Introduction
Recombinant human growth hormone (rhGH) may be
applied to growth hormone deficiency (GHD), gonadal dysgenesis,
Noonan syndrome, SBS, chronic renal insufficiency, Prader-Willi
syndrome, idiopathic short stature (ISS), SHOX gene deletion
and SGA (1,2). It can not only promote linear growth,
but also improve body composition and metabolism, increase bone
density, and improve the quality of life. Relevant instructions of
various countries provide guidance for indication, application
notes, adverse reaction monitoring to ensure the safety and
effectiveness of the drugs (3–5).
Previous studies showed that growth hormone (GH)
secretion is similar to pulse releasing in that its excitation test
cannot diagnose dwarfism and assess the therapeutic effect
efficiently (6,7). Previous findings showed that the
effects of GH growth promotion mechanism, insulin-like growth
factor (IGF)-1 and IGF-binding protein (IGFBP)-3 are associated
with the SHOX gene (8,9).
Additionally, the stability of IGF-1 and IGFBP-3 in vivo may
become a good index of evaluating the disease process. Thyroid
hormone plays an important role in growth and metabolism and early
intellectual development (10).
Consequently, the present study analyzed the effects of rhGH in the
treatment of dwarfism and the relationship between IGF-1, IGFBP-3
and thyroid hormone.
Materials and methods
Patients
In total, 66 patients diagnosed with dwarfism from
January, 2005 to January, 2010 were selected retrospectively, of
whom 36 cases were GHD and 30 cases were ISS, according to the ISS
diagnosis criteria and the GH application guidelines by American
Lawson-Wilkins Pediatric Endocrine Society, ESPE, GHRS and AACE
(3–5). The initial therapeutic dose GHD 0.10
IU/kg·day and ISS 0.15 IU/kg·day were injected subcutaneously every
night before sleep until adulthood. The dose was adjusted according
to the therapeutic effect and evaluation index. When the height
reached the normal adult height range (>-2 SD), or next to the
normal height, i.e., growth rate <2 cm/year, boy's BA >16
years, girl's BA >14 years, the drugs were stopped. The drugs
were also used until 6–7 years after reaching adult height.
Congenital dysplasia, chromosomal abnormalities, nutritional
disorders, and imperfect clinical data lost to follow-up were all
excluded. The study was approved by the Ethics Committee of the
Dongying People's Hospital (Shandong, China). All of the families
of the patients were informed of the aims of the study and the
parents gave informed consent. The GHD group included 20 boys and
16 girls; aged 2–10 years, with an average of 6.6±2.4 years. The
ISS group included 16 boys and 14 girls; aged 2.5–13 years, with an
average of 6.9±2.5 years. The differences of gender and age of the
two groups were not statistically significant (P>0.05).
Observation index
The patients were followed up until January 2016,
with an average follow-up of ~5 years; the effects and indexes,
including height, BA, secondary test of growth hormone (GH peak),
IGF-1, IGFBP-3 and thyroid hormone (FT3, FT4 and TSH) were
evaluated every 3 months. The height was measured by a specially
assigned individual with the same tool (produced by Shanghai Nine
Peaks Weighing Apparatus Factory, Shanghai, China). The under
collars were fixed, heels, buttocks, occiputs touched the column at
the same time, and the average value was taken after 3 continuous
measurements, with centimeters as the unit. The BA was measured by
taking X-ray of the left hand, including the hand bone, wrist and
radial ulnar stem 3–4 cm. The same specially assigned investigator
scanned the image and evaluated the BA according to the Chinese
bone maturation evaluation standard scoring method. Growth hormone
stimulation test included: Pyridostigmine bromide (4 mg/kg, max 60
mg) and clonidine (2.5 µg/kg, max 150 µg) taken orally on an empty
stomach. Subsequently, 3 ml of median elbow vein blood was drawn 0,
60, 90 and 120 min after taking the drugs. The serum GH level was
measured with the Siemens automated Immulite 2000 chemiluminescence
detection instrument (Siemens Healthcare Diagnostics, Los Angeles,
CA, USA) and the original kit; IGF-1 and IGFBP-3 were measured with
the double antibody sandwich method and the kits were provided by
Sigma-Aldrich (St. Louis, MO, USA). FT3, FT4 and TSH were measured
using the radio immunity method, the kits were provided by China
Institute of Atomic Energy (Beijing, China), and the measuring tool
was SN-682 γ-calculating instrument produced by Shanghai Institute
of Atomic Energy (Shanghai, China).
