Introduction
Primary aldosteronism (PA) is a disorder typically
characterized by resistant hypertension, hypokalemia and metabolic
alkaosis, associated with suppressed plasma renin activity and
excessive aldosterone production (1). It is among the most common causes of
secondary hypertension; PA is reported to account for 5–13% of
patients with secondary hypertension (2). Aldosterone-producing adenoma and
bilateral adrenal hyperplasia are the two most prevalent causes of
primary aldosteronism (3). The
majority of patients present with typical features and are easily
diagnosed. However, patients with atypical symptoms may present a
challenge of diagnosis and treatment. Although many cases with PA
do have hypokalemia (>50%), patients with PA associated with
hypokalemic myopathy are rare (1).
Kotsaftis et al (4) reported
a rare case of hypokalemia-induced myopathy as the first
manifestation of primary hyperaldosteronism due to unilateral
adrenal hyperplasia. In addition, Goto et al (5) reported a case of PA associated with
severe rhabdomyolysis due to profound hypokalemia.
In the present study, a case of PA is described who
presented at hospital with prominently hypokalemic myopathy (HM)
simulating polymyositis (PM). The patient provided informed consent
for the publication of this case report.
Case report
A 44-year-old Chinese woman visited the emergency
department of Lishui Hospital of Zhejiang University (Lishui,
China) in July 2013 with weakness in the lower extremity and
difficulty walking for 2 days. Serum creatine kinase (CK) was 2,373
IU/l (normal, 30–135 IU/l) and serum potassium was 1.53 mmol/l
(normal, 3.60–5.00 mmol/l). The patient was admitted for suspected
PM. The patient had a history of hypertension for 9 years, with a
highest recorded blood pressure of 160/100 mmHg, and had been
treated with antihypertensive agents; captopril and indapamide had
been administered in the previous 15 months. The patient's blood
pressure was maintained at 130–140/80–90 mmHg on admission to the
emergency department. Recurrent episodes of limb muscle weakness
had been experienced for the previous year, but the patient did not
see a doctor. The patient had diarrhea for a number of days prior
to admission. Physical examination revealed that her blood pressure
was 128/78 mmHg and her pulse rate was 68 beats per minute. No rash
was observed and the thyroid gland was not enlarged. Respiratory
and cardiovascular examinations were normal. Abdominal examination
was unremarkable. The liver and spleen were not palpable. Muscle
power was grade 3/5 over proximal and grade 4/5 for distal muscle
groups in all four limbs. Sensory testing was normal. Knee reflex
was diminished and plantar response was downward.
Laboratory investigations revealed abnormally high
CK 10,767 IU/l (normal, 22–430 IU/l), increasing gradually to
17,291 IU/l, potassium 2.11 mmol/l (after potassium supplement;
normal, 3.50–5.60 mmol/l), sodium 139.3 mmol/l, chloride 102.6
mmol/l, magnesium 0.65 mmol/l, calcium 2.35 mmol/l and
CO2 23.3 mmol/l. Urinalysis revealed pH 7.5, blood +++
and protein +++. Complete blood count, erythrocyte sedimentation
rate, blood urea nitrogen, creatinine, glucose, total protein,
albumin and thyroid hormones were normal. Autoantibody profiles
included antinuclear antibody, anti-extractable nuclear antigen
antibodies, anti-double stranded DNA antibodies, and complement,
immunoglobulins and rheumatoid factor were normal.
Electrocardiography showed sinus rhythm, flat T waves in all leads
and obvious U waves. Chest radiographs were normal. B-mode
ultrasonography of bilateral kidneys detected no abnormalities.
Electromyography (EMG) confirmed myogenic damage.
The patient was treated with a 3-day course of 0.5
g/day methylprednisolone (Pfizer, Inc., New York, NY, USA) since
the presence of PM was suspected. As the possibility of
drug-induced hypokalemia, which could be deteriorated by diarrhea,
was also considered, the administration of indapamide was
discontinued at the time of admission. Treatment was initiated by
oral and intravenous supplementation of potassium (9 g/day
potassium chloride). After 3 days of treatment, muscle weakness
improved markedly and blood testing revealed CK 7,336 IU/l and
potassium 2.52 mmol/l. This treatment course was not consistent
with PM, and the hypokalemia persisted in spite of high dose
supplementation of potassium. Considering the presence of
concomitant hypertension and hypokalemia, it was agreed that the
patient was more likely to have PA which prominently characterized
HM rather than PM. Steroid use was then discontinued. Further
evaluation revealed elevated urinary potassium excretion (45.2
mmol/l), suppressed plasma renin activity (<0.1 ng/ml/h; normal,
0.1–2.0 ng/ml/h), excessive aldosterone production (26.6 ng/dl;
normal, 3.6–24.0 ng/dl) and extremely high aldosterone-to-renin
ratio (>266 ng/dl per ng/ml/h; normal, <30 ng/dl per
ng/ml/h). The increase in serum aldosterone concentration was
<30% after 2 h of standing in the posture test (before vs.
after). Adrenocortical functions were normal. Metanephrine and
normetadrenaline were in the normal range.
