Introduction
Colorectal cancer (CRC) is commonly observed in
clinical settings (1). To improve
the prognosis in patients with CRC, prompt and accurate diagnosis
is essential. Screening for CRC is performed using fecal occult
blood testing, and is diagnosed with colonoscopy (2).
Abdominal ultrasound (US) is useful for the safe and
easy diagnosis of patients (3–6). During
US screening of the abdomen, CRC is sometimes encountered (7). A thickened colonic wall has been
reported as a criteria for the diagnosis of CRC (8). Changes in stratification and contour
illustrated with abdominal US are associated with the depth of
invasion, in either the subserosa or the extra subserosa (7).
Contrast-enhanced ultrasonography (CEUS) enables the
evaluation of tissue vascularity with low blood flow velocity
(9). Primary or metastatic liver
tumors are the most common indication examined by CEUS (10,11).
Regarding the alimentary tract, guidelines put forth by the
European Federation of Societies for Ultrasound in Medicine and
Biology recommend use of CEUS in inflammatory bowel disease for
diagnosis, activity assessment, and examining complications such as
stenosis or fistula (9). In
addition, CEUS is useful for the diagnosis of gastrointestinal
bleeding (12).
Sonazoid™ consists of perfluorocarbon microbubbles
with a median diameter ≤3 mm, which are stable during examination
and act as a strong contrast agent (13). Sonazoid™ is primarily used for the
management of hepatocellular carcinoma, while no reports yet exist
regarding the use of Sonazoid™ in CRC (14,15).
In the present study, we analyzed CEUS images using
Sonazoid™ to examine its usefulness in the diagnosis of CRC. Blood
vessel density was compared between tumorous areas and non-tumorous
areas and supplemented by immunostaining for cluster of
differentiation (CD)31, a pan-endothelial cell marker (16).
Materials and methods
Patients
Between August 2011 and May 2015, 13 patients were
diagnosed with CRC using US screening at the National Hospital
Organization Shimoshizu Hospital (Yotuskaido, Japan). Of those,
three patients were subjected to CEUS with Sonazoid™ to examine for
liver metastasis. In all cases, CRC was observed prior to
examination for liver metastasis. The study was approved by the
National Hospital Organization Shimoshizu Hospital Ethics
Committee, and written informed consent was obtained from all three
patients. All procedures followed were in accordance with ethical
standards put forth by the responsible institutional and national
committees on human experimentation, and with the Helsinki
Declaration of 1964 and later versions. Patient characteristics are
listed in Table I. Clinical
parameters analyzed by blood tests were white blood cell count,
hemoglobin, C-reactive protein, carcinoembryonic antigen and
carbohydrate antigen 19-9.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
|
| Normal range | Patient 1 | Patient 2 | Patient 3 |
|---|
| Age |
| 74 | 73 | 84 |
| Gender |
| Male | Female | Female |
| Location |
| Sigmoid | Ascending | Ascending |
| Pathology |
| Moderate | Well | Well |
| Size (cm) |
| 3.7 | 5.5 | 5.5 |
| Depth |
| pSS | pSS | pSS |
| WBC, /µl | 3500–8500 | 19000 | 5200 | 4400 |
| Hb, g/dl | 13.5–17.0 | 13.7 | 6.4 | 5.9 |
| CRP, mg/dl | 0.00–0.30 | 2.8 | 0.17 | 0.16 |
| CEA, ng/ml | 0.0–5.0 | 44.2 | 2.9 | 48.4 |
| CA19-9, U/ml |
0.0–37.0 | 47.3 | 7.6 | 27.3 |
Patients two and three consented to further
investigation, and agreed to provide surgical specimens for
analysis.
Abdominal US and administration of
Sonazoid™
Abdominal US was performed by Senior Fellows of the
Japan Society of Ultrasonics in Medicine using a SSA-700A US system
(Toshiba Medical Systems Corporation, Ohtawara, Japan) with a
3.75-MHz curved-array probe (PVT-375BT; Toshiba Medial Systems
Corporation) or an 8.0-MHz linear-array probe (PLT-805AT; Toshiba
Medical Systems Corporation). Sonazoid™ (Daiichi Sankyo Co., Ltd.,
Tokyo, Japan) was administered intravenously at 0.015 ml/kg
following the manufacturer's instruction.