Adverse reactions such as retention of water and
sodium (eyelid and facial edema, arthritis and carpal tunnel
syndrome), impaired glucose tolerance, benign intracranial
hypertension, hypothyroidism, slipped capital femoral epiphysis,
scoliosis, pigmented nevus, adenoid hypertrophy, hands and feet
become, local swelling and rash, otitis media and male mammary
gland development, and tumors were all under detection.
Statistical analysis. SPSS 19.0 statistical software
(Chicago, IL, USA) was used for statistical input and analysis, and
data were expressed as mean ± standard deviation. Comparisons
within the group were made by the paired t-test, comparisons
between groups were made by the independent sample t-test, and
comparisons of different time-points were made by repeated measure
variance. Qualitative data were expressed as cases or percentage
(%), and comparisons between groups were made using χ2
test. Quantitative data were analyzed using Pearson. P<0.05 was
statistically significant.
Results
Comparison of the observation index
among the two groups of children
For children in the GHD group, their height, BA, GH
peak, IGF-1 and IGFBP-3 all increased after treatment, and the
differences were statistically significant (P<0.05), but no
obvious change in FT3, FT4 and TSH was observed/obtained
(P>0.05). For children In the ISS group, their height and BA
increased after treatment, but no obvious change in other indexes.
There was no obvious change in the height, BA, FT3, FT4 or TSH of
the ISS group and GHD group before and after treatment, GH peaks of
the ISS group before and after treatment were higher than those of