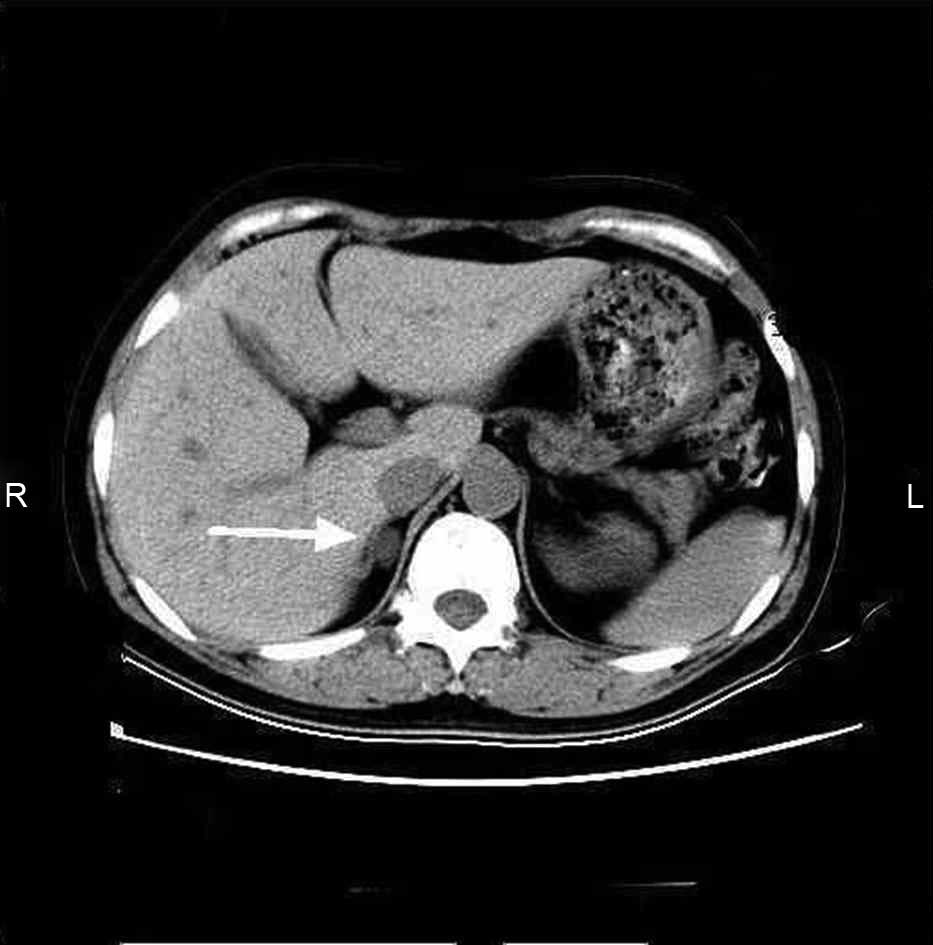
Contrast enhanced computed tomography scan of
bilateral adrenal glands showed a 1.8×1.0-cm adenoma in the right
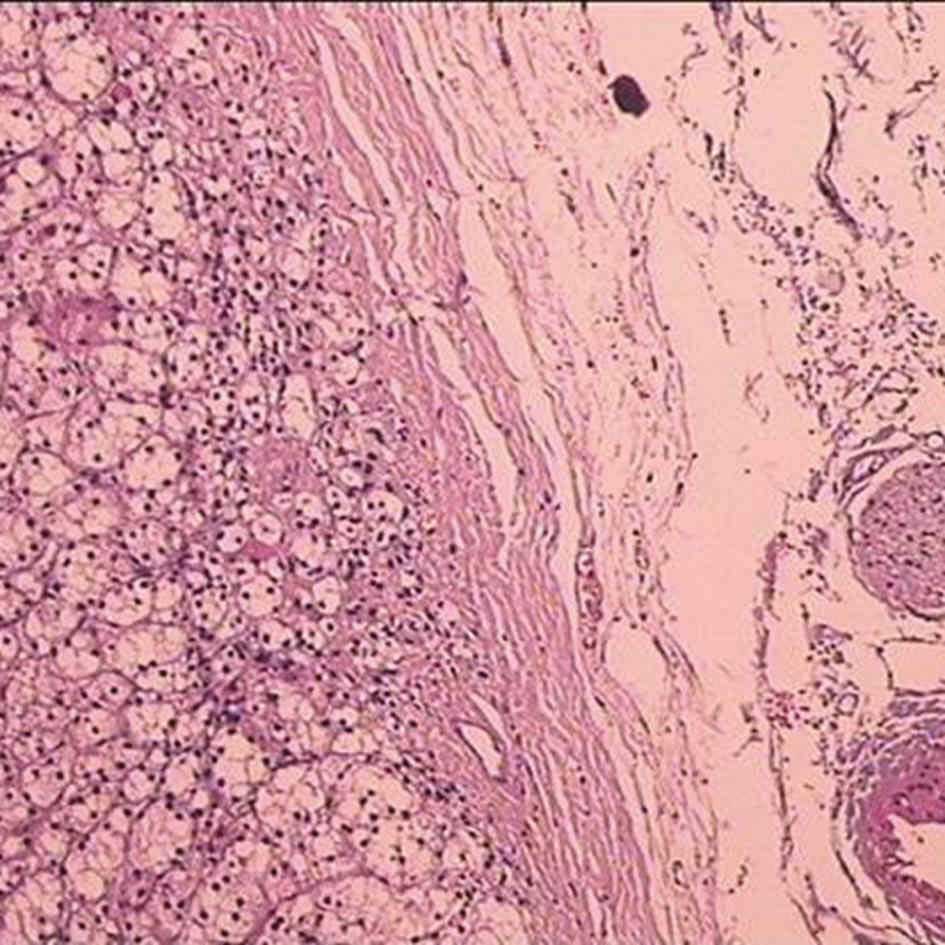
adrenal area (Fig. 1). Following
surgical removal of the adenoma, neoplastic tissue was fixed with
neutral formalin prior to paraffin embedding. The paraffin blocks
were cut into 3-µm sections, and stained with hematoxylin and
eosin. The pathology report confirmed adrenocortical adenoma
(Fig. 2). Following surgery, the
patient's symptoms were resolved. The serum tests and blood
pressure returned to and remained normal (serum potassium, 4.85
mmol/l; and CK, 93 IU/l) without any drugs. The patient reported no
recurrence of the symptoms during the 8-month follow-up.
Discussion
Resistant hypertension and hypokalemia are the most
common symptoms of PA. In special cases, severe skeletal muscle
injury may be complicated and HM may occur (2,5,6). PA prominently characterized by HM is
often misdiagnosed as PM in clinical practice because patients with
PA who have severe skeletal muscle injury and significantly
increased muscle enzyme levels are very rarely encountered by
clinicians (2). PM refers to
nonsuppurative inflammation of striated muscle due to an autoimmune
cause, which is characterized by symmetric proximal muscle
weakness, myalgia, elevated serum muscle enzymes, myogenic damage
on EMG, and varying degrees of muscle inflammation and destruction
confirmed pathologically (7).
The histopathological findings of HM typically
include muscle fiber necrosis, vacuolar changes, and inflammatory
cell infiltration and regeneration (6). It is difficult to distinguish between
HM and PM histopathologically because of similar histopathological
features. Vacuolar changes, which are rarely seen in PM, bear
importance in differential diagnosis of these two conditions.
However, in a previous study, vacuolar changes were not also
observed in patients with HM who underwent muscle biopsy (2). Thus, HM and PM share similar clinical
and histological characteristics and cannot be differentiated by
determination of muscle enzymes, myoglobins, or EMG findings, or by
histopathological evaluation alone. Nevertheless, there are marked
differences between HM and PM. HM may be accompanied by profound
hypokalemia, while PM is not associated with serum potassium
levels, but due to an autoimmune cause (8). Patients with HM may achieve rapid and
complete improvement following the correction of serum potassium to
normal levels and etiology-specific interventions, and are far less
likely to experience recurrence, whereas patients with PM may
require long-term use of steroids to become stable and are more
prone to recurrence (9).