Criteria for the diagnosis of CRC
The diagnostic criteria for CRC used were localized
irregular wall thickening or a hypoechoic mass mixed with
hyperechoic lesions (a pseudokidney sign) (8). The former is a common finding in
patients with CRC (17), and the
latter represents tumor tissue with air in the residual lumen
(18).
Pathological analysis and
immunostaining
The depth of invasion by the CRC was determined by
pathologists analyzing specimens obtained via surgical resection,
using standard histological methods. Immunostaining proceeded as
follows. Serial sections were cut from formalin-fixed
paraffin-embedded surgical samples. The sections were
deparaffinized, and autoclaved in 0.05 M citrate buffer at pH 6.0.
Endogenous peroxidase was inactivated by incubating with 0.1%
hydrogen peroxide in 100% methanol for 30 min at 4°C. To prevent
non-specific antibody binding, the sections were incubated with 2%
normal goat serum (Cappel, Aurora, OH, USA) in phosphate-buffered
saline for 30 min at 4°C. Staining for CD31 was used as a marker of
vascular endothelial cells (19).
After a 4°C overnight incubation with mouse anti-human CD31
antibody at a 1:100 dilution (3528S; Cell Signaling Technology,
Inc., Danvers, MA, USA), sections were incubated at 4°C for 2 h
with alkaline phosphatase-labeled goat anti-mouse IgG with a
1:1,000 dilution (S3721; Promega Corporation, Madison, WI, USA).
Subsequently, Vector Red Substrate (Vector Laboratories, Inc.,
Burlingame, CA, USA) was applied to the sections as a chromogen.
The nuclei were counterstained with hematoxylin (Muto Pure
Chemicals Co., Ltd., Tokyo, Japan) for 10 sec. Specimens were
observed and photographed under an AX80 microscope (Olympus
Corporation, Tokyo, Japan). To determine blood vessel density, the
number of blood vessels staining positive with CD31 were counted
per field at ×400 magnification under the microscope. The number of
positive blood vessels across five fields for each patient was
examined and the average determined.
Statistical analysis
Blood vessel densities were compared between
tumorous areas and corresponding non-tumorous areas by using a
one-factor analysis of variance. Statistical analysis was performed
using JMP 10.0.2 software (SAS Institute, Cary, NC, USA). P<0.05
was considered to indicate a statistically significant
difference.
Results
Contrast-enhanced ultrasonography of
colorectal cancer
Prior to the administration of Sonazoid™, a
thickened colonic wall with an irregular shape was observed in
patients one, two and three, as shown in Fig. 1A-C, respectively. One minute after
administration, most of the thickened wall was enhanced in patients
one, two and three, as shown in Fig.
1D-F, respectively, with some parts of the thickened wall
remaining unenhanced (indicated by arrows). Ten minutes after the
administration of Sonazoid™, the enhanced areas of the thickened
wall returned to a hypoechoic state in patients one, two and three,
depicted in Fig. 1G-I, respectively.
The shapes of the unenhanced areas resembled those of tumorous
areas identified in post-surgical samples from patients two
(Fig. 1J) and three (Fig. 1K). These results suggest that areas
remaining unenhanced 1 min after the administration of Sonazoid™
may be tumorous. It might be postulated that the blood vessel
density was lower in tumorous areas compared with surrounding
non-tumorous areas.