the GHD group; before treatment, IGF-1 and IGFBP-3 were higher than
those of the GHD group, but no difference after treatment (Table I).
 | Table I.Comparison of observation index among
the two groups of children. |
Table I.
Comparison of observation index among
the two groups of children.
|
| GHD group | ISS group |
|---|
|
|
|
|
|---|
| Observation
index | Before treatment | 5 years
follow-up | t-test | P-value | Before treatment | 5 years
follow-up | t-test | P-value |
|---|
| Height (cm) |
106.0±2.5 |
142.6±3.3 | 23.624 | <0.001 |
103.2±2.4a |
139.8±3.5a | 20.513 | <0.001 |
| BA (years) |
5.0±1.3 |
9.4±1.6 | 12.625 | <0.001 |
4.9±1.4a |
9.2±1.5a | 11.528 | <0.001 |
| GH peak (ng/ml) |
5.6±1.3 |
7.7±1.6 | 6.625 | 0.022 |
12.4±3.3b |
12.5±3.2b | 0.724 | 0.532 |
| IGF-1 (ng/ml) |
156.2±72.7 |
325.2±93.3 | 35.212 | <0.001 |
284.5±69.2b |
312.4±72.1a | 1.230 | 0.965 |
| IGFBP-3 (µg/ml) |
3.0±1.1 |
3.8±1.2 | 7.541 | 0.013 |
3.5±1.4b |
3.6±1.2a | 0.636 | 0.825 |
| FT3 (pmol/l) |
5.2±1.3 |
5.3±1.4 | 0.628 | 0.426 |
5.1±1.2a |
5.0±1.1a | 0.323 | 0.421 |
| FT4 (pmol/l) |
16.2±2.5 |
16.5±2.4 | 0.936 | 0.864 |
16.3±2.3a |
16.4±2.5a | 0.627 | 0.539 |
| TSH (µIU/ml) |
3.2±0.8 |
3.1±0.7 | 0.328 | 0.427 |
3.2±0.6a |
3.3±0.5a | 0.392 | 0.214 |
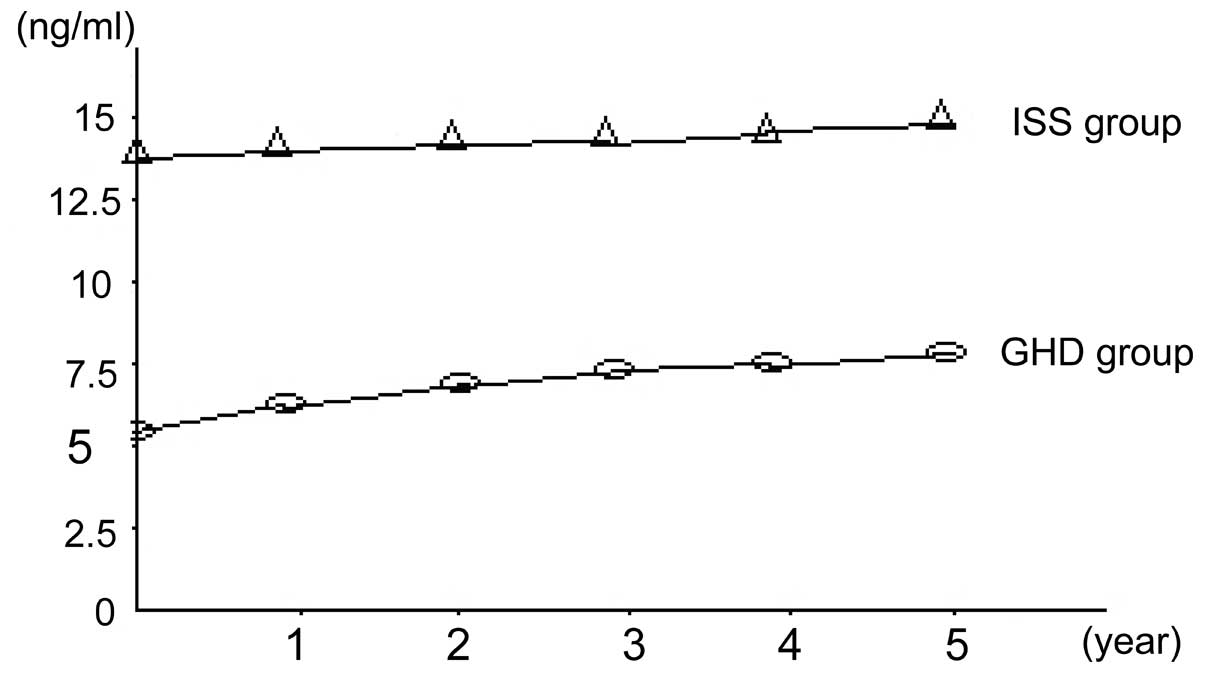
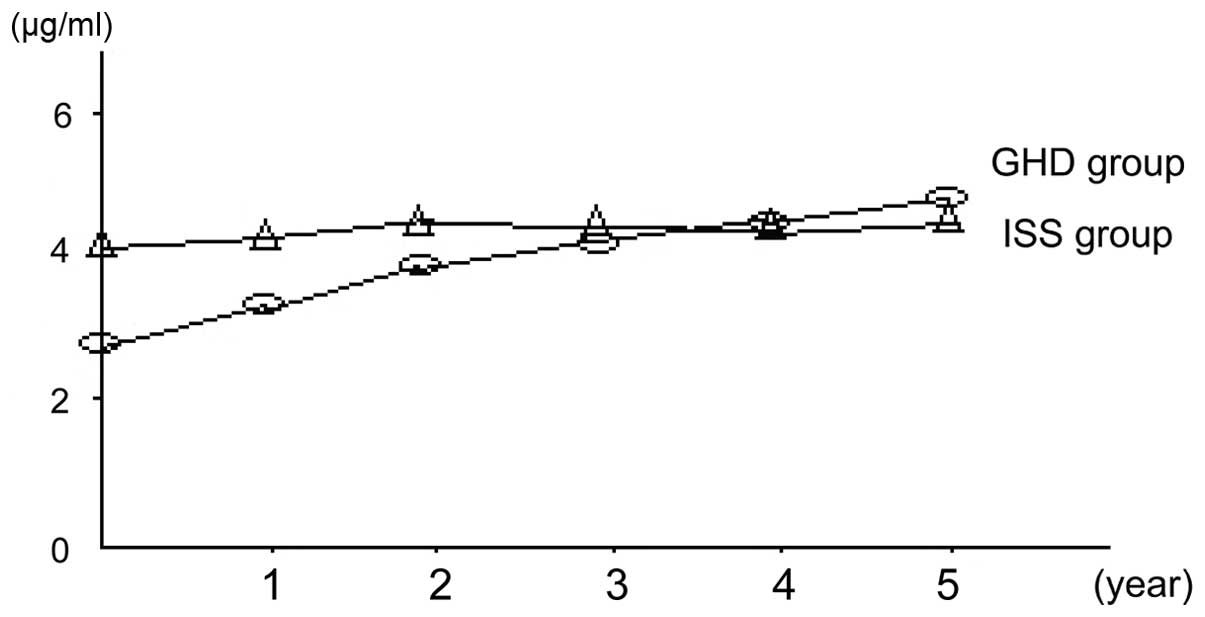
Comparison of GH peak, IGF-1 and
IGFBP-3 of the two groups at different time-points
Comparison of GH peak, IGF-1 and IGFBP-3 of the GHD
group at different time-points suggested that the differences were
statistically significant (P<0.05). A comparison of the ISS
group suggested the differences were not statistically significant
(Figs. 1–3).
