Introduction
Esthesioneuroblastoma (ENB), or olfactory
neuroblastoma, was first described by Berger et al in 1924
(1). ENB is a rare malignant tumor
accounting for 3% of all intranasal tumors (2), with an estimated incidence of 0.4 cases
per million in the general population (3,4). The
tumor may occur at any age, however, it has a bimodal distribution
with incidence peaks in the 2nd and 6th decades of life. In
addition, there appears to be no gender bias in the incidence of
ENB (4,5). Whilst the histological origin of this
tumor is not fully known, it has been proposed that ENB originates
from stem cells of the olfactory epithelium-derived neural crest
(6,7). The most common symptoms are nasal
obstruction, epistaxis and persistent nasal discharge. Less
commonly, ENB may manifest as visual alterations, headache, orbital
proptosis, diplopia, hyposmia, anosmia, pain and facial sweating
(4,7). This tumor appears as a polyploid mass
surrounding the upper aspect of the nasal cavity, with frequent
involvement of the cribriform plate region. Tumor expansion
predominantly occurs at the paranasal sinuses, orbits and skull
base, while the tumor growth ranges from indolent to rapid in
certain cases (3). Metastasis to the
cervical lymph nodes occurs in 10–44% of ENB cases (8,9).
However, to the best of our knowledge, only 4 cases of
retropharyngeal lymph node metastases have been reported in the
literature to date (10).
For the diagnosis, staging and follow-up of ENBs,
computed tomography (CT) and magnetic resonance imaging (MRI) are
used, which commonly detect the presence of a heterogeneous mass in
the upper nasal cavity, cribriform plate and anterior cranial fossa
(11). Staging of ENB tumors follows
the criteria described by Kadish et al (12) in 1976. Patients presenting with the
tumor restricted to the nasal cavity are classified into stage A,
patients with cancer involving the nasal cavity and at least one
sinus are classified into stage B, and stage C refers to malignancy
with extension beyond the paranasal cavities (12).
An effective standard treatment for ENB has yet to
be established. A meta-analysis performed by Dulguerov et al
(7) indicated that optimal treatment
is complete surgical resection followed by radiation therapy, which
showed lower recurrence rates and 65% survival at five years.
Multimodality therapy, including chemotherapy, has been suggested
by a number of studies (13–16). In addition, recent study by Uslu
et al (17) reported the case
of a 69-year-old patient with olfactory neuroblastoma who was
treated by combined surgical excision and radiotherapy. Currently,
treatment with radionuclides bound to somatostatin analogues is
performed in selected patients with neuroendocrine tumors, with
considerable response. In order to confirm the presence of
somatostatin receptors in the tumor, a whole body scan (WBS) with
indium-111 (111In)-octreotide is commonly performed.
Lutetium-177 (177Lu) is a radionuclide that emits β
particles and γ photons, and can be used in the treatment of
certain neoplasms when attached to a somatostatin analogue, such as
DOTA-octreotate (known as 177Lu-DOTA-TATE). Patients
with somatostatin-positive neuroendocrine tumors may be
administered three to four doses of 177Lu-DOTA-TATE
intravenously, accumulating a total dose of 22,200–29,600 GBq
(18,19). Co-treatment with amino acids (such as
2.5% arginine and 2.5% lysine) is recommended for renal protection,
and is administered prior to and following each therapeutic dose
(20). However, adjuvant treatment
with somatostatin analogues has not been previously investigated in
patients with ENB, due to the rarity of the disease.
The present study described the case of a
74-year-old female with numerous recurrences of ENB following
multiple treatments and without possibility of resection, who was
successfully treated with 177Lu-DOTA-TATE. The present
study was approved by the Research and Ethics Committee of Barretos
Cancer Hospital (São Paulo, Brazil).