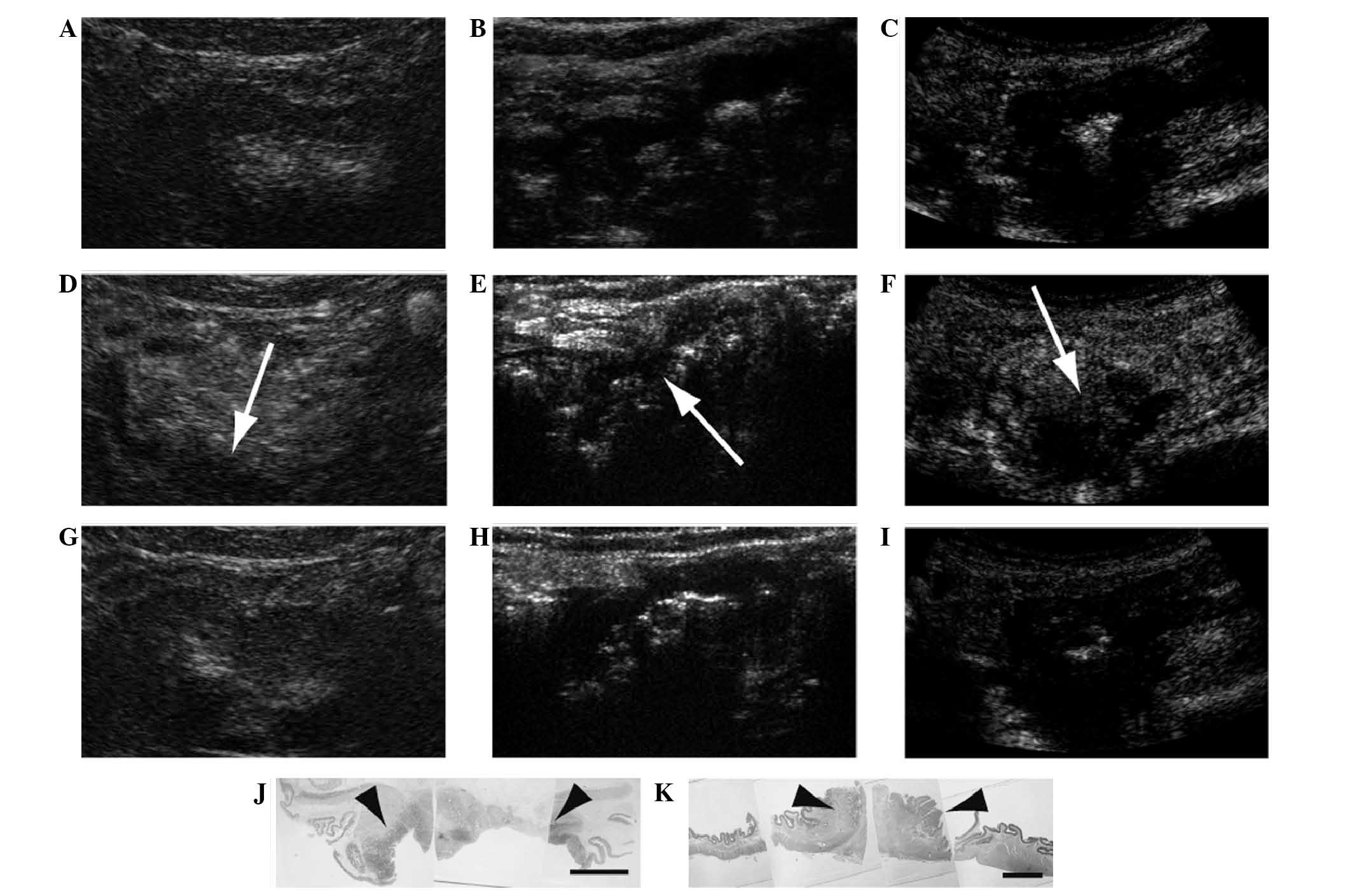 | Figure 1.Contrast-enhanced ultrasonography of
colorectal cancer. (A-C) Colonic wall showing thickening, irregular
shape and low echo, and (D-F) 1 min after and (G-I) 10 min after
administration of Sonazoid™. Patients (A, D, G) one, (B, E, H) two
and (C, F, I) three showed the same enhancement trend. (B, E, H)
The thickened wall was enhanced with Sonazoid™ 1 min after its
administration. (D, E, F) Part of the thickened wall remained
unenhanced (indicated by arrows). (D, F) Shapes of tumorous areas
(indicated by arrowheads) resembled those of the unenhanced areas
in patient (J) two and (K) three. Scale bar, 10 mm. |
Vascular structure of colorectal
cancer
To compare the blood vessel densities between
tumorous areas and the surrounding non-tumorous areas,
immunostaining with an antibody to CD31 was performed. Varieties of
blood vessel sections were observed (Fig. 2A). Specimens remained negative in the
absence of incubation with anti-CD31 antibody (Fig. 2B). All positive signals observed were
thought to be blood vessels. Surgical specimens from patients two
(Fig. 2C and D) and three (Fig. 2E and F) were subjected to anti-CD31
immunostaining. Non-tumorous areas (Fig.
