Introduction
The repair of large segments of defective bone is
frequently necessary in oral, maxillofacial, orthopedic, plastic
and reconstructive surgery (1,2). The
challenges in treating large bone defects lie in designing devices
and biomaterials that are able to foster the bone wound healing
process into the appropriate pathway that leads toward the complete
regeneration of the missing tissue (3). Autologous bone or allografts to repair
large bone defects have significant limitations in terms of
availability, morbidity, efficacy, immunological reactions and
disease transmission (4,5). Tissue engineering is a promising
alternative approach that permits the efficient reconstruction of
bone defects through use of three main components: Multipotent stem
cells, scaffolds to direct tissue development and utilization of
tissue-inducing substances such as growth factors (6).
Among many available sources, mesenchymal stem cells
(MSCs) derived from bone marrow (BMSCs) are typically used as
multipotent autologous cell sources for bone tissue engineering
(7). BMSCs may be collected via
relatively noninvasive methods and provide osteoblasts to support
the process of bone remodeling under physiological conditions
(8). A number of previous studies
have demonstrated the advantages of using MSCs for the regeneration
of bone (9–11). Furthermore, MSCs have been applied
clinically for >10 years (12).
The results of clinical trials have demonstrated the efficacy of
bone tissue engineering using BMSCs, and their clinical use appears
to be relatively safe (12–14).
Scaffolds used for tissue engineering applications
are typically biocompatible and biodegradable, support cell
proliferation and differentiation, and are able to provide
appropriate mechanical support (15). Cell sheet engineering, as a novel
tissue engineering technique, recreates a biological
microenvironment similar to that of a regenerative milieu (16). Without typical proteolytic enzyme or
EDTA treatments, cultured cells are able to be harvested as a
single contiguous cell sheet, retaining cell-cell junctions, as
well as deposited extracellular matrix (ECM) on the basal sheet
surface (17). Many research groups
have reported bone formation or regeneration by the cell sheet
itself (18,19). Synthetic bone substitutes such as
hydroxyapatite (HA), β-tricalcium phosphate and combinations of
these have been used for bone tissue engineering (20,21).
Recent advances in nanoscience and nanotechnology have reignited
interest in the formation of nanosized HA and the study of its
properties on the nanoscale (15).
It has been reported that nanocrystalline hydroxyapatite (nano-HA)
powder exhibited improved mechanical properties and better
bioactivity compared with coarser crystals (22,23).
Based on these findings, composites of cell sheets and nano-HA may
be a suitable candidate material for bone tissue engineering.
Growth factors are also expected to serve a
significant role in bone tissue engineering. Platelet concentrates
have previously been used as a source of growth factors in many
studies of bone regeneration (24–26).
Platelet-rich fibrin (PRF) has been referred to as the
second-generation platelet concentrate, which has been demonstrated
to have several advantages over traditionally prepared
platelet-rich plasma including ease of preparation and no
biochemical handling of blood (27,28). The
autologous origin of PRF does not lead to any risk of immunologic
reaction or transmissible diseases (28). Platelets contain a variety of active
growth factors, which are able to stimulate wound healing and bone
formation (29,30). PRF is defined as a leukocyte-rich and
platelet-rich fibrin biomaterial (31), and it has previously been
hypothesized that leukocytes are able to influence cell reactions
and growth factor release (32).
In the present study, it was hypothesized that a
bone tissue engineering strategy consisting of an MSC sheet,
nano-HA and PRF granules may be able to repair critical-size bone
defects in a rabbit model. This bone graft method, based on tissue
engineering concepts, may reveal novel opportunities for the
clinical treatment of large bone defects.
Materials and methods
Isolation of mesenchymal stem cells
from bone marrow
Animals were anesthetized with an intravenous
injection of 100 mg/kg sodium barbiturate (Sigma-Aldrich; Merck
KGaA, Darmstadt, Germany). Bone marrow was subsequently aspirated
from the hind limb bones under sterile conditions. MSCs were
isolated from the aspirated bone marrow using the Percoll density
gradient centrifugation method (Histopaque-1077; Sigma-Aldrich;
Merck KGaA) and were cultured in α-Minimum Essential Medium (α-MEM;
Gibco; Thermo Fisher Scientific, Inc., Waltham, MA, USA)
supplemented with 10% fetal bovine serum (FBS; Gibco; Thermo Fisher
Scientific, Inc.), 2 mM L-glutamine (Invitrogen; Thermo Fisher
Scientific, Inc.), 100 U/ml penicillin and 100 mg/ml streptomycin
(Gibco; Thermo Fisher Scientific, Inc.) in a humidified atmosphere
containing 5% CO2 at 37°C. The culture medium was
changed twice per week. When MSCs reached 80–90% confluence, they
were trypsinized and re-seeded for further expansion.
Induction of osteogenic
differentiation of MSCs in vitro
In total, 1×105 MSCs were seeded into
each well of 6-well plates and cultured in α-MEM supplemented with
10% FBS, 2 mM L-glutamine, 100 U/ml penicillin and 100 mg/ml
streptomycin in a humidified atmosphere containing 5%
CO2 at 37°C. When cells reached 80% confluence, MSCs
were cultured in α-MEM supplemented with 10% FBS, 2 mM L-glutamine,
100 nM dexamethasone (Sigma-Aldrich; Merck KGaA), 50 µg/ml of
ascorbic acid, and 5 mM β-glycerophosphate (Sigma-Aldrich; Merck
KGaA) to induce osteoblast differentiation. The media were changed
every two days. Alkaline phosphatase (ALP) staining was performed
using a 5-bromo-4-chloro-3-indolyl phosphate/nitro blue tetrazolium
alkaline phosphatase color development kit (Beyotime Institute of
Biotechnology, Haimen, China) following 7 days of culture according
to the manufacturer's protocols. Following 21 days of culture with
the osteogenic supplements, the cells were washed twice PBS
(Beyotime Institute of Biotechnology, Haimen, Jiangsu, China),
fixed in a 70% ethanol solution for 1 h at 37°C, then stained with
Alizarin red to reveal mineralized nodules. Cells were subsequently
washed with PBS, and observed and imaged using an inverted
microscope.
Construction of cell sheets
Cell sheets were prepared as previously reported
(33). To create the cell sheet,
MSCs were seeded at 2.5×104 cells/cm2 in 9-cm
culture plates for subculture at 37°C with 10 nM dexamethasone and
50 µg/ml ascorbic acid until reaching 80% confluence on day 14. The
medium was changed every 2 days.
