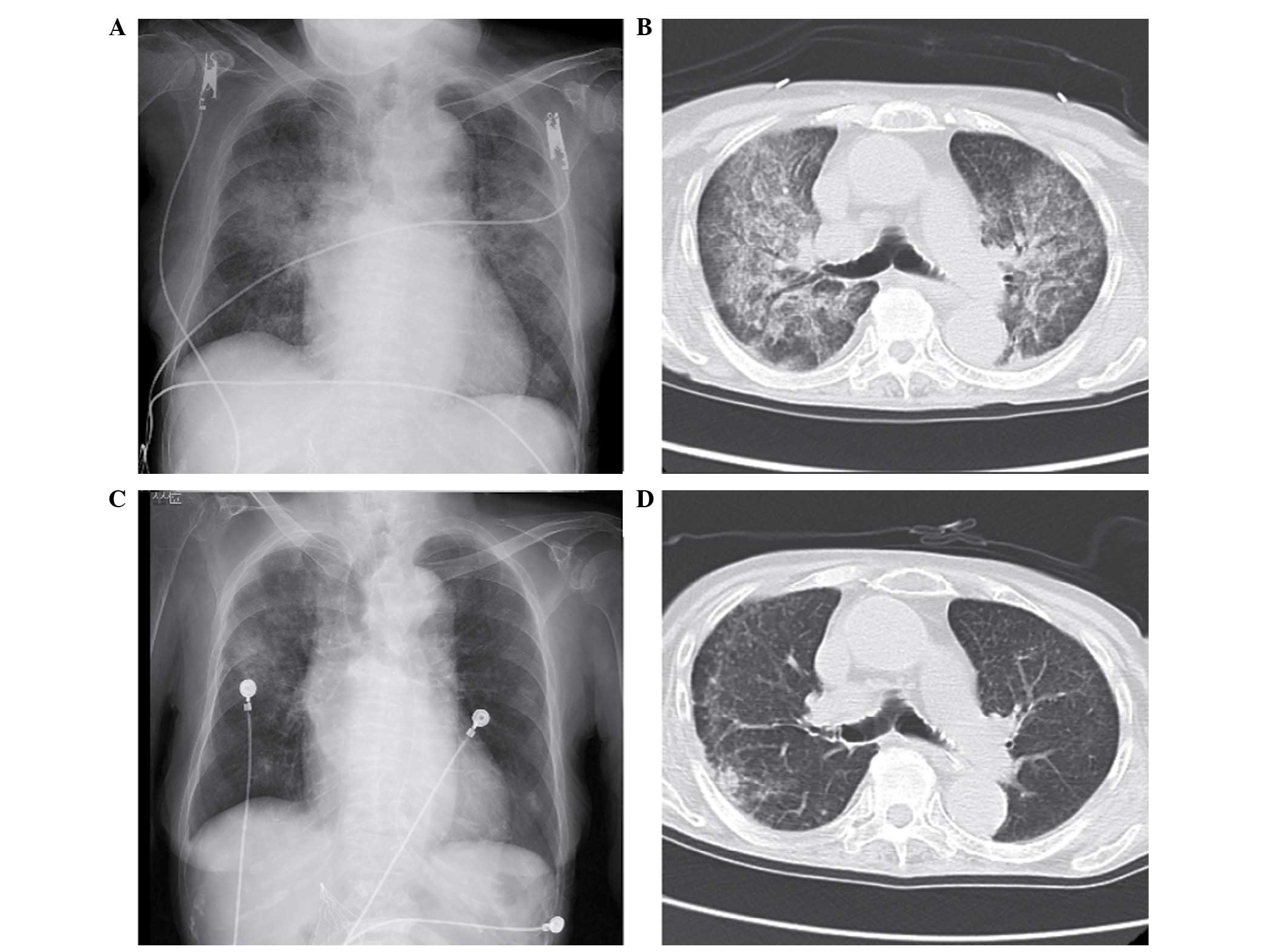
PaO2:FiO2 ratio was 178. Chest X-ray film and
CT identified diffuse bilateral pulmonary infiltrates (Fig. 2A and B). The sputum test for
acid-fast bacillus at the time of admission was smear negative.
Based on the results of the examination and the
episodes of difficulty in swallowing, the patient was clinically
diagnosed with ARDS resulting from aspiration pneumonia. Meropenem
(0.5 g every 12 h; Meiji Seika Pharma, Co., Ltd.) and minocycline
(100 mg once daily; Sawai Pharmaceutical, Co., Ltd., Tokyo, Japan)
antibiotics were administered for 11 days, in addition to oxygen
therapy and intravenous feeding. The treatment was successful
(improved oxygenation and a reduced fever) and the patient was
discharged to a nursing home on 6th April. A chest X-ray film
obtained at the time of discharge from the hospital revealed that
the diffuse bilateral consolidation had almost disappeared;
however, a patchy shadow remained in the right middle lung field
(Fig. 2C). On 14th April, an
acid-fast bacillus examination of the sputum obtained from the
patient upon admission revealed culture-positive results, and a PCR
test for M. tuberculosis was positive. The patient was
immediately readmitted to the hospital and underwent sputum tests
and a chest CT scan. The chest CT scan identified diffuse bilateral
micro-nodules and pale consolidation in the right S2 region; these
nodules and consolidation were proposed to be the focus of the
tuberculosis infection (Fig. 2D). In
addition, acid-fast bacillus re-examination of the sputum revealed
smear-positive results. The patient was diagnosed with
smear-positive, active pulmonary tuberculosis and was transferred
to the National Hospital Organization Higashinagoya National
Hospital (Nagoya, Japan) for anti-tuberculous treatment with
isoniazid (200 mg once daily), rifampicin (300 mg once daily) and
ethambutol (500 mg once daily). Fortunately, nosocomial
transmission of tuberculosis from this patient to other patients
and/or medical staff was not reported.