2C and E) exhibited more positive signals compared with
tumorous areas (Fig. 2D and F).
Measurements of blood vessel densities for non-tumorous areas and
tumorous areas in patient two (25.2±2.5 and 5.2±1.1, respectively)
were found to be significantly different (P<0.0001; Fig. 2G). Similarly, measurements of blood
vessel densities for non-tumorous areas compared with tumorous
areas in patient three (19.0±3.1 and 2.2±0.8, respectively) were
found to be significantly different (P<0.0001; Fig. 2H). These results clearly indicate
that blood vessel densities were significantly lower in tumorous
areas compared with non-tumorous areas.
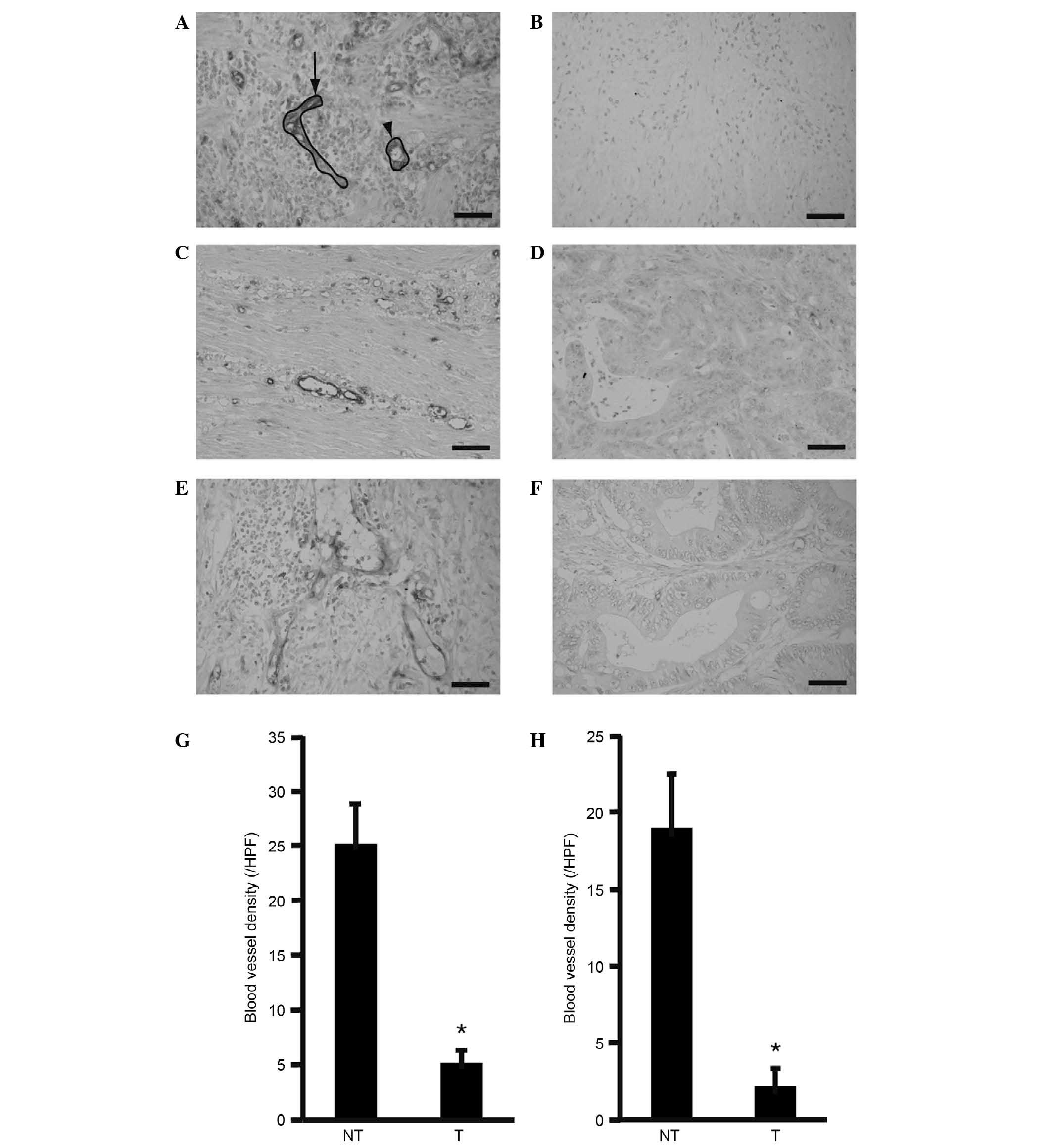 | Figure 2.Blood vessel density in tumorous and
non-tumorous tissues. Surgical specimens were immunostained for
CD31. Longitudinal (arrow) and cross (arrowhead) sections of blood
vessels were observed, and (A) examples outlined. Each section was
counted as one blood vessel. (B) A control section without staining
for CD31 showed no signal. Sections from patients (C, D) two and
(E, F) three were examined. (C, E) Non-tumorous areas exhibited
more blood vessels than (D, F) tumorous areas. The number of blood
vessels was counted in each of five fields at ×400 magnification,
and then averaged to determine the blood vessel density. The blood
vessel density was compared between non-tumorous and tumorous areas
in patients (G) two and (H) three. Original magnification: 400x.
Scale bar, 50 µm. Error bar, standard deviation. *P<0.05 vs. NT.
n=5. CD31, cluster of differentiation 31; HPF, high power field;
NT, non-tumorous; T, tumorous. |
Discussion
During CEUS, non-tumorous areas are enhanced by
using Sonazoid™. In the liver, non-tumorous areas become diffusely
enhanced while liver abscesses and metastases remained unenhanced
(20,21). In the present study, CEUS revealed
enhancement of non-tumorous areas, while CRC tissue remained
unenhanced while using Sonazoid™. Previous studies have shown the
bowel to be diffusely enhanced under examination with CEUS
(22). Tumorous areas of CRC have
been reported to not be enhanced with CEUS (23). The results of previous studies are in