In the present study, the patient had been diagnosed
as having essential hypertension since the age of 35, and had
recurrent episodes of limb muscle weakness following treatment with
indapamide. Although the record of basic serum potassium level was
not acquired, we assume the initiation of the diuretic aggravated
the hypokalemia, eventually causing severe HM.
The cause of hypokalemia-induced myopathy in PA is
obscure, but a number of reports suggest that the enhanced muscle
sodium-potassium pump activity in patients with PA may result in an
increase of potassium entry into the cells (4,6,10). The potassium ion is considered to be
a major factor mediating the rise of muscle blood flow. When serum
potassium level is decreased to below 2.0 mmol/l, a patient with PA
may have marked elevation of serum muscle enzymes. In such a case,
histological findings include diffuse necrosis and vacuolization of
muscle fibers in damaged muscle under light microscopy, and
complete dissolution of myofilaments with the disappearance of
sarcoplasmic reticulum and T-tubules in the necrotic muscle fibers
under electron microscopy. It has been reported that PA associated
with hypokalemia-induced rhabdomyolysis or hypokalemic paralysis
may be more common in Asian populations (10).
HM and PM are both established causes of myopathy
that may be easily confused because of similar presentations.
Hypokalemia should be considered in the specific and differential
diagnosis of both myopathies. Special care should be taken in the
diagnosis of PM. When typical signs of PM and profound hypokalemia
are concurrently present, HM should be considered. Concomitant
hypertension strongly suggests PA-induced HM. The present case
serves to highlight the need for physicians to be aware of the risk
of hypokalemia-induced HM among patients, particularly in Asian
patients, with PA.
References
|
1
|
Funder JW, Carey RM, Fardella C,
Gomez-Sanchez CE, Mantero F, Stowasser M, Young WF Jr and Montori
VM: Endocrine Society: Case detection, diagnosis, and treatment of
patients with primary aldosteronism: An Endocrine Society clinical
practice guideline. J Clin Endocrinol Metab. 93:3266–3281. 2009.
View Article : Google Scholar
|
|
2
|
Tang YC, Wang SK and Yuan WL: Primary
aldosteronism simulating polymyositis. J Rheumatol. 38:1529–1533.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Funder JW, Carey RM, Mantero F, Murad MH,
Reincke M, Shibata H, Stowasser M and Young WF Jr: The management
of primary aldosteronism: Case detection, diagnosis, and treatment:
An Endocrine Society clinical practice guideline. J Clin Endocrinol
Metabol. 101:1889–1916. 2016. View Article : Google Scholar
|
|
4
|
Kotsaftis P, Savopoulos C, Agapakis D,
Ntaios G, Tzioufa V, Papadopoulos V, Fahantidis E and Hatzitolios
A: Hypokalemia induced myopathy as first manifestation of primary
hyperaldosteronism - an elderly patient with unilateral adrenal
hyperplasia: A case report. Cases J. 2:68132009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Goto A, Takahashi Y, Kishimoto M, Minowada
S, Aibe H, Hasuo K, Kajio H and Noda M: Primary aldosteronism
associated with severe rhabdomyolysis due to profound hypokalemia.
Intern Med. 48:219–223. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Becker NJ, Hinman M, Giles MN, Kepes JJ
and Abdou NI: Polymyositis with hypokalemia: Correction with
potassium replacement in the absence of steroids. J Rheumatol.
14:1042–1044. 1987.PubMed/NCBI
|
|
7
|
Sugawara H, Shiraiwa H, Otsuka M and Ueki
A: A case of primary aldosteronism presenting hypokalemic myopathy
induced by benidipine hydrochloride; a dihydropyridine calcium
channel blocker. Rinsho Shinkeigaku. 40:446–451. 2000.(In
Japanese). PubMed/NCBI
|
|
8
|
Atluri RB: Inflammatory myopathies. Mo
Med. 113:127–130. 2016.PubMed/NCBI
|
|
9
|
Hiraga A, Kamitsukasa I, Kojima K and
Kuwabara S: Clinical features and recovery patterns of acquired
non-thyrotoxic hypokalemic paralysis. J Neurol Sci. 313:42–45.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ma JT, Wang C, Lam KS, Yeung RT, Chan FL,
Boey J, Cheung PS, Coghlan JP, Scoggins BA and Stockigt JR: Fifty
cases of primary hyperaldosteronism in Hong Kong Chinese with a
high frequency of periodic paralysis. Evaluation of techniques for
tumour localisation. Q J Med. 61:1021–1037. 1986.PubMed/NCBI
|