Case report
A 74-year-old female experienced an episode of
epistaxis in June 1993. At the time, an MRI scan of the sinuses
revealed an expansive lesion involving the nasal cavity and
sphenoid sinus, ethmoid cells and infiltration of the dura mater
and cribriform lamina. The patient underwent surgical resection of
the tumor at Catanduya's Hospital (São Paulo, Brazil) and
pathological tests indicated a diagnosis of ENB. Subsequently, the
patient underwent radiotherapy with 6,760 cGy (between July and
August, 1993) and chemotherapy with cyclophosphamide, cisplatin and
etoposide (July, 1993).
In 2003, the patient noticed a right cervical node,
and following excision, a nodular lymph node metastasis of the
primary tumor was confirmed by immunohistochemistry. Subsequently,
in 2005, another cervical node was identified. This was removed by
biopsy and immunohistochemical tests confirmed further ENB
metastasis.
In 2008, the patient was referred to the Barretos
Cancer Hospital (Barretos, Brazil) because of neck and malar
nodules causing local deformity, and was admitted to the Department
of Head and Neck Surgery (February, 2008). The patient exhibited
growth of the cervical nodes, however, did not present with other
complaints. Clinical physical examination revealed a 6.0 cm nodule
in the right cervical region, with a solid and not very mobile
lymph node located in the left submandibular region, while 4.0 and
2.0 cm nodules with the same features were also observed in the
left cervical aspect. The patient subsequently underwent right neck
dissection at levels I, II, III and IV (April, 2008), from which
pathological tests, including immunohistochemistry, indicated
poorly-differentiated neoplasms in 10/13 of the removed lymph nodes
and multiple foci of venous invasion. Immunohistochemical analysis