Relevant analysis
Analysis on the relationship between the GH peak,
IGF-1, IGFBP-3, FT3, FT4, TSH and height and BA was made, and the
results showed that, the GH peak, IGF-1, IGFBP-3 of the GHD group
was positively correlated with height (r=0.326, P=0.030; r=0.357,
P=0.026; r=0.040, P=0.022), but was not associated with BA
(P<0.05). The above indexes of the ISS group had no obvious
relationship with height and BA (P<0.05).
Discussion
The innovation of the present study was that it
compared separately the effects of rhGH on the height and BA of the
GHD children and the ISS children. It also analyzed the variation
trends of GH peak, IGF-1, IGFBP-3, FT3, FT4 and TSH. The average
follow-up lasted for 5 years, in the course of which no obvious
complication was found and the drug was used continually after
symptomatic treatment, which showed that proper dose of rhGH was
safe. At the same time, the medication time was long, and 90% of
the children continued to use the drug after the follow-up
observation.
The study showed that, for children in the GHD
group, their height, BA, GH peak, IGF-1 and IGFBP-3 all increased
after treatment, and the differences were statistically significant
(P<0.05), but no obvious change was observed in FT3, FT4 and TSH
(P>0.05). For children belonging to the ISS group, their height
and BA increased after treatment, but no obvious change was
observed in other indexes. There was no obvious change in the
height, BA, FT3, FT4 or TSH of the ISS and GHD groups before or
after treatment. The GH peaks of the ISS group before and after
treatment were higher than those of the GHD group, where before
treatment, IGF-1 and IGFBP-3 were higher than those of the GHD
group, but no difference was observed after treatment. rhGH may act
on GHD and ISS by promoting linear growth and bone growth. It was
previously shown that rhGH had a good effect on ISS by promoting
linear growth, and GH-IGH-1 axis played an important role (11,12). GH
promoted tissues outside the skeletal system, especially the liver
to produce IGF-1, which entered the target organs to exert the
endocrine function, thus mediating the growth-promoting effect of
GH (13,14). GH had s direct influence on the
target cells as it could promote the differentiation of the
anterior chondrocytes into chondrocytes, stimulate synthesis and
secretion of IGF-1 in certain parts of the body. Furthermore, IGF-1
could promote the chondrocyte proliferation in an autocrine and
paracrine manner and stimulate the liver to produce IGF-1 and
IGFBP-3, IGFBP-3 in circulation, which regulated the biological
availability of IGF-1 in the target cells (15). However, previous studies showed that
the BA maturity promotion effect of rhGH was limited (16,17). The
reason may be concerned with the time of treatment and follow-up;
however, the specific mechanism remains to be further analyzed. ISS
is a diagnosis of exclusion, i.e., it is in reality a combination
of a group of unknown dwarfisms. With the development of the gene
detection technique, more ISS children were found to be defected in
hypothalamus-pituitary insulin-like growth factor axis function,
which may be one of the effective theories of treating ISS with
rhGH (18). At the same time, it was
identified that the GH peak, IGF-1 and IGFBP-3 had no significant
change before and after treatment. Therefore it was considered that
GH-IGF-1 axis may not play a major role in the pathogenesis. The
study also found that the ISS children may suffer a defect of
growth hormone because the protein binding level of their serum GH
decreased (19). Mutation or
abnormal signal transmission of the GH receptor may cause part
insensitivity of GH and the gene-like SHOX was also reported to
have the same effect.
A comparison of the GH peak, IGF-1 and IGFBP-3 of
the GHD group at different time points suggested the differences
were statistically significant. The Pearson relevant analysis
revealed that the GH peak, IGF-1 and IGFBP-3 of the GHD group were
positively correlated with height, while no relationship with BA
was identified. The above indexes of the ISS group had no obvious
relationship with height or BA. It was suggested that the height
promotion effect of rhGH treatment was related to GH peak, IGF-1
and IGFBP-3. Thus, regular monitoring rhGH may be useful in the
treatment effect evaluation. In conclusion, rhGH was effective for
GHD and ISS, and the GHD effect was positively associated with the
GH peak, IGF-1 and IGFBP-3. ISS had no obvious relationship with
the GH peak, IGF-1 and IGFBP-3; however, other influencing factors
may be involved.