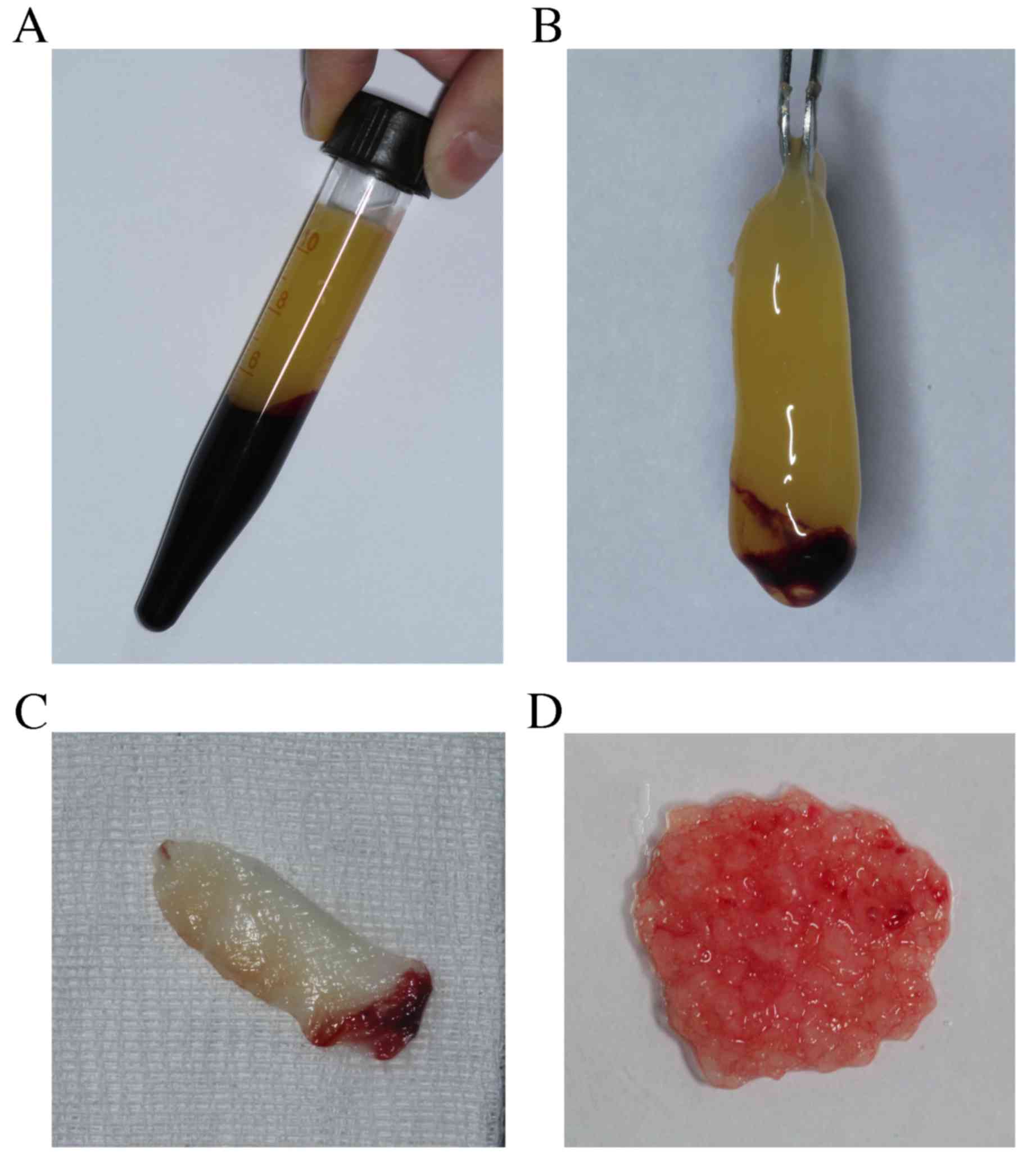
PRF preparation
A total of 10 ml of autologous whole blood was
harvested from the central ear artery of each rabbit. Blood samples
were treated according to the PRF protocol (34). Briefly, the blood sample was
transferred into a 10 ml glass tube without anticoagulants. The
tube was immediately centrifuged at 400 × g for 10 min at room
temperature. A fibrin clot was obtained in the middle of the tube,
which was easily separated from the red corpuscles at the bottom
and the acellular plasma at the top of the tube (Fig. 1A). Following compression with sterile
dry gauze, the fluids trapped in the fibrin matrix were driven out,
and the clot became a very resistant autologous fibrin membrane
(Fig. 1B and C). The obtained
membrane was cut into small granules with sizes of up to 1
mm3 using sterile scissors (Fig. 1D) for the following in vivo
experiment.
Scanning electron microscopy (SEM)
analysis
To identify the ultrastructure of the PRF, the
specimens of PRF membrane were fixed with a solution of 2.5%
glutaraldehyde (Hubei Shengtian Hengchuang Biotechnology Co., Ltd.,
Wuhan, China) at 4°C for 1 h and subsequently dehydrated using
graded ethanol, as previously described (35). Images were captured using SEM
(S-4800; Hitachi, Ltd., Tokyo, Japan).
Animals
A total of 15 male New Zealand rabbits (Zhongchuang
Biotechnology Co., Ltd., Guangzhou, China), aged 3–5 months and
with a mean weight of 3.1 kg, were used in the present study. All
experiments were performed following the guidelines of the Chinese
government for the care and use of laboratory animals (http://scitech.people.com.cn/GB/126054/139095/8378670.html).
All protocols were approved by the Animal Welfare Committee of
Zhengzhou University. The rabbits were housed in a
temperature-controlled room (21–23°C) and maintained under a 12 h
light-dark cycle. Each rabbit was housed in an individual cage and
fed a standard dried diet and water ad libitum. Commercially
available nano-HA powder (Sigma-Aldrich; Merck KGaA) was sterilized
using 60Co irradiation. For ectopic transplantation, 100
mg nano-HA was wrapped in a piece of cell sheet with or without
autologous PRF granules to generate a composite. Rabbits were
randomly divided into three groups: MSC/PRF (n=6), MSC (n=6) and
control groups (n=3). In the MSC/PRF group, defects were repaired
using MSC/PRF composites with 100 mg nano-HA, as mentioned above.
In the MSC group, defects were repaired with the MSC composites,
also with 100 mg nano-HA. In the control group, defects were
untreated.
Surgical procedure
All rabbits were anesthetized with an intravenous
injection of 100 mg/kg sodium barbiturate (Sigma-Aldrich; Merck
KGaA). The surgical region was shaved and aseptically prepared,
with sterile barriers to limit the surgical field. A tongue-shaped
incision was made over the head and the skin, and underlying
tissues, including the temporal muscle, were subsequently retracted
to expose the full extent of the cranium. The periosteum was
resected to avoid any influence on bony regeneration. A 15-mm
diameter full-thickness defect, which was demonstrated to be the
critical-size defect (CSD) in previous studies (36,37), was
carefully prepared to avoid dural tears using a dental bar and
continuous irrigation with sterile saline at room temperature.
Rabbits were subsequently administered with their respective
treatments. The scalp was repositioned and sutured to achieve
primary closure. Each rabbit received a prophylactic intramuscular
injection of penicillin (25,000 IU/kg).
Computerized tomography
All rabbits were subjected to postoperative
computerized tomography (CT) examinations at 4, 6 and 8 weeks
post-surgery. CT image acquisition, processing, and manipulation
were performed according to the standard protocol of Zhengzhou
University (Zhengzhou, China). CT data were reconstructed into
three-dimensional (3D) images using CT included software (AW Basic
Display ver. 4.1; GE Healthcare Life Sciences, Chalfont, UK). The
craniofacial bone was extracted from the 3D CT images with the
threshold adjusted to remove the soft tissue and display the
bone.
Bone histological and
histomorphometric analysis
At 8 weeks post-surgery, rabbits were euthanized
humanely with an intravenous overdose of sodium barbiturate
(Sigma-Aldrich; Merck kGaA) (200 mg/kg). Calvaria were harvested,
decalcified in 10% formic acid and subsequently embedded in
paraffin. Serial sections of 5-µm thickness were cut perpendicular
to the mid-sagittal suture from the center of each defect using a
microtome (RM2155; Leica Microsystems GmbH, Wetzlar, Germany) and
stained with hematoxylin and eosin. The section displaying the
widest defect area was selected. Digital images of the selected
sections were captured using a light microscope at ×5 magnification
(DM16000; Leica Microsystems GmbH). New bone formation within the
defect was calculated histomorphometrically using Image-Pro Plus
7.0 software (Media Cybernetics, Inc., Rockville, MD, USA). The
percentage of new bone was calculated by dividing the bone area by
the whole defect area. All data were collected and analyzed by an
independent investigator to reduce bias and errors.
Statistical analysis
Data analysis was conducted using SPSS version 17.0
software (SPSS, Inc., Chicago, IL, USA). All data are presented as
the mean ± standard deviation. Comparisons between groups were
performed using the Student's t-test following a homogeneity test
of variance. P<0.05 was considered to indicate a statistically
significant difference.