confirmed the presence of metastatic ENB; results showed positivity
for 34B, 35B, cromogramine and S11, and negativity for AE1/AE3,
p63, synaptofisine and enolasis. Subsequent radical surgery of the
left neck lymph nodes (June, 2008) revealed conglomerate lymph node
metastases in 7/13 of the removed nodes, with soft tissue invasion
to the adjacent dermis. In March 2009, an oropharynx CT scan
indicated metastatic masses with unclear limits. One of the masses
was located in the left malar region measuring 2.7×1.5×2.5 cm,
superficial to the maxillary sinus and covering the intra-orbital
foramen, and another was located in the left retropharyngeal
region, measuring 1.8×1.5×2.1 cm and surrounding the internal
carotid artery. Resection was not an option at this point, and the
patient was treated with radiotherapy.
In July 2009, the patient reported a left malar node
and upon clinical examination, the mass was observed to be solid,
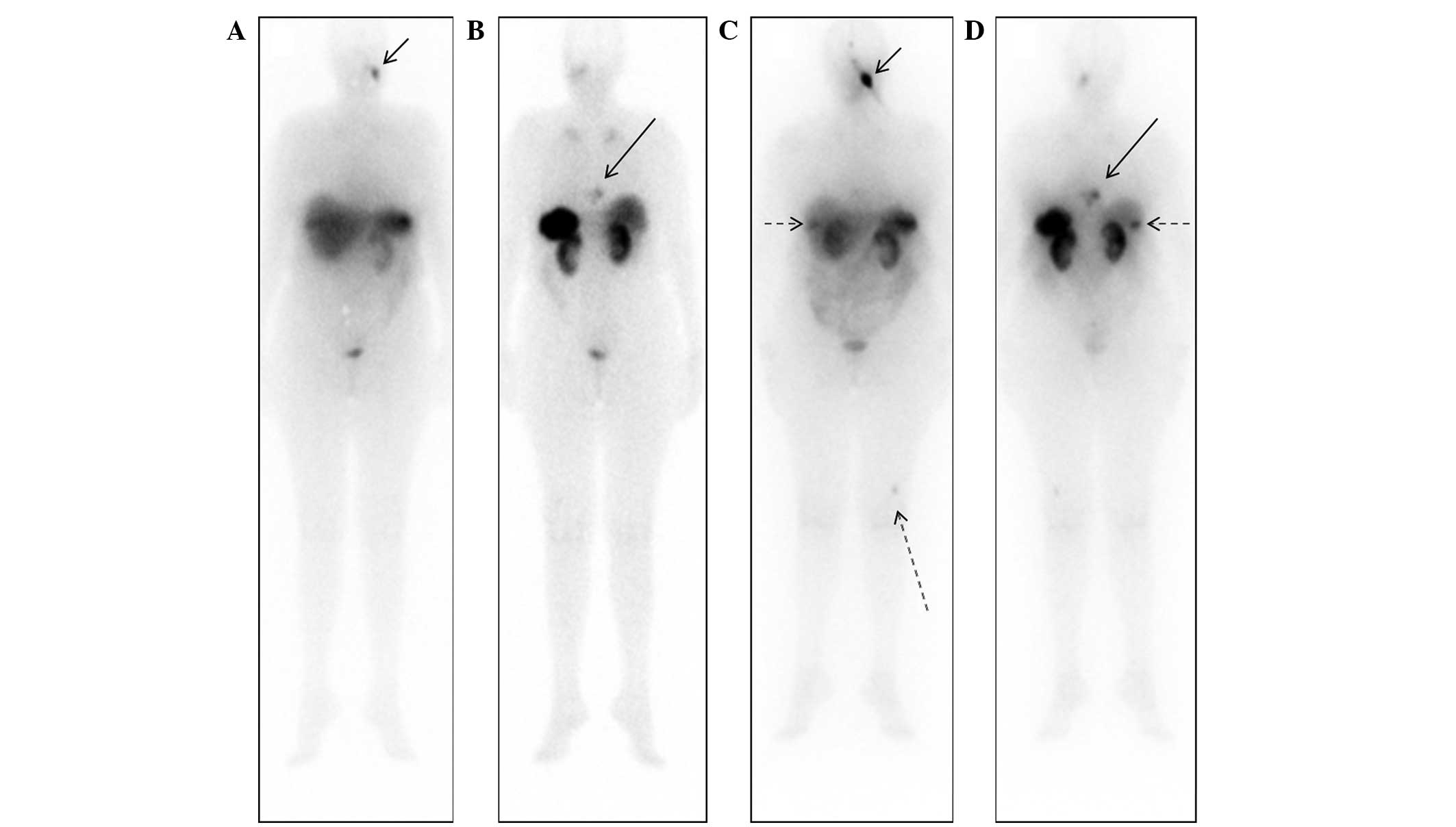
deep and difficult to measure. A WBS using
iodine-131-metaiodobenzylguanidine (Nuclear and Energetic Research
Institute, São Paulo, Brazil) identified no abnormal uptake;
however, a diagnostic WBS with 111In-octreotide (Nuclear
and Energetic Research Institute) showed uptake in the left malar
and posterior thoracic regions (Fig. 1A
and B), indicating the potential for treatment with
somatostatin analogue therapy using 177Lu-DOTA-TATE
(Nuclear and Energetic Research Institute). A thoracic CT scan at
this time indicated mild sclerosis of the T9 vertebra. The first
treatment with 7,400 MBq of 177Lu-DOTA-TATE was
administered in January 2010. A WBS at 24 h post-treatment with
111In-Octreotide revealed uptake in the left malar
region, lower thoracic segment, segments VI/VII of the liver and in
the distal femur (Fig. 1C and D).