Discussion
The present study reports two cases of aspiration
pneumonia with bilateral pulmonary infiltrates that resulted in the
delayed diagnosis of pulmonary tuberculosis. The patients were
diagnosed with pulmonary tuberculosis following discharge from the
hospital, possibly due to the fact that the acid-fast bacillus
examination of sputum was performed only once and the result was
smear-negative/culture-positive. Although it may be difficult to
diagnose complicated pulmonary tuberculosis in all patients with
aspiration pneumonia at the time of admission, clinicians should
pay careful attention to the course of pulmonary infiltration and
should perform the acid-fast bacillus test on the sputum a minimum
of three times.
The increasing ratio of elderly patients with newly
diagnosed tuberculosis is a major medical and healthcare issue in
Japan (6,7). The incidence of tuberculosis infection
was frequent in Japan prior to the 1960s, and the aging of these
infected individuals is one of the reasons for the relatively high
prevalence in Japan at present (7–9,11). Elderly patients tend not to present
with typical symptoms, such as weight loss, coughing and fever, and
may not be able to expectorate sputum spontaneously, resulting in a
delayed diagnosis (6,7,9,12,13). In
addition, as the life expectancy of the Japanese population
increases, the increasing incidence of aspiration pneumonia in
elderly patients emerges as a key medical and healthcare concern
(1,2,4,5,14,15). As
symptoms of aspiration pneumonia tend to be non-specific and
overlap with those of pulmonary tuberculosis, the risk of
aspiration pneumonia combined with pulmonary tuberculosis is
prominent in medical care for elderly patients (6,16).
The diagnostic delay of tuberculosis can be divided
into patient and doctor delay (12,16,17).
Patient delay refers to the time from the onset of symptoms to the
first visit to a medical institution, and doctor delay refers to
the time from the patient's first visit to the doctor to diagnosis.
In elderly individuals, patient delay is shorter than in younger
individuals, and doctor delay affects a relatively high percentage
of cases in the elderly population (16,17). The
major causes for late diagnosis following a visit to a medical
institution can be divided into two types: i) The doctor did not
suspect pulmonary tuberculosis at the first visit; or ii) the
results of the acid-fast bacillus examination were delayed
(18). When elderly patients with
pulmonary tuberculosis visit a hospital or arrive there by
ambulance, they are typically diagnosed with aspiration pneumonia
(6). In addition, elderly patients
are more frequently diagnosed with tuberculosis at the hospital
while receiving treatment for other illnesses, in comparison with
younger patients (17). These
observations suggest that diagnosing active tuberculosis is
difficult in elderly patients as a result of nonspecific symptoms
that may be confused with other diseases or the aging process. To
improve this issue, medical staff involved in the care of elderly
patients should be on alert for tuberculosis infection and should
perform adequate examinations, including sputum tests for acid-fast
bacillus, at the first opportunity.
In the two cases presented in the current study, an
age-associated decline in immune function was considered to have
affected the development of tuberculosis and to have contributed to
a decline in the patients' general conditions. In addition, the
compromised general condition of these patients may have
facilitated the development of aspiration pneumonia. Finally,
resulting from a reduction in SaO2, they were
transported to the hospital by ambulance and were initially
diagnosed with ARDS caused by aspiration pneumonia. On evaluation
of the chest CT scans at the time of readmission, tuberculous
lesions, such as nodules with satellite lesions and centrilobular
micronodules, were detected. However, at the time of first
admission, these tuberculous lesions were obscured by the diffuse
bilateral pulmonary infiltration associated with ARDS. In addition,
the smear-negative result in the sputum test for acid-fast bacillus
at the time of initial admission may have had a significant impact
on the delay in diagnosis. Considering the cases presented in the
current study, the following two strategies to prevent diagnostic
delay of pulmonary tuberculosis in elderly aspiration pneumonia
patients should be adopted: i) The sputum test for acid-fast
bacillus examination should be performed at least three times upon
initial admission to hospital; and ii) if the observations are
equivocal on chest X-ray films, regardless of any improvement of
aspiration pneumonia, a chest CT should be performed to closely
evaluate the shadow on the film.