Results
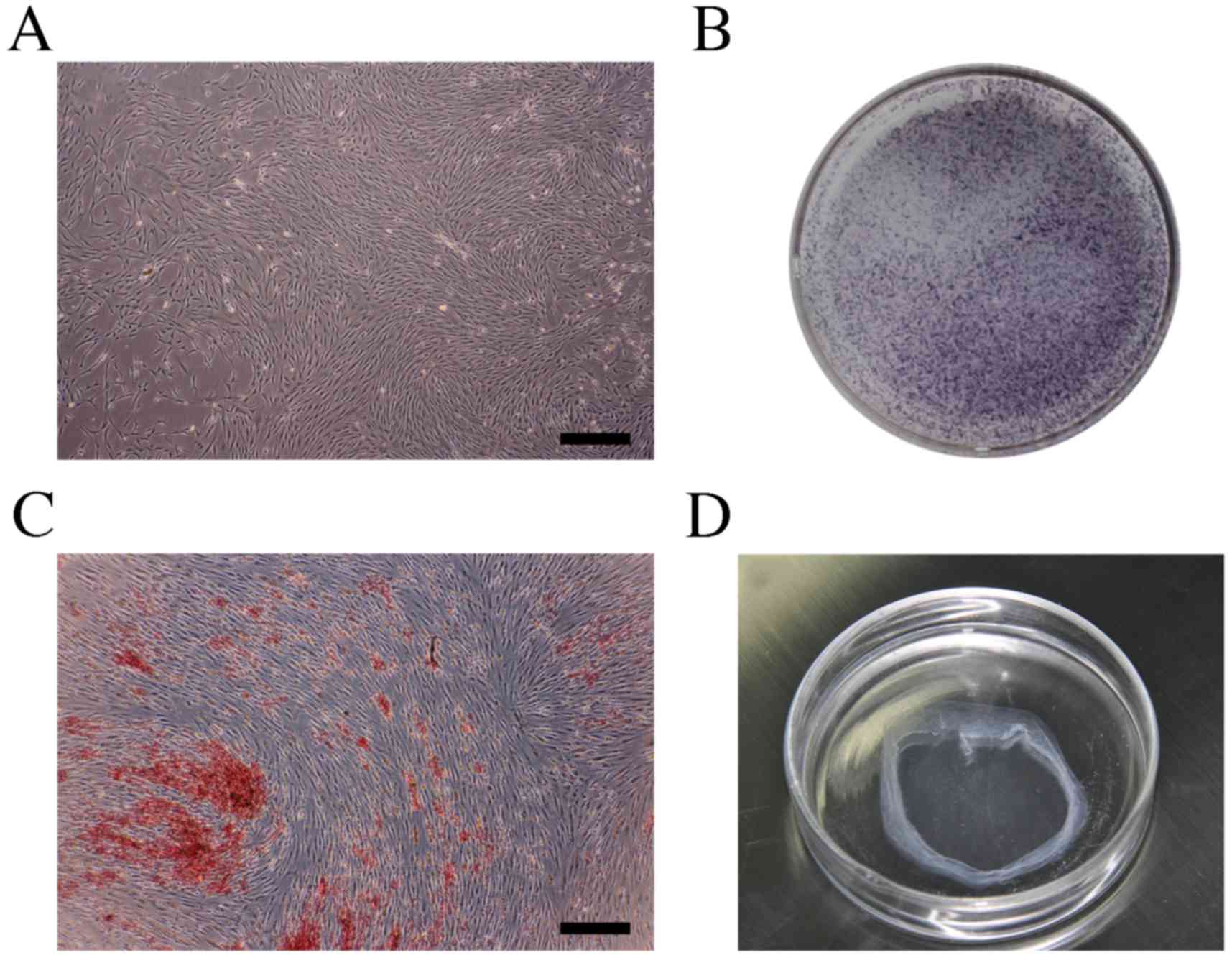
Osteogenic differentiation
ability
The osteogenic differentiation capacity was studied
after 7–21 days of culture under osteogenic culture conditions.
ALP, which catalyzes hydrolysis of phosphate esters at an alkaline
pH, is a well-known enzyme used as a marker of the osteogenic
phenotype (19). The morphology of
MSCs prior to osteogenic differentiation was recorded (Fig. 2A). In osteo-induced MSCs, ALP
staining revealed high ALP activity (Fig. 2B). Alizarin red S staining also
revealed a marked osteogenic differentiation capacity (Fig. 2C). These findings indicated that
cultured MSCs were able to differentiate into functional
osteoblast-like cells in vitro.
Fabrication of cell sheets
With 10 nM dexamethasone and 50 µg/ml ascorbic acid
stimulation, MSCs exhibited an increase in the synthesis of
extracellular matrix and formed dense cell sheets. Following 14
days of culture, cells were washed twice with PBS. Intact cell
sheets were subsequently able to be detached using a cell scraper
(Fig. 2D) and further manipulated
for wrapping with PRF/HA or HA alone.
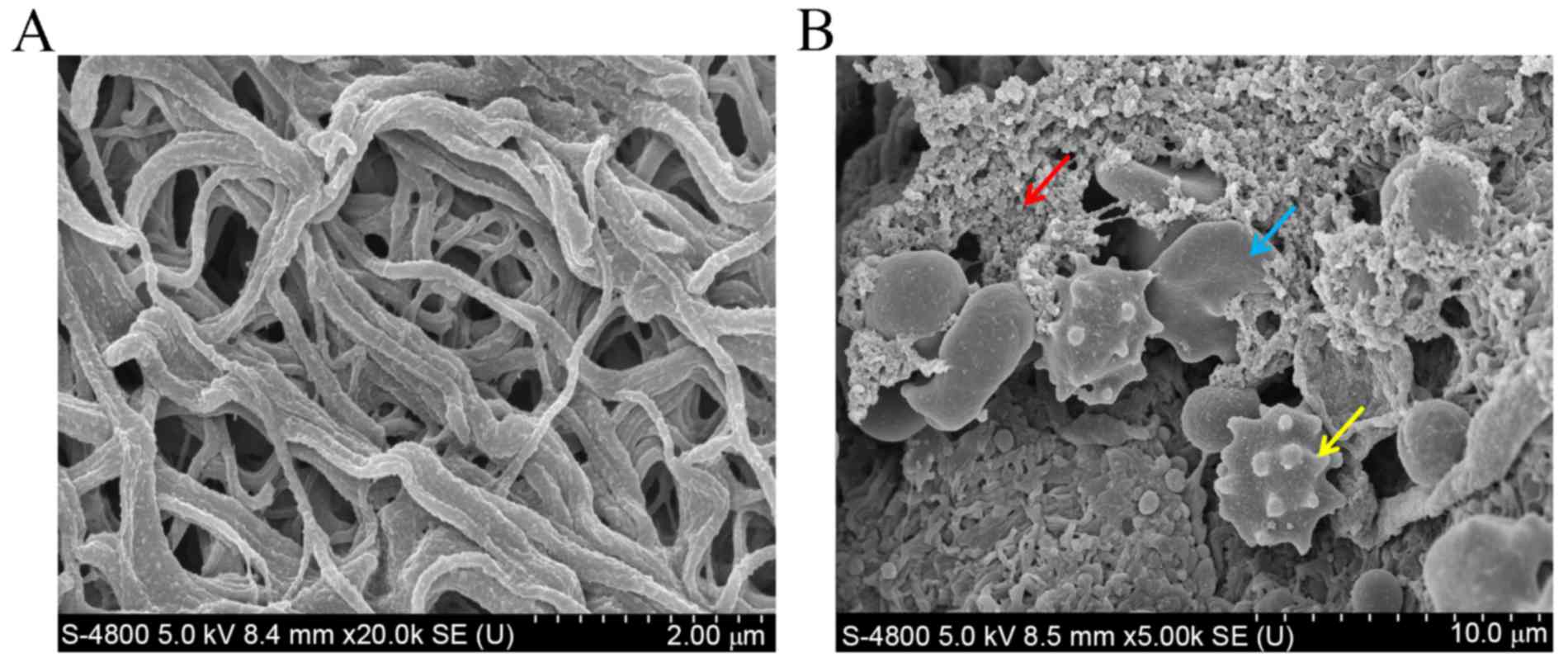
Ultrastructure of the PRF
SEM observation of the PRF clot revealed a scaffold
appearance, which contained randomly arranged fibrillar elements of
almost homogeneous thickness, constituting a 3D network (Fig. 3A). In the lower region of the fibrin
clot in particular, platelets, leukocytes and red blood cells were
embedded in the network (Fig. 3B).
It appeared, therefore, that the lower region of the PRF was more
suitable for clinical application.