The second round of 7,400 MBq of 177Lu-DOTA-TATE therapy
was administered in April 2010, with good uptake of the
radiopharmaceutical and without marked alterations in the imaging
pattern. A CT scan performed at this time revealed a hyperdense
nodule in the right lobe of the liver and increased sclerosis in
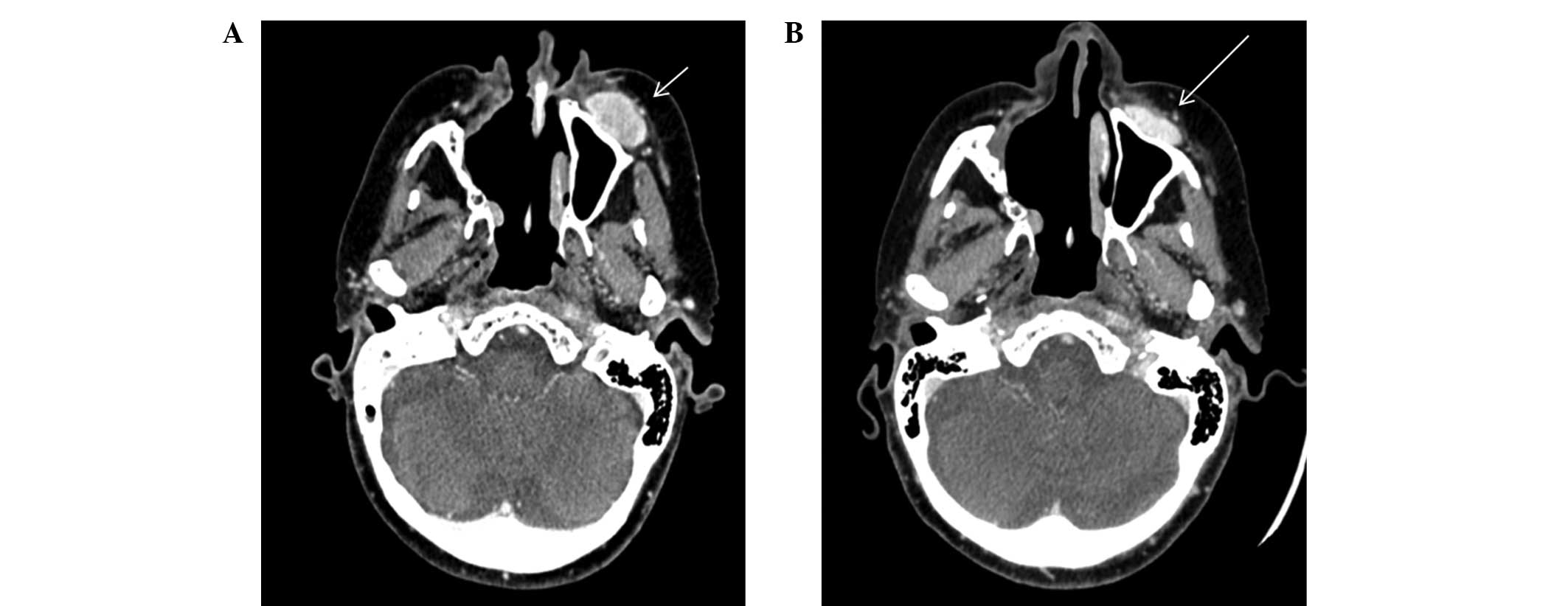
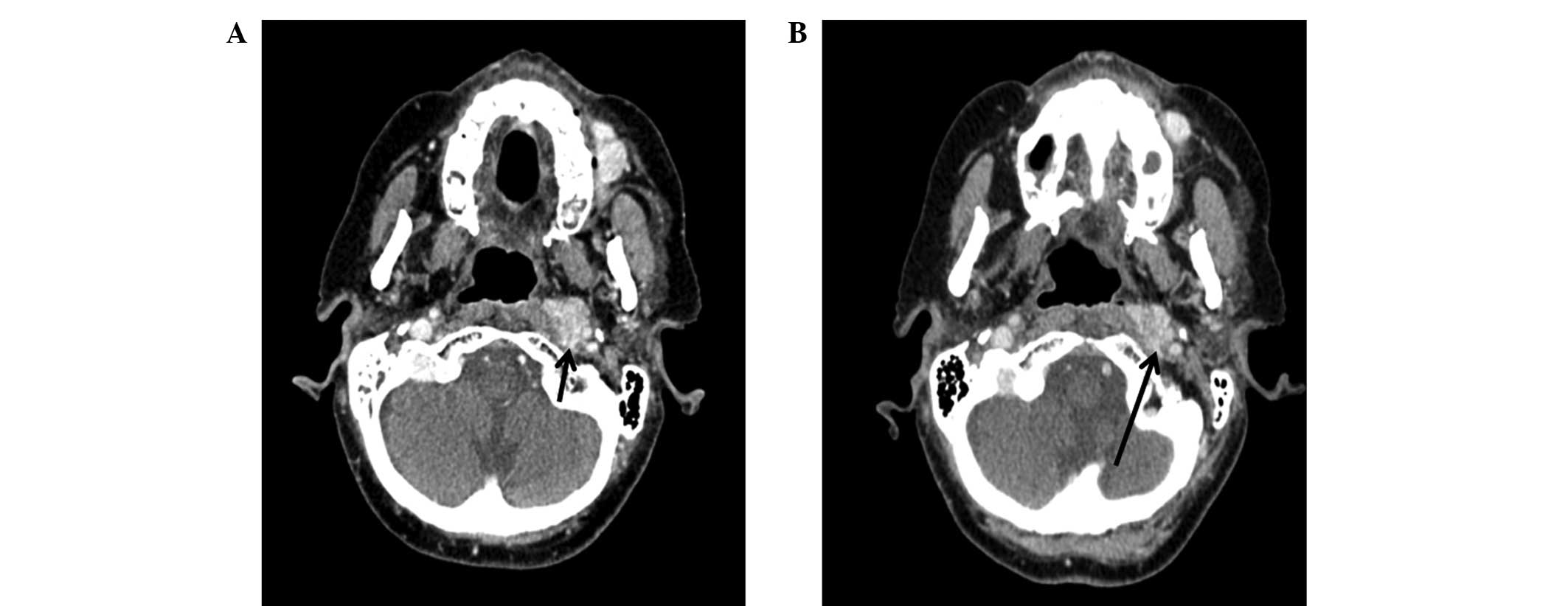
the T9 vertebra. The third round of 7,400 MBq of
177Lu-DOTA-TATE therapy was administered in June 2010,
and a WBS post-treatment with 111In-Octreotide revealed
a marked reduction in the size of the lesions. However, CT scans
indicated minimal reduction of the left malar nodule (Fig. 2) and the persistence of the
retropharyngeal node (Fig. 3).
A follow-up WBS with 111In-Octreotide in
March 2011 demonstrated near complete resolution of the thoracic
lesion and a marked reduction of the lesion in the liver and the
region corresponding to the malar lesion. In addition, a CT scan in
January 2012 confirmed the radiological stability of the disease
following the three treatments with 177Lu-DOTA-TATE.
Discussion
ENB is a rare neuroectodermal neoplasm arising from
the olfactory neuroepithelium. A study performed in Denmark,
reviewing patients with ENB between 1978 and 2000, gave an
incidence of 0.4 patients/million inhabitants per year (40 cases)
(3). Staging such rare tumors can be
challenging, since small series of subjects are analyzed. Morita
et al (21) proposed a
modification of the Kadish system, redefining stage C and adding
stage D, for patients with distant metastasis. By means of that