accordance with this previously published literature (20–23).
Previous reports and the results from the present study clearly
suggest that under examination with CEUS using Sonazoid™
non-tumorous areas are enhanced, while tumorous areas remain
unenhanced in CRC. In the present study, vascular structure was not
evaluated. Vascular structure is often irregular in CRC and this
can be evaluated using CEUS (24).
In the present study, blood vessel densities were
found to be lower in tumorous areas as compared with non-tumorous
areas. A number of prior studies have investigated blood vessel
density in tumorous areas (25).
Blood vessel density was demonstrated to not correlate with
histological grade in CRC (26).
Additionally, the number of blood vessels positive for CD31 was
found to be lower in tumorous areas compared with non-tumorous
areas (23). The results of the
present study are consistent with these prior reports, and may be
supported by the fact that intensity of enhancement in CEUS
positively correlates with the density of blood vessels (27).
The use of Sonazoid™ in CEUS may be useful for the
diagnosis of cancers other than primary or metastatic liver tumors.
For example, metastasis has been successfully diagnosed in axillary
lymph nodes of patients with breast cancer using Sonazoid™
(28). Clinical trials are currently
being performed, aiming to differentiate benign and malignant focal
lesions in the breast (29). The
present study shows a possible application for Sonazoid™ in CRC. In
the future, Sonazoid™ may be used for the diagnosis of tumors other
than those in the liver.
One major limitation of this study was that it was
based on a small number of patients. The next step would be to
increase the number of patients under investigation.
In conclusion, during examination by CEUS, tumorous
areas of CRC were not enhanced 1 min after the administration of
Sonazoid™. In addition, blood vessel density was lower in tumorous
areas compared with non-tumorous areas as evidenced by
immunohistochemistry with CD31. These findings suggest that CEUS
may be useful for the determination of the extent of CRC.