Gross morphology of bone regeneration
in rabbits
All rabbits tolerated the anesthesia and the
surgical procedures well and experienced no complications during
the experimental period. There was no evidence of wound infection
or dehiscence from the implantation. The implants were well
integrated into the surrounding calvarial bone, and the defects
were closed. Palpation of the defects revealed that tight bone-like
structures filled the defect in the MSC/PRF and MSC groups. There
were no obvious macroscopic differences between the two
experimental groups. In the control group, all empty defects were
occupied with soft consistency tissue and no bone filling was
detected by palpation or exploration.
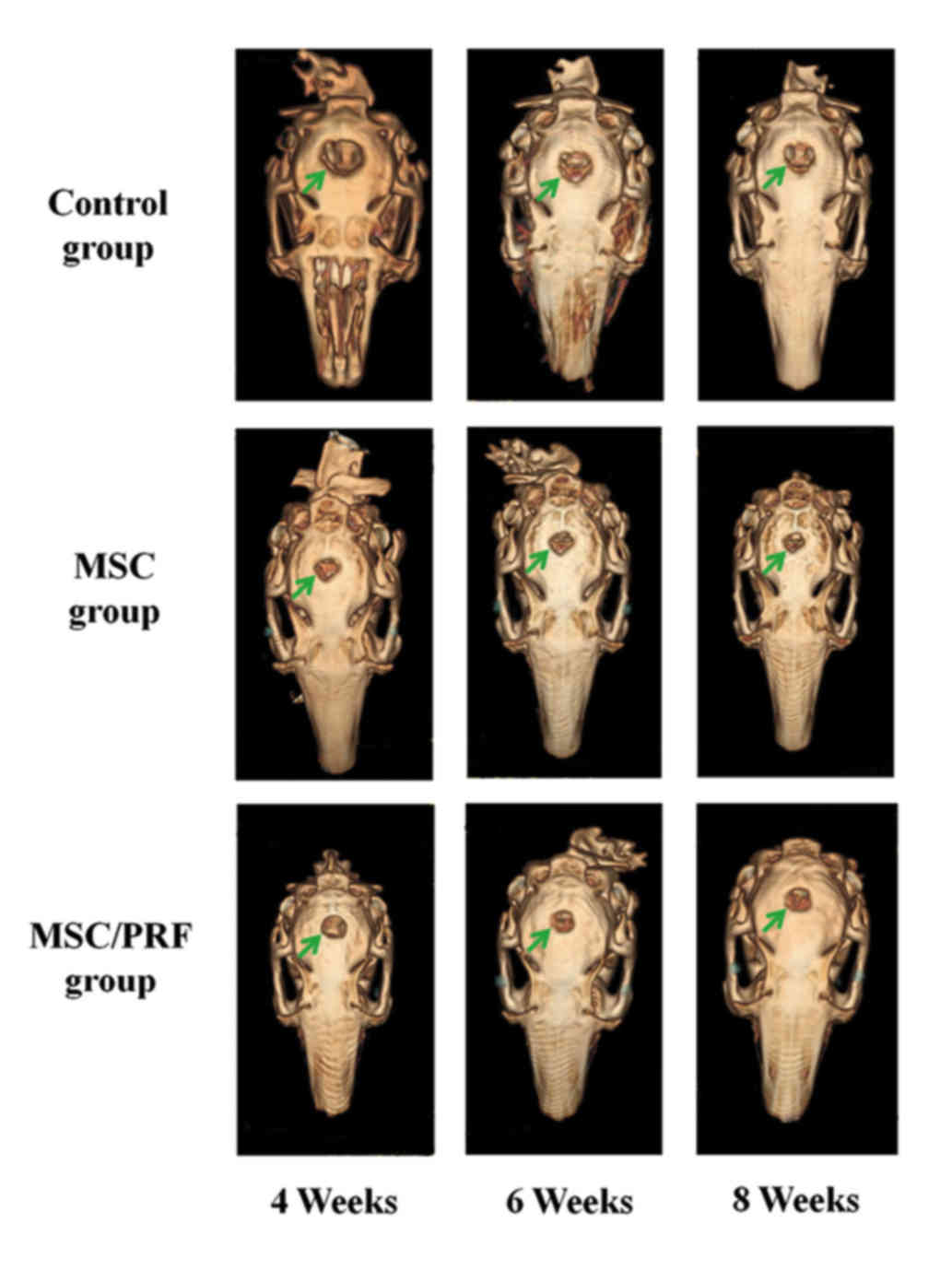
3D CT reconstruction results
Representative 3D CT images from each group are
presented in Fig. 4. Although a
lower radiodensity area was observed in part of the calvarium,
almost complete union was observed throughout the defect in the
group implanted with MSC/PRF composite, suggesting that substantial
levels of new bone were formed in the defect site. Most of area was
occupied by bone-like structures in the defect filled with PRF
composite; however, the center of the defect was still radiolucent,
which suggests less bone formation. In the control group, bone
formation close to the borders of the surrounding host calvarial
bone was observed, suggesting the lowest amount of bone formation
of the three groups.
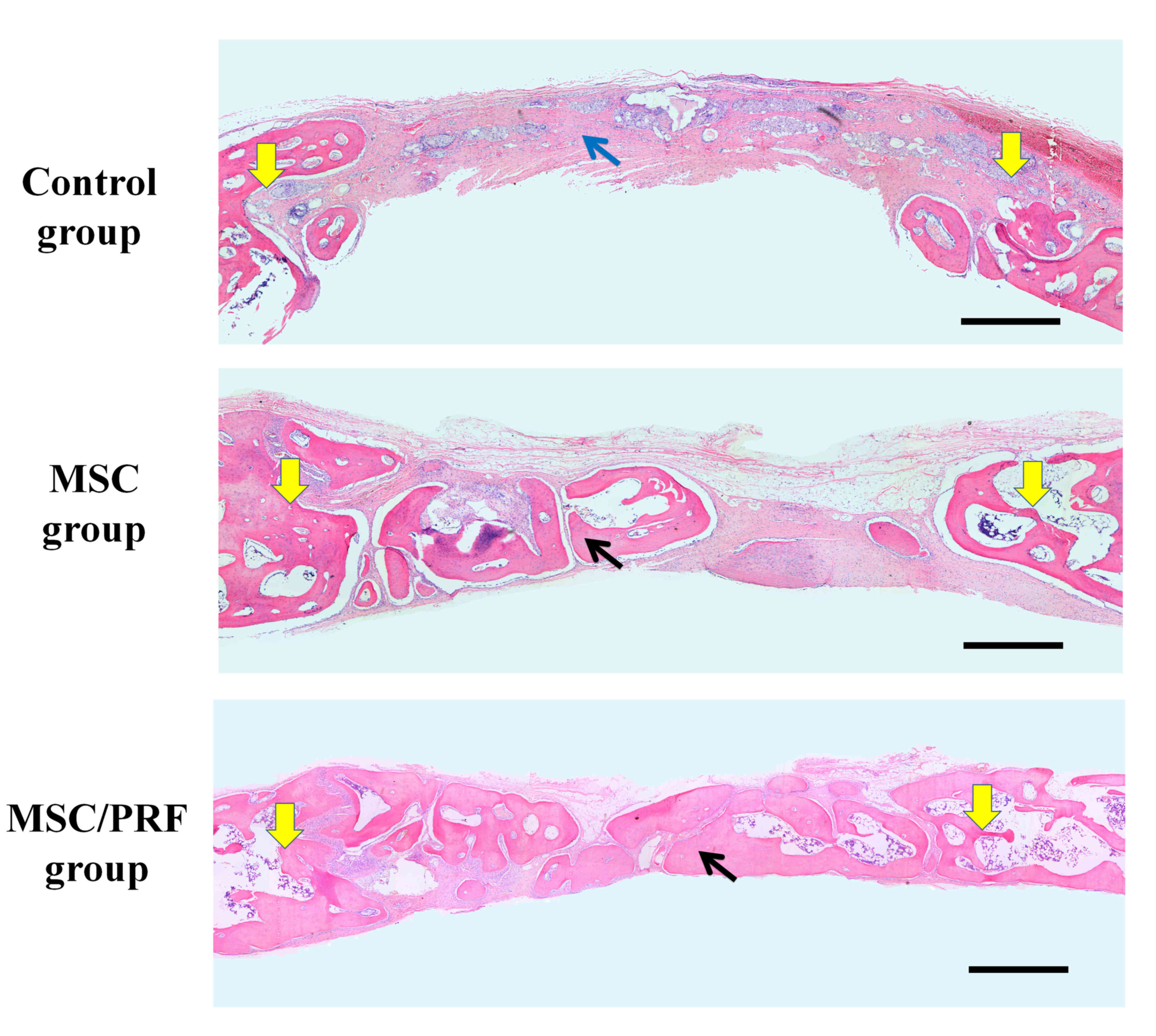
Histological results
Similar to the results obtained from 3D CT data, the
histological examination revealed variable amounts of calcification
in the defect sites of the calvarial specimens. Representative
histologic images for each group are presented in Fig. 5, with yellow arrows indicating the
sites of defect and blue/black arrows showing typical regenerative
tissue. In the MSC/PRF group, bony bridging and new bone formation
was observed throughout the center and the edges of the defect.