classification, the patient in the present study fits in stage C
with disease spreading beyond the paranasal sinuses. The rationale
for the treatment in the present study was the fact that
somatostatin receptors are expressed at high levels in ENB
(22) and thus it would be
susceptible to somatostatin analogues, such as DOTA-DATE-177Lu.
In a previous study, immunohistochemical analysis
was performed on ENB samples in order to investigate the presence
of somatostatin receptor subtypes (20). The study demonstrated that type 2
somatostatin receptors have a high affinity for octreotide
(20). In the MAURITIUS Phase II
clinical trial, the use of 90Y-DOTA, which has an
affinity for type 2, 3, 4 and 5 somatostatin receptors, led to the
regression or stabilization of disease in 60% of patients with
varying types of progressive neuroendocrine cancer (23). However, an agent specific for the
type 2 somatostatin receptor has yet to be reported (22). The occurrence of metastasis to the
retropharyngeal lymph nodes reported in the current case study is
considered rare. To the best of our knowledge, the present study is
the first report of the use of somatostatin analogues in the
treatment of ENB. Treatments performed since 1993 follows
literature recommendations of Dulguerov's meta-analysis (7), including surgery, radiation therapy and
chemotherapy. Adjuvant chemotherapy was performed with cisplatin
and etopside, but without the subsequent proton radiaton used by
Harvard University in a series of 9 patients, with good results
(24).