References
|
1
|
Brenner H, Kloor M and Pox CP: Colorectal
cancer. Lancet. 383:1490–1502. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Stracci F, Zorzi M and Grazzini G:
Colorectal cancer screening: Tests, strategies, and perspectives.
Front Public Health. 2:2102014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Puylaert JB, van der Zant FM and Rijke AM:
Sonography and the acute abdomen: Practical considerations. AJR Am
J Roentgenol. 168:179–186. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Laméris W, van Randen A, Dijkgraaf MG,
Bossuyt PM, Stoker J and Boermeester MA: Optimization of diagnostic
imaging use in patients with acute abdominal pain (OPTIMA): Design
and rationale. BMC Emerg Med. 7:92007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dhillon S, Halligan S, Goh V, Matravers P,
Chambers A and Remedios D: The therapeutic impact of abdominal
ultrasound in patients with acute abdominal symptoms. Clin Radiol.
57:268–271. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tomizawa M, Shinozaki F, Sugiyama T,
Yamamoto S, Sueishi M and Yoshida T: Ultrasonography for
leukocytosis or elevated C-reactive protein.
Hepatogastroenterology. 58:1156–1158. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tomizawa M, Shinozaki F, Hasegawa R, Fugo
K, Shirai Y, Ichiki N, Sugiyama T, Yamamoto S, Sueishi M and
Yoshida T: Screening ultrasonography is useful for the diagnosis of
gastric and colorectal cancer. Hepatogastroenterology. 60:517–521.
2013.PubMed/NCBI
|
|
8
|
Shirahama M, Koga T, Ishibashi H, Uchida S
and Ohta Y: Sonographic features of colon carcinoma seen with
high-frequency transabdominal ultrasound. J Clin Ultrasound.
22:359–365. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Piscaglia F, Nolsøe C, Dietrich CF,
Cosgrove DO, Gilja OH, Nielsen M Bachmann, Albrecht T, Barozzi L,
Bertolotto M, Catalano O, et al: The EFSUMB guidelines and
recommendations on the clinical practice of contrast enhanced
ultrasound (CEUS): Update 2011 on non-hepatic applications.
Ultraschall Med. 33:33–59. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Claudon M, Dietrich CF, Choi BI, Cosgrove
DO, Kudo M, Nolsøe CP, Piscaglia F, Wilson SR, Barr RG, Chammas MC,
et al: World Federation for Ultrasound in Medicine; European
Federation of Societies for Ultrasound; Guidelines and good
clinical practice recommendations for contrast enhanced ultrasound
(CEUS) in the liver-update 2012: A WFUMB-EFSUMB initiative in
cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and
ICUS. Ultraschall Med. 34:11–29. 2013.PubMed/NCBI
|
|
11
|
Esteban JM, Mollá MA, Tomás C and
Maldonado L: Improved detection of liver metastases with
contrast-enhanced wideband harmonic imaging: Comparison with CT
findings. Eur J Ultrasound. 15:119–126. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ueno N, Kawamura H, Hoshino T, Kadowaki A
and Nakamura K: Detection of alimentary tract hemorrhage on
contrast-enhanced ultrasonography. J Ultrasound Med. 25:683–686.
2006.PubMed/NCBI
|
|
13
|
Marelli C: Preliminary clinical experience
in cardiology with sonazoid. Am J Cardiol. 86:10G–13G. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kudo M, Matsui O, Izumi N, Iijima H,
Kadoya M and Imai Y: Liver Cancer Study Group of Japan:
Surveillance and diagnostic algorithm for hepatocellular carcinoma
proposed by the Liver Cancer Study Group of Japan: 2014 update.
Oncology. 87:(Suppl 1). S7–S21. 2014. View Article : Google Scholar
|
|
15
|
Ikeda K, Osaki Y, Nakanishi H, Nasu A,
Kawamura Y, Jyoko K, Sano T, Sunagozaka H, Uchino K, Minami Y, et
al: Recent progress in radiofrequency ablation therapy for
hepatocellular carcinoma. Oncology. 87:(Suppl 1). S73–S77. 2014.