However, in the MSC group, relatively sparser bone formation was
observed, in particular at the center of the defect. In the control
group, fibrous tissues alone were observed in the defect area, with
a small amount of new bone formation at the defect margins. The
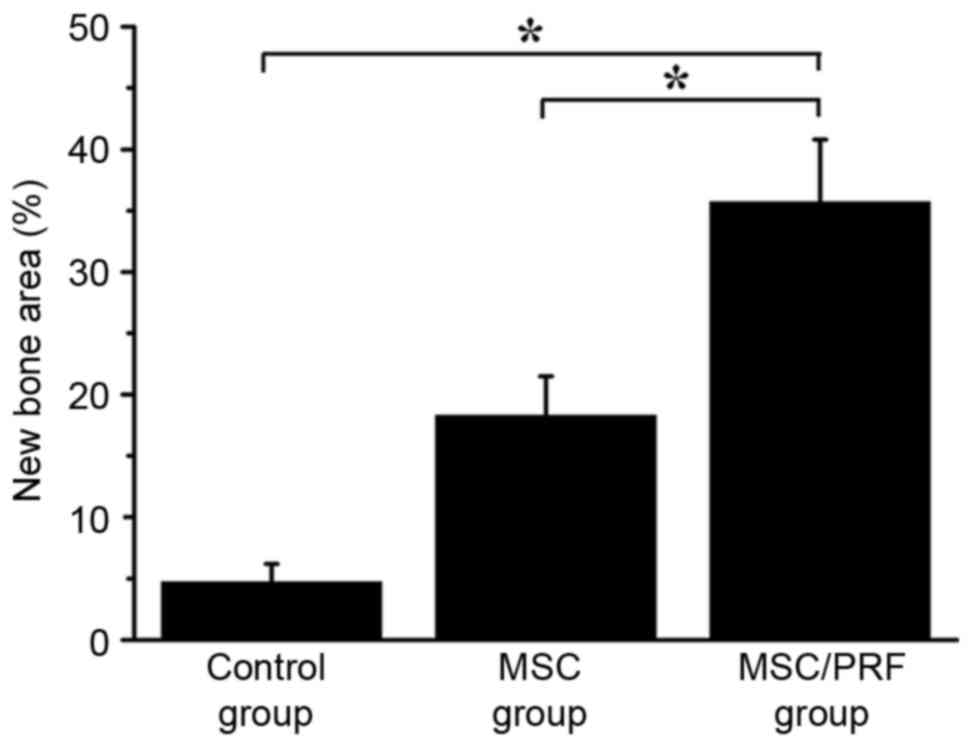
extent of new bone formation (% new bone area) in each group was
evaluated using Image-Pro Plus software. The amount of new bone was
significantly greater in the MSC/PRF group (35.7±5.1%) compared
with the MSC group (18.3±3.2%; P<0.05; Fig. 6). The percentage of new bone in the
MSC/PRF group was also significantly higher than that in the
control groups (4.7±1.5%; P<0.05, Fig. 6).
Discussion
The reconstruction of large bone defects caused by
tumors, trauma or inflammation remains a major clinical challenge
and tissue engineering is a promising technique for resolving this
problem (6). Tissue engineering
involves three main components: Multipotent stem cells,
biocompatible and biodegradable scaffolds and cytokines (38). Numerous attempts have been made to
optimize protocols for bone tissue engineering (39,40). In
the present study, it was hypothesized that a process may be
developed that incorporates MSC sheets with nano-HA and autologous
PRF granules for enhanced bone formation within a rabbit CSD model.
The results demonstrated that the MSC/PRF group regenerated
significantly more bone within the defect and achieved greater bony
bridging of the defect compared with the other two groups.
When comparing 3D CT images, different bone
regeneration modes specific to the three groups were clearly
observed. In the MSC/PRF group, bone regeneration was observed
progressively throughout both the center and the edges of the
defects. However, in the MSC group, bone formation occurred mainly
from the periphery of the defect, leaving the center of the defect
almost empty. In spite of this, by the end of the study the size of
the defect was significantly smaller than its original size. These
findings suggested that the presence of granular PRF may be an
essential requirement for effective bone regeneration. In the
control group, bone regenerated only at the edge of the defect, and
there was no obvious reduction in the defect area. The histological
and histomorphometry results supported those of the CT evaluation,
suggesting that the MSC/PRF group achieved the best osteogenic
healing effect. Compared with the MSC/PRF group, a sparser and
smaller amount of new bone formation was observed in the MSC group,
in particular in the center of the defect. At the end of the study,
the defect was almost completely occupied with fibrous tissues in
the control group.
In bone tissue engineering, the use of autologous
bone marrow-derived mesenchymal stem cells as sources, combined
with a biodegradable scaffold, is the golden standard (1). Bone marrow MSCs were first described by
Friedenstein et al (41) and
isolated by their adherence properties to plastic in tissue
culture. One of the critical functions of MSCs is to support the
process of bone remodeling by providing osteoblasts (42). In the present study, positive
Alizarin red and ALP staining also demonstrated that rabbit MSCs
were successfully induced into osteoblasts under the conditions of
osteogenic medium. Additionally, MSCs have been positioned at the
forefront of bone tissue engineering due to their other biological
properties, including paracrine and immunoregulatory capabilities
(43). A number of previous studies
have indicated that the secretion of various trophic factors and
cytokines may be a mechanism for use of MSCs in bone repair
(44,45). For instance, a broad repertoire of
angiogenic factors have been detected in the secretome of MSCs,
including vascular endothelial growth factor (VEGF), fibroblast
growth factor-2, angiopoietin-1, monocyte chemoattractant protein
−1, and interleukin (IL)-6 (8,45–48),
which may be important in bone regeneration. The immunosuppressive
effect of MSCs is well established in previous literature (49,50).
Specialized bioactive molecules secreted by MSCs may be able to
prevent unfavorable immune reactions and provide support to
repairing injured tissues (45). The
local immunosuppressive actions of MSCs have also led to
suggestions of allogeneic MSCs treatment in settings where the use
of autologous cells is limited or even impossible (42).