In summary, the present study describes two cases of
pulmonary tuberculosis complicated with aspiration pneumonia. Early
diagnosis of pulmonary tuberculosis was difficult in the present
cases, and acid-fast bacillus examination of the sputum should have
been performed more than once in order to prevent nosocomial spread
of tuberculosis. These cases should remind physicians to consider
the clinical significance of pulmonary tuberculosis, which may
provide further insight into aspiration pneumonia in elderly
patients.
References
|
1
|
Tomono K: Stop Pneumonia Campaign. Nihon
Kyobu Rinsho. 73:S238–S243. 2014.(In Japanese).
|
|
2
|
Ishida T: Epidemiology of pneumonia in
Japan - current status and future considerations. Nihon Naika
Gakkai Zasshi. 100:3484–3489. 2011.(In Japanese). View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ota K and Shibata S: Diagnosis and medical
treatment of aspiration pneumonia. J Clin Rehab. 22:877–885.
2013.(In Japanese).
|
|
4
|
Teramoto S, Fukuchi Y, Sasaki H, Sato K,
Sekizawa K and Matsuse T: Japenese Study Group on Aspiration
Pulmonary Disease: High incidence of aspiration pneumonia in
community- and hospital-acquired pneumonia in hospitalized
patients: A multicenter, prospective study in Japan. J Am Geriatr
Soc. 56:577–579. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Komiya K, Ishii H, Umeki K, Mizunoe S,
Okada F, Johkoh T and Kadota J: Impact of aspiration pneumonia in
patients with community-acquired pneumonia and
healthcare-associated pneumonia: A multicenter retrospective cohort
study. Respirology. 18:514–521. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ubukata S, Jingu D, Yajima T, Shoji M and
Takahashi H: Occurrence and clinical characteristics of
tuberculosis among home medical care patients. Kekkaku. 89:649–654.
2014.(In Japanese). PubMed/NCBI
|
|
7
|
Toyota E, Machida K, Nagayama N, Yamane A,
Komiya K, Ito S, Suzuki J, Kashizaki F, Shimada M, Matsui Y, et al:
Clinical investigation among elderly patients with tuberculosis.
Kekkaku. 85:655–660. 2010.(In Japanese). PubMed/NCBI
|
|
8
|
Tuberculosis Surveillance Center; RIT;
JATA: Tuberculosis Annual Report 2012. (1). Summary of tuberculosis
notification statistics and foreign-born tuberculosis patients.
Kekkaku. 89:619–625. 2014.(In Japanese). PubMed/NCBI
|
|
9
|
Fukushima Y, Shiobara K, Shiobara T,
Tatewaki M, Anzai M, Fukushima F, Yamada I, Hirata H, Sugiyama K
and Fukuda T: Patients in whom active tuberculosis was diagnosed
after admission to a Japanese university hospital from 2005 through
2007. J Infect Chemother. 17:652–657. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bernard GR, Artigas A, Brigham KL, Carlet
J, Falke K, Hudson L, Lamy M, Legall JR, Morris A and Spragg R: The
American-European Consensus Conference on ARDS. Definitions,
mechanisms, relevant outcomes, and clinical trial coordination. Am
J Respir Crit Care Med. 149:818–824. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tuberculosis Surveillance Center; RIT;
JATA: Tuberculosis annual report 2012 - (2) Childhood and elderly
tuberculosis. Kekkaku. 89:673–678. 2014.(In Japanese). PubMed/NCBI
|
|
12
|
Lin CY, Lin WR, Chen TC, Lu PL, Huang PM,
Tsai ZR, Huang MS, Tsai WC and Chen YH: Why is in-hospital
diagnosis of pulmonary tuberculosis delayed in southern Taiwan? J
Formos Med Assoc. 109:269–277. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rajagopalan S: Tuberculosis and aging: A
global health problem. Clin Infect Dis. 33:1034–1039. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kadota J: Guideline for nursing and
healthcare-associated pneumonia (NHCAP). Nippon Naika Gakkai
Zasshi. 100:3503–3509. 2011.(In Japanese). View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Teramoto S: Preventive strategy for
reccuurent aspiration pneumoina. Nippon Naika Gakkai Zasshi.
100:3578–3585. 2011.(In Japanese). View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Akagawa S: Present situation and practical
treatment of elderly tuberculosis patients in Japan. Nippon Ronen
Igakkai Zasshi. 47:165–173. 2010.(In Japanese).
|
|
17
|
Ohmori M, Ozasa K, Mori T, Wada M,
Yoshiyama T, Aoki M, Uchimura K and Ishikawa N: Trends of delays in
tuberculosis case finding in Japan and associated factors. Int J
Tuberc Lung Dis. 9:999–1005. 2005.PubMed/NCBI
|
|
18
|
Yamamoto K, Osumi M, Kinoshita A, Matsuoka
Y, Yanagihara K, Sakito O, Inoue Y, Fukushima K, Yonekura M and
Kohno S: Incidence of tuberculosis and evaluation of diagnostic
delay in admitted patients during past four years at national
hospital organization Nagasaki Medical Center. IRYO. 62:323–330.
2008.(In Japanese).
|