View Article : Google Scholar
|
|
16
|
Giatromanolaki A, Koukourakis MI, Sivridis
E, Gatter KC, Trarbach T, Folprecht G, Shi MM, Lebwohl D, Jalava T,
Laurent D, et al: Tumour and Angiogenesis Research Group: Vascular
density analysis in colorectal cancer patients treated with
vatalanib (PTK787/ZK222584) in the randomised CONFIRM trials. Br J
Cancer. 107:1044–1050. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Truong M, Atri M, Bret PM, Reinhold C,
Kintzen G, Thibodeau M, Aldis AE and Chang Y: Sonographic
appearance of benign and malignant conditions of the colon. AJR Am
J Roentgenol. 170:1451–1455. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
O'Malley ME and Wilson SR: US of
gastrointestinal tract abnormalities with CT correlation.
Radiographics. 23:59–72. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sullivan HC, Edgar MA, Cohen C, Kovach CK,
HooKim K and Reid MD: The utility of ERG, CD31 and CD34 in the
cytological diagnosis of angiosarcoma: An analysis of 25 cases. J
Clin Pathol. 68:44–50. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kishina M, Koda M, Tokunaga S, Miyoshi K,
Fujise Y, Kato J, Matono T, Sugihara T and Murawaki Y: Usefulness
of contrast-enhanced ultrasound with Sonazoid for evaluating liver
abscess in comparison with conventional B-mode ultrasound. Hepatol
Res. 45:337–342. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hiraoka A, Kume M, Miyagawa M, Tazuya N,
Ichiryu M, Ochi H, Tanabe A, Nakahara H, Shinbata Y, Kan M, et al:
Diagnostic value of sonazoid for hepatic metastasis: Comparison
with FDG PET/CT. Hepatogastroenterology. 57:1237–1240.
2010.PubMed/NCBI
|
|
22
|
Girlich C, Schacherer D, Jung EM, Klebl F
and Huber E: Comparison between quantitative assessment of bowel
wall vascularization by contrast-enhanced ultrasound and results of
histopathological scoring in ulcerative colitis. Int J Colorectal
Dis. 27:193–198. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pysz MA, Foygel K, Panje CM, Needles A,
Tian L and Willmann JK: Assessment and monitoring tumor vascularity
with contrast-enhanced ultrasound maximum intensity persistence
imaging. Invest Radiol. 46:187–195. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Onji K, Yoshida S, Tanaka S, Takemura Y,
Oka S, Yoshihara M, Yamada H, Okajima M and Chayama K:
Microvascular structure and perfusion imaging of colon cancer by
means of contrast-enhanced ultrasonography. Abdom Imaging.
37:297–303. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang Y, Yao X, Ge J, Hu F and Zhao Y: Can
vascular endothelial growth factor and microvessel density be used
as prognostic biomarkers for colorectal cancer? A systematic review
and meta-analysis. Scientific World Journal.
2014:1027362014.PubMed/NCBI
|
|
26
|
Sun H, Xu Y, Yang Q and Wang W: Assessment
of tumor grade and angiogenesis in colorectal cancer: Whole-volume
perfusion CT. Acad Radiol. 21:750–757. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wang Y, Li L, Wang YX, Cui NY, Zou SM,
Zhou CW and Jiang YX: Time-intensity curve parameters in rectal
cancer measured using endorectal ultrasonography with sterile
coupling gels filling the rectum: Correlations with tumor
angiogenesis and clinicopathological features. Biomed Res Int.
2014:5878062014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Matsuzawa F, Einama T, Abe H, Suzuki T,
Hamaguchi J, Kaga T, Sato M, Oomura M, Takata Y, Fujibe A, et al:
Accurate diagnosis of axillary lymph node metastasis using
contrast-enhanced ultrasonography with Sonazoid. Mol Clin Oncol.
3:299–302. 2015.PubMed/NCBI
|
|
29
|
Miyamoto Y, Ito T, Takada E, Omoto K,
Hirai T and Moriyasu F: Efficacy of sonazoid (perflubutane) for
contrast-enhanced ultrasound in the differentiation of focal breast
lesions: Phase 3 multicenter clinical trial. AJR Am J Roentgenol.
202:W400–W407. 2014. View Article : Google Scholar : PubMed/NCBI
|