The cell sheet technique was used to harvest cells
and produce tissue-engineered bone. The application of cell sheets,
as a scaffold-free cell delivery system, has previously been
reported in the transplantation of MSCs to enhance the bone
formation (16,19). The use of cell sheets has several
advantages compared with current methods; firstly, as no invasive
enzymatic treatment is used, the intact cell sheet is harvested
along with its ECM, which is important for cell differentiation and
bone formation (51). Secondly, the
cell sheet also maintains cell-to-cell and cell-to-ECM connections,
which are typically required for the creation of functional tissues
(52). Adhesion molecules on the
cell surface, cell-to-cell interactions, and cell interconnections
with gap junctions, which mediate the reciprocal exchange of small
molecules and proteins, were addressed in a previous study by the
present authors (53). However, cell
sheets also have an intrinsic shortcoming as they have poor
mechanical strength, making them insufficient for larger defects
(54). To overcome this, previous
studies have utilized cell sheets reinforced with scaffold
materials. Zhou et al (6),
for example, used biodegradable scaffold-bone marrow stromal cell
sheet complexes. Layered cell sheets wrapped in a
polycaprolactone-tri-calcium phosphate scaffold were used to
enhance in vivo bone formation. Such complexes possess good
mechanical strength, so cell sheet techniques may provide a
potential novel approach to bone tissue engineering. In the present
study, nano-HA scaffolds were used to promote bone regeneration and
maintain the initial shape and volume of cell sheets, which
typically shrank spontaneously following detachment. Based on the
literature, it appears that nanocrystalline HA powders have better
biocompatibility, osteoinductivity, and even angioconductive
potential compared with coarser crystals, due to their superior
biological and biomechanical properties (55,56).
Additionally, Cai et al (57)
demonstrated that MSCs prepared with nano-HA exhibited greater cell
viability and proliferation properties compared with conventional
HA. The cell sheet/nano-HA scaffold may therefore contribute to
bone engineering due to its favorable mechanical properties,
including toughness and plasticity from the cell sheet and strength
from the nano-HA.
PRF belongs to a second generation of platelet
concentrates, and was used as a source of growth factors in the
current study. PRF is often defined as an autologous leukocyte- and
platelet-rich fibrin (28) and has
been widely used in maxillofacial and plastic surgery, and
tissue-engineering paradigms (26,58–60). The
results of the present study indicate that the PRF clot forms a
mechanically strong fibrin matrix with a 3D architecture in which
plenty of the platelets and leukocytes from the harvested blood are
concentrated in the lower red region of the clot. This is
concurrent with several previous reports (34,61).
Platelets are activated during the prepared process, which leads to
a substantial embedding of platelet growth factors into the fibrin
matrix (62), including
platelet-derived growth factor, insulin-like growth factors,
transforming growth factor β, VEGF and a myriad of other substances
which promote bone healing. The PRF protocol also induced an
increase in leukocyte degranulation (31). Many leukocyte growth factors, such as
IL-1β, IL-6, and tumor necrosis factor α, were trapped in the
fibrin networks during polymerization. With these cytokines
contributing to anti-infectious action and immune regulation, the
PRF clot may additionally be considered to be an immune organizing
node. Following application, the strong fibrin matrix of PRF was
slowly remodeled in a way similar to a natural blood clot (28) and growth factors were released in a
controlled and progressive way (63–65). A
previous study by the present authors (35) revealed that PRF growth factors were
released in a time-dependent manner. Such a releasing pattern may
result in longer-lasting biological effects, which initiate and
foster bone regeneration. The results of the present study suggest
that the use of PRF may offer an easy, cost-effective way to obtain
high concentrations of growth factors and stimulate bone
formation.
In the present study, a rabbit calvarial CSD model
was used because it is a well-documented model for evaluating bony
healing (66). It has previously
been suggested that calvaria is an anatomic area of limited
mechanical stress and relative stability of the surrounding
structures, and so is an ideal candidate for the study of
interactions between new bone constructs and in situ bone
(67). Furthermore, the patterns of
bone accretion and overall bone mass in rabbits during skeletal
maturation are similar to those in humans (68). Hollinger and Kleinschmidt (36) defined a CSD as a 15-mm defect in this
animal. To create a more challenging environment for bone
generation, the periosteum was also resected. The recommended
method of blood collection from rabbits is debated and a cardiac
puncture is often recommended (37).
In the present study, whole blood was harvested from the central
ear artery while the rabbit was restrained in a restraining box, a
method previously used by Lee and Pripatnanont (59,69).
The method of bone tissue engineering used in the
present study offers several advantages compared with the current
strategies used. Firstly, a cell sheet combined with nano-HA acted
as a bioactive scaffold in this bone regeneration protocol. An
ideal scaffold for bone tissue engineering is a matrix that acts as
a temporary substrate, allowing cell growth and tissue development
(15). The cell sheet/nano-HA
scaffold mimics the structure and biological function of the native
ECM in terms of both chemical composition and physical structure.
The composite scaffold had a certain degree of mechanical strength
and was able to fill the defect, and the scaffold may also be
biodegradable past the endpoint of the current study. Secondly,
granular PRF was used as the autologous growth factor carrier in
the present study. PRF has been the focus of previous experimental
and clinical studies (35,70,71).
However, as revealed by SEM in the present study, the structure of
PRF was non-homogenous. In the centrifugation process, slow
polymerization of collagen fibers in the blood formed a 3D network
structure. Due to the centrifugal force, the cellular components of
the blood were redistributed to the lower part of the tubes. Red
blood cells pelleted at the bottom of the tube, whereas platelets,
embedded into the fibrin matrix, lay between red blood cells and
the fibrous structure of PRF. This suggests that the most
functional section of the PRF was in the lower region of the fibrin
clot, which may be referred to as the ‘red tip’ due to its
adjacency to red blood cells, as it was able to provide numerous
growth factors. Therefore, the PRF was cut into small pieces and
mixed together to distribute the red tip and provide an even
concentration of growth factors across the whole bone regeneration
site.
There are several limitations to the present study.
Micro-CT 3D imaging of the specimen was not performed due to a lack
of equipment, and normal CT 3D imaging only provided a crude
demonstration of the effect of bone regeneration in the three
groups. Micro-CT may be able to provide more detailed pictures, and
so this tool should be utilized in future research. Another
limitation was the potential risk of using ex vivo expanded
MSCs. The expansion of MSCs in this study used α-MEM supplemented
with 10% FBS, which may introduce the risk of contamination or
adverse cellular changes (72,73).
Surgeons are hesitant to use a bovine derivative in human bone
regenerative procedures as a number of reports have documented the
development of anti-bovine antibodies that may cross-react with
human clotting agents (72–74). In order to replace the FBS, and thus
limit the potential re-implantation problems of cultivated MSCs,
previous researchers have attempted to find some substitutes
(7,44). Notably, PRF has been suggested as a
potential substitute (32). With
technological advancements, this issue may eventually be
resolved.
In conclusion, the combined application of an MSC
sheet with nano-HA and granular PRF may provide a novel approach
for bone tissue regeneration in large bone defects. Such a bone
tissue engineering protocol would be a promising therapeutic
strategy in bone regenerative medicine.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant nos. 31400839, 81400492
and 81402231).
References
|
1
|
Uchiyama H, Yamato M, Sasaki R, Sekine H,
Yang J, Ogiuchi H, Ando T and Okano T: In vivo 3D analysis with
micro-computed tomography of rat calvaria bone regeneration using
periosteal cell sheets fabricated on temperature-responsive culture
dishes. J Tissue Eng Regen Med. 5:483–490. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Giovanini AF, Deliberador TM, Gonzaga CC,
de Oliveira Filho MA, Göhringer I, Kuczera J, Zielak JC and de
Andrade Urban C: Platelet-rich plasma diminishes calvarial bone
repair associated with alterations in collagen matrix composition
and elevated CD34+ cell prevalence. Bone. 46:1597–1603. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Intini G: The use of platelet-rich plasma
in bone reconstruction therapy. Biomaterials. 30:4956–4966. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Burstein FD, Simms C, Cohen SR, Work F and
Paschal M: Iliac crest bone graft harvesting techniques: A
comparison. Plast Reconstr Surg. 105:34–39. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Monaco AP: The beginning of clinical
tolerance in solid organ allografts. Exp Clin Transplant.