Although described as rare, retropharyngeal lymph
node metastasis was considered as frequent in a study by Howella
et al (25). Despite the
absence of a central nervous system invasion, the patient in the
present study showed a vertebrae lesion with somatostatin analogue
uptake, highly suggestive of secondary involvement. In addition,
hepatic metastasis has been reported (26).
To the best of our knowledge, at the treatment
period time, no other patient with ENB was treated with
somatostatin receptor analogue linked to Lutetium 177. However, in
April 2015 a case report was published with the initiative. The
subject was submitted to four cycles of octreotide-111In and three
cycles of DOTA-TATE-177Lu, alleviating the symptoms and improving
quality of life. However, the disease progressed and the patient
passed away shortly thereafter (27). The patient in the present study is
still alive, being treated with palliative care only, even with
multiple bone lesions and hepatic involvement.
In conclusion, the current case report indicates
that treatment with radiolabeled somatostatin analogues may be an
effective alternative in similar cases where the neoplastic disease
is inoperable and metastatic. This therapy was able to successfully
control the disease, indicating that it may be a novel therapeutic
strategy for this pathology.
References
|
1
|
Berger L, Luc G and Richard D:
L'esthésioneuroépithéliome olfactif. Bull Assoc Franç Étude Cancer.
13:410–421. 1924.(In French).
|
|
2
|
Chirico G, Pergolizzi S, Mazziotti S,
Santacaterina A and Ascenti G: Primary sphenoid
esthesioneuroblastoma studied with MR. Clin Imaging. 27:38–40.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Theilgaard SA, Buchwald C and Ingeholm P:
Esthesioneuroblastoma: A Danish demographic study of 40 patients
registered between 1978 and 2000. Acta Otolaryngol. 123:433–439.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Thompson LD: Olfactory neuroblastoma. Head
Neck Pathol. 3:252–259. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Schiro BJ, Escott EJ, Mchugh JB and Carrau
RL: Bone invasion by an esthesioneuroblastoma mimicking fibrous
dysplasia. Eur J Radiol. 65:69–72. 2008.
|
|
6
|
Bhattacharyya N, Thornton AF, Joseph MP,
Goodman ML and Amrein PC: Successful treatment of
esthesioneuroblastoma and neuroendocrine carcinoma with combined
chemotherapy and proton radiation: Results in 9 cases. Arch
Otolaryngol Head Neck Surg. 123:34–40. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dulguero VP, Allal AS and Calcaterra TC:
Esthesioneuroblastoma: A meta-analysis and review. Lancet Oncol.
2:683–690. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rinaldo R, Ferlito A, Shaha AR, Wei WI and
Lund VJ: Esthesioneuroblastoma and cervical lymph node metastases:
Clinical and therapeutic implications. Acta Otolaryngol.
122:215–221. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pickuth D, Heywang-Köbrunner SH and
Speilman RP: Computed tomography and magnetic resonance imaging
features of olfactory neuroblastoma: An analysis of 22 cases. Clin
Otolaryngol Allied Sci. 24:457–461. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zollinger LV, Wiggins RH, Cornelius RS and
Phillips CD: Retropharyngeal lymph node metastasis from
esthesioneuroblastoma: A review of the therapeutic and prognostic
implications. AJNR Am J Neuroradiol. 29:1561–1563. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
de Vos FY, Willemse PH and de Vries EG:
Successful treatment of metastatic esthesioneuroblastoma. Neth J
Med. 61:414–416. 2003.PubMed/NCBI
|
|
12
|
Kadish S, Goodman M and Wang CC: Olfatory
neuroblastoma. A clinical analysis of 17 cases. Cancer.