References
|
1
|
Iglesias P and Díez JJ: Clinical
applications of recombinant human growth hormone in adults. Expert
Opin Pharmacother. 1:97–107. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sassolas G: Potential therapeutic
applications of growth hormone in adults. Horm Res. 42:72–78. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wilson TA, Rose SR, Cohen P, Rogol AD,
Backeljauw P, Brown R, Hardin DS, Kemp SF, Lawson M, Radovick S, et
al: Lawson Wilkins Pediatric Endocrinology Society Drug and
Therapeutics Committee: Update of guidelines for the use of growth
hormone in children: The Lawson Wilkins Pediatric Endocrinology
Society Drug and Therapeutics Committee. J Pediatr. 143:415–421.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Growth Hormone Research Society; GH
Research Society, . Consensus guidelines for the diagnosis and
treatment of growth hormone (GH) deficiency in childhood and
adolescence: summary statement of the GH Research Society. J Clin
Endocrinol Metab. 85:3990–3993. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gharib H, Cook DM, Saenger PH, Bengtsson
BA, Feld S, Nippoldt TB, Rodbard HW, Seibel JA, Vance ML and
Zimmerman D: American Association of Clinical Endocrinologists
Growth Hormone Task Force: American Association of Clinical
Endocrinologists medical guidelines for clinical practice for
growth hormone use in adults and children - 2003 update. Endocr
Pract. 9:64–76. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Teran E, Chesner J and Rapaport R: Growth
and growth hormone: an overview. Growth Horm IGF Res. 28:3–5. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Albertsson-Wikland K: Growth hormone
therapy needs to be tailored based on individual responsiveness in
children with idiopathic short stature. J Pediatr. 159:5162011.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liu Z, Mohan S and Yakar S: Does the
GH/IGF-1 axis contribute to skeletal sexual dimorphism? Evidence
from mouse studies. Growth Horm IGF Res. 27:7–17. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hawkes CP and Grimberg A: Insulin-like
growth factor-I is a marker for the nutritional state. Pediatr
Endocrinol Rev. 13:499–511. 2015.PubMed/NCBI
|
|
10
|
Gaspari L, Paris F, Leboucq N, Bonafé A
and Sultan C: Reversible growth failure and complete GH deficiency
in a 4-year-old girl with very early Hashimoto's thyroiditis and
subsequent hyperplasia of pituitary thyrotroph cells. Eur J Pediat.
Feb 2–2016.(Epub ahead of print). View Article : Google Scholar
|
|
11
|
Inzaghi E and Cianfarani S: The challenge
of growth hormone deficiency diagnosis and treatment during the
transition from puberty into adulthood. Front Endocrinol
(Lausanne). 4:342013.PubMed/NCBI
|
|
12
|
Cook DM, Yuen KC, Biller BM, Kemp SF and
Vance ML: American Association of Clinical Endocrinologists:
American Association of Clinical Endocrinologists medical
guidelines for clinical practice for growth hormone use in growth
hormone-deficient adults and transition patients - 2009 update:
executive summary of recommendations. Endocr Pract. 15:580–586.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ho KK: 2007 GH Deficiency Consensus
Workshop Participants: Consensus guidelines for the diagnosis and
treatment of adults with GH deficiency II: a statement of the GH
Research Society in association with the European Society for
Pediatric Endocrinology, Lawson Wilkins Society, European Society
of Endocrinology, Japan Endocrine Society, and Endocrine Society of
Australia. Eur J Endocrinol. 157:695–700. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Molitch ME, Clemmons DR, Malozowski S,
Merriam GR and Vance ML: Endocrine Society: Evaluation and
treatment of adult growth hormone deficiency: an Endocrine Society
clinical practice guideline. J Clin Endocrinol Metab. 96:1587–1609.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Clayton PE, Cuneo RC, Juul A, Monson JP,
Shalet SM and Tauber M: European Society of Paediatric
Endocrinology: Consensus statement on the management of the
GH-treated adolescent in the transition to adult care. Eur J
Endocrinol. 152:165–170. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bell J, Parker KL, Swinford RD, Hoffman
AR, Maneatis T and Lippe B: Long-term safety of recombinant human
growth hormone in children. J Clin Endocrinol Metab. 95:167–177.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tritos NA and Klibanski A: Effects of
growth hormone on bone. Prog Mol Biol Transl Sci. 138:193–211.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cohen P, Rogol AD, Deal CL, Saenger P,
Reiter EO, Ross JL, Chernausek SD, Savage MO and Wit JM: 2007 ISS
Consensus Workshop participants: Consensus statement on the
diagnosis and treatment of children with idiopathic short stature:
a summary of the Growth Hormone Research Society, the Lawson
Wilkins Pediatric Endocrine Society, and the European Society for
Paediatric Endocrinology Workshop. J Clin Endocrinol Metab.
93:4210–4217. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Salerno M, Balestrieri B, Matrecano E,
Officioso A, Rosenfeld RG, Di Maio S, Fimiani G, Ursini MV and
Pignata C: Abnormal GH receptor signaling in children with
idiopathic short stature. J Clin Endocrinol Metab. 86:3882–3888.
2001. View Article : Google Scholar : PubMed/NCBI
|