2:153–161. 2004.PubMed/NCBI
|
|
6
|
Zhou Y, Chen F, Ho ST, Woodruff MA, Lim TM
and Hutmacher DW: Combined marrow stromal cell-sheet techniques and
high-strength biodegradable composite scaffolds for engineered
functional bone grafts. Biomaterials. 28:814–824. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kretlow JD, Spicer PP, Jansen JA, Vacanti
CA, Kasper FK and Mikos AG: Uncultured marrow mononuclear cells
delivered within fibrin glue hydrogels to porous scaffolds enhance
bone regeneration within critical-sized rat cranial defects. Tissue
Eng Part A. 16:3555–3568. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Porada CD, Zanjani ED and Almeida-Porad G:
Adult mesenchymal stem cells: A pluripotent population with
multiple applications. Curr Stem Cell Res Ther. 1:365–369. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gazit D, Turgeman G, Kelley P, Wang E,
Jalenak M, Zilberman Y and Moutsatsos I: Engineered pluripotent
mesenchymal cells integrate and differentiate in regenerating bone:
A novel cell-mediated gene therapy. J Gene Med. 1:121–133. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kon E, Muraglia A, Corsi A, Bianco P,
Marcacci M, Martin I, Boyde A, Ruspantini I, Chistolini P, Rocca M,
et al: Autologous bone marrow stromal cells loaded onto porous
hydroxyapatite ceramic accelerate bone repair in critical-size
defects of sheep long bones. J Biomed Mater Res. 49:328–337. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bianco P, Riminucci M, Gronthos S and
Robey PG: Bone marrow stromal stem cells: Nature, biology, and
potential applications. Stem Cells. 19:180–192. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Quarto R, Mastrogiacomo M, Cancedda R,
Kutepov SM, Mukhachev V, Lavroukov A, Kon E and Marcacci M: Repair
of large bone defects with the use of autologous bone marrow
stromal cells. N Engl J Med. 344:385–386. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yamada Y, Ueda M, Hibi H and Nagasaka T:
Translational research for injectable tissue-engineered bone
regeneration using mesenchymal stem cells and platelet-rich plasma:
From basic research to clinical case study. Cell Transplant.
13:343–355. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Meijer GJ, de Bruijn JD, Koole R and van
Blitterswijk CA: Cell based bone tissue engineering in jaw defects.
Biomaterials. 29:3053–3061. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhou H and Lee J: Nanoscale hydroxyapatite
particles for bone tissue engineering. Acta Biomater. 7:2769–2781.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jin H, Zhang K, Qiao C, Yuan A, Li D, Zhao
L, Shi C, Xu X, Ni S, Zheng C, et al: Efficiently engineered cell
sheet using a complex of polyethylenimine-alginate nanocomposites
plus bone morphogenetic protein 2 gene to promote new bone
formation. Int J Nanomedicine. 9:2179–2190. 2014.PubMed/NCBI
|
|
17
|
Yang J, Yamato M, Shimizu T, Sekine H,
Ohashi K, Kanzaki M, Ohki T, Nishida K and Okano T: Reconstruction
of functional tissues with cell sheet engineering. Biomaterials.
28:5033–5043. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ma D, Ren L, Liu Y, Chen F, Zhang J, Xue Z
and Mao T: Engineering scaffold-free bone tissue using bone marrow
stromal cell sheets. J Orthop Res. 28:697–702. 2010.PubMed/NCBI
|
|
19
|
Nakamura A, Akahane M, Shigematsu H,
Tadokoro M, Morita Y, Ohgushi H, Dohi Y, Imamura T and Tanaka Y:
Cell sheet transplantation of cultured mesenchymal stem cells
enhances bone formation in a rat nonunion model. Bone. 46:418–424.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bohner M: Calcium orthophosphates in
medicine: From ceramics to calcium phosphate cements. Injury.
31:(Suppl 4). S37–S47. 2000. View Article : Google Scholar
|
|
21
|
Johnson Wagoner AJ and Herschler BA: A
review of the mechanical behavior of CaP and CaP/polymer composites
for applications in bone replacement and repair. Acta Biomater.
7:16–30. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
LeGeros RZ: Biodegradation and
bioresorption of calcium phosphate ceramics. Clin Mater. 14:65–88.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Dorozhkin SV: Nanosized and
nanocrystalline calcium orthophosphates. Acta Biomater. 6:715–734.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kim ES, Park EJ and Choung PH: Platelet
concentration and its effect on bone formation in calvarial
defects: An experimental study in rabbits. J Prosthet Dent.
86:428–433. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ito K, Yamada Y, Naiki T and Ueda M:
Simultaneous implant placement and bone regeneration around dental
implants using tissue-engineered bone with fibrin glue, mesenchymal
stem cells and platelet-rich plasma. Clin Oral Implants Res.
17:579–586. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Liao HT, Chen CT, Chen CH, Chen JP and
Tsai JC: Combination of guided osteogenesis with autologous
platelet-rich fibrin glue and mesenchymal stem cell for mandibular
reconstruction. J Trauma. 70:228–237. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Anitua E, Sanchez M, Nurden AT, Nurden P,
Orive G and Andía I: New insights into and novel applications for
platelet-rich fibrin therapies. Trends Biotechnol. 24:227–234.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ehrenfest Dohan DM, Rasmusson L and
Albrektsson T: Classification of platelet concentrates: From pure
platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin
(L-PRF). Trends Biotechnol. 27:158–167. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Eppley BL, Woodell JE and Higgins J:
Platelet quantification and growth factor analysis from
platelet-rich plasma: Implications for wound healing. Plast
Reconstr Surg. 114:1502–1508. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tong W, Glimcher MJ, Katz JL, Kuhn L and
Eppell SJ: Size and shape of mineralites in young bovine bone
measured by atomic force microscopy. Calcif Tissue Int. 72:592–598.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Dohan DM, Choukroun J, Diss A, Dohan SL,
Dohan AJ, Mouhyi J and Gogly B: Platelet-rich fibrin (PRF): A
second-generation platelet concentrate. Part III: Leucocyte
activation: A new feature for platelet concentrates? Oral Surg Oral
Med Oral Pathol Oral Radiol Endod. 101:e51–e55. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ehrenfest Dohan DM, Doglioli P, de Peppo
GM, Del Corso M and Charrier JB: Choukroun's platelet-rich fibrin
(PRF) stimulates in vitro proliferation and differentiation of
human oral bone mesenchymal stem cell in a dose-dependent way. Arch
Oral Biol. 55:185–194. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Shimizu T, Yamato M, Isoi Y, Akutsu T,
Setomaru T, Abe K, Kikuchi A, Umezu M and Okano T: Fabrication of
pulsatile cardiac tissue grafts using a novel 3-dimensional cell
sheet manipulation technique and temperature-responsive cell
culture surfaces. Circ Res. 90:e402002. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Dohan DM, Choukroun J, Diss A, Dohan SL,
Dohan AJ, Mouhyi J and Gogly B: Platelet-rich fibrin (PRF): A
second-generation platelet concentrate. Part I: Technological
concepts and evolution. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 101:e37–e44. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zhao YH, Zhang M, Liu NX, Lv X, Zhang J,
Chen FM and Chen YJ: The combined use of cell sheet fragments of
periodontal ligament stem cells and platelet-rich fibrin granules
for avulsed tooth reimplantation. Biomaterials. 34:5506–5520. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hollinger JO and Kleinschmidt JC: The
critical size defect as an experimental model to test bone repair
materials. J Craniofac Surg. 1:60–68. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ehrenfest Dohan DM, Lemo N, Jimbo R and
Sammartino G: Selecting a relevant animal model for testing the in
vivo effects of Choukroun's platelet-rich fibrin (PRF): Rabbit
tricks and traps. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
110:413–418. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Langer R and Vacanti JP: Tissue
engineering. Science. 260:920–926. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Mattar P and Bieback K: Comparing the
immunomodulatory properties of bone marrow, adipose tissue and
birth-associated tissue mesenchymal stromal cells. Front Immunol.
6:5602015. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Yu X, Tang X, Gohil SV and Laurencin CT:
Biomaterials for bone regenerative engineering. Adv Healthc Mater.
4:1268–1285. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Friedenstein AJ, Chailakhyan RK, Latsinik
NV, Panasyuk AF and Keiliss-Borok IV: Stromal cells responsible for
transferring the microenvironment of the hemopoietic tissues.
Cloning in vitro and retransplantation in vivo. Transplantation.