37:1571–1576. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chamberlain MC: Treatment of intracranial
metastatic esthesioneuroblastoma. Cancer. 95:243–248. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lund VJ, Howard D, Wei W and Spittle M:
Olfactory neuroblastoma: Past, present, and future? Laryngoscope.
113:502–507. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Eich HT, Hero B, Staar S, Micke O,
Seegenschmiedt H, Mattke A, Berthold F and Müller RP: Multimodality
therapy including radiotherapy and chemotherapy improves event free
survival in stage C esthesioneuroblastoma. Strahlenther Onkol.
179:233–240. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Diaz EM Jr, Johnigan RH, Pero C, El-Naggar
AK, Roberts DB, Barker JL and DeMonte F: Olfactory neuroblastoma:
The 22-year experience at one comprehensive cancer center. 27.
138–49. 2005.
|
|
17
|
Uslu GH, Canyilmaz E, Zengin AY, Mungan S,
Yoney A, Bahadir O and Gocmez H: Olfactory neuroblastoma: A case
report. Oncol Letters. 10:3651–3654. 2015.
|
|
18
|
Bodei L, Brand J Mueller, Baum RP, Pavel
ME, Hörsh D, O'Dorisio MS, O'Dorisio TM, Howe JR, Cremonesi M,
Kwekkeboom DJ and Zaknun JJ: The JOINT IAEA, EANM and SNMMI
practical guidance on peptide receptor radionuclide therapy (PRRNT)
in neuroendocrine tumors. Eur J Nucl Med Mol Imaging. 40:800–816.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kwekkeboom DJ, de Herder WW, Kam BL, van
Eijck CH, van Essen M, Kooij PP, Feelders RA, van Aken MO and
Krenning EP: Treatment with the radiolabeled somato- statin analog
[177Lu-DOTA0, Tyr3]octreotate: Toxicity, efficacy, and survival. J
Clin Oncol. 26:2124–2130. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
De Jong M, Breeman WA, Bernard BF, Bakker
WH, Schaar M, van Gameren A, Bugaj JE, Erion J, Schmidt M,
Srinivasan A and Krenning EP: 177Lu-DOTA (0), Tyr3
octreotate for somatostatin receptor targeted radionuclide therapy.
Int J Cancer. 92:628–633. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Morita A, Ebersold MJ, Olsen KD, Foote RL,
Lewis JE and Quast LM: Esthesioneuroblastoma: Prognosis and
management. Neurosurgery. 32:706–714. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Rostomily RC, Elias M, Deng M, Elias P,
Born DE, Muballe D, Silbergeld DL, Futran N, Weymuller EA, Mankoff
DA and Eary J: Clinical utility of somatostatin receptor
scintigraphic imaging (Octreoscan) in esthesioneuroblastoma: A case
study and survey of somatostatin receptor subtype expression. Head
Neck. 28:305–312. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Virgolini I, Britton K, Buscombe J,
Moncayo R, Paganelli G and Riva P: In- and Y-DOTA-lanreotide:
Results and implication of the MAURITIUS trial. Semin Nucl Med.
32:148–155. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Fitzek MM, Thornton AF and Varvares M:
Neuroendocrine tumors of the sinonasal tract. Results of a
prospective study incorporating chemotherapy, surgery, and combined
proton-photon radiotherapy. Cancer. 94:2623–2634. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Howell MC, Branstetter BF and Snyderman
CH: Patterns of Regional Spread for Esthesioneuroblastoma. AJNR AM
J Neuroradiol. 32:929–933. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rajesh, Shekhar S and Madhavan S:
Esthesioneuroblastoma with hepatic and splenic metastasis. Indian J
Radiol Imag. 13:219–222. 2003.
|
|
27
|
Makis W, McCann K and McEwan A:
Esthesioneuroblastoma (olfactory neuroblastoma) treated with
111In-octreotide and 177Lu-DOTATATE PRRT. Clin Nucl Med. 4:317–321.
2015. View Article : Google Scholar
|