17:331–340. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Bronckaers A, Hilkens P, Martens W,
Gervois P, Ratajczak J, Struys T and Lambrichts I: Mesenchymal
stem/stromal cells as a pharmacological and therapeutic approach to
accelerate angiogenesis. Pharmacol Ther. 143:181–196. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Satija NK, Singh VK, Verma YK, Gupta P,
Sharma S, Afrin F, Sharma M, Sharma P, Tripathi RP and Gurudutta
GU: Mesenchymal stem cell-based therapy: A new paradigm in
regenerative medicine. J Cell Mol Med. 13:4385–4402. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kagami H, Agata H and Tojo A: Bone marrow
stromal cells (bone marrow-derived multipotent mesenchymal stromal
cells) for bone tissue engineering: Basic science to clinical
translation. Int J Biochem Cell Biol. 43:286–289. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Caplan AI and Correa D: The MSC: An injury
drugstore. Cell Stem Cell. 9:11–15. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kinnaird T, Stabile E, Burnett MS, Lee CW,
Barr S, Fuchs S and Epstein SE: Marrow-derived stromal cells
express genes encoding a broad spectrum of arteriogenic cytokines
and promote in vitro and in vivo arteriogenesis through paracrine
mechanisms. Circ Res. 94:678–685. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Wu Y, Chen L, Scott PG and Tredget EE:
Mesenchymal stem cells enhance wound healing through
differentiation and angiogenesis. Stem Cells. 25:2648–2659. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Chen L, Tredget EE, Wu PY and Wu Y:
Paracrine factors of mesenchymal stem cells recruit macrophages and
endothelial lineage cells and enhance wound healing. PLoS One.
3:e18862008. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Del Papa N, Quirici N, Soligo D, Scavullo
C, Cortiana M, Borsotti C, Maglione W, Comina DP, Vitali C,
Fraticelli P, et al: Bone marrow endothelial progenitors are
defective in systemic sclerosis. Arthritis Rheum. 54:2605–2615.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Nauta AJ and Fibbe WE: Immunomodulatory
properties of mesenchymal stromal cells. Blood. 110:3499–3506.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Holtorf HL, Jansen JA and Mikos AG:
Ectopic bone formation in rat marrow stromal cell/titanium fiber
mesh scaffold constructs: Effect of initial cell phenotype.
Biomaterials. 26:6208–6216. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Yang J, Yamato M, Kohno C, Nishimoto A,
Sekine H, Fukai F and Okano T: Cell sheet engineering: Recreating
tissues without biodegradable scaffolds. Biomaterials.
26:6415–6422. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Wang X, Sha XJ, Li GH, Yang FS, Ji K, Wen
LY, Liu SY, Chen L, Ding Y and Xuan K: Comparative characterization
of stem cells from human exfoliated deciduous teeth and dental pulp
stem cells. Arch Oral Biol. 57:1231–1240. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Chen F, Zhou Y, Barnabas ST, Woodruff MA
and Hutmacher DW: Engineering tubular bone constructs. J Biomech.
40:(Suppl 1). S73–S79. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Stupp SI and Ciegler GW: Organoapatites:
Materials for artificial bone. I. Synthesis and microstructure. J
Biomed Mater Res. 26:169–183. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Appleford MR, Oh S, Oh N and Ong JL: In
vivo study on hydroxyapatite scaffolds with trabecular architecture
for bone repair. J Biomed Mater Res A. 89:1019–1027. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Cai Y, Liu Y, Yan W, Hu Q, Tao J, Zhang M,
Shi Z and Tang R: Role of hydroxyapatite nanoparticle size in bone
cell proliferation. J Mater Chem. 17:3780–3787. 2007. View Article : Google Scholar
|
|
58
|
Granchi D, Devescovi V, Baglio SR, Magnani
M, Donzelli O and Baldini N: A regenerative approach for bone
repair in congenital pseudarthrosis of the tibia associated or not
associated with type 1 neurofibromatosis: Correlation between
laboratory findings and clinical outcome. Cytotherapy. 14:306–314.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Pripatnanont P, Nuntanaranont T,
Vongvatcharanon S and Phurisat K: The primacy of platelet-rich
fibrin on bone regeneration of various grafts in rabbit's calvarial
defects. J Craniomaxillofac Surg. 41:e191–e200. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Xuan F, Lee CU, Son JS, Jeong SM and Choi
BH: A comparative study of the regenerative effect of sinus bone
grafting with platelet-rich fibrin-mixed Bio-Oss® and
commercial fibrin-mixed Bio-Oss®: An experimental study.
J Craniomaxillofac Surg. 42:e47–e50. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Tunali M, Özdemir H, Küçükodaci Z, Akman S
and Firatlı E: In vivo evaluation of titanium-prepared
platelet-rich fibrin (T-PRF): A new platelet concentrate. Br J Oral
Maxillofac Surg. 51:438–443. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Dohan DM, Choukroun J, Diss A, Dohan SL,
Dohan AJ, Mouhyi J and Gogly B: Platelet-rich fibrin (PRF): A
second-generation platelet concentrate. Part II: Platelet-related
biologic features. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 101:e45–e50. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Ehrenfest Dohan DM, de Peppo GM, Doglioli
P and Sammartino G: Slow release of growth factors and
thrombospondin-1 in Choukroun's platelet-rich fibrin (PRF): A gold
standard to achieve for all surgical platelet concentrates
technologies. Growth Factors. 27:63–69. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
He L, Lin Y, Hu X, Zhang Y and Wu H: A
comparative study of platelet-rich fibrin (PRF) and platelet-rich
plasma (PRP) on the effect of proliferation and differentiation of
rat osteoblasts in vitro. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod. 108:707–713. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Liu B, Tan XY, Liu YP, Xu XF, Li L, Xu HY,
An R and Chen FM: The adjuvant use of stromal vascular fraction and
platelet-rich fibrin for autologous adipose tissue transplantation.
Tissue Eng Part C Methods. 19:1–14. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Schmitz JP and Hollinger JO: The critical
size defect as an experimental model for craniomandibulofacial
nonunions. Clin Orthop Relat Res. 299–308. 1986.PubMed/NCBI
|
|
67
|
Ade Costa M, Kobayashi GS, Bueno DF,
Martins MT, Mde Ferreira C, Passos-Bueno MR and Alonso N: An
experimental model for the study of craniofacial deformities. Acta
Cir Bras. 25:264–268. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Djasim UM, Wolvius EB, van Neck JW,
Weinans H and van der Wal KGH: Recommendations for optimal
distraction protocols for various animal models on the basis of a
systematic review of the literature. Int J Oral Maxillofac Surg.
36:877–883. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Lee EH, Kim JY, Kweon HY, Jo YY, Min SK,
Park YW, Choi JY and Kim SG: A combination graft of
low-molecular-weight silk fibroin with Choukroun platelet-rich
fibrin for rabbit calvarial defect. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod. 109:e33–e38. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Zhang Y, Tangl S, Huber CD, Lin Y, Qiu L
and Rausch-Fan X: Effects of Choukroun's platelet-rich fibrin on
bone regeneration in combination with deproteinized bovine bone
mineral in maxillary sinus augmentation: A histological and
histomorphometric study. J Craniomaxillofac Surg. 40:321–328. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Li Q, Pan S, Dangaria SJ, Gopinathan G,
Kolokythas A, Chu S, Geng Y, Zhou Y and Luan X: Platelet-rich
fibrin promotes periodontal regeneration and enhances alveolar bone
augmentation. Biomed Res Int. 2013:6380432013.PubMed/NCBI
|
|
72
|
Boquest AC, Shahdadfar A, Frønsdal K,
Sigurjonsson O, Tunheim SH, Collas P and Brinchmann JE: Isolation
and transcription profiling of purified uncultured human stromal
stem cells: Alteration of gene expression after in vitro cell
culture. Mol Biol Cell. 16:1131–1141. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Lepperdinger G, Brunauer R, Jamnig A,
Laschober G and Kassem M: Controversial issue: Is it safe to employ
mesenchymal stem cells in cell-based therapies? Exp Gerontol.
43:1018–1023. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Lawson JH: The clinical use and
immunologic impact of thrombin in surgery. Semin Thromb Hemost.
32:(Suppl 1). S98–S110. 2006. View Article : Google Scholar
|